Introduction: Endogenous Cushing's syndrome (CS) is a known cause of secondary osteoporosis, characterized by a loss of bone mass and density. Cushing's osteopathy is one of it’s most severe complications. Abnormal bone turnover, decreased bone mineral density (BMD), and increased fracture risk are common effects of glucocorticoid excess. Objectives: The aim of our work is to determine the bone densitometric profile of patients followed for Cushing's disease, to define the characteristics of osteoporosis and osteopenia in these patients, and to analyze the factors influencing BMD. Materials and methods: This is a retrospective descriptive study involving patients followed for Cushing's disease in the endocrinology-diabetology department of the public hospital establishment (EPH) of Bologhine-Algiers, during a period of 10 years, going from the January 2013 to January 2023. Results: 58 patients were followed during this period with an average age was 34 years, with a clear female predominance and a sex ratio of ≈ 4. Average Z score was (-1.6) at the vertebral level and (-1.09) at the femoral level. Osteoporosis was found in 44.8% (n = 26) patients and osteopenia in 37.9% (n = 22), while normal BMD was found in 17.24% (n = 10). Note that Z-score values were significantly lower at the lumbar spine than at the femoral neck. No significant difference in BMD was found between eumenorrheic and hypo-/amenorrheic females with Cushing's disease. Our study demonstrated a significant negative correlation between morning plasma cortisol and BMD. While there is a significant positive correlation between BMD and ACTH concentration in CD patients, BMD at the lumbar spine and femoral neck also had a significant positive correlation with weight and BMI. Conclusion: Early detection and management of CS are essential to reduce bone complications. BMD examinations should be performed to enable rapid recognition and intervention for osteoporosis. Lumbar bone loss occurs earlier and more extensively.
| Published in | International Journal of Diabetes and Endocrinology (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijde.20240901.12 |
| Page(s) | 13-21 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Bone Mineral Density, Cushing’s Disease, Fracture, Osteopenia, Osteoporosis
Mean ± SD | Percentage (%) | |
|---|---|---|
Sex (Female/male) | - | 79.3/20.6 |
Age (years) | 34 ±13.46 | |
BMI (kg/m2) | 31.06 ±5.48 | |
ACTH (pg/ml) | 93.7 ±71.05 | |
8 am serum cortisol (nmol/l) | 917.2 ±535.98 | |
midnight serum cortisol at (nmol/l) | 556.8 ±313.5 | |
24-h UFC (nmol/24H) | 1187 ±1294.7 | |
Serum Calcium (N: 81 -104) (mg/dl) | 91.4 ±10.75 | |
Phosphoremia (N: 40 -70) (mg/dl) | 33.7 ±9.71 | |
ALP (N: <275 IU/L) | 123.2 ±84.39 |
Clinical signs and comorbidities | Effective n=58 | Percentage (%) |
|---|---|---|
Facio-truncular obesity | 50 | 86.2 |
Large, purple stretch marks | 41 | 70.6 |
Easy bruising | 28 | 48.2 |
Proximal muscle wasting | 34 | 58 |
Stool sign | 25 | 43.1 |
Bone pain | 22 | 38.59 |
Psychiatric disorders | 61 | 10.9 |
Melanoderma | 18 | 62.2 |
Hirsutism | 28 | 17.24 |
HTA | 38 | 65.5 |
Diabetes | 33 | 56.8 |
Dyslipidemia | 24 | 41.3 |
Clinical signs | Osteoporotic patients n=26 Workforce (%) | Non-osteoporotic patients n=32 Workforce (%) | P-value |
|---|---|---|---|
Facio-truncular obesity | 22 (84.6) | 28 (87.5) | 0.25 |
Large, purple stretch marks | 16 (61.5) | 25 (78.1) | 0.28 |
Easy bruising | 13 (50) | 15 (46.8) | 0.25 |
Proximal muscle wasting | 18 (69.2) | 16 (50) | 0.25 |
