Diabetic retinopathy (DR), an ocular complication of diabetes mellitus, is the leading cause of permanent blindness in the United States for young adults. Due to biological and environmental factors, diabetes mellitus is well known to disproportionally affect people of color and those of lower socioeconomic status; however, the racial and socioeconomic disparities of DR are less researched. The purpose of this research is to elucidate any differences in DR presentation that arise across racial and socioeconomic lines and to determine if diabetic control can be a predicting factor for DR severity. For this study, a retrospective patient chart analysis was performed on 511 consecutive newly referred patients with diabetes at New England Retina Associates, a vitreo-retinal ophthalmology practice with four locations throughout Connecticut. Our analysis shows that, when compared to their White and Asian counterparts, Black/African American and Hispanic patients present with DR at younger ages, had the higher HbA1c, were uninsured at higher rates, and presented with severe forms of DR in higher rates when compared to their counterparts. Many of these patterns are mirrored in patients that are uninsured or on Medicaid, indicators of lower socioeconomic status. Additionally, regardless of race or socioeconomic status, patients with higher HbA1c tended to present with more severe forms of DR. These findings indicate that DR disproportionately affects racial minority populations and those in socioeconomically disadvantageous positions, but effective glycemic control and routine eye exam screening can improve the outcomes of these patients. It is important for medical providers to recognize the disparities in these vulnerable populations in order to facilitate the timely referrals and the proper care for their long-term ocular health.
| Published in | International Journal of Ophthalmology & Visual Science (Volume 9, Issue 3) |
| DOI | 10.11648/j.ijovs.20240903.11 |
| Page(s) | 30-39 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Diabetic Retinopathy, Socioeconomic Differences, Healthcare Disparities, Social Determinants Of Health, Diabetes Mellitus
Whole Population | White | Black/African American | Asian | Hispanic | Other | Did Not List | |
|---|---|---|---|---|---|---|---|
n=511 (100) | n=224 (43.8) | n=81 (15.9) | n=22 (4.3) | n=93 (18.2) | n=12 (2.3) | n=79 (15.5) | |
Avg. Age | 63.5 | 66.0 | 59.3 | 62.8 | 59.6 | 65.0 | 65.27 |
Sex | |||||||
Male | 235 (45.99) | 108 (48.21) | 34 (41.98) | 12 (54.55) | 45 (48.39) | 2 (16.67) | 34 (43.04) |
Female | 276 (54.01) | 116 (51.79) | 47 (58.02) | 10 (45.45 | 48 (51.61) | 10 (83.33) | 45 (56.96) |
Insurance | |||||||
Medicare | 222 (43.4) | 109 (48.7) | 31 (38.3) | 11 (50.0) | 27 (29.0) | 4 (33.3) | 40 (50.0) |
Medicaid | 62 (12.13) | 13 (5.8) | 12 (14.8) | 2 (9.1) | 21 (22.6) | 1 (8.3) | 13 (16.25) |
Commercial | 199 (38.9) | 97 (43.3) | 34 (42.0) | 9 (40.9) | 33 (35.5) | 6 (50.0) | 20 (25.0) |
None | 28 (5.5) | 5 (2.2) | 4 (4.9) | 0 (0) | 12 (12.9) | 1 (8.3) | 6 (7.5) |
Whole Population | White | Black/African American | Asian | Hispanic | Other | Did Not List | |
|---|---|---|---|---|---|---|---|
n=511 (100) | n=224 (43.8) | n=81 (15.9) | n=22 (4.3) | n=93 (18.2) | n=12 (2.3) | n=79 (15.5) | |
Avg. HbA1c | 7.68 | 7.39 | 8.00 | 6.59 | 8.11 | 7.78 | 8.11 |
