Abstract
Purpose: To describe the incidence and characteristics of negative dysphotopsia (ND) as well as the risk factors contributing to it. Methods: For this retrospective study, data from patients who underwent cataract surgery between January 2018 and December 2019 at our department (Department of Ophthalmology, Hietzing Hospital, Vienna, Austria) was analyzed. A total of 8122 eyes had cataract surgery performed. Three different intraocular lenses (IOLs) have been used (EyeCee® One by Bausch + Lomb, TECNIS® by Johnson & Johnson, HOYA Vivienx ™ by HOYA). Data from patients who postoperatively complained about ND as well as data from a gender and age-matched control group (34 eyes in each) was further analyzed: pupil size, axial length, anterior chamber depth, angle kappa, IOL power and other biometrical factors. The scotomas were depicted on a Harms tangent screen. Results: An incidence of 1.99% of ND was found, of which 1.58% was transient and 0.42% persistent. The average duration of the symptoms was 5.40 (±6.15) weeks in the transient ND group. In the total cohort of 8122 eyes, there was no difference in the distribution of implanted IOL types or IOL power; neither played the surgeon a significant role in the development of ND. There was no significant difference between ND and control eyes regarding pupil size, axial length, and angle kappa. The anterior chamber was significantly shallower in the ND group: 5.1±0.58mm vs. 5.41±0.61mm (p=0.03). Conclusion: According to our findings, a shallower anterior chamber poses a risk to the development of ND.
Keywords
Cataract Surgery, Negative Dysphotopsia, Intraocular Lens, Anterior Chamber Depth
1. Introduction
Cataract surgery is one of the most frequently performed surgeries in the world, and patients’ expectations of the visual outcome of cataract surgery are constantly rising.
Even though the surgery is presumed to be safe, there are few postoperative complications known, including, among others, negative dysphotopsia (ND).
Although ND was labelled in 2000
| [1] | R. Tester, N. L. Pace, M. Samore, and R. J. Olson, “Dysphotopsia in phakic and pseudophakic patients: incidence and relation to intraocular lens type,” J. Cataract Refract. Surg., vol. 26, no. 6, pp. 810–816, Jun. 2000, https://doi.org/10.1016/S0886-3350(00)00427-2 |
[1]
, the causes of it are not entirely known. Osher described that corneal edema combined with a beveled temporal incision can cause negative dysphotopsia
| [2] | R. H. Osher, “Negative dysphotopsia: Long-term study and possible explanation for transient symptoms,” J. Cataract Refract. Surg., vol. 34, no. 10, pp. 1699–1707, 2008, https://doi.org/10.1016/j.jcrs.2008.06.026 |
[2]
. Vamosi et al concluded that the reduction of the Iris-IOL-distance after IOL exchange can resolve negative dysphotopsia
| [3] | P. Vámosi, B. Csákány, and J. Németh, “Intraocular lens exchange in patients with negative dysphotopsia symptoms,” J. Cataract Refract. Surg., vol. 36, no. 3, pp. 418–424, 2010, https://doi.org/10.1016/j.jcrs.2009.10.035 |
[3]
. Holladay et al used ray-tracing techniques that showed that ND can occur when some rays miss the optic of the IOL
. Masket et al. found a neuroadaptive or a component of the central nervous system as part of the development of ND.
| [5] | S. Masket, Z. Rupnik, and N. R. Fram, “Neuroadaptive changes in negative dysphotopsia during contralateral eye occlusion,” J. Cataract Refract. Surg., vol. 45, no. 2, pp. 242–243, 2019, https://doi.org/10.1016/j.jcrs.2018.12.010 |
[5]
There are different aspects that have been examined, but as far as we know no study has analyzed so many parameters in so many patients as we have
| [6] | Wenzel M, Langenbucher A, Eppig T. "Ursachen, Diagnose und Therapie der negativen Dysphotopsie" [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klin Monbl Augenheilkd. 2019 Jun; 236(6): 767-776. German. https://doi.org/10.1055/s-0043-112855 |
[6]
.
The aim of our study was to find risk factors which contribute to the development of ND, as well as to confirm our theory which says that there is a relation between pupil size, axial length, anterior chamber depth and other biometrical factors as suggested in studies before
.
Furthermore, we wanted to examine the incidence of ND and identify the average period of ND, since there are only few and inconsistent data concerning this matter. For a better understanding of the patients’ complaints, we tried to illustrate the perceived shade in the visual field.
We also evaluated ND-patients’ satisfaction with the outcome of cataract surgery.
2. Methods
2.1. Study Design
In this retrospective study, data from patients who underwent cataract surgery from January 2018 to December 2019 at the Department of Ophthalmology at Clinic Hietzing in Vienna, were analyzed. Eight experienced surgeons performed all cataract extractions under local anesthesia. The 2.4 mm superior-temporal incision, injection of viscoelastic substance, capsulorhexis (with 360° overlapping edges), phacoemulsification, irrigation/aspiration of cortical material were performed as standard procedures. The IOL was implanted via an injector into the capsular bag. Only patients whose surgery had been uncomplicated were included in this study.
During the above period, a total of 8122 eyes underwent cataract surgery. To simplify the analysis of the results, only cases of surgeons who had performed at least 300 surgeries in these 2 years, were included. Three different IOLs have been implanted (EyeCee® One by Bausch&Lomb, TECNIS® by Johnson&Johnson, HOYA Vivienx ™ by HOYA), whereby all IOLs are hydrophobic acrylic aspheric monofocal one-piece IOls with C-loop haptics. The Power of every IOL that had been implanted was documented.
Data from patients who complained about negative dysphotopsia (ND) postoperatively were further analyzed, as well as data from a gender and age-matched control group. NDs that lasted for a period longer than 3 months were considered persistent. Before surgery, the patients were informed about ND and our study, however, postoperatively we did not ask specifically for ND symptoms in the first eye, but when the patients informed us about negative dysphotopsia in the first eye, we phoned them 3 months later and asked about the other eye as well.
The present study was approved by the local ethics committee, adhered to the tenets of the Declaration of Helsinki, and was performed by the rules of Good Clinical Practice of the ICH-WHO.
