Psittacosis, an infectious disease caused by Chlamydia psittaci, has clinical manifestations ranging from asymptomatic infection to severe atypical pneumonia, and even rare fatal meningitis. Psittacosis is difficult to identify early due to its nonspecific clinical presentation. In this report, we describe a male patient with atypical severe pneumonia and meningitis caused by Chlamydia psittacosis. The patient presented to the Department of Neurology with a fever for 5 days, abnormal mental behavior for 5 h, and no history of avian or poultry exposure. Following empirical antimicrobial therapy, the patient’s condition deteriorated rapidly, and he suffered respiratory failure, shock, and psychiatric disorders. The patient was rapidly transferred to ICU, where he received antishock, invasive mechanical ventilation therapy, and organ support therapy. Sputum and cerebrospinal fluid metagenomic secondary sequencing (mNGS) identified sequence reads related to Chlamydia thermosum. The patient was administered targeted drugs, as well as fluoroquinolone antimicrobial agents. As a result, the patient improved and left the ICU after 25 days, before returning to a near-premorbid condition after discharge. Psittacosis and meningitis should be considered in patients suffering from atypical pneumonia with fever, headache, and neuropsychiatric symptoms, and mNGS is a useful test for etiological screening. The case reports in this study hopefully help to provide some references for earlier diagnosis of psittacosis and development of life-saving treatment plan.
| Published in | International Journal of Medical Case Reports (Volume 4, Issue 1) |
| DOI | 10.11648/j.ijmcr.20250401.12 |
| Page(s) | 7-16 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Psittacosis, Chlamydia Psittaci, Severe Pneumonia, Meningitis, Metagenomic Sequencing
Laboratory projects | Result | Normal range of value |
|---|---|---|
RBC | 3.59×10^12/L; | (4.0-5.5)×10^12 |
HGB | 122 g/L | 120-160 |
WBC | 2.58×10^9/L | (4.0-10.0)×10^9 |
NEUT ratio | 93.30% | 50%-70% |
PLT | 148 × 10^9/ L | (100-300)×10^9 |
CRP | >200.0 mg/L | 0.0-10.0 |
SAA | >600.0 mg/L | 0.0-10.0 |
PCT | >100.0 ng/ml | 0.0-0.05 |
intracranial pressure | 450 mmH2O | 80-180 |
CSF biochemical protein quantification | 134 mg/L | 150-450 |
CSF glucose | 5.23 mmol/L | 2.5-4.4 |
CSF chloride | 144.1 mmol/L | 120-130 |
CSF of ADA | 1 U/L | 0-8.0 |
CSF of LDH | 38 U/L | 0-4.0 |
CSF of complement C3 | 0.01 g/L | 0.005-0.009 |
CSF of complement C4 | 0 g/L | 0.005-0.009 |
CSF of IgG | 0.09 g/L | 0.01-004 |
CSF of RBC | 20×10^6/L | 0-0.0 |
CSF of WBC | 2×10^6/L | (0-8.0)×10^6 |
CSF of blood serum bacterial endotoxin | 0.031 EU/mL | 0-0.11 |
G test | <37.500 pg/mL | 0-70.0 |
total bilirubin | 23.6 umol/L | 0.0-21.0 |
direct bilirubin | 14 umol/L | 1.70-6.80 |
ALT | 70 U/L | 7.0-40.0 |
AST | 346 U/L | 13.0-35.0 |
ALB | 26.6 g/L | 40.0-55.0 |
creatinine | 86.3 umol/L | 44.0-115.0 |
CK | 9874.0 U/L | 40.0-200.0 |
CK-MB | 105 U/L | 0.0-24.0 |
HBD | 693.5 U/L | 76.0-195.0 |
