Purpose: To evaluate the visual recovery and intraocular pressure control after cataract surgery in patients of phacolytic glaucoma. Methods: 23 patients diagnosed clinically as phacolytic glaucoma and included in the study were operated upon using either SICS or Phacoemulsification procedure after lowering of the Intraocular pressure (IOP) and control of ocular inflammation. Results: Post-operatively 21.73% of patients achieved a best corrected visual acuity (BCVA) of 6/60-6/12, 43.82% had a BCVA of 4/60-6/60 and 30.43% achieved a final BCVA between 4/60 to only perception of light. However 86.95% of patients maintained an IOP less than 20 mm Hg, 8.69% had an IOP between 20-23 mm Hg and 4.34% had an IOP between 24-30 mm Hg requiring a Glaucoma filtering surgery. Conclusion: Patients of Phacolytic Glaucoma if present at an early stage can have a good visual recovery and well controlled IOP in the post-operative period.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Phacolytic Glaucoma, Small Incision Cataract Surgery (SICS), Intraocular Pressure (IOP)
1. Introduction
Phacolytic glaucoma is a type of lens-induced glaucoma seen in long-standing or neglected hypermature cataracts
[1]
Kelly L, Sarwat S. Lens-Induced Glaucoma: Diagnosis and Management. AAO.org. posted October 01, 2016.
[1]
. The condition is rarely seen nowadays, however, in developing countries like India, the condition still exists although less common. One big factor for the occurrence of Phacolytic glaucoma in India is a huge cataract backlog making patients reach the stage of hypermature cataracts before being taken for surgery.
In a hypermature / Morgagnian cataract, the cortical lens fibers get disintegrated into hydrosoluble proteins. These proteins leak through microscopic pores in the anterior lens capsule into the anterior chamber, where they incite an acute inflammatory reaction. Besides the lens proteins get engulfed by the macrophages in the anterior chamber
[2]
Morton SJ, Meirick T, Flanary WE, Oetting TA. Phacolytic Glaucoma due to Morgagnian Cataract. EyeRounds.org. posted April 25, 2018.
[3]
Epstein DL, Jedziniak JA, Grant WM. Identification of heavy molecular-weight soluble protein in aqueous humor in human phacolytic glaucoma. Invest Ophthalmol Vis Sci. 1978; 17: 398–402.
[2, 3]
. Both protein-laden macrophages and free proteins clog the trabecular meshwork causing an acute rise in IOP
[1]
Kelly L, Sarwat S. Lens-Induced Glaucoma: Diagnosis and Management. AAO.org. posted October 01, 2016.
[1]
. The prognosis for visual recovery post cataract surgery in PG.
Therefore depends on the period that the IOP has been on the higher side thereby causing a permanent optic nerve damage.
Phacolytic glaucoma often presents as a long-standing visual loss due to hypermature/Morgagnian cataract and acutely with ocular pain, redness, watering and photophobia. Slit lamp examination reveals corneal edema, moderate to severe anterior chamber reaction with or without pseudohypopyon, and multiple white iridescent or hyper refringent particles in the anterior chamber which represent calcium oxalate and cholesterol crystals liberated from the degenerated cataractous lens with wrinkled but intact capsule. Yoo Ha et al. in 2014 used scanning electron microscopy to find these full-thickness dehiscences and holes in the anterior lens capsule despite an intact macroscopic appearance
[2]
Morton SJ, Meirick T, Flanary WE, Oetting TA. Phacolytic Glaucoma due to Morgagnian Cataract. EyeRounds.org. posted April 25, 2018.
[4]
Yoo WS, Kim BJ, Chung IY, Seo SW, Yoo JM, Kim SJ. A case of Phacolytic glaucoma with anterior lens capsule disruption identified by scanning electron microscopy. BMC Ophthalmol. 2014; 14: 133.
[2, 4]
.
Gifford et al in 1900 was the first to reveal a rise in IOP due to hypermature cataracts
[5]
Gifford, H.: Danger of the Spontaneous Cure of Senile Cataract.Am. J. Ophth. 1900; 17: 289-293.