# DNK | 177 (34.64) | 61 (27.23) | 27 (33.75) | 11 (50) | 42 (45.16) | 1 (8.33) | 33 (41.25) |
# of Meds | 6.05 | 6.29 | 6.07 | 4.27 | 6.00 | 8.08 | 5.57 |
# of DM Meds | 1.83 | 1.81 | 1.69 | 1.76 | 2.07 | 2.42 | 1.71 |
DR Severity | |||||||
None | 235 (23.0%) | 122 (27.2%) | 24 (14.8%) | 12 (27.3%) | 47 (25.3%) | 6 (25.0%) | 24 (15.2%) |
Mild | 236 (23.1%) | 114 (25.4%) | 21 (13.0%) | 16 (36.4%) | 34 (18.3%) | 5 (20.8%) | 46 (29.1%) |
Moderate | 277 (27.1%) | 138 (30.8%) | 41 (25.3%) | 11 (25.0%) | 46 (24.7%) | 8 (33.3%) | 33 (20.9%) |
Severe NP | 95 (9.3%) | 25 (5.6%) | 22 (13.6%) | 2 (4.6%) | 14 (7.5%) | 4 (16.7%) | 28 (17.7%) |
Proliferative | 179 (17.5%) | 49 (10.9%) | 54 (33.3%) | 3 (6.8%) | 45 (24.2%) | 1 (4.2%) | 27 (17.1%) |
Avg. VA (logMar) | 0.35 | 0.31 | 0.45 | 0.36 | 0.37 | 0.44 | 0.35 |
Whole Population | Commercial | Medicaid | Medicare | None | |
|---|---|---|---|---|---|
n=511 (100) | n=199 (38.9) | n=62 (12.13) | n=222 (43.4) | n=28 (5.5) | |
Avg. Age | 63.5 | 57.85 | 55.98 | 71.5 | 56.82 |
Sex | |||||
Male | 235 | 107 | 24 | 90 | 14 |
Female | 276 | 92 | 38 | 132 | 14 |
Avg. HbA1C | 7.68 | 7.95 | 7.64 | 7.30 | 8.48 |
# DNK | 177 (34.64) | 57 (28.64) | 28 (45.16) | 82 (36.94) | 11 (39.29) |
Avg. VA (logMar) | 0.35 | 0.29 | 0.35 | 0.41 | 0.42 |
DR Severity | |||||
None | 235 (22.0) | 83 (20.85) | 23 (18.55) | 120 (27.03) | 9 (16.07) |
Mild | 236 (23.1) | 84 (21.11) | 23 (18.55) | 126 (28.38) | 3 (5.36) |
Moderate | 277 (28.2) | 116 (29.15) | 31 (25.00) | 108 (24.32) | 22 (39.29) |
Severe NPDR | 95 (9.3) | 35 (8.79) | 18 (14.52) | 40 (9.01) | 2 (3.57) |
PDR | 179 (17.4) | 80 (20.10) | 29 (23.39) | 50 (11.04) | 20 (35.71) |
# of Meds # of DM Meds | 6.05 | 5.18 | 5.63 | 7.12 | 4.82 |
Male + Comm. | Female + Comm. | Male + Medicaid | Female + Medicaid | Male + Medicare | Female + Medicare | Male + None | Female+ None | |
|---|---|---|---|---|---|---|---|---|
DR Severity | ||||||||
None | 37(17.29%) | 46(25.00%) | 7(14.58%) | 16(21.05%) | 52(28.89%) | 68(25.76%) | 7(25.00%) | 2(7.14%) |
Mild | 52(24.30%) | 32(17.395) | 6(12.50%) | 17(22.37%) | 56(31.11%) | 70(26.52%) | 1(3.57%) | 2(7.14%) |
Moderate | 57(26.64%) | 59(32.07%) | 14(29.17%) | 17(22.37%) | 41(22.78%) | 67(25.38%) | 8(28.57%) | 14(50.00%) |
Severe | 24(11.21%) | 11(5.98%) | 7(14.58%) | 11(14.47%) | 10(5.56%) | 30(11.36%) | 2(7.14%) | 0(0.00%) |
Proliferative | 44(20.56%) | 36(19.57%) | 14(29.17%) | 15(19.74%) | 21(11.67%) | 29(10.98%) | 10(35.71%) | 10(35.71%) |
Total | 214(100%) | 184(100%) | 48(100%) | 76(100%) | 180(100%) | 264(100%) | 28(100%) | 28(100%) |
DNK | Did Not Know |
DR | Diabetic Retinopathy |
HbA1c | Hemoglobin A1c |
NPDR | Nonproliferative Diabetic Retinopathy |
PDR | Proliferative Diabetic Retinopathy |
VA | Visual Acuity |
VEGF | Vascular Endothelial Growth Factor |
| [1] | Banday MZ, Sameer AS, Nissar S. Pathophysiology of diabetes: An overview. Avicenna J Med. 2020; 10(4): 174-188. Published 2020 Oct 13. |
| [2] | Bancks MP, Kershaw K, Carson AP, Gordon-Larsen P, Schreiner PJ, Carnethon MR. Association of Modifiable Risk Factors in Young Adulthood With Racial Disparity in Incident Type 2 Diabetes During Middle Adulthood. JAMA. 2017; 318(24): 2457-2465. |
| [3] |
Centers for Disease Control and Prevention. National Diabetes Statistics Report website.