LDH | 1084 U/L | 120.0-250.0 |
pH | 7.227 | 7.35-7.45 |
PCO2 | 33.9 mmHg | 35-45 |
PO2 | 145 mmHg | 80-100 |
lactate | 8.9 mmol/L | 0.5-2.0 |
mNGS | Metagenomic Secondary Sequencing |
CSF | Cerebrospinal Fluid |
RBC | Red Blood Cell |
HGB | Hemoglobin |
WBC | White Blood Cell |
PLT | Platelet |
CRP | C-reactive Protein |
SAA | Serum Amyloid A Protein |
PCT | Procalcitonin |
CT | Computed Tomography |
ICU | Intensive Care Unit |
APACHE-II | Acute Physiology and Chronic Health Evaluation |
SOFA | Sepsis Related Organ Failure Assessment |
ADA | Adenosine Deaminase |
LDH | Lactate Dehydrogenase |
G test | Fungal D-glucan Detection |
ALT | Alanine Transaminase |
AST | Aspartate Aminotransferase |
ALB | Albumin |
HBD | Hydroxybutyric Dehydrogenase |
BALF | Bronchoalveolar Lavage Fluid |
PCR | Polymerase Chain Reaction |
| [1] | Kozuki E, Arima Y, Matsui T, et al. Human psittacosis in Japan: notification trends and differences in infection source and age distribution by gender, 2007 to 2016. Ann Epidemiol. 2020; 44: 60-63. |
| [2] | Hogerwerf L, DE Gier B, Baan B, VAN DER Hoek W. Chlamydia psittaci (psittacosis) as a cause of community-acquired pneumonia: a systematic review and meta-analysis. Epidemiol Infect. 2017; 145(15): 3096-3105. |
| [3] | Cheng Y-J, Lin K-Y, Chen C-C, Huang Y-L, Liu C-E, Li S-Y. Zoonotic atypical pneumonia due to Chlamydophila psittaci: first reported psittacosis case in Taiwan. J Formos Med Assoc. 2013; 112(7): 430-3. |
| [4] | Shaw KA, Szablewski CM, Kellner S, Kornegay L, Bair P, Brennan S, et al. Psittacosis outbreak among workers at chicken slaughter plants, Virginia and Shi et al. BMC Infectious Diseases (2021) 21: 621Page 7 of 8Georgia, USA, 2018. Emerg Infect Dis. 2019; 25(11): 2143-5. |
| [5] | Branley JM, Weston KM, England J, Dwyer DE, Sorrell TC. Clinical features of endemic community-acquired psittacosis. New Microbe New Infect. 2014; 2(1): 7-12. |
| [6] | Yung AP, Lindsay GM. Psittacosis - a review of 135 cases. Med J. 1988; 148: 228-33. |
| [7] | Chen X, Cao K, Wei Y, et al. Metagenomic next-generation sequencing in the diagnosis of severe pneumonias caused by Chlamydia psittaci. Infection. 2020; 48(4): 535-542. |
| [8] | Peng Li, Lihua Song, Jinhua Miao. Progress in the pathogenic mechanism of Chlamydia psittaci. International Journal of Laboratory Medicine, 2016, 37(06): 780-782. |
| [9] | Zeidler H, Kuipers J, Köhler L. Chlamydia-induced arthritis. Curr Opin Rheumatol. 2004; 16(4): 380-392. |
| [10] | Mingyi Shu, Zhongyu Li. Progress in studying the pathogenic mechanism of Chlamydia. The Chinese Journal of Zoonosis, 2021, 37(06): 542-547. |
| [11] | Elwell C, Mirrashidi K, Engel J. Chlamydia cell biology and pathogenesis. Nat Rev Microbiol. 2016; 14(6): 385-400. |
| [12] | Radomski N, Einenkel R, Müller A, Knittler MR. Chlamydia-host cell interaction not only from a bird's eye view: some lessons from Chlamydia psittaci. FEBS Lett. 2016; 590(21): 3920-3940. |