[5]
. However, the term Phacolytic Glaucoma was coined by Flocks et al in 1955 who stated that the lens proteins leak through an intact capsule and incite an inflammatory anterior chamber reaction
[6]
Flocks M, Littwin CS, Zimmerman LE. Phacolytic glaucoma; a clinic-pathologic study of one hundred thirty-eight cases of glaucoma associated with hypermature cataract. AMA Arch Ophthalmol. 1955; 54(1): 37-45.
[6]
. He also stated that protein-laden macrophages cause obstruction of the trabecular meshwork leading to a rise in IOP. Experimental studies by Epstein et al demonstrate that high molecular weight proteins could occlude the trabecular meshwork even in the absence of macrophages
[7]
Epstein DL, Jedziniak JA, Grant WM. Obstruction of aqueous outflow by lens particles and by heavy-molecular-weight soluble lens proteins. Invest Ophthalmol Vis Sci. 1978; 17(3): 272-7.
[7]
.
2. Methods
23 patients diagnosed clinically with phacolytic glaucoma were included in the study after consent. The study was conducted at SKIMS Medical College Hospital, Kashmir between March 2020 and March 2023. The patients presented with a history of long-standing severe diminution of vision and ocular pain and redness for the last 5-10 days. Slit lamp biomicroscopy was done in all the patients to look for corneal edema, anterior chamber reaction, free-floating particles, and shiny crystals in the anterior chamber. Intraocular pressure was measured using Goldmann applanation tonometery and B-Scan Ultrasonography was done in all the patients to look for any posterior segment pathology. Visual acuity was measured, although all the patients presented with vision varying from hand movement to perception of light. Three patients presented with defective projection of light, but were managed surgically as patients with phacolytic glaucoma with severe anterior chamber reaction might present with defective projection of light, but would get some useful vision postoperatively.
After admission, raised IOP was managed with systemic acetazolamide and topical anti-glaucoma medication. Intravenous mannitol 20% was given wherever necessary. The aim of lowering the IOP was to clear the corneal edema to facilitate the surgical procedure which would take 3-5 days. Anterior chamber reaction was managed with topical steroids and cycloplegic eye drops.
The patients were operated upon using either small incision cataract surgery or Phacoemulsification with intraocular lens implantation by a single surgeon. The choice of surgical procedure was decided based on nuclear sclerosis. Since hypermature / morgagnian cataracts usually present with weak zonules, patients with grade IV nuclei were selected for small incision cataract surgery while others were operated on by phacoemulsification procedure.
Post-operatively all the patients were advised topical steroid-antibiotic and cycloplegic eye drops. Systemic steroids were included in patients with severe post-operative uveitic reaction. All the patients were put on topical anti-glaucoma medication varying from 1 - 3 weeks or till the intraocular pressure was normal. All the patients were examined on post-op day 1, day 3, day 8, 2 weeks, 4 weeks, and finally after 8 weeks. The final examination was done about visual acuity, IOP measurement, and any post-operative complications.
3. Results
Table 1. Male: Female distribution.
Total patients
Male
Female
23
9
14
A total of 23 eyes of 23 patients were included in the study, out of which 14 (60.86%) were females and 9 (39.13%) were males.
Table 2. Pre-operative visual acuity.
Total
PR defective
PL, PR accurate
HM
FC
14 FEMALES
2
11
-
1
9 MALES
1
8
-
-
Out of 14 female patients, 11 patients had perception and accurate projection of light, 1 patient had finger counting at 3 meters and 2 patients presented with defective projection of light. Out of 9 male patients, 8 had perception and accurate projection of light, while 1 patient had defective projection of light. All 3 patients (2 females and 1 male) with defective projection of light however underwent cataract extraction with IOL implantation and got useful vision in the post-operative period.
Table 3. Pre-operative IOP.
Total patients
30-40mmHg
24-30mmHg
14 females
12
2
9 males
6
3
Out of 14 females, 12 had IOP from 30 to > 40 mmHg, and 2 had IOP between 24-30 mmHg. Out of 9 males, 6 had IOP from 30 to > 40 mmHg, and 3 had IOP between 24-30 mmHg.
