A 48 year dark skinned North Indian male presented first time to our outpatient with history of bilateral visual decline of 3 weeks duration with associated features of headache, myalgia and rhinitus of 4 weeks duration. A detailed examination confirmed bilateral active anterior granulomatous uveitis with bilateral disc oedema with serous retinal detachment. Multimodal imaging examination was carried out with nideks mirante. Diagnosis in favour of vogt koyanagi harada disease was confirmed. The posterior segment was assessed for various changes in acute and remission phase of vogt koyanagi harada disease with fundus fluorescein angiography, fundus autoflourescence, retroillumination and optical coherence tomography. Thickness and structural change related to central macula thickness, retinal pigment epithelium and choroid were assessed pre and post treatment with additional support of optical coherence tomography and retroillumination. Both these techniques were able to document a greater value change pre and post treatment in these structures. Hence we conclude the need to include these techniques in retinal pigment epithelium and choroidal assessment in vogt koyanagi harada disease.
| Published in | International Journal of Ophthalmology & Visual Science (Volume 9, Issue 2) |
| DOI | 10.11648/j.ijovs.20240902.12 |
| Page(s) | 23-29 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Imaging, VKHD, RPE, Choroid
Subfoveal Choroidal Thickness | ||
|---|---|---|
Right Eye | Left Eye | |
At Presentation | 593 microns | 486 microns |
After Therapy | 430 microns | 410 microns |
Right Eye | Left Eye | |
|---|---|---|
Horizontal Diameter | 1382 microns | 1504 microns |
Vertical Diameter | 1461 microns | 1636 microns |
Right Eye | Left Eye | |
|---|---|---|
At Presentation | 42.906 mm2 | 55.443 mm2 |
After Therapy | 14.661 mm2 | 19.931 mm2 |
VKHD | Vogt Koyanagi Harada Disease |
FAF | Fundus Auto-Flourescence |
OCT | Optical Coherence Tomography |
MMF | Mycophenolate Mofetil |
RPE | Retinal Pigment Epithelium |
BLD | Bacillary Layer Detachment |
HROL | Hyper-Reflective Outer Nuclear Layer |
| [1] | Moorthy RS, Inomata H, Rao NA. Vogt–Koyanagi–Harada syndrome. Surv Ophthalmol 1995; 39: 265–92. |
| [2] | Shimizu K. Harada’s, Behçet’s, Vogt–Koyanagi syndromes: are they clinical entities? Trans Am Acad Ophthalmol Otolaryngol 1973; 77: 281–90. |
| [3] | Forster DJ, Green RL, Rao NA. Unilateral manifestation of the Vogt–Koyanagi–Harada syndrome in a 7-year-old child. Am J Ophthalmol 1991; 111: 380–2. |
| [4] | Sugita S, Takase H, Imai Y, et al. Immunopathogenic mechanism of melanocyte-specific autoimmune disease: a cross reaction between tyrosinase peptides and cytomegalovirus antigen. Invest OphthalmolVis Sci. 2002: 43: 1529. |
| [5] | Jacob N, Tyagi M, Chhablani J, Narayanan R, Kelgaonkar A, Jain M, Singh SR et al. Retinal Pigment Epithelial Characteristics in Acute and Resolved Vogt-Koyanagi-Harada Disease. J Clin Med 2023, 12(6), 2638; |
| [6] |
O'Keefe GA, Rao NA. Vogt-Koyanagi-Harada disease. Surv Ophthalmol. 2017 Jan-Feb; 62(1): 1-25.
https://doi.org/10.1016/j.survophthal.2016.05.002 Epub 2016 May 27. PMID: 27241814. |
| [7] |
Maruko I, Iida T, Sugano Y, Oyamada H, Sekiryu T, Fujiwara T, Spaide RF. Subfoveal choroidal thickness after treatment of Vogt-Koyanagi-Harada disease. Retina. 2011 Mar; 31(3): 510-7.
https://doi.org/10.1097/IAE.0b013e3181eef053 PMID: 20948460. |
| [8] |
Nakai K, Gomi F, Ikuno Y, Yasuno Y, Nouchi T, Ohguro N, Nishida K. Choroidal observations in Vogt-Koyanagi-Harada disease using high-penetration optical coherence tomography. Graefes Arch Clin Exp Ophthalmol. 2012 Jul; 250(7): 1089-95.
https://doi.org/10.1007/s00417-011-1910-7 Epub 2012 Jan 13. PMID: 22240936. |
| [9] |
Hirooka K, Saito W, Namba K, Mizuuchi K, Iwata D, Hashimoto Y, Ishida S. Significant role of the choroidal outer layer during recovery from choroidal thickening in Vogt-Koyanagi-Harada disease patients treated with systemic corticosteroids. BMC Ophthalmol. 2015 Dec 18; 15: 181.
