Introduction: Drug-resistant TB poses a significant threat to global TB care and prevention and remains a major public health issue in many countries and Testicular drug-resistant tuberculosis (testicular DR-TB) refers to a form of tuberculosis that specifically affects the testicles and is resistant to standard anti-TB medications, isolated testicular involvement is uncommon. Case presentation: a twenty-seven-year-old male patient presented with painful swelling of the scrotum for one month. He was treated with first-line anti-TB (RHZE/RH) and completed a month back at the health center. He had a similar complaint during the first diagnosis. While he was on treatment, the swelling subsided and recurred while he discontinued the medication. Our hospital received a referral for this complaint. Otherwise, he has no history of chronic illness, no surgical procedure at any site, no usage of second-line anti-TB drugs, or contact with a DR-TB patient. During the presentation, his vital signs were within normal range. The only pertinent finding was in the genitourinary system, which is that the scrotum is swollen and tender. Following clinical examinations and investigation findings with the diagnosis of RR-EPTB (testicular TB), we put him on an individualized longer regimen (Lfx/Cs/Cfz/Bdq/Cfz/Lzd) and pyridoxine. After 18 months of treatment, the outcome is declared as completed. After being advised on danger signs, he was appointed after six months for post-treatment follow-up according to the Ethiopian DR-TB management protocol. Conclusion: This case highlights the importance of timely diagnosis and adherence to treatment in managing drug-resistant extrapulmonary tuberculosis (RR-EPTB), specifically testicular TB. The patient's recurrent symptoms following discontinuation of first-line anti-TB therapy illustrate the challenges faced in treatment adherence and the potential consequences of inadequate management.
| Published in | International Journal of Medical Case Reports (Volume 4, Issue 1) |
| DOI | 10.11648/j.ijmcr.20250401.11 |
| Page(s) | 1-6 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
DR-TB, Testicular TB, EPTB, Case Report, Ethiopia
Date | 05/01/2023 | 01/09/2023 | 01/12/2023 | 09/21/2023 | 11/20/2023 | 03/21/2024 | |
|---|---|---|---|---|---|---|---|
CBC | WBC (x 10³) | 8.9 | 5.44 | 5.7 | |||
L/N (%) | 15.9/69 | 31.4/57.2 | 33/54 | ||||
Hg/HCT | 17/47.7 | 16/46 | 14.6/37.7 | ||||
MCV/MCH | 91.5/32.6 | 92/35 | |||||
Platelet (x 10³) | 230 | 168 | 121 | ||||
RFT | Urea (mg/dL) | 20 | 17 | 15 | 16.4 | 17 | |
Cr. (mg/dL) | 0.89 | 0.42 | 0.82 | 0.96 | 1.1 | ||
LFT | GOT (U/L) | 20 | 117.5 | 19.6 | 71 | 30 | |
GPT (U/L) | 13 | 64.3 | 11.1 | 7 | |||
ALP (U/L) | 119 | 64 | 109 | 120 | |||
Bil D/T (mg/dL) | 0.24/0.6 | 0.3/0.7 | 0.2/0.5 | 0.38/0.43 | |||
Serum alb. (g/dL) | --- | --- | --- | 3.4 | |||
Visual Acuity | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 | 6/6 | |
ECG (02/07/2023) | Sinus rhythm | ||||||
Genexpert from the scrotal Abscess (01/13/2023) | MTB detected and Rifampicin resistance | ||||||
PICT (01/19/2023) | Non-reactive | ||||||
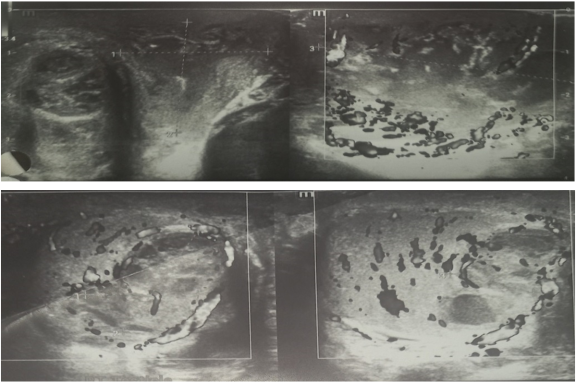
Inguino-scrotal ultrasound (01/09/2023) (figure 1) | Findings: There are right testicular two locules of hypoechoic collections seen with internal debris seen measured 0.83 cm by 0.75 cm and 0.86 cm by 0.61 cm. there are bilateral testicle microcalcifications seen. There are multiple locules of hypoechoic collections the largest measured 2.68 cm by 1.43 cm with internal debris and peripheral fat stranding seen. The scrotal wall has normal thickness but there is hypoechoic collection with debris measured 3.88 cm by 2.50 cm. Conclusion: Right testicular and epididymis abscess collection, Scrotal skill cold abscess and testicular microlithiasis\ DDx: TB epididymorchitis and funiculitis | ||||||
