Background: Diabetes Mellitus (DM), a chronic disease characterized by elevated blood glucose levels, is associated with severe complications. Type 2 DM (T2DM), the most prevalent form of DM in adults, is characterized by varying degrees of insulin deficiency or resistance. The prevention or delay of macrovascular and microvascular problems associated with DM depends on achieving appropriate glycemic control. The percentage of T2DM patients failing to reach glycemic targets keeps rising even with the expanded availability of numerous anti-hyperglycemic drugs and evidence-based treatment guidelines. The delay in treatment intensification despite inadequate glucose control—often referred to as clinical or therapeutic inertia-contributes significantly to this trend. Objective: This study aims to evaluate the understanding and perceptions of insulin therapy among patients with T2DM. The study focuses on patients under follow-up care at the Adult Endocrine Clinic of St. Paul Hospital Millennium Medical College. Method and Material: An institutional-based, cross-sectional study was carried out from January to March 2021 to evaluate knowledge and attitudes regarding insulin therapy and related factors. A structured questionnaire was used for interviews with a representative sample of 271 T2DM patients who are receiving follow-up care at the endocrine clinic at SPHMMC. The SPSS, version 25, was the software utilized. The statistical significance of the relationship between the dependent and independent variables was assessed using a 95% confidence interval and a p-value less than 0.05. Results: The majority of the respondents were between the ages of 56 and 65, with a mean age of 57.35 years. More than half of the participants, accounting for 231 (85.2%) of the total, were from urban areas. Out of the 271 respondents, approximately 85.6% demonstrated poor knowledge of insulin therapy, and around 37.6% exhibited negative attitudes towards it. Factors such as age, occupation, and a history of long-term Oral Antidiabetic Drug use were found to be associated with the level of knowledge about insulin. In addition to these factors, marital status and a family history of insulin use were found to be associated with patients’ attitudes towards insulin. Conclusions: Our study identified a significant knowledge gap about insulin usage among T2DM patients in the designated study area. We recommend the implementation of regular, structured health education programs, delivered by trained health professionals. This approach is expected to enhance both the knowledge and attitudes toward insulin usage among patients attending follow-up sessions at the SPHMMC diabetic clinic.
| Published in | International Journal of Diabetes and Endocrinology (Volume 9, Issue 2) |
| DOI | 10.11648/j.ijde.20240902.11 |
| Page(s) | 22-38 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Diabetes Mellitus, Insulin, Knowledge, Attitude, Ethiopia
2.1. Study Area and Period
2.2. Study Design
2.3. Population
2.3.1. Source Population
2.3.2. Study Population
2.4. Inclusion and Exclusion Criteria
2.4.1. Inclusion Criteria
2.4.2. Exclusion Criteria
2.5. Sample Size and Sampling Technique
2.6. Study Variables
2.6.1. Independent Variables
2.6.2. Dependent Variables
2.7. Operational Definitions
2.8. Data Collection and Analysis
2.9. Data Quality Assurance and Management
2.10. Ethical Consideration
3.1. Sociodemographic Characteristics
Variable | Frequency | Percent |
|---|---|---|
Age | ||
45 &below | 47 | 17.3 |
46-55 | 76 | 28.0 |
56-65 | 85 | 31.4 |
Above 65 | 63 | 23.2 |
Sex | ||
Male | 134 | 49.4 |
Female | 137 | 50.6 |