https://doi.org/10.1186/s12886-015-0171-3 PMID: 26677974; PMCID: PMC4683749. |
| [10] | Spraul CW, Lang GE, Lang GK, Grossniklaus HE. Morphometric changes of the choriocapillaris and the choroidal vasculature in eyes with advanced glaucomatous changes. Vision Res. 2002; 42: 923–32. |
| [11] |
Hirota Y, Muraoka Y, Kogo T, Ishikura M, Kadomoto S, Nishigori N, Ishihara K, Morooka S, Uji A, Tsujikawa A. Association of Retinal Pigment Epithelium Reflectivity on Optical Coherence Tomography with Recurrence of Vogt-Koyanagi-Harada Disease: A Retrospective Observational Study. Clin Ophthalmol. 2023 Jul 21; 17: 2071-2079.
https://doi.org/10.2147/OPTH.S419546 PMID: 37496848; PMCID: PMC10368137. |
| [12] |
Inomata H, Rao NA. Depigmented atrophic lesions in sunset glow fundi of Vogt-Koyanagi-Harada disease. Am J Ophthalmol. 2001 May; 131(5): 607-14.
https://doi.org/10.1016/s0002-9394(00)00851-5 PMID: 11336935. |
| [13] |
Rao NA. Pathology of Vogt-Koyanagi-Harada disease. Int Ophthalmol. 2007 Apr-Jun; 27(2-3): 81-5.
https://doi.org/10.1007/s10792-006-9029-2 Epub 2007 Apr 14. PMID: 17435969. |
| [14] |
Miura M, Makita S, Azuma S, Yasuno Y, Sugiyama S, Mino T, Yamaguchi T, Agawa T, Iwasaki T, Usui Y, Rao NA, Goto H. Evaluation of Retinal Pigment Epithelium Layer Change in Vogt-Koyanagi-Harada Disease With Multicontrast Optical Coherence Tomography. Invest Ophthalmol Vis Sci. 2019 Aug 1; 60(10): 3352-3362.
https://doi.org/10.1167/iovs.19-27378 PMID: 31917451. |
| [15] |
Huang Y, Yang YT, Lin B, Huang SH, Sun ZH, Zhou R, Li YZ, Liu XL. Melanin change of retinal pigment epithelium and choroid in the convalescent stage of Vogt-Koyanagi-Harada disease. Int J Ophthalmol. 2020 Dec 18; 13(12): 1928-1932.
https://doi.org/10.18240/ijo.2020.12.13 PMID: 33344192; PMCID: PMC7708368. |
| [16] |
Hashizume K, Imamura Y, Fujiwara T, Machida S, Ishida M, Kurosaka D. RETINAL PIGMENT EPITHELIUM UNDULATIONS IN ACUTE STAGE OF VOGT- KOYANAGI-HARADA DISEASE: Biomarker for Functional Outcomes After High-Dose Steroid Therapy. Retina. 2016 Feb; 36(2): 415-21.
https://doi.org/10.1097/IAE.0000000000000728 PMID: 26352553. |
| [17] |
Fonollosa A, Charcán I, Giralt L, Artaraz J, Soto A, Ruiz-Arruza I, Agarwal A. Hyper-Reflective Outer Nuclear Layer (HONL) in Vogt-Koyanagi-Harada Disease and Sympathetic Ophthalmia. Ocul Immunol Inflamm. 2022 Nov 4: 1-5.
https://doi.org/10.1080/09273948.2022.2134038 Epub ahead of print. PMID: 36332138. |
| [18] |
Agarwal A, Freund KB, Kumar A, Aggarwal K, Sharma D, Katoch D, Bansal R, Gupta V; OCTA Study Group. BACILLARY LAYER DETACHMENT IN ACUTE VOGT-KOYANAGI-HARADA DISEASE: A Novel Swept-Source Optical Coherence Tomography Analysis. Retina. 2021 Apr 1; 41(4): 774-783.
https://doi.org/10.1097/IAE.0000000000002914 PMID: 32833410. |
| [19] |
Atas F, Kaya M, Saatci AO. The effect of pulse steroid treatment of ten days' long on the improvement of bacillary layer detachment in a patient with Vogt-Koyanagi Harada disease. Rom J Ophthalmol. 2021 Apr-Jun; 65(2): 183-186.
https://doi.org/10.22336/rjo.2021.36 PMID: 34179585; PMCID: PMC8207875. |
| [20] |
Kwak JJ, Lee J, Byeon SH. Clinical Features and Prognostic Value of Bacillary Layer Detachment in Acute Vogt-Koyanagi-Harada Disease. Retina. 2023 Jun 8.