https://www.cdc.gov/diabetes/data/statistics-report/index.html Accessed January 13, 2024. |
| [4] | Wang W, Lo ACY. Diabetic Retinopathy: Pathophysiology and Treatments. Int J Mol Sci. 2018; 19(6): 1816. Published 2018 Jun 20. |
| [5] | Williams R, Airey M, Baxter H, Forrester J, Kennedy-Martin T, Girach A. Epidemiology of diabetic retinopathy and macular oedema: a systematic review. Eye (Lond). 2004; 18(10): 963-983. |
| [6] | Nsiah-Kumi P, Ortmeier SR, Brown AE. Disparities in diabetic retinopathy screening and disease for racial and ethnic minority populations--a literature review. J Natl Med Assoc. 2009; 101(5): 430-437. Published 2009 May. |
| [7] | Thomas CG, Channa R, Prichett L, Liu TYA, Abramoff MD, Wolf RM. Racial/Ethnic Disparities and Barriers to Diabetic Retinopathy Screening in Youths. JAMA Ophthalmol. 2021; 139(7): 791-795. |
| [8] | Huang BB, Radha Saseendrakumar B, Delavar A, Baxter SL. Racial Disparities in Barriers to Care for Patients With Diabetic Retinopathy in a Nationwide Cohort. Transl Vis Sci Technol. 2023; 12(3): 14. Published 2023 March. |
| [9] | Rodríguez JE, Campbell KM. Racial and Ethnic Disparities in Prevalence and Care of Patients With Type 2 Diabetes. Clin Diabetes. 2017; 35(1): 66-70. Published 2017 Jan 1. |
| [10] | Coney JM, Scott AW. Racial disparities in the screening and treatment of diabetic retinopathy. J Natl Med Assoc. 2022; 114(2): 171-181. Published 2022 Jan 31. |
| [11] | Kulkarni, Karmeen. Food, Culture, and Diabetes in the United States. Clin Diabetes. 22(4): 190–192. Published 2004 Oct 1. |
| [12] | Al Shamsi H, Almutairi AG, Al Mashrafi S, Al Kalbani T. Implications of Language Barriers for Healthcare: A Systematic Review. Oman Med J. 2020; 35(2): e122. Published 2020 Apr 30. |
| [13] | Handtke O, Schilgen B, Mösko M. Culturally competent healthcare - A scoping review of strategies implemented in healthcare organizations and a model of culturally competent healthcare provision. PLoS One. 2019; 14(7): e0219971. Published 2019 Jul 30. |
| [14] | Kempen JH, O'Colmain BJ, Leske MC, et al. The prevalence of diabetic retinopathy among adults in the United States. Arch Ophthalmol. 2004; 122(4): 552-563. |
| [15] | Fenwick E, Rees G, Pesudovs K, et al. Social and emotional impact of diabetic retinopathy: a review. Clin Exp Ophthalmol. 2012; 40(1): 27-38. Published 2011 May 17. |
APA Style
Huang, D., Channamsetty, S., Verter, E., Huang, J. (2024). Racial and Socioeconomic Differences Correlate with Healthcare Disparities in Patients with Diabetic Retinopathy. International Journal of Ophthalmology & Visual Science, 9(3), 30-39. https://doi.org/10.11648/j.ijovs.20240903.11
ACS Style
Huang, D.; Channamsetty, S.; Verter, E.; Huang, J. Racial and Socioeconomic Differences Correlate with Healthcare Disparities in Patients with Diabetic Retinopathy. Int. J. Ophthalmol. Vis. Sci. 2024, 9(3), 30-39. doi: 10.11648/j.ijovs.20240903.11
@article{10.11648/j.ijovs.20240903.11,
author = {Deven Huang and Sara Channamsetty and Erol Verter and John Huang},
title = {Racial and Socioeconomic Differences Correlate with Healthcare Disparities in Patients with Diabetic Retinopathy
},
journal = {International Journal of Ophthalmology & Visual Science},
volume = {9},
number = {3},