Stool sign | 11 (42.3) | 14 (43.7) | 0.25 |
Bone pain | 13 (50) | 09 (28.1) | 0.31 |
Melanoderma | 11 (42.3) | 07 (21.8) | 0.37 |
Hirsutism | 06 (23) | 22 (68.7) | 0.22 |
Mean ±SD | 95% CI for mean | |
|---|---|---|
Lumbar Spine T-score | -1.88 ±1.32 | (-2.22 to -1.54) |
Lumbar spine Z-score | -1.60 ±1.27 | (-1.92 to -1.28) |
Femoral neck T-score | -1.25 ±1.16 | (-1.55 to -0.95) |
Femoral neck Z-score | -1.09 ±1.18 | (-1.39 to -0.79) |
| [1] | H. Boro et al., “Trabecular bone score and bone mineral density as indices of skeletal fragility in endogenous Cushing’s syndrome,” Clin Endocrinol, 2023, |
| [2] | E. J. Ross and D. C. Linch, “Cushing’s syndrome—killing disease: discriminatory value of signs and symptoms aiding early diagnosis,” Lancet, vol. 320, no. 8299, pp. 646–649, 1982. |
| [3] | F. Manelli and A. Giustina, “Glucocorticoid-induced osteoporosis,” Trends Endocrinol. Metab., vol. 11, no. 3, pp. 79–85, 2000. |
| [4] | P. Vestergaard et al., “Increased risk of osteoporotic fractures in patients with Cushing’s syndrome,” Eur. J. Endocrinol., vol. 146, no. 1, pp. 51–56, 2002. |
| [5] | A. Tabarin et al., “Consensus statement by the French Society of Endocrinology (SFE) and French Society of Pediatric Endocrinology & Diabetology (SFEDP) on diagnosis of Cushing’s syndrome,” in Annales d’endocrinologie, Elsevier, 2022, pp. 119–141. |
| [6] | P. Zysset et al., “Clinical use of quantitative computed tomography–based finite element analysis of the hip and spine in the management of osteoporosis in adults: the 2015 ISCD official positions—part II,” J. Clin. Densitom., vol. 18, no. 3, pp. 359–392, 2015. |
| [7] | H. P. Dimai, “Use of dual-energy X-ray absorptiometry (DXA) for diagnosis and fracture risk assessment; WHO-criteria, T-and Z-score, and reference databases,” Bone, vol. 104, pp. 39–43, 2017. |
| [8] | A. of F. R. and I. A. to S. for P. Osteoporosis, “Report of a WHO study group,” World Heal. Organ Tech Rep Ser, vol. 843, pp. 1–129, 1994. |
| [9] | W. Guo et al., “Effect of hypercortisolism on bone mineral density and bone metabolism: A potential protective effect of adrenocorticotropic hormone in patients with Cushing’s disease,” J Int Med Res, vol. 46, no. 1, pp. 492–503, 2018, |
| [10] | den H. M. van der Eerden AW Oyen WJ, Hermus AR, “Cushing’s syndrome and bone mineral density: lowest Z scores in young patients”. |
| [11] | Tats. I. NARIKO OHMORI, KAORU NOMURA, KAZUE OHMORI, YOSHIHARU KATO* and E. K. TAKANO, “OSTEOPORISIS IS MORE PREVALENT IN ADRENAL THAN IN PITUITARY CUSHING’S SYNDROME.” 2003. |
| [12] | R. Naguib, E. Z. Elkemary, and K. M. Elsharkawi, “The severity of bone loss: a comparison between Cushing’s disease and Cushing’s syndrome,” J. Endocrinol. Metab., vol. 13, no. 1, pp. 33–38, 2023. |
| [13] | D. Chappard et al., “Altered trabecular architecture induced by corticosteroids: a bone histomorphometric study,” J. bone Miner. Res., vol. 11, no. 5, pp. 676–685, 1996. |
| [14] | M. S. Calvo, D. R. Eyre, and C. M. Gundberg, “Molecular basis and clinical application of biological markers of bone turnover,” Endocr. Rev., vol. 17, no. 4, pp. 333–368, 1996. |
| [15] | Filippo Manelli and Andrea Giustina, “Glucocorticoid-inducted osteoporosis,” 2000. |
| [16] | C. M. Francucci, P. Pantanetti, G. G. Garrapa, F. Massi, G. Arnaldi, and F. Mantero, “Bone metabolism and mass in women with Cushing’s syndrome and adrenal incidentaloma,” Clin. Endocrinol. (Oxf)., vol. 57, no. 5, pp. 587–593, 2002. |