| [13] | Balsamo G, Maxted AM, Midla JW, et al. Compendium of Measures to Control Chlamydia psittaci Infection Among Humans (Psittacosis) and Pet Birds (Avian Chlamydiosis), 2017. J Avian Med Surg. 2017; 31(3): 262-282. |
| [14] | Spoorenberg SM, Bos WJ, van Hannen EJ, et al. Chlamydia psittaci: a relevant cause of community-acquired pneumonia in two Dutch hospitals. Neth J Med. 2016; 74(2): 75-81. |
| [15] | Stewardson AJ, Grayson ML. Psittacosis. Infect Dis Clin N Am. 2010; 24(1): 7-25. |
| [16] | Katsura D, Tsuji S, Kimura F, Tanaka T, Eguchi Y, Murakami T. Gestational psittacosis: a case report and literature review. J Obstet Gynaecol Research. 2020; 46(5): 673-7. |
| [17] | Jin W, Liang R, Tian X, Cheng Y, Kong X, He F, Zhang C, Wang G, Li S, Lu H, Sun S, Shen L. Clinical features of psittacosis in 46 Chinese patients. Enferm Infecc Microbiol Clin (Engl Ed). 2023 Nov; 41(9): 545-548. |
| [18] | Stidham RA, Richmond-Haygood M. Case report: Possible psittacosis in a military family member-clinical and public health management issues in military settings. MSMR. 2019; 26(7): 2-7. |
| [19] | Fraeyman A, Boel A, Van Vaerenbergh K, De Beenhouwer H. Atypical pneumonia due to Chlamydophila psittaci: 3 case reports and review of literature. Acta Clin Belg. 2010; 65(3): 192-196. |
| [20] | Cunha BA. The atypical pneumonias: clinical diagnosis and importance. Clin Microbiol Infect. 2006; 12 Suppl 3: 12-24. |
| [21] | Corsaro D, Greub G. Pathogenic potential of novel Chlamydiae and diagnostic approaches to infections due to these obligate intracellular bacteria. Clin Microbiol Rev. 2006; 19(2): 283-297. |
| [22] | Nieuwenhuizen AA, Dijkstra F, Notermans DW, van der Hoek W. Laboratory methods for case finding in human psittacosis outbreaks: a systematic review. BMC Infect Dis. 2018; 18(1): 442. Published 2018 Aug 30. |
| [23] | Gu W, Miller S, Chiu CY. Clinical Metagenomic Next-Generation Sequencing for Pathogen Detection. Annu Rev Pathol. 2019; 14: 319-338. |
| [24] | Brown JR, Bharucha T, Breuer J. Encephalitis diagnosis using metagenomics: application of next generation sequencing for undiagnosed cases. J Infect. 2018; 76(3): 225-240. |
| [25] | Gu L, Liu W, Ru M, et al. The application of metagenomic next-generation sequencing in diagnosing Chlamydia psittaci pneumonia: a report of five cases. BMC Pulm Med. 2020; 20(1): 65. Published 2020 Mar 17. |
| [26] | Langelier C, Kalantar KL, Moazed F, et al. Integrating host response and unbiased microbe detection for lower respiratory tract infection diagnosis in critically ill adults. Proc Natl Acad Sci U S A. 2018; 115(52): E12353-E12362. |
| [27] | Kohlhoff SA, Hammerschlag MR. Treatment of Chlamydial infections: 2014 update. Expert Opin Pharmacother. 2015; 16(2): 205-212. |
| [28] | Drysdale MJ, Lentzen G, Matassova N, Murchie AI, Aboul-Ela F, Afshar M. RNA as a drug target. Prog Med Chem. 2002; 39: 73-119. |
| [29] | NI Y, ZHONG H, GU Y, et al. Clinical Features, Treatment, and Outcome of Psittacosis Pneumonia: A Multicenter Study [J]. Open Forum Infect Dis, 2023, 10(2): ofac518. |