pages = {30-39},
doi = {10.11648/j.ijovs.20240903.11},
url = {https://doi.org/10.11648/j.ijovs.20240903.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijovs.20240903.11},
abstract = {Diabetic retinopathy (DR), an ocular complication of diabetes mellitus, is the leading cause of permanent blindness in the United States for young adults. Due to biological and environmental factors, diabetes mellitus is well known to disproportionally affect people of color and those of lower socioeconomic status; however, the racial and socioeconomic disparities of DR are less researched. The purpose of this research is to elucidate any differences in DR presentation that arise across racial and socioeconomic lines and to determine if diabetic control can be a predicting factor for DR severity. For this study, a retrospective patient chart analysis was performed on 511 consecutive newly referred patients with diabetes at New England Retina Associates, a vitreo-retinal ophthalmology practice with four locations throughout Connecticut. Our analysis shows that, when compared to their White and Asian counterparts, Black/African American and Hispanic patients present with DR at younger ages, had the higher HbA1c, were uninsured at higher rates, and presented with severe forms of DR in higher rates when compared to their counterparts. Many of these patterns are mirrored in patients that are uninsured or on Medicaid, indicators of lower socioeconomic status. Additionally, regardless of race or socioeconomic status, patients with higher HbA1c tended to present with more severe forms of DR. These findings indicate that DR disproportionately affects racial minority populations and those in socioeconomically disadvantageous positions, but effective glycemic control and routine eye exam screening can improve the outcomes of these patients. It is important for medical providers to recognize the disparities in these vulnerable populations in order to facilitate the timely referrals and the proper care for their long-term ocular health.
},
year = {2024}
}
TY - JOUR T1 - Racial and Socioeconomic Differences Correlate with Healthcare Disparities in Patients with Diabetic Retinopathy AU - Deven Huang AU - Sara Channamsetty AU - Erol Verter AU - John Huang Y1 - 2024/07/02 PY - 2024 N1 - https://doi.org/10.11648/j.ijovs.20240903.11 DO - 10.11648/j.ijovs.20240903.11 T2 - International Journal of Ophthalmology & Visual Science JF - International Journal of Ophthalmology & Visual Science JO - International Journal of Ophthalmology & Visual Science SP - 30 EP - 39 PB - Science Publishing Group SN - 2637-3858 UR - https://doi.org/10.11648/j.ijovs.20240903.11 AB - Diabetic retinopathy (DR), an ocular complication of diabetes mellitus, is the leading cause of permanent blindness in the United States for young adults. Due to biological and environmental factors, diabetes mellitus is well known to disproportionally affect people of color and those of lower socioeconomic status; however, the racial and socioeconomic disparities of DR are less researched. The purpose of this research is to elucidate any differences in DR presentation that arise across racial and socioeconomic lines and to determine if diabetic control can be a