| [17] | A. Kawamata, M. Iihara, T. Okamoto, and T. Obara, “Bone Mineral Density Before and After Surgical Cure of Cushing’s Syndrome Due to Adrenocortical Adenoma: Prospective Study,” World J. Surg., vol. 32, no. 5, pp. 890–896, 2008, |
| [18] | S. H. Rahaman and P. Viveka, “Bone Health in Patients with Cushing’s Syndrome,” pp. 766–769, 2018, |
| [19] | C. A. O’Brien et al., “Glucocorticoids act directly on osteoblasts and osteocytes to induce their apoptosis and reduce bone formation and strength,” Endocrinology, vol. 145, no. 4, pp. 1835–1841, 2004, |
| [20] | E. Canalis, G. Mazziotti, A. Giustina, and J. P. Bilezikian, “Glucocorticoid-induced osteoporosis: pathophysiology and therapy,” Osteoporos. Int., vol. 18, no. 10, pp. 1319–1328, 2007. |
| [21] | Z. Wu, N. L. R. Bucher, and S. R. Farmer, “Induction of peroxisome proliferator-activated receptor γ during the conversion of 3T3 fibroblasts into adipocytes is mediated by C/EBPβ, C/EBPδ, and glucocorticoids,” Mol. Cell. Biol., vol. 16, no. 8, pp. 4128–4136, 1996. |
| [22] | N. E. Lane et al., “Glucocorticoid-treated mice have localized changes in trabecular bone material properties and osteocyte lacunar size that are not observed in placebo-treated or estrogen-deficient mice,” J. bone Miner. Res., vol. 21, no. 3, pp. 466–476, 2006. |
| [23] | R. S. Weinstein, “Glucocorticoid-induced bone disease,” N. Engl. J. Med., vol. 365, no. 1, pp. 62–70, 2011. |
| [24] | S. L. Teitelbaum, “Bone resorption by osteoclasts,” Science (80-.)., vol. 289, no. 5484, pp. 1504–1508, 2000. |
| [25] | D. Jia, C. A. O’brien, S. A. Stewart, S. C. Manolagas, and R. S. Weinstein, “Glucocorticoids act directly on osteoclasts to increase their life span and reduce bone density,” Endocrinology, vol. 147, no. 12, pp. 5592–5599, 2006. |
| [26] | T. P. Van Staa, R. F. Laan, I. P. Barton, S. Cohen, D. M. Reid, and C. Cooper, “Bone density threshold and other predictors of vertebral fracture in patients receiving oral glucocorticoid therapy,” Arthritis Rheum., vol. 48, no. 11, pp. 3224–3229, 2003. |
| [27] | M. Tóth and A. Grossman, “Glucocorticoid-induced osteoporosis: lessons from Cushing’s syndrome,” Clin. Endocrinol. (Oxf)., vol. 79, no. 1, pp. 1–11, 2013, |
| [28] | H. J. Lee, J. H. Je, J. H. Seo, Y. J. Na, and H. J. Yoo, “Mutiple spontaneous rib fractures in patient with Cushing’s syndrome,” J. bone Metab., vol. 21, no. 4, pp. 277–282, 2014. |
| [29] | G. Papadakis, B. Uebelhart, M. Goumaz, S. Zawadynski, and R. Rizzoli, “An unusual case of hypercortisolism with multiple weight-bearing bone fractures,” Clin. cases Miner. bone Metab., vol. 10, no. 3, p. 213, 2013. |
| [30] | B. Stachowska, J. Halupczok-Żyła, J. Kuliczkowska-Płaksej, J. Syrycka, and M. Bolanowski, “Decreased trabecular bone score in patients with active endogenous Cushing’s syndrome,” Front. Endocrinol. (Lausanne)., vol. 11, p. 593173, 2021. |
| [31] | E. Seeman and P. D. Delmas, “Bone quality—the material and structural basis of bone strength and fragility,” N. Engl. J. Med., vol. 354, no. 21, pp. 2250–2261, 2006. |
| [32] | C. De Laet et al., “Body mass index as a predictor of fracture risk: a meta-analysis,” Osteoporos. Int., vol. 16, pp. 1330–1338, |
| [33] | L. Tauchmanova et al., “Effects of sex steroids on bone in women with subclinical or overt endogenous hypercortisolism,” Eur. J. Endocrinol., vol. 157, no. 3, pp. 359–366, 2007. |
| [34] | M. Rousière, “De l’importance de prendre en charge l’ostéoporose,” Presse Med., vol. 40, no. 10, pp. 900–909, 2011. |
APA Style