APA Style
Sheng, S., Lin, Z., Li, L., Zhuang, Z., Yang, C., et al. (2025). Psittacosis with Abnormal Mental Behavior: A Rare Case Report and Literature Review. International Journal of Medical Case Reports, 4(1), 7-16. https://doi.org/10.11648/j.ijmcr.20250401.12
ACS Style
Sheng, S.; Lin, Z.; Li, L.; Zhuang, Z.; Yang, C., et al. Psittacosis with Abnormal Mental Behavior: A Rare Case Report and Literature Review. Int. J. Med. Case Rep. 2025, 4(1), 7-16. doi: 10.11648/j.ijmcr.20250401.12
AMA Style
Sheng S, Lin Z, Li L, Zhuang Z, Yang C, et al. Psittacosis with Abnormal Mental Behavior: A Rare Case Report and Literature Review. Int J Med Case Rep. 2025;4(1):7-16. doi: 10.11648/j.ijmcr.20250401.12
@article{10.11648/j.ijmcr.20250401.12,
author = {Shanfeng Sheng and Zhaohua Lin and Lianmao Li and Zhiquan Zhuang and Chunqiong Yang and Zheng Li},
title = {Psittacosis with Abnormal Mental Behavior: A Rare Case Report and Literature Review},
journal = {International Journal of Medical Case Reports},
volume = {4},
number = {1},
pages = {7-16},
doi = {10.11648/j.ijmcr.20250401.12},
url = {https://doi.org/10.11648/j.ijmcr.20250401.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmcr.20250401.12},
abstract = {Psittacosis, an infectious disease caused by Chlamydia psittaci, has clinical manifestations ranging from asymptomatic infection to severe atypical pneumonia, and even rare fatal meningitis. Psittacosis is difficult to identify early due to its nonspecific clinical presentation. In this report, we describe a male patient with atypical severe pneumonia and meningitis caused by Chlamydia psittacosis. The patient presented to the Department of Neurology with a fever for 5 days, abnormal mental behavior for 5 h, and no history of avian or poultry exposure. Following empirical antimicrobial therapy, the patient’s condition deteriorated rapidly, and he suffered respiratory failure, shock, and psychiatric disorders. The patient was rapidly transferred to ICU, where he received antishock, invasive mechanical ventilation therapy, and organ support therapy. Sputum and cerebrospinal fluid metagenomic secondary sequencing (mNGS) identified sequence reads related to Chlamydia thermosum. The patient was administered targeted drugs, as well as fluoroquinolone antimicrobial agents. As a result, the patient improved and left the ICU after 25 days, before returning to a near-premorbid condition after discharge. Psittacosis and meningitis should be considered in patients suffering from atypical pneumonia with fever, headache, and neuropsychiatric symptoms, and mNGS is a useful test for etiological screening. The case reports in this study hopefully help to provide some references for earlier diagnosis of psittacosis and development of life-saving treatment plan.},
year = {2025}
}