Residency | ||
Urban | 231 | 85.2 |
Rural | 40 | 14.8 |
Religion | ||
Orthodox | 121 | 44.6 |
Muslim | 68 | 25.1 |
Catholic | 20 | 7.4 |
Protestant | 61 | 22.5 |
Other | 1 | .4 |
Marital status | ||
Married | 181 | 66.8 |
Widowed | 37 | 13.7 |
Single | 37 | 13.7 |
Divorced | 16 | 5.9 |
Income | ||
<1000 | 57 | 21.0 |
1000-3000 | 97 | 35.8 |
>3000 | 117 | 43.2 |
3.2. DM-Related Characteristics
Variable | Frequency | Percent |
|---|---|---|
Duration of DM | ||
<5yrs | 82 | 30.3 |
5-10yrs | 109 | 40.2 |
>10yrs | 80 | 29.5 |
Current medication | ||
One OAD | 109 | 40.2 |
Two OADs | 162 | 59.8 |
For how long been on this medication | ||
<3yrs | 64 | 23.6 |
3-5yrs | 54 | 19.9 |
>5yrs | 153 | 56.5 |
Family hx of insulin use | ||
Yes | 75 | 27.7 |
No | 196 | 72.3 |
Member of EDA | ||
Yes | 81 | 29.9 |
No | 190 | 70.1 |
3.3. Insulin Knowledge of the Respondents
Variable | Frequency | Percent |
|---|---|---|
Do you know why insulin is prescribed for DM? | ||
To treat high blood pressure | 10 | 3.7 |
To lower blood glucose level | 152 | 56.1 |
To cure DM | 77 | 28.4 |
Don't know | 32 | 11.8 |
Do you know where or how to store insulin? | ||
Refrigerator | 84 | 31.0 |
Any cold place | 36 | 13.3 |
Sand soaked with water | 52 | 19.2 |
Anywhere | 14 | 5.2 |
Don't know | 85 | 31.4 |
Do you know the sites of insulin injection (more than one answer is possible) | ||
Deltoid | 40 | 14.8 |
Abdomen | 65 | 24.0 |
Thigh | 52 | 19.2 |
Gluteus | 11 | 4.1 |
Don't know | 103 | 38.0 |
Do you know how to inject insulin? | ||
Yes | 74 | 27.3 |
No | 192 | 70.8 |
Don't know | 5 | 1.8 |
Do you know the different types of insulin/insulin delivery systems? | ||
Yes | 35 | 12.9 |
No | 228 | 84.1 |
don't know | 8 | 3.0 |
Do you think it's necessary to rotate sites of injection? | ||
Yes | 115 | 42.4 |
No | 143 | 52.8 |
Don't know | 13 | 4.8 |
Frequency | Percent | |
|---|---|---|
Good knowledge | 39 | 14.4 |
Poor knowledge | 232 | 85.6 |
3.4. Insulin Attitude
Variable | S. agree | Agree | Agree nor Disagree | Disagree | S. disagree |
|---|---|---|---|---|---|
Taking insulin means I have failed to manage my DM with diet and tablets | 53 (19.6%) | 150 (55.4%) | 34 (12.5%) | 22 (8.1%) | 12 (4.4%) |
Taking insulin means my DM has become worse | 45 (16.6%) | 64 (23.6%) | 48 (17.7%) | 42 (15.5%) | 72 (26.6%) |
Taking insulin helps to prevent complications of DM | 27 (10.0%) | 126 (46.5%) | 71 (26.2%) | 41 (15.1%) | 6 (2.2%) |
Taking insulin means other people see me as a sicker person | 33 (12.2%) | 66 (24.4%) | 79 (29.2%) | 67 (24.7%) | 26 (9.6%) |
Taking insulin makes life less flexible | 25 (9.2%) | 57 (21.0%) | 95 (35.1%) | 76 (28.0%) | 18 (6.6%) |
I'm afraid of injecting myself with a needle | 37 (13.7%) | 82 (30.3%) | 40 (14.8%) | 85 (31.4%) | 27 (31.4%) |
Taking insulin increases the risk of low blood glucose level (hypoglycemia) | 17 (6.3%) | 78 (28.8%) | 101 (37.3%) | 56 (20.7%) | 19 (7.0%) |
Taking insulin helps to improve my health | 32 (11.8%) | 117 (43.2%) | 72 (26.6%) | 44 (16.2%) | 6 (2.2%) |
Insulin causes weight gain | 4 (1.5%) | 29 (10.7%) | 152 (56.1%) | 71 (26.2%) | 15 (5.5%) |
Managing insulin injection takes a lot of time and energy | 20 (7.4%) | 82 (30.3%) | 68 (25.1%) | 85 (31.4%) | 16 (5.9%) |
Taking insulin means I have to give up activities I enjoy | 25 (9.2%) | 73 (26.9%) | 102 (37.6%) | 62 (22.9%) | 9 (3.3%) |
Taking insulin means my health will deteriorate | 7 (2.6%) | 43 (15.9%) | 62 (22.9%) | 71 (26.2%) | 88 (32.5%) |
Injecting insulin is embarrassing | 21 (7.7%) | 40 (14.8%) | 57 (21.0%) | 121 (44.6%) | 32 (11.8%) |
Injecting insulin is painful | 28 (10.3%) | 92 (33.9%) | 37 (13.7%) | 99 (36.5% | 15 (5.5%) |