predicting factor for DR severity. For this study, a retrospective patient chart analysis was performed on 511 consecutive newly referred patients with diabetes at New England Retina Associates, a vitreo-retinal ophthalmology practice with four locations throughout Connecticut. Our analysis shows that, when compared to their White and Asian counterparts, Black/African American and Hispanic patients present with DR at younger ages, had the higher HbA1c, were uninsured at higher rates, and presented with severe forms of DR in higher rates when compared to their counterparts. Many of these patterns are mirrored in patients that are uninsured or on Medicaid, indicators of lower socioeconomic status. Additionally, regardless of race or socioeconomic status, patients with higher HbA1c tended to present with more severe forms of DR. These findings indicate that DR disproportionately affects racial minority populations and those in socioeconomically disadvantageous positions, but effective glycemic control and routine eye exam screening can improve the outcomes of these patients. It is important for medical providers to recognize the disparities in these vulnerable populations in order to facilitate the timely referrals and the proper care for their long-term ocular health. VL - 9 IS - 3 ER -
College of Arts and Science, New York University, New York City, United States; New England Retina Associates, ReFocus Eye Health, Hamden, United States
Student Body, Greenwich Academy, Greenwich, United States
New England Retina Associates, ReFocus Eye Health, Hamden, United States; Ophthalmology, Yale New Haven Hospital, New Haven, United States; Ophthalmology, Greenwich Hospital, Greenwich, United States; Ophthalmology, Bridgeport Hospital, Bridgeport, United States; Ophthalmology, Stamford Hospital, Stamford, United States; Ophthalmology, Saint Vincent’s Hospital, Bridgeport, United States
New England Retina Associates, ReFocus Eye Health, Hamden, United States; Ophthalmology, Yale New Haven Hospital, New Haven, United States; Ophthalmology, Greenwich Hospital, Greenwich, United States; Ophthalmology, Bridgeport Hospital, Bridgeport, United States;Ophthalmology, Saint Vincent’s Hospital, Bridgeport, United States; School of Medicine, Yale University, New Haven, United States; Administration, Connecticut Uveitis Foundation, West Hartford, United States
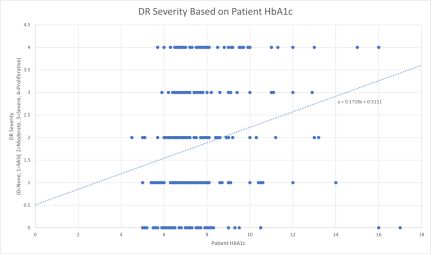
Figure 1. Plot of DR Severity for each eye by the patient’s HbA1c. 0 represents no retinopathy, 1 represents mild, 2 represents moderate, 3 represents severe, and 4 represents proliferative.
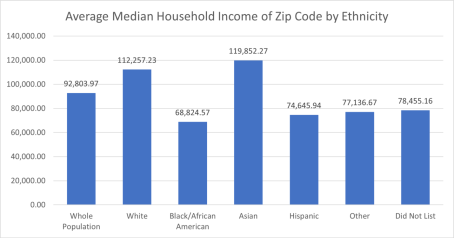
Figure 2. Average Median Household Income of Zip Code of Each Ethnic Group.
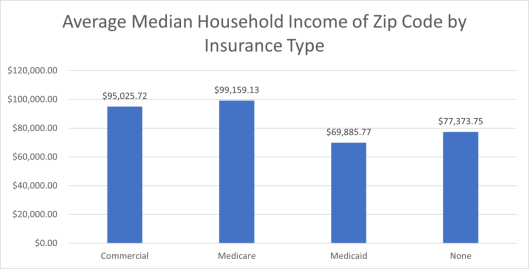
Figure 3. Average Median Household Income of Zip Code of Each Insurance Type.
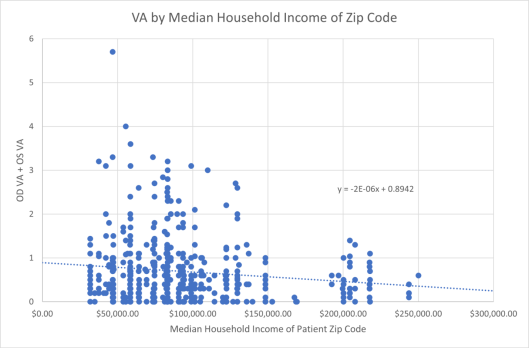
Figure 4. Plot of VA for each eye by the median household income of the patient’s zip code.
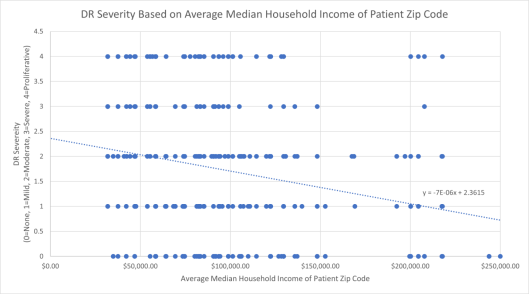
Figure 5. Plot of DR Severity for each eye by the median household income of the patient’s zip code. 0 represents no retinopathy, 1 represents mild, 2 represents moderate, 3 represents severe, and 4 represents proliferative.
Information