https://doi.org/10.1097/IAE.0000000000003858 Epub ahead of print. PMID: 37315551. |
APA Style
Arora, D., Sharma, A., Sharma, D., Sharma, D. (2024). Multimodal Imaging in Diagnosis of Vogt Koyanagi Harada Disease with Reference to Choroid and Retinal Pigment Epithelium. International Journal of Ophthalmology & Visual Science, 9(2), 23-29. https://doi.org/10.11648/j.ijovs.20240902.12
ACS Style
Arora, D.; Sharma, A.; Sharma, D.; Sharma, D. Multimodal Imaging in Diagnosis of Vogt Koyanagi Harada Disease with Reference to Choroid and Retinal Pigment Epithelium. Int. J. Ophthalmol. Vis. Sci. 2024, 9(2), 23-29. doi: 10.11648/j.ijovs.20240902.12
AMA Style
Arora D, Sharma A, Sharma D, Sharma D. Multimodal Imaging in Diagnosis of Vogt Koyanagi Harada Disease with Reference to Choroid and Retinal Pigment Epithelium. Int J Ophthalmol Vis Sci. 2024;9(2):23-29. doi: 10.11648/j.ijovs.20240902.12
@article{10.11648/j.ijovs.20240902.12,
author = {Deepesh Arora and Anuj Sharma and Devesh Sharma and Dinesh Sharma},
title = {Multimodal Imaging in Diagnosis of Vogt Koyanagi Harada Disease with Reference to Choroid and Retinal Pigment Epithelium
},
journal = {International Journal of Ophthalmology & Visual Science},
volume = {9},
number = {2},
pages = {23-29},
doi = {10.11648/j.ijovs.20240902.12},
url = {https://doi.org/10.11648/j.ijovs.20240902.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijovs.20240902.12},
abstract = {A 48 year dark skinned North Indian male presented first time to our outpatient with history of bilateral visual decline of 3 weeks duration with associated features of headache, myalgia and rhinitus of 4 weeks duration. A detailed examination confirmed bilateral active anterior granulomatous uveitis with bilateral disc oedema with serous retinal detachment. Multimodal imaging examination was carried out with nideks mirante. Diagnosis in favour of vogt koyanagi harada disease was confirmed. The posterior segment was assessed for various changes in acute and remission phase of vogt koyanagi harada disease with fundus fluorescein angiography, fundus autoflourescence, retroillumination and optical coherence tomography. Thickness and structural change related to central macula thickness, retinal pigment epithelium and choroid were assessed pre and post treatment with additional support of optical coherence tomography and retroillumination. Both these techniques were able to document a greater value change pre and post treatment in these structures. Hence we conclude the need to include these techniques in retinal pigment epithelium and choroidal assessment in vogt koyanagi harada disease.
},
year = {2024}
}
TY - JOUR T1 - Multimodal Imaging in Diagnosis of Vogt Koyanagi Harada Disease with Reference to Choroid and Retinal Pigment Epithelium AU - Deepesh Arora AU - Anuj Sharma AU - Devesh Sharma AU - Dinesh Sharma Y1 - 2024/05/30 PY - 2024 N1 - https://doi.org/10.11648/j.ijovs.20240902.12 DO - 10.11648/j.ijovs.20240902.12 T2 - International Journal of Ophthalmology & Visual Science JF - International Journal of Ophthalmology & Visual Science JO - International Journal of Ophthalmology & Visual Science SP - 23 EP - 29 PB - Science Publishing Group SN - 2637-3858 UR - https://doi.org/10.11648/j.ijovs.20240902.12 AB - A 48 year dark skinned North Indian male presented first time to our outpatient with history of bilateral visual decline of 3 weeks duration with associated features of headache, myalgia and rhinitus of 4 weeks duration. A detailed examination confirmed bilateral active anterior granulomatous uveitis with bilateral disc oedema with serous retinal detachment. Multimodal imaging examination was carried out with nideks mirante. Diagnosis in favour of vogt koyanagi harada disease was confirmed. The posterior segment was assessed for various changes in acute and remission phase of vogt koyanagi harada disease with fundus fluorescein angiography, fundus autoflourescence, retroillumination and optical coherence tomography. Thickness and structural change related to central macula thickness, retinal pigment epithelium and choroid were assessed pre and post treatment with additional support of optical coherence tomography and retroillumination. Both these techniques were able to document a greater value change pre and post treatment in these structures. Hence we conclude the need to include these techniques in retinal pigment epithelium and choroidal assessment in vogt koyanagi harada disease. VL - 9 IS - 2 ER -
Amritsar Eye Clinic, Dehradun, India
Amritsar Eye Clinic, Dehradun, India
Amritsar Eye Clinic, Dehradun, India
Amritsar Eye Clinic, Dehradun, India
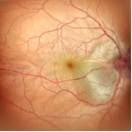
Figure 1. Fundus OD shows disc swelling, serous retinal detachment at posterior pole with presence of retinal folds extending from disc to macula.