It's difficult to inject the right amount of insulin correctly at a tight time every day | 109 (40.2%) | 98 (36.2%) | 31 (11.4%) | 24 (8.9%) | 9 (3.3%) |
Taking insulin makes it more difficult to fulfill my responsibilities (at work/home | 24 (8.9%) | 70 (25.8%) | 87 (32.1%) | 78 (28.8%) | 12 (4.4%) |
Taking insulin helps to maintain good control of blood glucose | 38 (14.0%) | 125 (46.1%) | 72 (26.6%) | 34 (12.5%) | 2 (.7%) |
Being on insulin causes family and friends to be more concerned about me | 70 (25.8%) | 69 (25.5%) | 63 (23.2%) | 60 (22.1%) | 9 (3.3%) |
Taking insulin helps to improve my energy level | 15 (5.5%) | 127 (46.9%) | 70 (25.8%) | 48 (17.7%) | 11 (4.1%) |
Taking insulin makes me more dependent on others | 45 (16.6%) | 70 (25.8%) | 35 (12.9%) | 62 (22.9%) | 59 (21.8%) |
Frequency | Percent | |
|---|---|---|
Negative Attitude | 102 | 37.6 |
Positive Attitude | 169 | 62.4 |
3.5. DM Knowledge
Variable | Frequency | Percent |
|---|---|---|
What is DM | ||
DM is a raised blood sugar level only | 182 | 67.2 |
DM is a disease which can affect any part of the body | 66 | 24.4 |
I don't know | 23 | 8.5 |
DM can be detected through | ||
Blood examination | 198 | 73.1 |
Urine examination | 55 | 20.3 |
Don't know | 18 | 6.6 |
Do you know the symptoms of poorly controlled DM? | ||
Passing lots of urine | 128 | 47.2 |
Excessive thirst | 87 | 32.1 |
Tiredness | 36 | 13.3 |
Weight loss | 13 | 4.8 |
Don't know | 7 | 2.6 |
What are the symptoms of hypoglycemia? | ||
Hunger | 69 | 25.5 |
Nervousness | 85 | 31.4 |
Dizziness and lightheadedness | 86 | 31.7 |
Sleepiness | 29 | 10.7 |
Don't know | 2 | .7 |
What type of lifestyle modification do you think will help the control of DM? | ||
Exercise | 111 | 41.0 |
Dietary modification | 143 | 52.8 |
Weight reduction | 17 | 6.3 |
Controlling blood glucose levels is important for reducing DM-related complications | ||
True | 228 | 84.1 |
False | 17 | 6.3 |
Don't know | 26 | 9.6 |
Do you know about hgba1c | ||
Yes | 157 | 57.9 |
No | 114 | 42.1 |
How frequently should a diabetic patient measure his/her glucose level? | ||
Daily | 27 | 10.0 |
Weekly | 106 | 39.1 |
Monthly | 111 | 41.0 |
Every six month | 27 | 10.0 |
Which is the best method for home glucose | ||
Blood | 9 | 3.3 |
Urine | 209 | 77.1 |
Don’t know | 53 | 19.6 |
Are you aware that insulin is mandatory for T2DM at some point? | ||
Yes | 165 | 60.9 |
No | 106 | 39.1 |
Frequency | Percent | |
|---|---|---|
Good knowledge | 167 | 61.6 |
Poor knowledge | 104 | 38.4 |
3.6. Factors Affecting Insulin Knowledge Using Multivariable Analysis
Variables | Knowledge of Insulin Model 1 | ||
|---|---|---|---|
n | P-value | AOR 95%CI | |
Age | |||
45 &below | 47 | .031* | 1 (R) |
46-55 | 76 | .005* | .015 (.001,.285) |
56-65 | 85 | .029* | .051 (.004,.732) |
Above 65 | 63 | .072 | .103 (.009, 1.221) |
Sex | |||
Male | 134 | 1 (R) | |
Female | 137 | .550 | 1.506 (.393, 5.779) |
Residency | |||
Urban | 231 | 1 (R) | |
Rural | 40 | .997 | .000 (.000) |
Marital status | |||
Married | 181 | .735 | 1 (R) |
Widowed | 37 | .642 | .580 (.058, 5.768) |
Single | 37 | .749 | 1.572 (.099, 25.044) |
Divorced | 16 | .884 | .823 (.060, 11.326) |
Income | |||
<1000 | 57 | .315 | 1 (R) |
1000-3000 | 97 | .903 | .855 (.069, 10.612) |
>3000 | 117 | .247 | 3.096 (.456, 21.021) |
Occupation | |||
Employed | 55 | .070 | 1 (R) |
Unemployed | 40 | .858 | .787 (.056, 10.992) |
Farmer | 13 | .745 | 1.557 (.108, 22.507) |
Daily laborer | 39 | .693 | 2.072 (.055, 77.424) |
Merchant | 74 | .021* | 83.212 (1.921, 3603.823) |
Retired | 9 | .355 | 3.198 (.272, 37.561) |
Other | 41 | .999 | 30204655.138 (.000) |