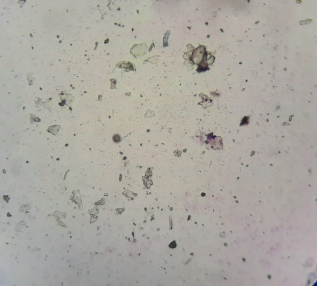
Figure 1. Aqueous tap showing multiple white iridescent or hyper refringent particles which represent calcium oxalate and cholesterol crystals liberated from the degenerated cataractous lens.
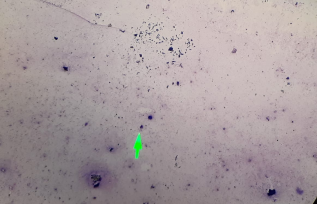
Figure 2. Aqueous tap showing protein-laden macrophages. Proteins being liberated from the degenerated cataractous lens.
Table 4. Post-Operative Visual Acuity.
Total patients
PL-4/60
5/60-6/60
6/60-6/12
14 females
4
7
3
9 males
3
4
2
Post-operatively 21.73% of patients achieved a BCVA between 6/60-6/12, 43.82% had a BCVA of 4/60-6/60 while 30.43% of patients achieved a final BCVA between 4/60 to only perception of light.
Table 5. Post-Operative Complications.
Total patients
Persistent corneal edema
Uveitis with inflammation
14 females
2
3
9 males
1
1
Post-operatively two female and one male patient had persistent corneal edema and despite all conservative measures the corneal edema failed to regress and by six months progressed to corneal decompensation.
Four patients (3 females and 1 male) had moderate to severe post-operative uveitic reaction. However, all the patients responded to systemic steroids and one patient needed YAG Laser membranectomy.
Table 6. Post-Operative IOP.
Total patients
<20
20-23
24-30
14 females
12
1
1
9 males
8
1
-
Post-operatively one female patient persisted with IOP between 24-30 mm Hg despite maximum anti-glaucoma medication and was advised Trabeculectomy. One male and one female patient maintained IOP between 20-23 mm Hg and were kept under regular follow-up for any glaucomatous optic nerve damage. 8 male and 12 female patients had well-controlled IOP below 20 mm Hg.
4. Discussion
Flocks coined the term - Phacolytic glaucoma
[5]
Gifford, H.: Danger of the Spontaneous Cure of Senile Cataract.Am. J. Ophth. 1900; 17: 289-293.
[5]
. Epstein described the role of high-molecular-weight lens protein (HMW-LP) in the pathogenesis of PLG
[6]
Flocks M, Littwin CS, Zimmerman LE. Phacolytic glaucoma; a clinic-pathologic study of one hundred thirty-eight cases of glaucoma associated with hypermature cataract. AMA Arch Ophthalmol. 1955; 54(1): 37-45.
[7]
Epstein DL, Jedziniak JA, Grant WM. Obstruction of aqueous outflow by lens particles and by heavy-molecular-weight soluble lens proteins. Invest Ophthalmol Vis Sci. 1978; 17(3): 272-7.
[6, 7]
. Microdefects in the cataractous lens capsule lead to a progressive leak of the soluble lens proteins into the aqueous humor. The macrophages phagocytose these proteins and block the trabecular meshwork (TM), causing acute open-angle glaucoma
[6]
Flocks M, Littwin CS, Zimmerman LE. Phacolytic glaucoma; a clinic-pathologic study of one hundred thirty-eight cases of glaucoma associated with hypermature cataract. AMA Arch Ophthalmol. 1955; 54(1): 37-45.
[6]
. The recent theory states that HMW-LP directly obstructs the TM to impede the aqueous outflow and precipitates PLG. The increase in the content of HMW-LP in the human lens with increasing age supports this theory.
Phacolytic Glaucoma although less common in the developed world, still poses a challenge for the Ophthalmologists in developing countries like India because of population overload and heavy backlog of cataract patients awaiting surgery.
The majority of surgeons prefer manual small incision cataract surgery (SICS) in phacolytic glaucoma due to possible zonular weakness in hypermature cataracts. However, phacoemulsification is nowadays considered a good choice if zonular weakness is not encountered
[8]
Braganza A, Thomas R, George T. Management of Phacolytic glaucoma: experience of 135 cases. Indian J Ophthalmol. 1998 Sep; 46(3): 139-43.