TY - JOUR T1 - Psittacosis with Abnormal Mental Behavior: A Rare Case Report and Literature Review AU - Shanfeng Sheng AU - Zhaohua Lin AU - Lianmao Li AU - Zhiquan Zhuang AU - Chunqiong Yang AU - Zheng Li Y1 - 2025/02/17 PY - 2025 N1 - https://doi.org/10.11648/j.ijmcr.20250401.12 DO - 10.11648/j.ijmcr.20250401.12 T2 - International Journal of Medical Case Reports JF - International Journal of Medical Case Reports JO - International Journal of Medical Case Reports SP - 7 EP - 16 PB - Science Publishing Group SN - 2994-7049 UR - https://doi.org/10.11648/j.ijmcr.20250401.12 AB - Psittacosis, an infectious disease caused by Chlamydia psittaci, has clinical manifestations ranging from asymptomatic infection to severe atypical pneumonia, and even rare fatal meningitis. Psittacosis is difficult to identify early due to its nonspecific clinical presentation. In this report, we describe a male patient with atypical severe pneumonia and meningitis caused by Chlamydia psittacosis. The patient presented to the Department of Neurology with a fever for 5 days, abnormal mental behavior for 5 h, and no history of avian or poultry exposure. Following empirical antimicrobial therapy, the patient’s condition deteriorated rapidly, and he suffered respiratory failure, shock, and psychiatric disorders. The patient was rapidly transferred to ICU, where he received antishock, invasive mechanical ventilation therapy, and organ support therapy. Sputum and cerebrospinal fluid metagenomic secondary sequencing (mNGS) identified sequence reads related to Chlamydia thermosum. The patient was administered targeted drugs, as well as fluoroquinolone antimicrobial agents. As a result, the patient improved and left the ICU after 25 days, before returning to a near-premorbid condition after discharge. Psittacosis and meningitis should be considered in patients suffering from atypical pneumonia with fever, headache, and neuropsychiatric symptoms, and mNGS is a useful test for etiological screening. The case reports in this study hopefully help to provide some references for earlier diagnosis of psittacosis and development of life-saving treatment plan. VL - 4 IS - 1 ER -
Wuming School of Clinical Medicine of Guangxi Medical University, Guangxi Medical University, Nanning, China
Wuming Hospital of Guangxi Medical University, Guangxi Medical University, Nanning, China
Wuming Hospital of Guangxi Medical University, Guangxi Medical University, Nanning, China
Wuming Hospital of Guangxi Medical University, Guangxi Medical University, Nanning, China
Wuming Hospital of Guangxi Medical University, Guangxi Medical University, Nanning, China
Wuming Hospital of Guangxi Medical University, Guangxi Medical University, Nanning, China
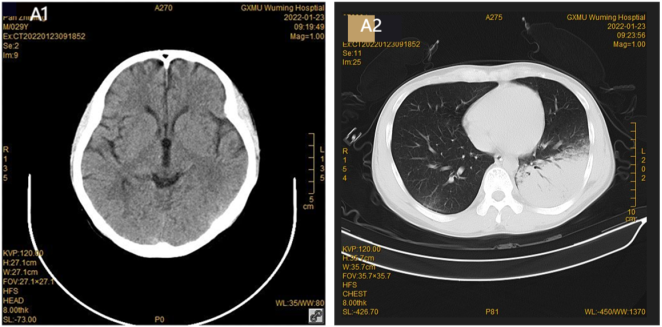
Figure 1. No A1 abnormal findings of cranial CT on admission. Sheet and plaque changes of the lower lobe of A2 lungs, and tracheal shadow on the left side.

Figure 2. Patient PO2/FiO2 trend chart of treatment changes in the ICU.
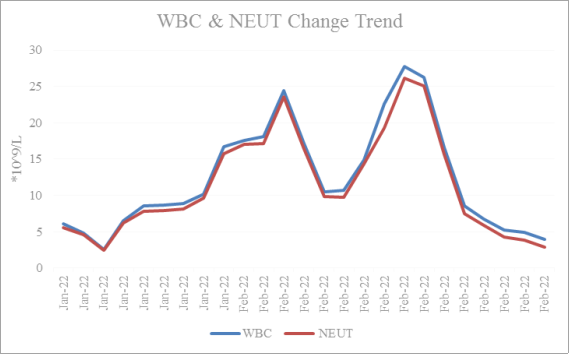
Figure 3. Trend ends of leukocytes (WBC) and neutrophils (NEUT).
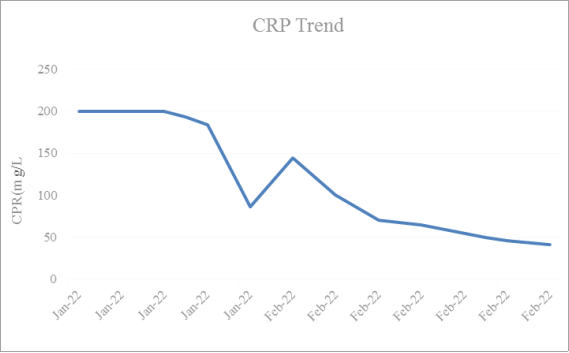
Figure 4. Trend chart of patients C-reactive protein (CRP).