Educational level | |||
Illiterate | 21 | .385 | 1 (R) |
Read and write | 42 | .998 | 8603684.196 (.000) |
Literate | 71 | .282 | .277 (.027, 2.871) |
Primary school | 44 | .462 | .472 (.064, 3.494) |
Secondary school | 93 | .056 | .152 (.022, 1.048) |
Duration of DM | |||
<5yrs | 82 | .339 | 1 (R) |
5-10yrs | 109 | .551 | 2.339 (.144, 38.049) |
>10yrs | 80 | .142 | 2.692 (.719, 10.078) |
Complications of DM | |||
Ophthalmologic | 117 | .240 | 1 (R) |
Renal failure | 43 | 1.000 | 16754178.241 (.000) |
Neurologic | 44 | 1.000 | 11659548.937 (.000) |
Cardiovascular | 46 | 1.000 | 14800764.571 (.000) |
Diabetic foot ulcer | 19 | 1.000 | 81166411.411 (.000) |
Don’t know | 2 | 1.000 | 3675091.924 (.000) |
For how long been on this medication | |||
<3yrs | 64 | .040* | 1 (R) |
3-5yrs | 54 | .011* | 7.227 (1.561, 33.464) |
>5yrs | 153 | .171 | 2.426 (.682, 8.631) |
Family hx of insulin use | |||
Yes | 75 | 1 (R) | |
No | 196 | .220 | .472 (.142, 1.566) |
Member of EDA | |||
Yes | 81 | 1 (R) | |
No | 190 | .094 | .376 (.120, 1.180) |
DM knowledge | |||
Good knowledge | 167 | 1 (R) | |
Poor knowledge | 104 | .108 | .310 (.074, 1.295) |
3.7. Factors Affecting Insulin Attitude Using Multivariable Analysis
Variables | Attitude of Insulin Model 2 | ||
|---|---|---|---|
n | P-value | AOR 95%CI | |
Age | |||
45 &below | 47 | .155 | 1 (R) |
46-55 | 76 | .033* | .210 (.050,.878) |
56-65 | 85 | .091 | .329 (.091, 1.194) |
Above 65 | 63 | .297 | .535 (.165, 1.734) |
Sex | |||
Male | 134 | ||
Female | 137 | .577 | .793 (.351, 1.792) |
Residency | |||
Urban | 231 | 1 (R) | |
Rural | 40 | .146 | .291 (.055, 1.536) |
Marital status | |||
Married | 181 | .075 | 1 (R) |
Widowed | 37 | .036* | .142 (.023,.883) |
Single | 37 | .032* | .096 (.011,.816) |
Divorced | 16 | .416 | .423 (.053, 3.360) |
Income | |||
<1000 | 57 | .189 | 1 (R) |
1000-3000 | 97 | .256 | .374 (.069, 2.042) |
>3000 | 117 | .068 | .309 (.087, 1.090) |
Occupation | |||
Employed | 55 | .482 | 1 (R) |
Unemployed | 40 | .086 | .230 (.043, 1.229) |
Farmer | 13 | .042* | .178 (.034,.937) |
Daily laborer | 39 | .676 | .515 (.023, 11.578) |
Merchant | 74 | .099 | .165 (.020, 1.404) |
Retired | 9 | .113 | .332 (.085, 1.298) |
Other | 41 | .085 | .085 (.005, 1.406) |
Educational level | |||
Illiterate | 21 | .595 | 1 (R) |
Read and write | 42 | .464 | 2.428 (.225, 26.144) |
Literate | 71 | .134 | 3.676 (.670, 20.153) |
Primary school | 44 | .335 | 1.918 (.510, 7.208) |
Secondary school | 93 | .712 | 1.297 (.327, 5.146) |
Duration of DM | |||
<5yrs | 82 | .275 | 1 (R) |
5-10yrs | 109 | .233 | 2.611 (.539, 12.645) |
>10yrs | 80 | .120 | 2.105 (.823, 5.388) |
Complications of DM | |||
Ophthalmologic | 117 | .161 | 1 (R) |
Renal failure | 43 | 1.000 | .000 (.000) |
Neurologic | 44 | 1.000 | .000 (.000) |
Cardiovascular | 46 | 1.000 | .000 (.000) |
Diabetic foot ulcer | 19 | 1.000 | 000 (.000) |
Don’t know | 2 | 1.000 | 000 (.000) |
For how long been on this medication | |||
<3yrs | 64 | .040* | 1 (R) |
3-5yrs | 54 | .011* | 7.227 (1.561, 33.464) |
>5yrs | 153 | .171 | 2.426 (.682, 8.631) |
Family hx of insulin use | |||
Yes | 75 | 1 (R) | |
No | 196 | .001* | .244 (.104,.569) |
Member of EDA | |||
Yes | 81 | 1 (R) | |
No | 190 | .083 | 2.064 (.909, 4.687) |
DM knowledge | |||
Good knowledge | 167 | 1 (R) | |
Poor knowledge | 104 | .074 | .467 (.203, 1.076) |
5.1. Strength of the Study
5.2. Limitation
| [1] | Atlas IDFD. (2019). IDF 2019. Retrieved from |
| [2] | World Health Organization. (n.d.). Global report on Diabetes. Retrieved from |