[9]
Chen TC. Lens-induced glaucoma: surgical techniques and complications. Middle East J Ophthalmol. 2004 May; 12(1): 40-52.
[10]
Venkatesh R, Tan CS, Kumar TT, Ravindran RD. Safety and efficacy of manual small incision cataract surgery for phacolytic glaucoma. Br J Ophthalmol. 2007 Mar; 91(3): 279-81.
[8-10]
.
The duration of acute symptoms of phacolytic glaucoma like ocular pain, redness, watering, and photophobia should be elicited as a delayed presentation by more than 5-7 days results in glaucomatous optic nerve damage and hence poor prognosis. However, a defective projection of light should not be seen as a contraindication for cataract surgery in phacolytic glaucoma patients. In a study by Mandal AK et al, 18 patients out of 45 phacolytic glaucoma patients presented with defective projection of light, and after undergoing cataract extraction with intraocular lens implantation, 44% of such patients regained a visual acuity of 20/40 or better
[11]
Mandal AK, Gothmal VK. Intraocular pressure control and visual outcome in patients with phacolytic glaucoma managed by extracapsular cataract extraction with or without posterior chamber intraocular lens implantation. Ophthalmic Surg Lasers. 1998 Nov; 29(11): 880-9.
[11]
. Almost similar results were found in our study where 3 patients with defective projection of light achieved useful vision after undergoing cataract surgery.
A study by Rajkumar P et al and Shrestha R et al showed female patients out-number males in both phacolytic glaucoma and phacomorphic glaucoma which could be due to social and cultural constraints. Similar results with females 60.86% would outnumber males 39.13% in our study
[12]
Rajkumar P, Suryachandra M. A Clinical study on lens induced glaucoma and its visual outcome in patients visiting RIMS, Srikakulam. Journal of Evolution of Medical and Dental Sciences. 2015 Jul 23; 4(59): 10294–10300.
[13]
Shrestha R, Godar M, Gurung S, Devkote P, Manandhar L D, Shrestha N. Lens in a tertiary eye care center in Western Nepal. Nepal J Ophthalmol. 2019; 11(22): 115–145.
[12, 13]
.
A prospective study by Sarkar K C et al showed that 72.2% of phacolytic glaucoma patients achieved a BCVA of more than 20/125 at final follow-up
[14]
Sarkar KC, Sarkar P, Das J. Clinical profile of lens induced glaucoma patients in a tertiary care center - A prospective study. Indian J Clin Exp Ophthalmol. 2018; 4(1): 36–39.
[14]
. Gnanadurai JSC et al analyzed the visual recovery in phacolytic glaucoma patients and found visual acuity of more than 6/12 in 56% of patients presenting within 5 days of symptoms
[15]
Gnanadurai JSC, Sanjana EF, Radhakrishnan M. Factors affecting visual outcome in phacolytic glaucoma. International journal of scientific study. 2016; 3(11): 24-27.
[15]
. However, the visual recovery was less than 6/60 in patients presenting beyond 10 days of symptoms. He also attributed poor visual acuity to glaucomatous optic neuropathy and persistent corneal odema in such patients. In our study, however only 21.73% of patients achieved a BCVA of 6/60 – 6/12, 47.82% achieved a BCVA of 4/60 – 6/60 and 30.43% of patients had a final BCVA of less than 4/60 to only perception of light. This low visual recovery could be due to late presentation and hence permanent glaucomatous damage.
In a study by Nannaware SL et al, 53% of phacolytic glaucoma patients present with visual acuity of perception of light, and 47% present with a vision of Hand movements
[16]
Nannaware SL, Singasandra SM, Mallaiah D, Venkataswamy SB. Management and visual outcome in patients of phacolytic glaucoma at a tertiary eye care hospital. IP International journal of ocular oncology and oculoplasty,2021; 7(4): 372-377.
[16]
. After surgery, 63% of patients achieved a BCVA of 6/6 – 6/12, 27% of patients achieved 6/18 – 6/60 and 3% of patients achieved a BCVA of less than 6/60.
