Background: Radical prostatectomy (RP) is the gold standard treatment for localised prostate cancer. It is performed at a low rate because of the difficulty in selecting patients. Patients are generally diagnosed at the metastatic stage. In the Ivorian literature, there are few reports on RP. We propose to describe an initial series. Objective: The aim of our study was to report the carcinological results of radical prostatectomy at Treichville University Hospital. Methods: We conducted a retrospective cohort from August 2019 to March 2023 at the Urology Department of Treichville University Hospital. We included all patients who had radical prostatectomy after being diagnosed with localised prostate cancer. Results: A total of 20 cases were selected. The mean age was 61.5 years. The most common Gleason score was 6 (3+3). 50% of patients were classified as pT3 and had a positive resection margin. Biological recurrence was observed in 75% of cases with positive resection margins after 6 months' follow-up. A 12-month recurrence-free survival analysis curve of the Klaplan Meier type was performed. Conclusion: The pT3 stage was associated with a positive resection margin and favoured biological recurrence. Later, we will expand the cohort. We are considering a research protocol on long-term functional outcomes.
| Published in | International Journal of Clinical Urology (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijcu.20250901.11 |
| Page(s) | 1-6 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Carcinology, Prostatectomy, Recurrence
pTNM Classification | Number | Positive resection margin (R1) |
|---|---|---|
pT2bN0 | 08 | 00 |
pT2cN0 | 02 | 00 |
pT3aN0 | 06 | 06 |
pT3bN0 | 04 | 04 |
Total | 20 | 10 |
M1 | 1st Month |
MRI | Magnetic Reasoning Imaging |
PSA | Prostate Specific Antigen |
R0 | Healthy Resection Margin |
R1 | Positive Resection Margin |
RP | Radical Prostatectomy |
| [1] | Salomon L, Azria D, Bastide C, Beuzeboc P, Cormier L, Cornud F, et al. (CCAFU). Recommandations en onco-urologie 2010: cancer de la prostate. Prog Urol 2010; 20(Suppl. 4): S217-51. |
| [2] | Ward JF, Slezak JM, Blute ML, Bergstralh EJ, Zincke H. Radical prostatectomy for clinically advanced (cT3) prostate cancer since the advent of prostate-specific antigen testing: 15-year outcome. BJU Int 2005; 95: 751-6. |
| [3] | Carver BS, Bianco FJ, Scardino PT, Eastham JA. Long-term outcome following radical prostatectomy in men with clinical stage T3 prostate cancer. J Urol 2006; 176: 564-8. |
| [4] | Bolla M, Van Poppel H, Collette L, Van Cangh P, Vekemans K, Da Pozzo L, et al. Postoperative radiotherapy after radical prostatectomy: a randomised controlled trial (EORTC trial 22911). Lancet 2005; 366: 572-8. |
| [5] | Walsh PC. Anatomic radical retropubic prostatectomy. In: Walsh PC, Retik AB, Vaugh ED Jr, Wein AJ, editors. Campbellâ’s Urology. Philadelphia, PA: Saunders. 2002; 8th ed(4). 3107-3129. |
| [6] | Freedland SJ, Partin AW, Humphreys EB, Mangold LA, Walsh PC. Radical prostatectomy for cT3a disease. Cancer 2007; 109: 1273-8. |
| [7] | Dangbayaola Basga Enock, Aspects épidémiologiques et histopathologiques des cancers de la prostate au Mali de 2016 à 2020: Données du registre des cancers; Faculté de Médecine et d’Odontostomatologie; 2021 – 2022 (These) |
| [8] | Nzamba Bisselou Paul Ludovic 1, Odo Bitti Addé1, Nziengui Tirogo Christian1, Kouassi et al, Cancer de la prostate chez le sujet de race noire en Côte d’Ivoire Prostate cancer in the black subjectin Côte d’Ivoire. Revue Internationale des Sciences Médicales d’Abidjan - RISM - Rev int sc méd Abj -RISM-2020; 22, 1: 72-74. |
| [9] | Ritch CR, Morrison BF, Hruby G, Coard KC, Mayhew R, Aiken W et al. Pathological outcome and biochemical recurrence-free survival after radical prostatectomy in AfricanAmerican, Afro-Caribbean (Jamaican) and Caucasian-American men: An international comparison. BJU Int. 2013; 111(4 Pt B): E186- 90. |
| [10] | McNeal JE. Normal histology of the prostate. Am J Surg Pathol. 1988; 12: 619-33. |
| [11] | Delongchamps NB, Peyromaurea M, Kpatchaa F, Beuvonb F, Legranda G, Zerbib M. Cancer de la prostate de stade pT3N0 traité par prostatectomie radicale en monothérapie: résultats carcinologiques et facteurs prédictifs de récidive. Prog Urol. 2012; 22: 100-105. |
| [12] | Pound CR, Partin AW, Eisenberger MA, Chan DW, Pearson JD, Walsh PC. Natural history of progression after PSA elevation following radical prostatectomy. JAMA. 1999; 281: 1591- 7. |