The patients who complained about ND were contacted by phone 3 to 6 months after their cataract surgery to complete a questionnaire about their satisfaction with the results of the surgery, about the duration of the ND symptoms, and about their impairment by these symptoms. If ND persisted until the call, a questionnaire had to be completed regarding complaints affecting their daily routines like reading, using a computer, driving during the day/night, and watching TV. Two scores were used to measure the overall satisfaction and disturbance in daily life tasks. The satisfaction score ranged from 0 to 3 (very satisfied = 0, satisfied = 1, little satisfied = 2, and not satisfied = 3). Each daily life task was given a disturbance score from 0 to 2 (not disturbed at all = 0, sometimes disturbed = 1, always disturbed = 2), a higher score showed a lower grade of satisfaction and a higher grade of impairment of the patient.
2.2. Measurements
Best-corrected visual acuity (BCVA) was assessed using Snellen equivalents, intra-ocular pressure using non-contact-tonometry (NCT). Refraction postoperatively was measured by auto-refractometer (Nidek ARK-30, Nidek Co. Ltd). A Pentacam Scheimpflug Camera (Oculus) was used to measure the postoperative anterior chamber depth (ACD), iridocorneal angle and iris-IOL distance. Anterior chamber depth (the distance between the anterior corneal surface and the anterior IOL surface) and iridocorneal angle, was automatically measured by the Pentacam, whereas iris-IOL distance had to be calculated manually with a caliper and was considered as the distance between the posterior surface of the iris and the anterior IOL surface at the pupil margin temporally on a horizontal scan.
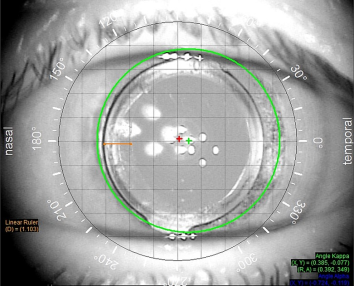
Axial length (AL) measurements were performed with the IOL Master 500 (Carl Zeiss Meditec AG). The iTrace VFA (Visual Function Analyzer manufactured by Tracey technologies) was used to measure the kappa angle, kappa distance, optic haptic orientation, IOL-bag overlap, and pupil diameter (PD). Iris-IOL-Overlap as well as kappa angle were measured as shown below. (
Figure 1)
Figure 1. The angle kappa display of the iTrace. The visual axis is marked with the red cross, the center of the pupil (green circle) is marked with the green cross. The screen displays the measurements of these distances (mm) in both polar coordinates and rectilinear coordinates in the bottom right of the eye image. The IOL overlapping part of the anterior capsular bag was measured with a caliper (linear ruler – orange colored in the bottom left of the eye image in mm, nasally and temporally by 0° und 180°.
Shadow distance and shadow orientation were depicted by the examiner on a Harms tangent screen reading chart. The patient was sitting only 1 m from the screen - instead of 2,5 meters – fixing the middle of the screen with one eye covered and was asked to show the perceived shadow with a laser pointer. The visual angle was then recalculated for a test distance of 1 m. For the graphical display of the results, a grid pattern was used.
2.3. Statistical Analysis
Statistical analyses were performed with SPSS 19.0 (SPSS Inc., Chicago, IL, USA). All data are presented as mean and standard deviation (SD). Patient demographics at baseline were analyzed using the chi-square and the Student-T-test. Student-T-test was used to compare parameters between the two study groups. Spearman’s rank correlation analysis was used to assess correlations. A p value of < 0.05 was considered significant.
3. Results
Over a 2-year-period, 8122 eyes underwent cataract surgery at our clinic, and 162 patients postoperatively complained of negative dysphotopsia. At 128 eyes, the symptoms disappeared within an average of 5.40 (±6.15) weeks, forming our transient group (NDt). We then further investigated the 34 eyes which suffered from persistent negative dysphotopsia (duration of symptoms longer than 3 months) and compared their biometrical data with an age- and gender-matched control group of 34 eyes. (
Table 1).
Table 1. Demographical data. Data are presented as mean ± SD.
| | N | NDt | NDp | CO |
Patients | | 130 | | | |
Eyes | | 196 | 128 | 34 | 34 |
Age (years) | | | 74.68 (±8) | 75 (±8) | 70 (±14) |
Sex | F | | 86 | 27 | 27 |
M | | 37 | 7 | 7 |
Side | R | | 51 | 12 | 20 |
L | | 70 | 22 | 14 |
IOL Type | B+L | | 53 | 15 | 7 |
Hoya | | 36 | 9 | 4 |
J&J | | 32 | 10 | 23 |
IOL Power (D) | | | | 23.44 (±1.95) | 22.56 (±3.07) |
Symptome Duration (weeks) | | | 5.40 (±6.148) | >12 | 0 |
NDt= transient negative dysphotopsia group, NDp = persistent negative dysphotopsia group, CO = Control group, IOL = intraocular lens, B+L= Bausch and Lomb IOL, J&J= Johnson and Johnson IOL
3.1. Results of the Total Cohort of 8122 Eyes
3.1.1. Incidence
This results in an incidence of 1.99% of negative dysphotopsia overall, an incidence of 1.58% of transient negative dysphotopsia cases, and an incidence of 0.42% of persistent negative dysphotopsia cases.
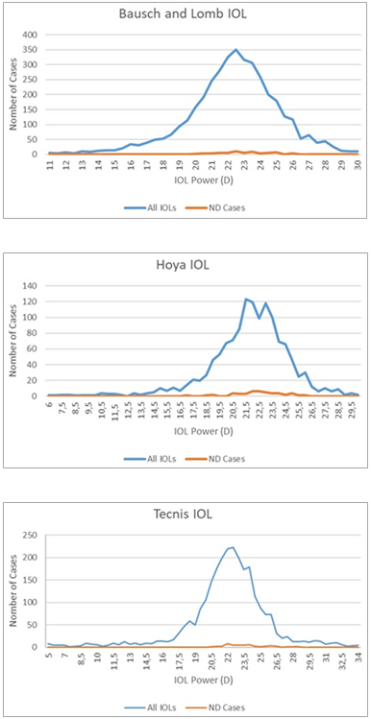
Besides the investigation of the incidence of negative dysphotopsia, our second objective was to determine the risk factors contributing to the development of negative dysphotopsia. As possible risk factors, we investigated 3 different IOL types, the surgeon and IOL power. The results are shown in
Figure 2A-C.
Figure 2. A, B and C show the Power distribution of the IOLs implanted, as well as the number of ND cases that occurred with each IOL separately.
3.1.2. Surgeon Factor
There was no statistically significant difference in the incidence of ND between the surgeons (p=0.15).