In Phacolytic glaucoma, the correlation between IOP and visual outcomes is significant both clinically and statistically as patients with pre-operative IOP of more than 40 mm Hg have a poor visual outcome as compared to patients with pre-operative IOP of less than 30 mm Hg where the visual recovery is significantly better, This could be the reason for a poor BCVA between 6/60 -6/12 in only 21.73% of patients in our study where an IOP between 30 to more than 40 mmHg was seen in 78.26% of patients at the time of presentation.
5. Conclusion
This study concludes that all patients of phacolytic glaucoma should be operated upon for cataract extraction using either small incision cataract surgery (SICS) or Phacoemulsification procedure, irrespective of the pre-operative visual status. However, if the patients present within 5 days of the symptoms, chances of achieving good post-operative visual acuity are high. Similarly, if the presenting intraocular pressures are very high or more than 40 mm Hg, the chances of glaucomatous optic nerve damage are also high with resultant poor post-operative visual recovery.
Conflicts of Interest
The author declares no conflicts of interest.
References
[1]
Kelly L, Sarwat S. Lens-Induced Glaucoma: Diagnosis and Management. AAO.org. posted October 01, 2016.
[2]
Morton SJ, Meirick T, Flanary WE, Oetting TA. Phacolytic Glaucoma due to Morgagnian Cataract. EyeRounds.org. posted April 25, 2018.
[3]
Epstein DL, Jedziniak JA, Grant WM. Identification of heavy molecular-weight soluble protein in aqueous humor in human phacolytic glaucoma. Invest Ophthalmol Vis Sci. 1978; 17: 398–402.
[4]
Yoo WS, Kim BJ, Chung IY, Seo SW, Yoo JM, Kim SJ. A case of Phacolytic glaucoma with anterior lens capsule disruption identified by scanning electron microscopy. BMC Ophthalmol. 2014; 14: 133.
[5]
Gifford, H.: Danger of the Spontaneous Cure of Senile Cataract.Am. J. Ophth. 1900; 17: 289-293.
[6]
Flocks M, Littwin CS, Zimmerman LE. Phacolytic glaucoma; a clinic-pathologic study of one hundred thirty-eight cases of glaucoma associated with hypermature cataract. AMA Arch Ophthalmol. 1955; 54(1): 37-45.
[7]
Epstein DL, Jedziniak JA, Grant WM. Obstruction of aqueous outflow by lens particles and by heavy-molecular-weight soluble lens proteins. Invest Ophthalmol Vis Sci. 1978; 17(3): 272-7.
[8]
Braganza A, Thomas R, George T. Management of Phacolytic glaucoma: experience of 135 cases. Indian J Ophthalmol. 1998 Sep; 46(3): 139-43.
[9]
Chen TC. Lens-induced glaucoma: surgical techniques and complications. Middle East J Ophthalmol. 2004 May; 12(1): 40-52.
[10]
Venkatesh R, Tan CS, Kumar TT, Ravindran RD. Safety and efficacy of manual small incision cataract surgery for phacolytic glaucoma. Br J Ophthalmol. 2007 Mar; 91(3): 279-81.
[11]
Mandal AK, Gothmal VK. Intraocular pressure control and visual outcome in patients with phacolytic glaucoma managed by extracapsular cataract extraction with or without posterior chamber intraocular lens implantation. Ophthalmic Surg Lasers. 1998 Nov; 29(11): 880-9.
[12]
Rajkumar P, Suryachandra M. A Clinical study on lens induced glaucoma and its visual outcome in patients visiting RIMS, Srikakulam. Journal of Evolution of Medical and Dental Sciences. 2015 Jul 23; 4(59): 10294–10300.
[13]
Shrestha R, Godar M, Gurung S, Devkote P, Manandhar L D, Shrestha N. Lens in a tertiary eye care center in Western Nepal. Nepal J Ophthalmol. 2019; 11(22): 115–145.
[14]
Sarkar KC, Sarkar P, Das J. Clinical profile of lens induced glaucoma patients in a tertiary care center - A prospective study. Indian J Clin Exp Ophthalmol. 2018; 4(1): 36–39.