| [3] | Muhammad, S., Shah, A., Butt, Z., & Hussain, K. (2017). Factors Leading to Psychological Insulin Resistance Among Patients with Type 2 Diabetes Mellitus. Annals of Pakistan Institute of Medical Sciences, 226-230. |
| [4] | Khunti, S., Davies, M. J., & Khunti, K. (2015). Clinical inertia in the management of type 2 diabetes mellitus: A focused literature review. British Journal of Diabetes & Vascular Disease, 15(2), 65-69. |
| [5] | van Bruggen, R., Gorter, K., Stolk, R., Klungel, O., & Rutten, G. (2009). Clinical inertia in general practice: Widespread and related to the outcome of diabetes care. Family Practice, 26(6), 428-436. |
| [6] | Gherman, A. (2011). Psychological insulin resistance: a critical review of the literature. Practical Diabetes International. Retrieved from Wiley Online Library. |
| [7] | Haque, M., Navsa, M., Emerson, S. H., Dennison, C. R., & Levitt, N. S. (2005). Barriers to initiating insulin therapy in patients with type 2 diabetes mellitus in public-sector primary health care centers in Cape Town. Journal of Endocrinology, Metabolism and Diabetes of South Africa, 10(3), 94–99. |
| [8] | Peyrot, M., Rubin, R. R., Lauritzen, T., Skovlund, S. E., Snoek, F. J., Matthews, D. R., & others. (2005). Resistance to insulin therapy among patients and providers: Results of the cross-national Diabetes Attitudes, Wishes, and Needs (DAWN) study. Diabetes Care, 28(11), 2673–2679. |
| [9] | Tan, A. M., Muthusamy, L., Ng, C. C., Phoon, K. Y., Ow, J. H., & Tan, N. C. (2011). Initiation of insulin for type 2 diabetes mellitus patients: What are the issues? A qualitative study. Singapore Medical Journal, 52(11), 801–809. |
| [10] | Woudenberg, Y. J. C., Lucas, C., Latour, C., & Scholte Op Reimer, W. J. M. (2012). Acceptance of insulin therapy: A long shot? Psychological insulin resistance in primary care. Diabetic Medicine, 29(6), 796–802. |
| [11] | Abu Hassan, H., Tohid, H., Mohd Amin, R., Long Bidin, M. B., Muthupalaniappen, L., & Omar, K. (2013). Factors influencing insulin acceptance among type 2 diabetes mellitus patients in a primary care clinic: A qualitative exploration. BMC Family Practice, 14. |
| [12] | Reach, G., Pechtner, V., Gentilella, R., Corcos, A., & Ceriello, A. (2017). Clinical inertia and its impact on treatment intensification in people with type 2 diabetes mellitus. Diabetes & Metabolism, 43(6), 501–511. Available from: |
| [13] | Ellis, K., Mulnier, H., & Forbes, A. (2018). Perceptions of insulin use in type 2 diabetes in primary care: A thematic synthesis. BMC Family Practice, 19(1), 1–21. |
| [14] | Lee, K. P. (2015). Psychosocial factors associated with psychological insulin resistance in primary care patients in Hong Kong. Journal of Clinical Translational Endocrinology, 2(4), 157–162. Available from: |
| [15] | Matthew, C. R., et al. (2020). Standards of Medical Care in Diabetes 2020 ADA. American Diabetes Association, 42(479), 960–1010. Available from: |
| [16] | Snoek, F. J., Skovlund, S. E., & Pouwer, F. (2007, December 20). Development and validation of the insulin treatment appraisal scale (ITAS) in patients with type 2 diabetes. Health and Quality of Life Outcomes. |
| [17] | Rita, S. L., Lubaki, F. J. P., Bompeka, L. F., Ogunbanjo, G. A., & Ngwala, L. P. (2019). Prevalence and determinants of psychological insulin resistance among type 2 diabetic patients in Kinshasa, Democratic Republic of Congo. African Journal of Primary Health Care & Family Medicine, 11(1), 1–5. |
| [18] | Fitzgerald, J. T., Funnell, M. M., Anderson, R. M., Nwankwo, R., Stansfield, R. B., & Piatt, G. A. (2016). Validation of the Revised Brief Diabetes Knowledge Test (DKT2). Diabetes Educator, 42(2), 178-187. |