Abdominal ultrasound (01/09/2023) | Unremarkable | ||||||
Fluid Cytology (01/11/2023) | Findings: Smear shows caseating necrosis only Conclusion: Scrotal fluid: Tuberculosis | ||||||
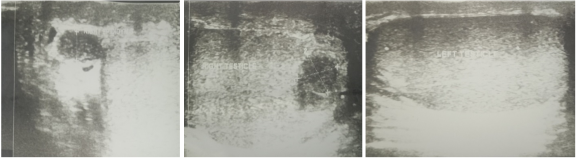
Scrotal ultrasound (8/24/2023) (figure 2) | Findings: There are multiple well-defined hetrogenously hypoechoic right testicular lesions seen. The largest measuring 0.9 cm by 0.8 cm in size. There are multiple small sized hyperechoic lesions seen having no posterior acoustic shadowing. The right epididymis is also enlarged in size having heterogeneously hypoechoic echogenicity, maximum AP diameter measuring 0.45 cm. Conclusion: Multiple right testicular hypoechoic lesions with enlargement of the right epididymis…..there is radiologic interval improvement seen as compared to previous ultrasound. Testicular microlithiasis | ||||||
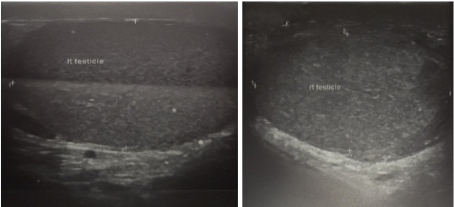
Scrotal Doppler Ultrasound (07/17/2024) (figure 3) NB: done during outcome declaration day. | Conclusion: right testicular scar (likely healed infection) | ||||||
AFB | Acid Fast Bacillus |
Bdq | Bedaquiline |
Cs | Cycloserine |
Cfz | Clofazimine |
FNAC | Fine Needle Aspiration Cytology |
GUTB | Genitourinary Tuberculosis |
INH | Isoniazid |
Lfx | Levofloxacin |
Lzd | Linezolid |
RR-EPTB | Resistance to Rifampicin Extra Pulmonary Tuberculosis |
RR-TB | Rifampicin-resistant TB |
SPSH | Saint Peter Specialized Hospital |
TB | Tuberculosis |
USG | Ultrasonography |
| [1] | Muttarak, M., W. ChiangMai, and B. Lojanapiwat, Tuberculosis of the genitourinary tract: imaging features with pathological correlation. Singapore medical journal, 2005. 46(10): p. 568. |
| [2] | Migliori, G. B., et al., Review of multidrug-resistant and extensively drug-resistant TB: global perspectives with a focus on sub-Saharan Africa. Tropical Medicine & International Health, 2010. 15(9): p. 1052-1066. |
| [3] | Organization, W. H., WHO country stories: delivering for all. 2023: World Health Organization. |
| [4] | Organization, W. H., Contributions of WHO to South Africa’s health agenda: evaluation of the Country Cooperation Strategy 2016-2020. 2022. |
| [5] | Seid, M. A., et al., Drug-susceptible tuberculosis treatment success and associated factors in Ethiopia from 2005 to 2017: a systematic review and meta-analysis. BMJ open, 2018. 8(9): p. e022111. |
| [6] | Wise, G. J., Urinary tuberculosis: modern issues. Current urology reports, 2009. 10(4): p. 313-318. |
| [7] | Goel, A., A. Seth, and R. Kumar, Autocystectomy following extensive genitourinary tuberculosis: Presentation and management. International urology and nephrology, 2002. 34: p. 325-327. |
| [8] | Eastwood, J. B., C. M. Corbishley, and J. M. Grange, Tuberculosis and the kidney. Journal of the American Society of Nephrology, 2001. 12(6): p. 1307-1314. |
| [9] | Carvalho, A. and R. Duarte, Tuberculose testicular: Caso clínico Testicular tuberculosis: Case report. Rev Port Pneumol, 2009. 15(6): p. 1193-1197. |
| [10] | Abraham, S., et al., A case of testicular tuberculosis mimicking malignancy in a healthy young man. Therapeutic advances in infectious disease, 2016. 3(3-4): p. 110-113. |
| [11] | Figueiredo, A. A. and A. M. Lucon, Urogenital tuberculosis: update and review of 8961 cases from the world literature. Reviews in urology, 2008. 10(3): p. 207. |
| [12] | Kinnear, S. H., B. G. Link, M. S. Ballan, and R. L. Fischbach, Understanding the experience of stigma for parents of children with autism spectrum disorder and the role stigma plays in families’ lives. Journal of autism and developmental disorders, 2016. 46: p. 942-953. |