3.1.3. IOL (Type, Power)
The difference between the numbers of cases of ND for each IOL was not statistically significant (p=0.19). The Power of the IOLs implanted, as well as the number of ND cases that occurred with each IOL separately, are shown in
Figures 2A-C. The differences in incidence of ND per IOL-Power for every IOL (Bausch & Lomb p: 0,629, Hoya p: 0,959, Tecnis p: 0.68 Pearson-chi-squared) were not statistically significant.
3.2. Cohort of Patients with ND and Controls
3.2.1. Biometric Data
Table 2 shows the postoperative data collected from both groups (NDp and CO). There was only one significant difference in the anterior chamber depth between the two groups (p=0.03). There was no statistically significant difference in the axial length, iris-IOL distance, pupil diameter, size of angle kappa, or the IOL overlapping part of the anterior capsular bag.
To determine if anterior chamber depth was a significant risk factor for negative dysphotopsia a logistic regression analysis was performed. The best fit model (Nagelkerke R quadrat=0,163) has identified anterior chamber depth as a significant confounder (P=0.03; Exp β=0.35).
Table 2. Biometric data. Data are presented as mean ± SD.
| NDp | CO | P |
NCT | 16.35 (±2.42) | 16.85 (±2.68) | 0.42 |
BCVA | 0.9 (±0.12) | 0.9 (±0.12) | 0.15 |
Refraction SE (D) | -0.64 (±0.83) | -0.55 (±0.48) | 0.58 |
ACD (mm) | 5.1 (±0.58) | 5.41 (±0.61) | 0.03 |
AL (mm) | 22.66 (±1.18) | 23.1 (1.07) | 0.12 |
Glaucoma | 2 | 1 | 0.55 |
Iris colour | Blue | 9 | 11 | 0.50 |
Brown | 19 | 19 |
Green | 4 | 1 |
Iris-IOL-Distance (mm) | 0.95 (±0.45) | 1.10 (±1.07) | 0.47 |
Kappa angle (mm) | 218.76 (±119.11) | 223.44 (±83.12) | 0.85 |
Kappa distance (mm) | 1.13 (±1.34) | 0.74 (±0.96) | 0.18 |
IOL-Bag overlap (mm) | Temp | 0.93 (±1.85) | 0.61 (±1.09) | 0.39 |
Nasal | 0.45 (±0.36) | 0.41 (±0.26) | 0.67 |
Iridocorneal angle (°) | 37.19 (±12.33) | 41.08 (±10.73) | 0.17 |
PD (mm) | mesopic | 4.51 (±1.26) | 4.48 (±0.78) | 0.894 |
photopic | 2.99 (±0.89) | 2.89 (±0.53) | 0.604 |
NDp = persistent negative dysphotopsia group, CO = Control group, IOL = intraocular lens, NCT= non-contact-tonometry, BCVA= best corrected visual acuity, SE= spherical equivalent, ACD=anterior chamber depth, AL= axial length, PD=pupil diameter
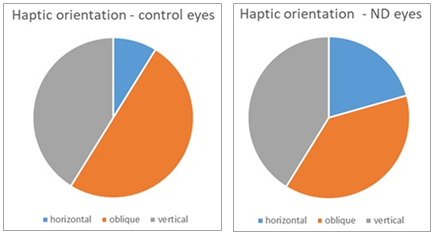
3.2.2. IOL Orientation
The haptic orientation of the IOL did not show a statistically significant correlation with the incidence of ND either, as shown in
Figure 3A-B (p=0.34). An orientation of the haptic at 0-30 degrees as well as 150-180 degrees was considered horizontal, an orientation at 30-60 as well as 120-150 degrees was considered oblique, and an orientation at 60-120 degrees was considered vertical. In the control group, 3 haptics were oriented horizontally, 17 were oriented oblique, and 14 were oriented vertically. In the NDp group, 7 haptics were oriented horizontally, 13 were oriented oblique, and 14 were oriented vertically.
Figure 3. A and B show the proportions of the haptic orientation in the two study groups.
3.2.3. Subjective Complaints (Scotomas, Satisfaction)
Table 3 shows the overall satisfaction and disturbance score of the patients during different daily life activities. The higher the score (range set in brackets), the less satisfied and the more disturbed the patient was.
Table 3. Questionnaire results. Data are presented as mean ± SD.
| Mean | Standard deviation |
Satisfaction (0-3) | 1.24 | 0.99 |
Disturbance (0-2) | 1.25 | 0.58 |
Reading (0-2) | 1.1 | 1.04 |
Using a computer (0-2) | 0.87 | 1.06 |
Driving during the day (0-2) | 1.16 | 1.07 |
Driving during the night (0-2) | 0.63 | 1.01 |
Watching TV (0-2) | 0.81 | 0.98 |
Overall Score (0-15) | 1.48 | 5.01 |
There was a statistically significant positive correlation between the patients’ general visual quality contentment and the height of their perceived shadow on the tangent screen (Spearman correlation coefficient: 0.51, P: 0.01). The larger the scotoma, the more dissatisfied the patient was.
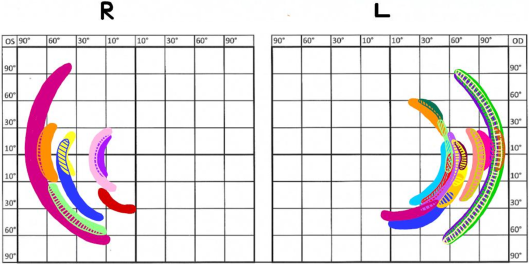
Figure 4 shows our attempt to display the scotomas graphically. Each colour is assigned to a patient. All scotomas were temporally, but there was a difference in height, as well as in the distance from the center. Some were situated more peripherally and some were larger than others. Just a few appeared to be superior, while most of them were placed in the lower visual field. Some patients were not able to show us the location of their shadow, so we were not able to include those.
Figure 4. Shows the graphical display of the scotomas. Each color is a different patient.