[15]
Gnanadurai JSC, Sanjana EF, Radhakrishnan M. Factors affecting visual outcome in phacolytic glaucoma. International journal of scientific study. 2016; 3(11): 24-27.
[16]
Nannaware SL, Singasandra SM, Mallaiah D, Venkataswamy SB. Management and visual outcome in patients of phacolytic glaucoma at a tertiary eye care hospital. IP International journal of ocular oncology and oculoplasty,2021; 7(4): 372-377.
Bashir, S. A., Lone, I. A., Wani, F. M., Sumaiya, Q. A. (2024). A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma. International Journal of Ophthalmology & Visual Science, 9(1), 8-12. https://doi.org/10.11648/j.ijovs.20240901.12
Bashir, S. A.; Lone, I. A.; Wani, F. M.; Sumaiya, Q. A. A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma. Int. J. Ophthalmol. Vis. Sci.2024, 9(1), 8-12. doi: 10.11648/j.ijovs.20240901.12
Bashir SA, Lone IA, Wani FM, Sumaiya QA. A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma. Int J Ophthalmol Vis Sci. 2024;9(1):8-12. doi: 10.11648/j.ijovs.20240901.12
@article{10.11648/j.ijovs.20240901.12,
author = {Sheikh Asma Bashir and Imtiyaz Ahmad Lone and Fayka Mohi-Ud-Din Wani and Qazi Afshana Sumaiya},
title = {A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma
},
journal = {International Journal of Ophthalmology & Visual Science},
volume = {9},
number = {1},
pages = {8-12},
doi = {10.11648/j.ijovs.20240901.12},
url = {https://doi.org/10.11648/j.ijovs.20240901.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijovs.20240901.12},
abstract = {Purpose: To evaluate the visual recovery and intraocular pressure control after cataract surgery in patients of phacolytic glaucoma. Methods: 23 patients diagnosed clinically as phacolytic glaucoma and included in the study were operated upon using either SICS or Phacoemulsification procedure after lowering of the Intraocular pressure (IOP) and control of ocular inflammation. Results: Post-operatively 21.73% of patients achieved a best corrected visual acuity (BCVA) of 6/60-6/12, 43.82% had a BCVA of 4/60-6/60 and 30.43% achieved a final BCVA between 4/60 to only perception of light. However 86.95% of patients maintained an IOP less than 20 mm Hg, 8.69% had an IOP between 20-23 mm Hg and 4.34% had an IOP between 24-30 mm Hg requiring a Glaucoma filtering surgery. Conclusion: Patients of Phacolytic Glaucoma if present at an early stage can have a good visual recovery and well controlled IOP in the post-operative period.
},
year = {2024}
}
TY - JOUR
T1 - A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma
AU - Sheikh Asma Bashir
AU - Imtiyaz Ahmad Lone
AU - Fayka Mohi-Ud-Din Wani
AU - Qazi Afshana Sumaiya
Y1 - 2024/05/24
PY - 2024
N1 - https://doi.org/10.11648/j.ijovs.20240901.12
DO - 10.11648/j.ijovs.20240901.12
T2 - International Journal of Ophthalmology & Visual Science
JF - International Journal of Ophthalmology & Visual Science
JO - International Journal of Ophthalmology & Visual Science
SP - 8
EP - 12
PB - Science Publishing Group
SN - 2637-3858
UR - https://doi.org/10.11648/j.ijovs.20240901.12
AB - Purpose: To evaluate the visual recovery and intraocular pressure control after cataract surgery in patients of phacolytic glaucoma. Methods: 23 patients diagnosed clinically as phacolytic glaucoma and included in the study were operated upon using either SICS or Phacoemulsification procedure after lowering of the Intraocular pressure (IOP) and control of ocular inflammation. Results: Post-operatively 21.73% of patients achieved a best corrected visual acuity (BCVA) of 6/60-6/12, 43.82% had a BCVA of 4/60-6/60 and 30.43% achieved a final BCVA between 4/60 to only perception of light. However 86.95% of patients maintained an IOP less than 20 mm Hg, 8.69% had an IOP between 20-23 mm Hg and 4.34% had an IOP between 24-30 mm Hg requiring a Glaucoma filtering surgery. Conclusion: Patients of Phacolytic Glaucoma if present at an early stage can have a good visual recovery and well controlled IOP in the post-operative period.