| [19] | Feleke, S. A. (2013). Assessment of the Level and Associated Factors with Knowledge and Practice of Diabetes Mellitus among Diabetic Patients Attending at FelegeHiwot Hospital, Northwest Ethiopia. Clinical Medical Research, 2(6), 110. |
| [20] | Yilmaz, Ü. D., & Tarhan, S. (2017). Determination of attitude and knowledge of type 2 diabetic patients towards insulin therapy in northern Cyprus. Journal of Pakistan Medical Association, 67(3), 343–349. |
| [21] | Choudhury, S., Das, S., & Hazra, A. (2014). Survey of knowledge-attitude-practice concerning insulin use in adult diabetic patients in eastern India. Indian Journal of Pharmacology, 46, 425–429. |
| [22] | Lele, R. D. (2015). Psychological insulin resistance in patients with type 2 diabetes mellitus. Journal of Association of Physicians of India, 63(OCTOBER 2015), 94. |
| [23] | Nam, S., Nam, S., & Song, Y. (2015). Role of Self-Efficacy in the Relationship Between Patient-Provider Relationships and Psychological Insulin Resistance Among Patients with Type 2 Diabetes. Journal of Contemporary Diabetes Research, 1(1), 1–15. Available from: |
| [24] | Gulam, A. H., CF Otieno, F., & Oyoo, G. O. (2017). Prevalence of Psychological Insulin Resistance among Patients with Type 2 Diabetes at Kenyatta National Hospital, Kenya. Health Science Journal, 11. |
APA Style
Hailu, S. S., Ababiya, R. H., Nurfeta, R. A., Ababiya, T. H., Tema, L. A., et al. (2024). Knowledge and Attitude Towards Insulin Therapy in Type 2 Diabetes Mellitus Patients and Associated Factors at an Adult Endocrine Clinic of SPHMMC Addis Ababa Ethiopia. International Journal of Diabetes and Endocrinology, 9(2), 22-38. https://doi.org/10.11648/j.ijde.20240902.11
ACS Style
Hailu, S. S.; Ababiya, R. H.; Nurfeta, R. A.; Ababiya, T. H.; Tema, L. A., et al. Knowledge and Attitude Towards Insulin Therapy in Type 2 Diabetes Mellitus Patients and Associated Factors at an Adult Endocrine Clinic of SPHMMC Addis Ababa Ethiopia. Int. J. Diabetes Endocrinol. 2024, 9(2), 22-38. doi: 10.11648/j.ijde.20240902.11
AMA Style
Hailu SS, Ababiya RH, Nurfeta RA, Ababiya TH, Tema LA, et al. Knowledge and Attitude Towards Insulin Therapy in Type 2 Diabetes Mellitus Patients and Associated Factors at an Adult Endocrine Clinic of SPHMMC Addis Ababa Ethiopia. Int J Diabetes Endocrinol. 2024;9(2):22-38. doi: 10.11648/j.ijde.20240902.11
@article{10.11648/j.ijde.20240902.11,
author = {Selamawit Seifu Hailu and Robel Habtamu Ababiya and Rediet Ajebu Nurfeta and Tsion Habtamu Ababiya and Lijalem Abera Tema and Bemnet Gossaye Teka and Bezaye Lemma Deregasso and Dereje Kebede Shane and Hundaol Shiferaw Bekele and Saron Negasi Gidey},
title = {Knowledge and Attitude Towards Insulin Therapy in Type 2 Diabetes Mellitus Patients and Associated Factors at an Adult Endocrine Clinic of SPHMMC Addis Ababa Ethiopia
},
journal = {International Journal of Diabetes and Endocrinology},
volume = {9},
number = {2},
pages = {22-38},
doi = {10.11648/j.ijde.20240902.11},
url = {https://doi.org/10.11648/j.ijde.20240902.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijde.20240902.11},
abstract = {Background: Diabetes Mellitus (DM), a chronic disease characterized by elevated blood glucose levels, is associated with severe complications. Type 2 DM (T2DM), the most prevalent form of DM in adults, is characterized by varying degrees of insulin deficiency or resistance. The prevention or delay of macrovascular and microvascular problems associated with DM depends on achieving appropriate glycemic control. The percentage of T2DM patients failing to reach glycemic targets keeps rising even with the expanded availability of numerous anti-hyperglycemic