4. Discussion
To our knowledge, only a few available studies examining ND have included such a large number of eyes as we have, analyzing the data of more than 8000 eyes
| [3] | P. Vámosi, B. Csákány, and J. Németh, “Intraocular lens exchange in patients with negative dysphotopsia symptoms,” J. Cataract Refract. Surg., vol. 36, no. 3, pp. 418–424, 2010, https://doi.org/10.1016/j.jcrs.2009.10.035 |
| [6] | Wenzel M, Langenbucher A, Eppig T. "Ursachen, Diagnose und Therapie der negativen Dysphotopsie" [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klin Monbl Augenheilkd. 2019 Jun; 236(6): 767-776. German. https://doi.org/10.1055/s-0043-112855 |
| [8] | S. Masket and N. R. Fram, “Pseudophakic Dysphotopsia: Review of Incidence, Cause, and Treatment of Positive and Negative Dysphotopsia,” Ophthalmology, 2020, https://doi.org/10.1016/j.ophtha.2020.08.009 |
| [9] | J. A. Davison, “Positive and negative dysphotopsia in patients with acrylic intraocular lenses,” J. Cataract Refract. Surg., vol. 26, no. 9, pp. 1346–1355, 2000, https://doi.org/10.1016/S0886-3350(00)00611-8 |
[3, 6, 8, 9]
. The studies that come close are from Davison
who included 6668 eyes in his retrospective study, Wenzel et al
| [6] | Wenzel M, Langenbucher A, Eppig T. "Ursachen, Diagnose und Therapie der negativen Dysphotopsie" [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klin Monbl Augenheilkd. 2019 Jun; 236(6): 767-776. German. https://doi.org/10.1055/s-0043-112855 |
[6]
, who included 6031 cases, as well as Vàmosi et al, who
| [3] | P. Vámosi, B. Csákány, and J. Németh, “Intraocular lens exchange in patients with negative dysphotopsia symptoms,” J. Cataract Refract. Surg., vol. 36, no. 3, pp. 418–424, 2010, https://doi.org/10.1016/j.jcrs.2009.10.035 |
[3]
included 3806 eyes.
The incidence of ND varies from study to study, and it was reported between 0.13 and 15.7 percent.
| [5] | S. Masket, Z. Rupnik, and N. R. Fram, “Neuroadaptive changes in negative dysphotopsia during contralateral eye occlusion,” J. Cataract Refract. Surg., vol. 45, no. 2, pp. 242–243, 2019, https://doi.org/10.1016/j.jcrs.2018.12.010 |
[5]
Especially authors who had actively asked the patients, experienced a higher rate
| [6] | Wenzel M, Langenbucher A, Eppig T. "Ursachen, Diagnose und Therapie der negativen Dysphotopsie" [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klin Monbl Augenheilkd. 2019 Jun; 236(6): 767-776. German. https://doi.org/10.1055/s-0043-112855 |
[6]
. We might have found a higher rate if we had asked all patients actively after the surgery of the second eye. We found an incidence of 1.99% in our study including 8122 eyes. In 128 (1.58%) eyes, the symptoms ceased spontaneously after 5.40 (±6.15) weeks on average, so that the incidence of persistent ND cases was found to be 0.42%. Vamosi et al found an incidence of 0.13%
| [3] | P. Vámosi, B. Csákány, and J. Németh, “Intraocular lens exchange in patients with negative dysphotopsia symptoms,” J. Cataract Refract. Surg., vol. 36, no. 3, pp. 418–424, 2010, https://doi.org/10.1016/j.jcrs.2009.10.035 |
[3]
of severe cases of ND. Wenzel et al found an incidence of 0.02% in patients with such severe ND symptoms that they would have agreed to a second operation and when they actively called 300 patients one day after cataract surgery they found that 6% had symptoms like ND
| [6] | Wenzel M, Langenbucher A, Eppig T. "Ursachen, Diagnose und Therapie der negativen Dysphotopsie" [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klin Monbl Augenheilkd. 2019 Jun; 236(6): 767-776. German. https://doi.org/10.1055/s-0043-112855 |
[6]
. Davison found an incidence of 0,12%
. De Vries et al. described an incidence of 2.6%
. Osher found an incidence of 15% one day after surgery and an incidence of 3.2% after one year and a derease to 2.4% later 2-3 years in his prospective study with 250 eyes
| [2] | R. H. Osher, “Negative dysphotopsia: Long-term study and possible explanation for transient symptoms,” J. Cataract Refract. Surg., vol. 34, no. 10, pp. 1699–1707, 2008, https://doi.org/10.1016/j.jcrs.2008.06.026 |
[2]
, which is one of the few studies that observed the average duration of ND
. Trattler et al reported ND typical to disappear after 2 to 3 weeks, which is considerably shorter than in our experience
| [11] | W. B. Trattler, J. C. Whitsett, and P. A. Simone, “Negative dysphotopsia after intraocular lens implantation irrespective of design and material,” J. Cataract Refract. Surg., vol. 31, no. 4, pp. 841–845, 2005, https://doi.org/10.1016/j.jcrs.2004.12.044 |
[11]
. Makhotkina et al. asked patients 2-4 months after surgery by interview via phone and therefore found an incidence of 19%
| [12] | N. Y. Makhotkina, M. D. Nijkamp, T. T. J. M. Berendschot, B. van den Borne, and R. M. M. A. Nuijts, “Effect of active evaluation on the detection of negative dysphotopsia after sequential cataract surgery: discrepancy between incidences of unsolicited and solicited complaints,” Acta Ophthalmol., vol. 96, no. 1, pp. 81–87, 2018, https://doi.org/10.1111/aos.13508 |
[12].
Generally, a higher incidence was found when patients were actively asked about ND symptoms as shown in
Table 4.
Table 4. Incidence.
Author | Study Eyes | Incidence | Active/Passive |
Vamosi et al. | [3] | P. Vámosi, B. Csákány, and J. Németh, “Intraocular lens exchange in patients with negative dysphotopsia symptoms,” J. Cataract Refract. Surg., vol. 36, no. 3, pp. 418–424, 2010, https://doi.org/10.1016/j.jcrs.2009.10.035 |
[3] | 3806 | 0,13% severe cases | passive |
Wenzel et al. | [6] | Wenzel M, Langenbucher A, Eppig T. "Ursachen, Diagnose und Therapie der negativen Dysphotopsie" [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klin Monbl Augenheilkd. 2019 Jun; 236(6): 767-776. German. https://doi.org/10.1055/s-0043-112855 |
[6] | 300 patients | 6% | active |
| 6031 | 0,02% severe cases | Not declared |
DeVries et al. | 76 | 2,6% | Not declared |
Osher | [2] | R. H. Osher, “Negative dysphotopsia: Long-term study and possible explanation for transient symptoms,” J. Cataract Refract. Surg., vol. 34, no. 10, pp. 1699–1707, 2008, https://doi.org/10.1016/j.jcrs.2008.06.026 |
[2] | 250 | 15,2% one day after surgery and 3.2% after one year 2,4% after 2 and 3 years | active |
Davison | 6668 | 0,12% | passive |
Makhotkina et al. | [12] | N. Y. Makhotkina, M. D. Nijkamp, T. T. J. M. Berendschot, B. van den Borne, and R. M. M. A. Nuijts, “Effect of active evaluation on the detection of negative dysphotopsia after sequential cataract surgery: discrepancy between incidences of unsolicited and solicited complaints,” Acta Ophthalmol., vol. 96, no. 1, pp. 81–87, 2018, https://doi.org/10.1111/aos.13508 |
[12] | 95 patients | 19% | active |
In addition, we did not find any other study including the same amount of biometrical data as ours, to investigate risk factors or parameters that could be responsible for the development of negative dysphotopsia, except for one study from van Vught et al.