| [13] | Godoy G, Tareen BU, Lepor H. Does benign prostatic tissue contribute to measurable PSA levels after radical prostatectomy? Urology. 2009; 74: 167-70. |
| [14] | Li Am, He C, Wood DP, Arbor A. Predictors of overall cancer-specific and disease-free survival after prostatectomy in men with high grade cancer. April 2011; 185(4): Suppl: p e65- e66. |
| [15] | Molina Escudero R, Herranz-Amo F, PaezBorda A, Hernandez Fernandez C. Predictive postoperative model for biochemical recurrence in patients with localized prostate cancer treated with radical prostatectomy as monotherapy. Arch Esp Urol. 2014 Apr; 67(3): 259-67. |
| [16] | Roehl KA, Han RC, Antenor JA, Catalona WJ. Cancer progression and survival rates following anatomical radical retropubic prostatectomy in 3478 consecutive patients: long-term results. September 2004, 172: 3; 910-914. |
| [17] | Vickers A, Bennette C, Steineck G, Adami HO, Johansson JE, Bill-Axelson A, Palmgren J, Garmo H, Holmberg L. Individualized estimation of the benefit of radical prostatectomy from the Scandinavian Prostate Cancer Group randomized trial. Eur Urol. 2012 Aug; 62(2): 204-9. |
| [18] | Xylinas E, Misraï V, Compérat E, RennardPennat R, Vaessen C. Résultats carcinologiques et fonctionnels de la prostatectomie totale dans les cancers de la prostate T3. Prog Urol. 2009; 19: 285-90. |
| [19] | Salomon L, Levrel O, De La Taille A, Hoznek A, Chopin D, Abbou C. Localisation des marges d´exérèse positives après prostatectomie radicale par voie rétropubienne, périnéale et laparoscopique. Prog Urol. 2002; 12: 628-34. |
| [20] | Wieder JA, Soloway MS. Incidence, etiology, location, prevention and treatment of positive surgical margins after radical prostatectomy for prostate cancer. The journal of urology. 1998; 160: 299-315. |
APA Style
Yao, E. K., Gnabro, G. A. P., Adebayo, T. B., Tuo, L. S. M., Odo, B. A., et al. (2025). Preliminary Carcinological Results of Radical Prostatectomies at Treichville University Hospital from 2019 to 2023 (Abidjan, Cote D’Ivoire). International Journal of Clinical Urology, 9(1), 1-6. https://doi.org/10.11648/j.ijcu.20250901.11
ACS Style
Yao, E. K.; Gnabro, G. A. P.; Adebayo, T. B.; Tuo, L. S. M.; Odo, B. A., et al. Preliminary Carcinological Results of Radical Prostatectomies at Treichville University Hospital from 2019 to 2023 (Abidjan, Cote D’Ivoire). Int. J. Clin. Urol. 2025, 9(1), 1-6. doi: 10.11648/j.ijcu.20250901.11
@article{10.11648/j.ijcu.20250901.11,
author = {Evrard Kouamé Yao and Gnakouri Alain Pacome Gnabro and Tawakaltu Bolasade Adebayo and Legnima Sekou Michel Tuo and Bitti Adé Odo and Donafologo Daouda Yeo and N’Zibla Marie Ange Yebouet and Noel Coulibaly},
title = {Preliminary Carcinological Results of Radical Prostatectomies at Treichville University Hospital from 2019 to 2023 (Abidjan, Cote D’Ivoire)
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {1},
pages = {1-6},
doi = {10.11648/j.ijcu.20250901.11},
url = {https://doi.org/10.11648/j.ijcu.20250901.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250901.11},
abstract = {Background: Radical prostatectomy (RP) is the gold standard treatment for localised prostate cancer. It is performed at a low rate because of the difficulty in selecting patients. Patients are generally diagnosed at the metastatic stage. In the Ivorian literature, there are few reports on RP. We propose to describe an initial series. Objective: The aim of our study was to report the carcinological results of radical prostatectomy at Treichville University Hospital. Methods: We conducted a retrospective cohort from August 2019 to March 2023 at the Urology Department of Treichville University Hospital. We included all patients who had radical prostatectomy after being diagnosed with localised prostate cancer. Results: A total of 20 cases were selected. The mean age was 61.5 years. The most common Gleason score was 6 (3+3). 50% of patients were classified as pT3 and had a positive resection margin. Biological recurrence was observed in 75% of cases with positive resection margins after 6 months' follow-up. A 12-month recurrence-free survival analysis curve of the Klaplan Meier type was performed. Conclusion: The pT3 stage was associated with a positive resection margin and favoured biological recurrence. Later, we will expand the cohort. We are considering a research protocol on long-term functional outcomes.