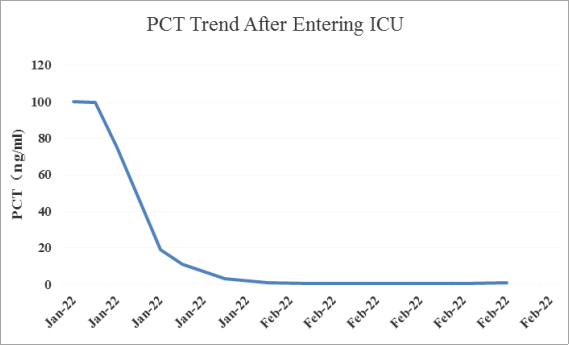
Figure 5. Patient change trend diagram of procalcitonin (PCT).
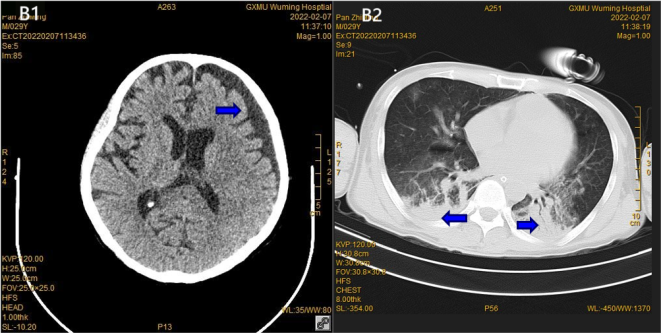
Figure 6. Review of B1 cranial CT after 15 days showed a small amount of subdural effusion in the left frontotemporal region. The corresponding brain parenchyma was shifted medially, the brain parenchyma density was normal, the ventricle, cisterna and sulcus morphology were normal, and the B2 pulmonary lesions increased on the right side and decreased on the left side.
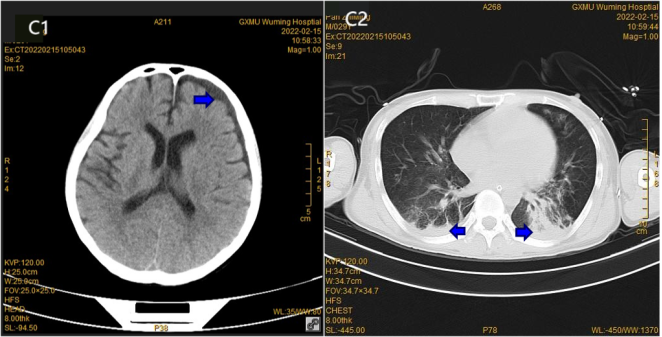
Figure 7. Left frontal and temporal subdural effusion of C1 showed a decrease after 23 days, and the C2 lung inflammation was improved compared to the anterior absorption.
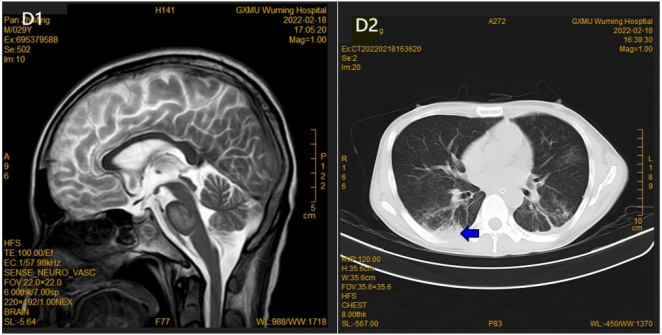
Figure 8. D1 MR subdural effusion was absorbed after 26 days; subacute cerebral infarction was suspected, and D2 inflammation of lungs was also absorbed.
Information