| [13] | L. van Vught, J. W. M. Beenakker, and G. P. M. Luyten, “Distinct differences in anterior chamber configuration and peripheral aberrations in negative dysphotopsia,” J. Cataract Refract. Surg., vol. 47, no. 1, pp. 140–141, 2021, https://doi.org/10.1097/j.jcrs.0000000000000431 |
[13]
, who found similar tendencies in their results. While they found a significant shorter axial length in their ND group, we found a significance in a shorter anterior chamber. It is logical that in an eye that is shorter, the anterior chamber is also shorter. We also made a great effort to gather real life data from real patients, while van Vught et al. collected a lot of their data through simulations.
The cause of ND is still unknown, although there are quite a few theories
. Trattler et al found the appearance of ND independent of IOL design or material, which matches our findings, in which we did not find a difference in IOL-types
| [11] | W. B. Trattler, J. C. Whitsett, and P. A. Simone, “Negative dysphotopsia after intraocular lens implantation irrespective of design and material,” J. Cataract Refract. Surg., vol. 31, no. 4, pp. 841–845, 2005, https://doi.org/10.1016/j.jcrs.2004.12.044 |
[11]
. Some authors tried different simulations in different eye models to find a cause for ND. Holladay et al found in one eye model, that a shadow is present when some rays miss the optic of the IOL
| [14] | J. T. Holladay and M. J. Simpson, “Negative dysphotopsia: Causes and rationale for prevention and treatment,” J. Cataract Refract. Surg., vol. 43, no. 2, pp. 263–275, 2017, https://doi.org/10.1016/j.jcrs.2016.11.049 |
[14]
. Besides, Holladay et al found that a small pupil, an axial space behind the iris, and a sharp optic edge are predisposing factors for ND, as well as the angle kappa and the nasal location of the pupil relative to the optical axis
. In our study, pupil size and angle kappa turned out not to be statistically significant, the same goes for the Iris-IOL-distance, but the anterior chamber depth postoperatively was significantly larger in the control group. Interestingly, anterior chamber depth didn`t show a significant difference between the two groups.
Vamosi et al also did not find the Iris-IOL-distance statistically significant, however, they found an improvement of ND, when the IOL was exchanged with a ciliary sulcus secondary IOL, but no improvement with a bag-to-bag exchange
| [3] | P. Vámosi, B. Csákány, and J. Németh, “Intraocular lens exchange in patients with negative dysphotopsia symptoms,” J. Cataract Refract. Surg., vol. 36, no. 3, pp. 418–424, 2010, https://doi.org/10.1016/j.jcrs.2009.10.035 |
[3]
. Masket et al also found ND only to appear with in-the-bag IOLs and not in ciliary sulcus-, anterior chamber-, or scleral suture-fixated IOLs, and a correlation with coverage of the anterior capsule edge. They, as well as Hong et al, found an improvement with reverse optic capture and piggyback secondary IOL, whereas a bag-to-bag exchange was not successful
| [15] | S. Masket and N. R. Fram, “Pseudophakic negative dysphotopsia: Surgical management and new theory of etiology,” J. Cataract Refract. Surg., vol. 37, no. 7, pp. 1199–1207, 2011, https://doi.org/10.1016/j.jcrs.2011.02.022 |
| [16] | S. Masket, N. R. Fram, A. Cho, I. Park, and D. Pham, “Surgical management of negative dysphotopsia,” J. Cataract Refract. Surg., vol. 44, no. 1, pp. 6–16, 2018, https://doi.org/10.1016/j.jcrs.2017.10.038 |
| [17] | X. Hong, Y. Liu, M. Karakelle, S. Masket, and N. R. Fram, “Ray-tracing optical modeling of negative dysphotopsia,” J. Biomed. Opt., vol. 16, no. 12, p. 125001, 2011, https://doi.org/10.1117/1.3656745 |
[15-17]
. Erie et al found an explanation for that in their simulation
| [18] | J. C. Erie, M. J. Simpson, and M. H. Bandhauer, “Effect of a sulcus-fixated piggyback intraocular lens on negative dysphotopsia: Ray-tracing analysis,” J. Cataract Refract. Surg., vol. 45, no. 4, pp. 443–450, 2019, https://doi.org/10.1016/j.jcrs.2018.10.041 |
[18]
. Hong et al found that the anterior capsulorhexis interacting with the intraocular lens could induce negative dysphotopsia. In our study we examined the IOL-bag overlap and did not find it statistically significant, and in none of our cases the bag was behind the optic of the IOL.
Makhotkina et al
| [19] | N. Y. Makhotkina, V. Dugrain, D. Purchase, T. T. J. M. Berendschot, and R. M. M. A. Nuijts, “Effect of supplementary implantation of a sulcus-fixated intraocular lens in patients with negative dysphotopsia,” J. Cataract Refract. Surg., vol. 44, no. 2, pp. 209–218, 2018, https://doi.org/10.1016/j.jcrs.2017.11.013 |
[19]
found the eyes that developed ND were significantly shorter and had a higher IOL power of their implanted lens than control eyes. In our study, we were not able to show any difference in axial length between ND eyes and non-ND eyes, however, we found that ND eyes presented a significantly shallower anterior chamber depth. (
Table 2) The iris – IOL distance was also slightly smaller in our ND group, but due to the larger spreading of the data, there was no statistically significant difference (
Table 2), which can be due to the fact that the imaging of the lens behind the iris is not so precise with the Pentacam as measuring the anterior chamber depth through the pupil, because Scheimpflug cameras don`t provide direct visualization of the lens behind the iris
| [20] | A. Konstantopoulos, P. Hossain, and D. F. Anderson, “Recent advances in ophthalmic anterior segment imaging: A new era for ophthalmic diagnosis?,” Br. J. Ophthalmol., vol. 91, no. 4, pp. 551–557, 2007, https://doi.org/10.1136/bjo.2006.103408 |
[20]
. Altogether, our finding is in accordance with the theory of Holladay et al
| [14] | J. T. Holladay and M. J. Simpson, “Negative dysphotopsia: Causes and rationale for prevention and treatment,” J. Cataract Refract. Surg., vol. 43, no. 2, pp. 263–275, 2017, https://doi.org/10.1016/j.jcrs.2016.11.049 |
[14]
, who suggested that a smaller Iris-IOL-distance is a factor associated with negative dysphotopsia.