drugs and evidence-based treatment guidelines. The delay in treatment intensification despite inadequate glucose control—often referred to as clinical or therapeutic inertia-contributes significantly to this trend. Objective: This study aims to evaluate the understanding and perceptions of insulin therapy among patients with T2DM. The study focuses on patients under follow-up care at the Adult Endocrine Clinic of St. Paul Hospital Millennium Medical College. Method and Material: An institutional-based, cross-sectional study was carried out from January to March 2021 to evaluate knowledge and attitudes regarding insulin therapy and related factors. A structured questionnaire was used for interviews with a representative sample of 271 T2DM patients who are receiving follow-up care at the endocrine clinic at SPHMMC. The SPSS, version 25, was the software utilized. The statistical significance of the relationship between the dependent and independent variables was assessed using a 95% confidence interval and a p-value less than 0.05. Results: The majority of the respondents were between the ages of 56 and 65, with a mean age of 57.35 years. More than half of the participants, accounting for 231 (85.2%) of the total, were from urban areas. Out of the 271 respondents, approximately 85.6% demonstrated poor knowledge of insulin therapy, and around 37.6% exhibited negative attitudes towards it. Factors such as age, occupation, and a history of long-term Oral Antidiabetic Drug use were found to be associated with the level of knowledge about insulin. In addition to these factors, marital status and a family history of insulin use were found to be associated with patients’ attitudes towards insulin. Conclusions: Our study identified a significant knowledge gap about insulin usage among T2DM patients in the designated study area. We recommend the implementation of regular, structured health education programs, delivered by trained health professionals. This approach is expected to enhance both the knowledge and attitudes toward insulin usage among patients attending follow-up sessions at the SPHMMC diabetic clinic.
},
year = {2024}
}
TY - JOUR T1 - Knowledge and Attitude Towards Insulin Therapy in Type 2 Diabetes Mellitus Patients and Associated Factors at an Adult Endocrine Clinic of SPHMMC Addis Ababa Ethiopia AU - Selamawit Seifu Hailu AU - Robel Habtamu Ababiya AU - Rediet Ajebu Nurfeta AU - Tsion Habtamu Ababiya AU - Lijalem Abera Tema AU - Bemnet Gossaye Teka AU - Bezaye Lemma Deregasso AU - Dereje Kebede Shane AU - Hundaol Shiferaw Bekele AU - Saron Negasi Gidey Y1 - 2024/04/28 PY - 2024 N1 - https://doi.org/10.11648/j.ijde.20240902.11 DO - 10.11648/j.ijde.20240902.11 T2 - International Journal of Diabetes and Endocrinology JF - International Journal of Diabetes and Endocrinology JO - International Journal of Diabetes and Endocrinology SP - 22 EP - 38 PB - Science Publishing Group SN - 2640-1371 UR - https://doi.org/10.11648/j.ijde.20240902.11 AB - Background: Diabetes Mellitus (DM), a chronic disease characterized by elevated blood glucose levels, is associated with severe complications. Type 2 DM (T2DM), the most prevalent form of DM in adults, is characterized by varying degrees of insulin deficiency or resistance. The prevention or delay of macrovascular and microvascular problems associated with DM depends on achieving appropriate glycemic control. The percentage of T2DM patients failing to reach glycemic targets keeps rising even with the expanded availability of numerous anti-hyperglycemic drugs and evidence-based treatment guidelines. The delay in treatment intensification