VL - 9
IS - 1
ER -
Bashir, S. A., Lone, I. A., Wani, F. M., Sumaiya, Q. A. (2024). A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma. International Journal of Ophthalmology & Visual Science, 9(1), 8-12. https://doi.org/10.11648/j.ijovs.20240901.12
Bashir, S. A.; Lone, I. A.; Wani, F. M.; Sumaiya, Q. A. A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma. Int. J. Ophthalmol. Vis. Sci.2024, 9(1), 8-12. doi: 10.11648/j.ijovs.20240901.12
Bashir SA, Lone IA, Wani FM, Sumaiya QA. A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma. Int J Ophthalmol Vis Sci. 2024;9(1):8-12. doi: 10.11648/j.ijovs.20240901.12
@article{10.11648/j.ijovs.20240901.12,
author = {Sheikh Asma Bashir and Imtiyaz Ahmad Lone and Fayka Mohi-Ud-Din Wani and Qazi Afshana Sumaiya},
title = {A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma
},
journal = {International Journal of Ophthalmology & Visual Science},
volume = {9},
number = {1},
pages = {8-12},
doi = {10.11648/j.ijovs.20240901.12},
url = {https://doi.org/10.11648/j.ijovs.20240901.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijovs.20240901.12},
abstract = {Purpose: To evaluate the visual recovery and intraocular pressure control after cataract surgery in patients of phacolytic glaucoma. Methods: 23 patients diagnosed clinically as phacolytic glaucoma and included in the study were operated upon using either SICS or Phacoemulsification procedure after lowering of the Intraocular pressure (IOP) and control of ocular inflammation. Results: Post-operatively 21.73% of patients achieved a best corrected visual acuity (BCVA) of 6/60-6/12, 43.82% had a BCVA of 4/60-6/60 and 30.43% achieved a final BCVA between 4/60 to only perception of light. However 86.95% of patients maintained an IOP less than 20 mm Hg, 8.69% had an IOP between 20-23 mm Hg and 4.34% had an IOP between 24-30 mm Hg requiring a Glaucoma filtering surgery. Conclusion: Patients of Phacolytic Glaucoma if present at an early stage can have a good visual recovery and well controlled IOP in the post-operative period.
},
year = {2024}
}
TY - JOUR
T1 - A Study of Visual Rehabilitation and Intraocular Pressure Control in Phacolytic Glaucoma
AU - Sheikh Asma Bashir
AU - Imtiyaz Ahmad Lone
AU - Fayka Mohi-Ud-Din Wani
AU - Qazi Afshana Sumaiya
Y1 - 2024/05/24
PY - 2024
N1 - https://doi.org/10.11648/j.ijovs.20240901.12
DO - 10.11648/j.ijovs.20240901.12
T2 - International Journal of Ophthalmology & Visual Science
JF - International Journal of Ophthalmology & Visual Science
JO - International Journal of Ophthalmology & Visual Science
SP - 8
EP - 12
PB - Science Publishing Group
SN - 2637-3858
UR - https://doi.org/10.11648/j.ijovs.20240901.12
AB - Purpose: To evaluate the visual recovery and intraocular pressure control after cataract surgery in patients of phacolytic glaucoma. Methods: 23 patients diagnosed clinically as phacolytic glaucoma and included in the study were operated upon using either SICS or Phacoemulsification procedure after lowering of the Intraocular pressure (IOP) and control of ocular inflammation. Results: Post-operatively 21.73% of patients achieved a best corrected visual acuity (BCVA) of 6/60-6/12, 43.82% had a BCVA of 4/60-6/60 and 30.43% achieved a final BCVA between 4/60 to only perception of light. However 86.95% of patients maintained an IOP less than 20 mm Hg, 8.69% had an IOP between 20-23 mm Hg and 4.34% had an IOP between 24-30 mm Hg requiring a Glaucoma filtering surgery. Conclusion: Patients of Phacolytic Glaucoma if present at an early stage can have a good visual recovery and well controlled IOP in the post-operative period.
VL - 9
IS - 1
ER -