Another assumption is that the position of the haptic contributes to the development of ND. Henderson et al found acrylic IOL implanted in the vertical position to lead to a higher incidence of ND than silicone IOL
| [21] | B. A. Henderson, D. H. Yi, J. B. Constantine, and I. I. Geneva, “New preventative approach for negative dysphotopsia,” J. Cataract Refract. Surg., vol. 42, no. 10, pp. 1449–1455, 2016, https://doi.org/10.1016/j.jcrs.2016.08.020 |
[21]
. In our study we only implanted acrylic IOLs, however we did not find a statistical significance in the position of the IOL haptics.
A more recent theory deals with the change of the location and size of the blind spot due to the exchange of the lens, as it was recently found that the shadow is less peripheral than originally assumed
| [22] | M. Wenzel, R. Menapace, T. Eppig, and A. Langenbucher, “Is the memory effect of the blind spot involved in negative dysphotopsia after cataract surgery?,” J. Ophthalmol., vol. 2015, no. December 2014, pp. 14–20, 2015, https://doi.org/10.1155/2015/786579 |
[22]
. Determining the location of the shadow is extremely difficult, since standard visual field testing often results in normal examination
| [15] | S. Masket and N. R. Fram, “Pseudophakic negative dysphotopsia: Surgical management and new theory of etiology,” J. Cataract Refract. Surg., vol. 37, no. 7, pp. 1199–1207, 2011, https://doi.org/10.1016/j.jcrs.2011.02.022 |
[15]
. Makhotkina et al tried with kinetic perimetry and found out that in 3 out of 9 patients a relative scotoma that matched the patients’ description was mapped during the study
| [19] | N. Y. Makhotkina, V. Dugrain, D. Purchase, T. T. J. M. Berendschot, and R. M. M. A. Nuijts, “Effect of supplementary implantation of a sulcus-fixated intraocular lens in patients with negative dysphotopsia,” J. Cataract Refract. Surg., vol. 44, no. 2, pp. 209–218, 2018, https://doi.org/10.1016/j.jcrs.2017.11.013 |
[19]
. Wenzel et al tried via a standard preprinted form sheet, normally used for Goldmann perimetry, which was presented to the patient at a reading distance. Wenzel et al also tried this method in another study and found the location at 17° temporally averagely
| [6] | Wenzel M, Langenbucher A, Eppig T. "Ursachen, Diagnose und Therapie der negativen Dysphotopsie" [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klin Monbl Augenheilkd. 2019 Jun; 236(6): 767-776. German. https://doi.org/10.1055/s-0043-112855 |
[6]
.
We also documented the shadow distance and orientation via a Harms tangent screen (
Figure 4). The results show that all scotomas are located temporally although there is a difference in the distance to the center and height. We found a correlation between the size of the shadow and the general satisfaction of the patient, which proves that these complaints are real and must be taken seriously by the ophthalmologists.
One of the most recent theories is from Masket et al who found that there is a neuroadaptive component or a component of the central nervous system, which contributes to the development of ND. They realized a spontaneous improvement in symptoms with translucent or opaque occlusion of the other eye
| [5] | S. Masket, Z. Rupnik, and N. R. Fram, “Neuroadaptive changes in negative dysphotopsia during contralateral eye occlusion,” J. Cataract Refract. Surg., vol. 45, no. 2, pp. 242–243, 2019, https://doi.org/10.1016/j.jcrs.2018.12.010 |
[5]
. In our study, after a few months, almost all of them learned to cope with their symptoms, which reinforces the theory of a neuroadaptive mechanism. Accordingly, we did not perform any IOL exchange or reverse optic capture as suggested by certain authors, because we were convinced that the complaints would decrease over time, and there is not enough evidence about the effectivity of this kind of surgery. Regarding the patients who were particularly unhappy, we suggested wearing spectacles, which also improved their symptoms.
There were some limitations to our study. We didn`t actively ask every patient about their symptoms, so it is possible that we missed some. Our sample size was limited by the retrospective nature of our study, as we only found 34 eyes with persistent negative dysphotopsia during the two years follow-up time. Further studies will be necessary to clarify the causes of negative dysphotopsia.
Logically, the Iris-IOL-distance should also be significant, which we could not detect. Probably due to our method of measurement, it was too imprecise. Measurements via ultrasound bio-microscopy should be performed.
5. Conclusion
There are several theories explaining the origin of negative dysphotopsia like: small pupil, an axial space behind the iris and a sharp optic edge. Also possible predisposing factors for ND might be a larger angle kappa and the nasal location of the pupil relative to the optical axis.
We have found that a shallow anterior chamber poses a risk for the development of ND. Furthermore, we have observed the outcome regarding the incidence of ND in our patients over a period of 2 years. We also examined the duration of the transient ND.
The reported incidence of ND was 1.99%, of which 1.58% was transient and 0.42% persistent. The average duration of the symptoms was 5.40 (±6.15) weeks.
Abbreviations
ND | Negative Dysphotopsia |
IOLs | Intraocular Lenses |
BCVA | Best-Corrected Visual Acuity |
NCT | Non-Contact-Tonometry |
ACD | Anterior Chamber Depth |
AL | Axial Length |
SD | Standard Deviation |
NDt | Transient Negative Dysphotopsia Group |
NDp | Persistent Negative Dysphotopsia Group |
CO | Control Group |
B+L | Bausch and Lomb IOL |
J&J | Johnson and Johnson IOL |
SE | Spherical Equivalent |
PD | Pupil Diameter |
Author Contributions
Tanja Spöttl: Methodology, Investigation, Writing - Original Draft Preparation
Kata Mihaltz: Conceptualization, Methodology, Investigation, Writing - Original Draft Preparation, Visualization, Supervision
Michael Burgmüller: Conceptualization, Methodology, Investigation, Writing - Review & Editing, Project Administration
Wolfgang Huf: Validation, Formal analysis
Alina Krencioch: Formal analysis, Investigation, Visualization, Writing - Review & Editing
Giovanna Reiterer: Validation, Data curation, Writing - Review & Editing
Andrzej Grzybowski: Conceptualization, Writing - Review & Editing
Pia Veronika Vécsei-Marlovits: Conceptualization, Resources, Writing - Review & Editing, Supervision
Funding
No government or non-government support.