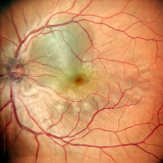
Figure 2. Fundus OS shows disc odema with multiple pockest of serous retinal detachment involving macula.
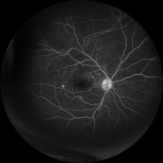
Figure 3. Fundus fluorescein angiography OD revealed disc leakage with blurred optic disc margin, multifocal pin point leaks seen at juxtapapillary and posterior pole.
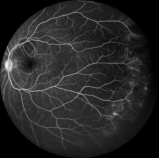
Figure 4. FFA OS periphery shows active leaks from multiple terminal vessels extending to ora.
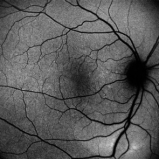
Figure 5. Fundus auto-flourescence (FAF) OD distinctively revealed hyper auto-fluorescence at posterior pole highlighting RPE (Retinal pigment epithelium) involvement.
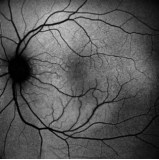
Figure 6. Fundus auto-flourescence (FAF) OS revealed hyper auto-fluorescence at posterior pole confirming retinal pigment epithelium involvement.
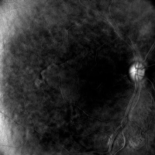
Figure 7. Retroillumination image of acute VKHD OD shows disc florescence and a large posterior pole leaf pattern area of hypoflourescence suggesting RPE involvement with patchy hyperflourescent areas of unaffected RPE surrounding it.
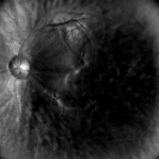
Figure 8. Retroillumination image of OS with acute VKHD showing detailed disc flourescence with large well demarcated posterior pole hypoflourescent area of RPE involvement surrounded by normal hyperflourescent pigment epithelium.
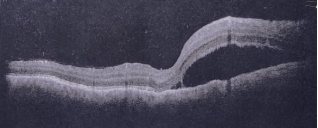
Figure 9. OCT – Macula OD shows intra-retinal odema, neurosensory detachment (NSD), bacillary layer detachment, subretinal hyperreflective dots, choroidal hyperreflective dots and retinal pigment epithelium vacuolation.
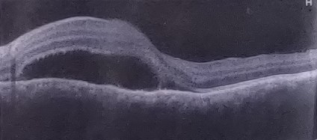
Figure 10. OCT –Macula OS shows bacillary layer detachment, subretinal and choroidal hyperreflective dots more prominent in this eye.

Figure 11. Fundus photo OD 3 weeks into post treatment shows hyperemic disc and radial foveal folds with a large area of RPE at posterior pole involved in acute VKH disease.
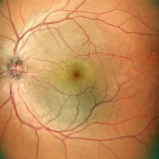
Figure 12. Fundus photo OS 3 weeks into post treatment shows a hyperemic disc with radial folds and a well demarcated area of RPE previously involved in acute VKHD seen at posterior pole.
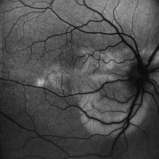
Figure 13. FAF photo OD shows a large leaf like area of hypoflourescence depicting RPE involvement seen at posterior pole.
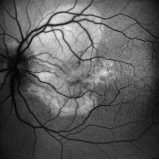
Figure 14. FAF image OS shows a large posterior pole hypoflourescent area extending outside of superior arcade and involving fovea correlating to poor visual recovery.
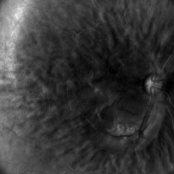
Figure 15. Retroillumination image OD shows hyperflourescent posterior pole intersperced with recovering hypoflourescent areas seen adjacent to inferior arcade.
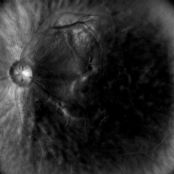
Figure 16. Retroillumination image OS during 3 week recovery phase shows large RPE defect as hypoflourescent patch at posterior pole.
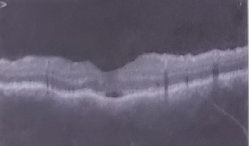
Figure 17. OCT- Macula VKHD early post recovery with presence of subretinal fluid, reduced presence of subretinal and choroidal hyperreflective dots with altered RPE reflectivity.
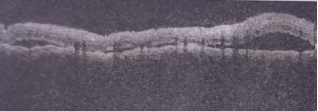
Figure 18. OCT-Macula OS reveals irregular inner and outer retinal layers with loss of architecture, presence of subretinal fluid, persistence of choroidal hyperreflective dots.
Information