Debbah, W., Mezoued, M., Bouzid, A., Talhi, R., Bessaid, K., et al. (2024). The Severity of Bone Loss in Cushing’s Diseases. International Journal of Diabetes and Endocrinology, 9(1), 13-21. https://doi.org/10.11648/j.ijde.20240901.12
ACS Style
Debbah, W.; Mezoued, M.; Bouzid, A.; Talhi, R.; Bessaid, K., et al. The Severity of Bone Loss in Cushing’s Diseases. Int. J. Diabetes Endocrinol. 2024, 9(1), 13-21. doi: 10.11648/j.ijde.20240901.12
AMA Style
Debbah W, Mezoued M, Bouzid A, Talhi R, Bessaid K, et al. The Severity of Bone Loss in Cushing’s Diseases. Int J Diabetes Endocrinol. 2024;9(1):13-21. doi: 10.11648/j.ijde.20240901.12
@article{10.11648/j.ijde.20240901.12,
author = {Wissame Debbah and Mouna Mezoued and Aicha Bouzid and Randa Talhi and Khadidja Bessaid and Malha Azzouz},
title = {The Severity of Bone Loss in Cushing’s Diseases
},
journal = {International Journal of Diabetes and Endocrinology},
volume = {9},
number = {1},
pages = {13-21},
doi = {10.11648/j.ijde.20240901.12},
url = {https://doi.org/10.11648/j.ijde.20240901.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijde.20240901.12},
abstract = {Introduction: Endogenous Cushing's syndrome (CS) is a known cause of secondary osteoporosis, characterized by a loss of bone mass and density. Cushing's osteopathy is one of it’s most severe complications. Abnormal bone turnover, decreased bone mineral density (BMD), and increased fracture risk are common effects of glucocorticoid excess. Objectives: The aim of our work is to determine the bone densitometric profile of patients followed for Cushing's disease, to define the characteristics of osteoporosis and osteopenia in these patients, and to analyze the factors influencing BMD. Materials and methods: This is a retrospective descriptive study involving patients followed for Cushing's disease in the endocrinology-diabetology department of the public hospital establishment (EPH) of Bologhine-Algiers, during a period of 10 years, going from the January 2013 to January 2023. Results: 58 patients were followed during this period with an average age was 34 years, with a clear female predominance and a sex ratio of ≈ 4. Average Z score was (-1.6) at the vertebral level and (-1.09) at the femoral level. Osteoporosis was found in 44.8% (n = 26) patients and osteopenia in 37.9% (n = 22), while normal BMD was found in 17.24% (n = 10). Note that Z-score values were significantly lower at the lumbar spine than at the femoral neck. No significant difference in BMD was found between eumenorrheic and hypo-/amenorrheic females with Cushing's disease. Our study demonstrated a significant negative correlation between morning plasma cortisol and BMD. While there is a significant positive correlation between BMD and ACTH concentration in CD patients, BMD at the lumbar spine and femoral neck also had a significant positive correlation with weight and BMI. Conclusion: Early detection and management of CS are essential to reduce bone complications. BMD examinations should be performed to enable rapid recognition and intervention for osteoporosis. Lumbar bone loss occurs earlier and more extensively.
},
year = {2024}
}