Financial Disclosure
None of the authors have financial interest in the materials presented herein.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
R. Tester, N. L. Pace, M. Samore, and R. J. Olson, “Dysphotopsia in phakic and pseudophakic patients: incidence and relation to intraocular lens type,” J. Cataract Refract. Surg., vol. 26, no. 6, pp. 810–816, Jun. 2000,
https://doi.org/10.1016/S0886-3350(00)00427-2
|
| [2] |
R. H. Osher, “Negative dysphotopsia: Long-term study and possible explanation for transient symptoms,” J. Cataract Refract. Surg., vol. 34, no. 10, pp. 1699–1707, 2008,
https://doi.org/10.1016/j.jcrs.2008.06.026
|
| [3] |
P. Vámosi, B. Csákány, and J. Németh, “Intraocular lens exchange in patients with negative dysphotopsia symptoms,” J. Cataract Refract. Surg., vol. 36, no. 3, pp. 418–424, 2010,
https://doi.org/10.1016/j.jcrs.2009.10.035
|
| [4] |
J. T. Holladay, H. Zhao, and C. R. Reisin, “Negative dysphotopsia: The enigmatic penumbra,” J. Cataract Refract. Surg., vol. 38, no. 7, pp. 1251–1265, 2012,
https://doi.org/10.1016/j.jcrs.2012.01.032
|
| [5] |
S. Masket, Z. Rupnik, and N. R. Fram, “Neuroadaptive changes in negative dysphotopsia during contralateral eye occlusion,” J. Cataract Refract. Surg., vol. 45, no. 2, pp. 242–243, 2019,
https://doi.org/10.1016/j.jcrs.2018.12.010
|
| [6] |
Wenzel M, Langenbucher A, Eppig T. "Ursachen, Diagnose und Therapie der negativen Dysphotopsie" [Causes, Diagnosis and Therapy of Negative Dysphotopsia]. Klin Monbl Augenheilkd. 2019 Jun; 236(6): 767-776. German.
https://doi.org/10.1055/s-0043-112855
|
| [7] |
J. Schwiegerling, “Recent developments in pseudophakic dysphotopsia,” Curr. Opin. Ophthalmol., vol. 17, no. 1, pp. 27–30, 2006,
https://doi.org/10.1097/01.icu.0000193065.09499.7e
|
| [8] |
S. Masket and N. R. Fram, “Pseudophakic Dysphotopsia: Review of Incidence, Cause, and Treatment of Positive and Negative Dysphotopsia,” Ophthalmology, 2020,
https://doi.org/10.1016/j.ophtha.2020.08.009
|
| [9] |
J. A. Davison, “Positive and negative dysphotopsia in patients with acrylic intraocular lenses,” J. Cataract Refract. Surg., vol. 26, no. 9, pp. 1346–1355, 2000,
https://doi.org/10.1016/S0886-3350(00)00611-8
|
| [10] |
N. E. De Vries et al., “Dissatisfaction after implantation of multifocal intraocular lenses,” J. Cataract Refract. Surg., vol. 37, no. 5, pp. 859–865, 2011,
https://doi.org/10.1016/j.jcrs.2010.11.032
|
| [11] |
W. B. Trattler, J. C. Whitsett, and P. A. Simone, “Negative dysphotopsia after intraocular lens implantation irrespective of design and material,” J. Cataract Refract. Surg., vol. 31, no. 4, pp. 841–845, 2005,
https://doi.org/10.1016/j.jcrs.2004.12.044
|
| [12] |
N. Y. Makhotkina, M. D. Nijkamp, T. T. J. M. Berendschot, B. van den Borne, and R. M. M. A. Nuijts, “Effect of active evaluation on the detection of negative dysphotopsia after sequential cataract surgery: discrepancy between incidences of unsolicited and solicited complaints,” Acta Ophthalmol., vol. 96, no. 1, pp. 81–87, 2018,
https://doi.org/10.1111/aos.13508
|
| [13] |
L. van Vught, J. W. M. Beenakker, and G. P. M. Luyten, “Distinct differences in anterior chamber configuration and peripheral aberrations in negative dysphotopsia,” J. Cataract Refract. Surg., vol. 47, no. 1, pp. 140–141, 2021,
https://doi.org/10.1097/j.jcrs.0000000000000431
|
| [14] |
J. T. Holladay and M. J. Simpson, “Negative dysphotopsia: Causes and rationale for prevention and treatment,” J. Cataract Refract. Surg., vol. 43, no. 2, pp. 263–275, 2017,
https://doi.org/10.1016/j.jcrs.2016.11.049
|
| [15] |
S. Masket and N. R. Fram, “Pseudophakic negative dysphotopsia: Surgical management and new theory of etiology,” J. Cataract Refract. Surg., vol. 37, no. 7, pp. 1199–1207, 2011,
https://doi.org/10.1016/j.jcrs.2011.02.022
|
| [16] |
S. Masket, N. R. Fram, A. Cho, I. Park, and D. Pham, “Surgical management of negative dysphotopsia,” J. Cataract Refract. Surg., vol. 44, no. 1, pp. 6–16, 2018,
https://doi.org/10.1016/j.jcrs.2017.10.038
|
| [17] |
X. Hong, Y. Liu, M. Karakelle, S. Masket, and N. R. Fram, “Ray-tracing optical modeling of negative dysphotopsia,” J. Biomed. Opt., vol. 16, no. 12, p. 125001, 2011,
https://doi.org/10.1117/1.3656745
|
| [18] |
J. C. Erie, M. J. Simpson, and M. H. Bandhauer, “Effect of a sulcus-fixated piggyback intraocular lens on negative dysphotopsia: Ray-tracing analysis,” J. Cataract Refract. Surg., vol. 45, no. 4, pp. 443–450, 2019,
https://doi.org/10.1016/j.jcrs.2018.10.041
|
| [19] |
N. Y. Makhotkina, V. Dugrain, D. Purchase, T. T. J. M. Berendschot, and R. M. M. A. Nuijts, “Effect of supplementary implantation of a sulcus-fixated intraocular lens in patients with negative dysphotopsia,” J. Cataract Refract. Surg., vol. 44, no. 2, pp. 209–218, 2018,
https://doi.org/10.1016/j.jcrs.2017.11.013
|
| [20] |
A. Konstantopoulos, P. Hossain, and D. F. Anderson, “Recent advances in ophthalmic anterior segment imaging: A new era for ophthalmic diagnosis?,” Br. J. Ophthalmol., vol. 91, no. 4, pp. 551–557, 2007,
https://doi.org/10.1136/bjo.2006.103408
|
| [21] |
B. A. Henderson, D. H. Yi, J. B. Constantine, and I. I. Geneva, “New preventative approach for negative dysphotopsia,” J. Cataract Refract. Surg., vol. 42, no. 10, pp. 1449–1455, 2016,
https://doi.org/10.1016/j.jcrs.2016.08.020
|
| [22] |
M. Wenzel, R. Menapace, T. Eppig, and A. Langenbucher, “Is the memory effect of the blind spot involved in negative dysphotopsia after cataract surgery?,” J. Ophthalmol., vol. 2015, no. December 2014, pp. 14–20, 2015,