| [13] | Das, A., S. Batabyal, S. Bhattacharjee, and A. Sengupta, A rare case of isolated testicular tuberculosis and review of literature. Journal of family medicine and primary care, 2016. 5(2): p. 468-470. |
| [14] | Mohamed Alı, A., A. Doğan, M. A. Ali, and B. S. Çakmak, Testicular tuberculosis: two rare case report. International Medical Case Reports Journal, 2023: p. 339-343. |
| [15] | Manchanda, S., B. B. Sharma, and S. Kumar, Tuberculous epididymo-orchitis MRI appearance. Urology Journal, 2012. 9(1): p. 351. |
| [16] | Man, J., et al., Diagnosis and treatment of epididymal tuberculosis: a review of 47 cases. PeerJ, 2020. 8: p. e8291. |
| [17] | Wininger, F. A., et al., Case report: Case report. Can Fam Physician, 2020. 47(10): p. 788-9. |
| [18] | Türkvatan, A., E. Kelahmet, Ç. Yazgan, and T. Ölçer, Sonographic findings in tuberculous epididymo-orchitis. Journal of Clinical Ultrasound, 2004. 32(6): p. 302-305. |
| [19] | Chirindel, A., F. Martinez, J. A. Gagliardi, and M. F. Armm, Testicular tuberculosis without epididymitis simulating neoplasm. Radiology Case Reports, 2008. 3(3): p. 133. |
APA Style
Yesuf, M. H., Mohammed, A. S., Yesuf, A. H., Semaga, S. A., Oumer, R. S., et al. (2025). A Rare Case of Isolated Testicular Drug–Resistant Tuberculosis (Testicular DR-TB): Case Report. International Journal of Medical Case Reports, 4(1), 1-6. https://doi.org/10.11648/j.ijmcr.20250401.11
ACS Style
Yesuf, M. H.; Mohammed, A. S.; Yesuf, A. H.; Semaga, S. A.; Oumer, R. S., et al. A Rare Case of Isolated Testicular Drug–Resistant Tuberculosis (Testicular DR-TB): Case Report. Int. J. Med. Case Rep. 2025, 4(1), 1-6. doi: 10.11648/j.ijmcr.20250401.11
@article{10.11648/j.ijmcr.20250401.11,
author = {Mustofa Hassen Yesuf and Abdurehman Seid Mohammed and Ali Hassen Yesuf and Simret Arega Semaga and Rani Seid Oumer and Solyana Haileselassie Admassie},
title = {A Rare Case of Isolated Testicular Drug–Resistant Tuberculosis (Testicular DR-TB): Case Report},
journal = {International Journal of Medical Case Reports},
volume = {4},
number = {1},
pages = {1-6},
doi = {10.11648/j.ijmcr.20250401.11},
url = {https://doi.org/10.11648/j.ijmcr.20250401.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijmcr.20250401.11},
abstract = {Introduction: Drug-resistant TB poses a significant threat to global TB care and prevention and remains a major public health issue in many countries and Testicular drug-resistant tuberculosis (testicular DR-TB) refers to a form of tuberculosis that specifically affects the testicles and is resistant to standard anti-TB medications, isolated testicular involvement is uncommon. Case presentation: a twenty-seven-year-old male patient presented with painful swelling of the scrotum for one month. He was treated with first-line anti-TB (RHZE/RH) and completed a month back at the health center. He had a similar complaint during the first diagnosis. While he was on treatment, the swelling subsided and recurred while he discontinued the medication. Our hospital received a referral for this complaint. Otherwise, he has no history of chronic illness, no surgical procedure at any site, no usage of second-line anti-TB drugs, or contact with a DR-TB patient. During the presentation, his vital signs were within normal range. The only pertinent finding was in the genitourinary system, which is that the scrotum is swollen and tender. Following clinical examinations and investigation findings with the diagnosis of RR-EPTB (testicular TB), we put him on an individualized longer regimen (Lfx/Cs/Cfz/Bdq/Cfz/Lzd) and pyridoxine. After 18 months of treatment, the