despite inadequate glucose control—often referred to as clinical or therapeutic inertia-contributes significantly to this trend. Objective: This study aims to evaluate the understanding and perceptions of insulin therapy among patients with T2DM. The study focuses on patients under follow-up care at the Adult Endocrine Clinic of St. Paul Hospital Millennium Medical College. Method and Material: An institutional-based, cross-sectional study was carried out from January to March 2021 to evaluate knowledge and attitudes regarding insulin therapy and related factors. A structured questionnaire was used for interviews with a representative sample of 271 T2DM patients who are receiving follow-up care at the endocrine clinic at SPHMMC. The SPSS, version 25, was the software utilized. The statistical significance of the relationship between the dependent and independent variables was assessed using a 95% confidence interval and a p-value less than 0.05. Results: The majority of the respondents were between the ages of 56 and 65, with a mean age of 57.35 years. More than half of the participants, accounting for 231 (85.2%) of the total, were from urban areas. Out of the 271 respondents, approximately 85.6% demonstrated poor knowledge of insulin therapy, and around 37.6% exhibited negative attitudes towards it. Factors such as age, occupation, and a history of long-term Oral Antidiabetic Drug use were found to be associated with the level of knowledge about insulin. In addition to these factors, marital status and a family history of insulin use were found to be associated with patients’ attitudes towards insulin. Conclusions: Our study identified a significant knowledge gap about insulin usage among T2DM patients in the designated study area. We recommend the implementation of regular, structured health education programs, delivered by trained health professionals. This approach is expected to enhance both the knowledge and attitudes toward insulin usage among patients attending follow-up sessions at the SPHMMC diabetic clinic. VL - 9 IS - 2 ER -
Department of Internal Medicine, Wolaita Sodo University Comprehensive Specialized Hospital, Wolaita Sodo, Ethiopia
Department of Internal Medicine, Wolaita Sodo University Comprehensive Specialized Hospital, Wolaita Sodo, Ethiopia
Department of Internal Medicine, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
Department of Internal Medicine, Wolaita Sodo University Comprehensive Specialized Hospital, Wolaita Sodo, Ethiopia
Department of Internal Medicine, Wolaita Sodo University Comprehensive Specialized Hospital, Wolaita Sodo, Ethiopia
School of Medicine, Addis Ababa University, Addis Ababa, Ethiopia
Department of Internal Medicine, Hawassa University Referral Hospital, Hawassa, Ethiopia
Department of Internal Medicine, Wachemo University, Hadiya Hosanna, Ethiopia
Department of Internal Medicine, Madda Walabu University, Bale Robe, Ethiopia
School of Medicine, Mekelle University, Mekelle, Ethiopia
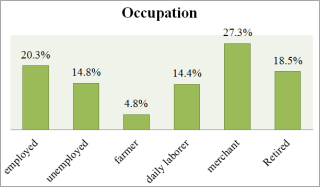
Figure 1. Occupation of the respondents.

Figure 2. Educational level of the respondents.
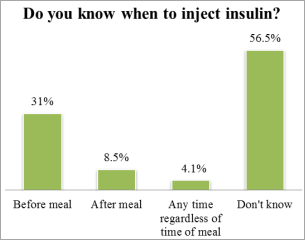
Figure 3. Knowledge of the respondents on what time to inject insulin.
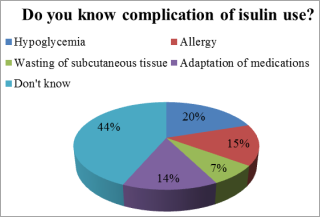
Figure 4. Knowledge of the respondents on complications of insulin use.

Figure 5. Risk factors for DM.
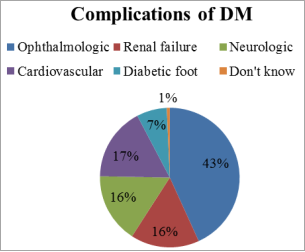
Figure 6. Complications of DM.
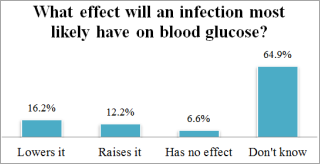
Figure 7. Effect of infection on blood glucose level.
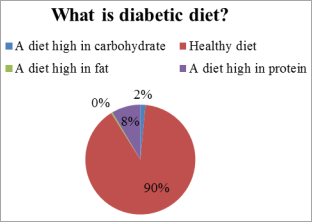
Figure 8. What a diabetic diet is.
Information