https://doi.org/10.1155/2015/786579
|
Cite This Article
-
APA Style
Spöttl, T., Miháltz, K., Burgmüller, M., Huf, W., Krencioch, A., et al. (2024). Retrospective Analysis of Negative Dysphotopsia After Cataract Surgery. International Journal of Ophthalmology & Visual Science, 9(2), 13-22. https://doi.org/10.11648/j.ijovs.20240902.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Spöttl, T.; Miháltz, K.; Burgmüller, M.; Huf, W.; Krencioch, A., et al. Retrospective Analysis of Negative Dysphotopsia After Cataract Surgery. Int. J. Ophthalmol. Vis. Sci. 2024, 9(2), 13-22. doi: 10.11648/j.ijovs.20240902.11
Copy
|
Download
AMA Style
Spöttl T, Miháltz K, Burgmüller M, Huf W, Krencioch A, et al. Retrospective Analysis of Negative Dysphotopsia After Cataract Surgery. Int J Ophthalmol Vis Sci. 2024;9(2):13-22. doi: 10.11648/j.ijovs.20240902.11
Copy
|
Download
-
@article{10.11648/j.ijovs.20240902.11,
author = {Tanja Spöttl and Kata Miháltz and Michael Burgmüller and Wolfgang Huf and Alina Krencioch and Giovanna Reiterer and Andrzej Grzybowski and Pia Veronika Vécsei-Marlovits},
title = {Retrospective Analysis of Negative Dysphotopsia After Cataract Surgery
},
journal = {International Journal of Ophthalmology & Visual Science},
volume = {9},
number = {2},
pages = {13-22},
doi = {10.11648/j.ijovs.20240902.11},
url = {https://doi.org/10.11648/j.ijovs.20240902.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijovs.20240902.11},
abstract = {Purpose: To describe the incidence and characteristics of negative dysphotopsia (ND) as well as the risk factors contributing to it. Methods: For this retrospective study, data from patients who underwent cataract surgery between January 2018 and December 2019 at our department (Department of Ophthalmology, Hietzing Hospital, Vienna, Austria) was analyzed. A total of 8122 eyes had cataract surgery performed. Three different intraocular lenses (IOLs) have been used (EyeCee® One by Bausch + Lomb, TECNIS® by Johnson & Johnson, HOYA Vivienx ™ by HOYA). Data from patients who postoperatively complained about ND as well as data from a gender and age-matched control group (34 eyes in each) was further analyzed: pupil size, axial length, anterior chamber depth, angle kappa, IOL power and other biometrical factors. The scotomas were depicted on a Harms tangent screen. Results: An incidence of 1.99% of ND was found, of which 1.58% was transient and 0.42% persistent. The average duration of the symptoms was 5.40 (±6.15) weeks in the transient ND group. In the total cohort of 8122 eyes, there was no difference in the distribution of implanted IOL types or IOL power; neither played the surgeon a significant role in the development of ND. There was no significant difference between ND and control eyes regarding pupil size, axial length, and angle kappa. The anterior chamber was significantly shallower in the ND group: 5.1±0.58mm vs. 5.41±0.61mm (p=0.03). Conclusion: According to our findings, a shallower anterior chamber poses a risk to the development of ND.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Retrospective Analysis of Negative Dysphotopsia After Cataract Surgery
AU - Tanja Spöttl
AU - Kata Miháltz
AU - Michael Burgmüller
AU - Wolfgang Huf
AU - Alina Krencioch
AU - Giovanna Reiterer
AU - Andrzej Grzybowski
AU - Pia Veronika Vécsei-Marlovits
Y1 - 2024/05/24
PY - 2024
N1 - https://doi.org/10.11648/j.ijovs.20240902.11
DO - 10.11648/j.ijovs.20240902.11
T2 - International Journal of Ophthalmology & Visual Science
JF - International Journal of Ophthalmology & Visual Science
JO - International Journal of Ophthalmology & Visual Science
SP - 13
EP - 22
PB - Science Publishing Group
SN - 2637-3858
UR - https://doi.org/10.11648/j.ijovs.20240902.11
AB - Purpose: To describe the incidence and characteristics of negative dysphotopsia (ND) as well as the risk factors contributing to it. Methods: For this retrospective study, data from patients who underwent cataract surgery between January 2018 and December 2019 at our department (Department of Ophthalmology, Hietzing Hospital, Vienna, Austria) was analyzed. A total of 8122 eyes had cataract surgery performed. Three different intraocular lenses (IOLs) have been used (EyeCee® One by Bausch + Lomb, TECNIS® by Johnson & Johnson, HOYA Vivienx ™ by HOYA). Data from patients who postoperatively complained about ND as well as data from a gender and age-matched control group (34 eyes in each) was further analyzed: pupil size, axial length, anterior chamber depth, angle kappa, IOL power and other biometrical factors. The scotomas were depicted on a Harms tangent screen. Results: An incidence of 1.99% of ND was found, of which 1.58% was transient and 0.42% persistent. The average duration of the symptoms was 5.40 (±6.15) weeks in the transient ND group. In the total cohort of 8122 eyes, there was no difference in the distribution of implanted IOL types or IOL power; neither played the surgeon a significant role in the development of ND. There was no significant difference between ND and control eyes regarding pupil size, axial length, and angle kappa. The anterior chamber was significantly shallower in the ND group: 5.1±0.58mm vs. 5.41±0.61mm (p=0.03). Conclusion: According to our findings, a shallower anterior chamber poses a risk to the development of ND.
VL - 9
IS - 2
ER -
Copy
|
Download