TY - JOUR T1 - The Severity of Bone Loss in Cushing’s Diseases AU - Wissame Debbah AU - Mouna Mezoued AU - Aicha Bouzid AU - Randa Talhi AU - Khadidja Bessaid AU - Malha Azzouz Y1 - 2024/04/02 PY - 2024 N1 - https://doi.org/10.11648/j.ijde.20240901.12 DO - 10.11648/j.ijde.20240901.12 T2 - International Journal of Diabetes and Endocrinology JF - International Journal of Diabetes and Endocrinology JO - International Journal of Diabetes and Endocrinology SP - 13 EP - 21 PB - Science Publishing Group SN - 2640-1371 UR - https://doi.org/10.11648/j.ijde.20240901.12 AB - Introduction: Endogenous Cushing's syndrome (CS) is a known cause of secondary osteoporosis, characterized by a loss of bone mass and density. Cushing's osteopathy is one of it’s most severe complications. Abnormal bone turnover, decreased bone mineral density (BMD), and increased fracture risk are common effects of glucocorticoid excess. Objectives: The aim of our work is to determine the bone densitometric profile of patients followed for Cushing's disease, to define the characteristics of osteoporosis and osteopenia in these patients, and to analyze the factors influencing BMD. Materials and methods: This is a retrospective descriptive study involving patients followed for Cushing's disease in the endocrinology-diabetology department of the public hospital establishment (EPH) of Bologhine-Algiers, during a period of 10 years, going from the January 2013 to January 2023. Results: 58 patients were followed during this period with an average age was 34 years, with a clear female predominance and a sex ratio of ≈ 4. Average Z score was (-1.6) at the vertebral level and (-1.09) at the femoral level. Osteoporosis was found in 44.8% (n = 26) patients and osteopenia in 37.9% (n = 22), while normal BMD was found in 17.24% (n = 10). Note that Z-score values were significantly lower at the lumbar spine than at the femoral neck. No significant difference in BMD was found between eumenorrheic and hypo-/amenorrheic females with Cushing's disease. Our study demonstrated a significant negative correlation between morning plasma cortisol and BMD. While there is a significant positive correlation between BMD and ACTH concentration in CD patients, BMD at the lumbar spine and femoral neck also had a significant positive correlation with weight and BMI. Conclusion: Early detection and management of CS are essential to reduce bone complications. BMD examinations should be performed to enable rapid recognition and intervention for osteoporosis. Lumbar bone loss occurs earlier and more extensively. VL - 9 IS - 1 ER -
Department of Endocrinology and Metabolism, Benyoucef Benkhedda University, Algiers, Algeria
Department of Endocrinology and Metabolism, Benyoucef Benkhedda University, Algiers, Algeria; Research Laboratory of Endocrinolgy and Métabolism (LEM 1), Algiers University, Algiers, Algeria
Department of Endocrinology and Metabolism, Benyoucef Benkhedda University, Algiers, Algeria; Research Laboratory of Endocrinolgy and Métabolism (LEM 1), Algiers University, Algiers, Algeria
Department of Epidemiology, Benyoucef Benkhedda University, Algiers, Algeria
Department of Endocrinology and Metabolism, Benyoucef Benkhedda University, Algiers, Algeria; Research Laboratory of Endocrinolgy and Métabolism (LEM 1), Algiers University, Algiers, Algeria
Department of Endocrinology and Metabolism, Benyoucef Benkhedda University, Algiers, Algeria; Research Laboratory of Endocrinolgy and Métabolism (LEM 1), Algiers University, Algiers, Algeria
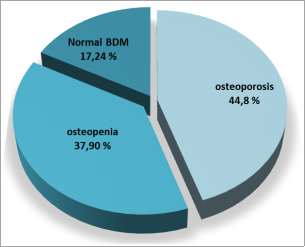
Figure 1. Distribution of bone damage in our cohort.
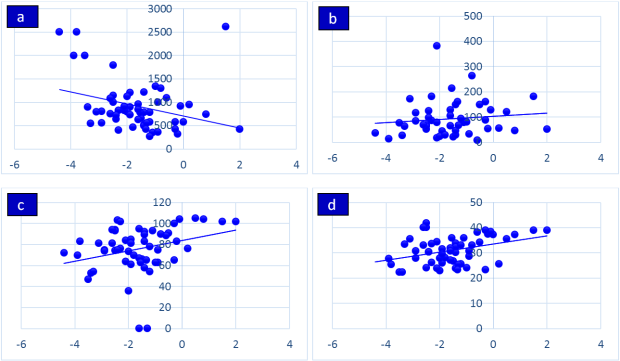
Figure 2. Correlation of lumbar BMD and morning serum cortisol (a), adrenocorticotropic hormone (ACTH) (b), weight (c), BMI (d).
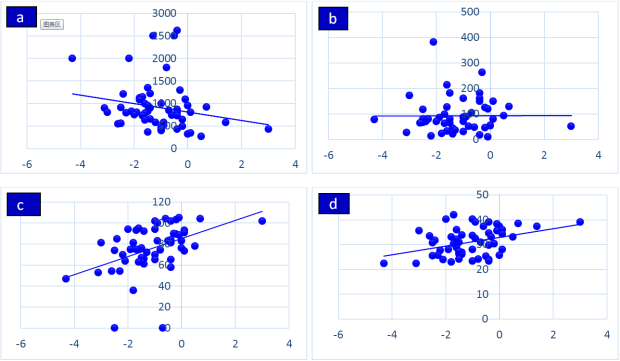
Figure 3. Correlation of hip BMD and morning serum cortisol (a), adrenocorticotropic hormone (ACTH) (b), weight (c), BMI (d).
Information