outcome is declared as completed. After being advised on danger signs, he was appointed after six months for post-treatment follow-up according to the Ethiopian DR-TB management protocol. Conclusion: This case highlights the importance of timely diagnosis and adherence to treatment in managing drug-resistant extrapulmonary tuberculosis (RR-EPTB), specifically testicular TB. The patient's recurrent symptoms following discontinuation of first-line anti-TB therapy illustrate the challenges faced in treatment adherence and the potential consequences of inadequate management.},
year = {2025}
}
TY - JOUR T1 - A Rare Case of Isolated Testicular Drug–Resistant Tuberculosis (Testicular DR-TB): Case Report AU - Mustofa Hassen Yesuf AU - Abdurehman Seid Mohammed AU - Ali Hassen Yesuf AU - Simret Arega Semaga AU - Rani Seid Oumer AU - Solyana Haileselassie Admassie Y1 - 2025/01/14 PY - 2025 N1 - https://doi.org/10.11648/j.ijmcr.20250401.11 DO - 10.11648/j.ijmcr.20250401.11 T2 - International Journal of Medical Case Reports JF - International Journal of Medical Case Reports JO - International Journal of Medical Case Reports SP - 1 EP - 6 PB - Science Publishing Group SN - 2994-7049 UR - https://doi.org/10.11648/j.ijmcr.20250401.11 AB - Introduction: Drug-resistant TB poses a significant threat to global TB care and prevention and remains a major public health issue in many countries and Testicular drug-resistant tuberculosis (testicular DR-TB) refers to a form of tuberculosis that specifically affects the testicles and is resistant to standard anti-TB medications, isolated testicular involvement is uncommon. Case presentation: a twenty-seven-year-old male patient presented with painful swelling of the scrotum for one month. He was treated with first-line anti-TB (RHZE/RH) and completed a month back at the health center. He had a similar complaint during the first diagnosis. While he was on treatment, the swelling subsided and recurred while he discontinued the medication. Our hospital received a referral for this complaint. Otherwise, he has no history of chronic illness, no surgical procedure at any site, no usage of second-line anti-TB drugs, or contact with a DR-TB patient. During the presentation, his vital signs were within normal range. The only pertinent finding was in the genitourinary system, which is that the scrotum is swollen and tender. Following clinical examinations and investigation findings with the diagnosis of RR-EPTB (testicular TB), we put him on an individualized longer regimen (Lfx/Cs/Cfz/Bdq/Cfz/Lzd) and pyridoxine. After 18 months of treatment, the outcome is declared as completed. After being advised on danger signs, he was appointed after six months for post-treatment follow-up according to the Ethiopian DR-TB management protocol. Conclusion: This case highlights the importance of timely diagnosis and adherence to treatment in managing drug-resistant extrapulmonary tuberculosis (RR-EPTB), specifically testicular TB. The patient's recurrent symptoms following discontinuation of first-line anti-TB therapy illustrate the challenges faced in treatment adherence and the potential consequences of inadequate management. VL - 4 IS - 1 ER -
Department of Internal Medicine, Saint Peter’s Specialized Hospital, Addis Ababa, Ethiopia
Department of Public Health, Saint Peter’s Specialized Hospital, Addis Ababa, Ethiopia
Department of Urologic -Surgery, Wollo University, Dessie, Ethiopia
Department of Internal Medicine, Saint Peter’s Specialized Hospital, Addis Ababa, Ethiopia
School of Medicine, Africa Medical College, Addis Ababa, Ethiopia
Department of Radiology, Saint Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia
Information