},
year = {2025}
}
TY - JOUR T1 - Preliminary Carcinological Results of Radical Prostatectomies at Treichville University Hospital from 2019 to 2023 (Abidjan, Cote D’Ivoire) AU - Evrard Kouamé Yao AU - Gnakouri Alain Pacome Gnabro AU - Tawakaltu Bolasade Adebayo AU - Legnima Sekou Michel Tuo AU - Bitti Adé Odo AU - Donafologo Daouda Yeo AU - N’Zibla Marie Ange Yebouet AU - Noel Coulibaly Y1 - 2025/01/16 PY - 2025 N1 - https://doi.org/10.11648/j.ijcu.20250901.11 DO - 10.11648/j.ijcu.20250901.11 T2 - International Journal of Clinical Urology JF - International Journal of Clinical Urology JO - International Journal of Clinical Urology SP - 1 EP - 6 PB - Science Publishing Group SN - 2640-1355 UR - https://doi.org/10.11648/j.ijcu.20250901.11 AB - Background: Radical prostatectomy (RP) is the gold standard treatment for localised prostate cancer. It is performed at a low rate because of the difficulty in selecting patients. Patients are generally diagnosed at the metastatic stage. In the Ivorian literature, there are few reports on RP. We propose to describe an initial series. Objective: The aim of our study was to report the carcinological results of radical prostatectomy at Treichville University Hospital. Methods: We conducted a retrospective cohort from August 2019 to March 2023 at the Urology Department of Treichville University Hospital. We included all patients who had radical prostatectomy after being diagnosed with localised prostate cancer. Results: A total of 20 cases were selected. The mean age was 61.5 years. The most common Gleason score was 6 (3+3). 50% of patients were classified as pT3 and had a positive resection margin. Biological recurrence was observed in 75% of cases with positive resection margins after 6 months' follow-up. A 12-month recurrence-free survival analysis curve of the Klaplan Meier type was performed. Conclusion: The pT3 stage was associated with a positive resection margin and favoured biological recurrence. Later, we will expand the cohort. We are considering a research protocol on long-term functional outcomes. VL - 9 IS - 1 ER -
Urology Departement, Treichville University Hospital, Abidjan, Cote d’Ivoire; Surgery Departement, Military Hospital of Abidjan, Abidjan, Cote d’Ivoire; University Félix Houphouët Boigny, Abidjan, Cote d’Ivoire
Biography: Evrard Kouamé Yao is a military urologist and officer in the Ivory Coast army. He is an assistant professor at the Felix Houphouet Boigny University (Abidjan). He is head of clinic at the urology department of the Treichville university hospital. He has published works on surgical complications of renal transplants in the Ivory Coast and variations in the renal pedicle during renal transplants.
Research Fields: Kidney Transplantation, Onco urology, Andrology, Uro Gynecology, Urological trauma

Urology Departement, Cocody University Hospital, Abidjan, Cote d’Ivoire; University Félix Houphouët Boigny, Abidjan, Cote d’Ivoire
Research Fields: Onco urology, Emergency in urology, Urinary stones, Lower urinary tract syndrome, Endo urology
Urology Departement, Treichville University Hospital, Abidjan, Cote d’Ivoire; University Félix Houphouët Boigny, Abidjan, Cote d’Ivoire
Research Fields: Urinary Stones, uro infectiology, Onco urology, Endo urology, Andrology
Urology Departement, Treichville University Hospital, Abidjan, Cote d’Ivoire; University Félix Houphouët Boigny, Abidjan, Cote d’Ivoire
Research Fields: Andrology, Onco urology, Kidney transplantation, Urology imaging, Urinary stones
University Félix Houphouët Boigny, Abidjan, Cote d’Ivoire; Oncology Departement, Treichville University Hospital, Abidjan, Cote d’Ivoire
Research Fields: Onco urology, Onco gynecology, Radiotherapy, Geriatric, Pediatric oncology
Urology Departement, Treichville University Hospital, Abidjan, Cote d’Ivoire
Research Fields: Onco urology, Uro gynecology, uro pediatric, Neuro urology, Urodynamic
Urology Departement, Treichville University Hospital, Abidjan, Cote d’Ivoire
Urology Departement, Treichville University Hospital, Abidjan, Cote d’Ivoire; University Félix Houphouët Boigny, Abidjan, Cote d’Ivoire
Research Fields: Onco urology, Kidney transplantation, Urinary stones, Neuro urology, Endo urology

Figure 1. Posterior view of a prostato vesiculectomy specimen.
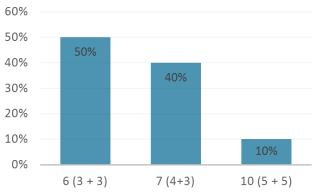
Figure 2. Distribution of patients according to preoperative Gleason score.
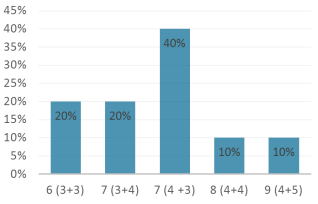
Figure 3. Distribution of patients according to the Gleason score of the surgical specimen.
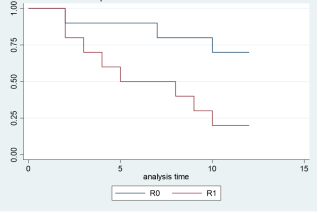
Figure 4. Recurrence-free survival at 12 months according to resection margins.
Information

