Introduction: Renal artery aneurysm is rare and has reported incidence of 0.09% of the general population. The occurrence of a giant renal artery aneurysm from the main renal artery has even been more rarely reported. Endovascular intervention is ideal for the treatment of patients with vascular anomalies of the renal artery especially in cases where surgical morbidity is high. This article reports our experience in the treatment of giant complex renal artery aneurysm by endovascular techniques in a young man with poor performance status. Case report: A 25-year-old male with no significant past medical history presented with progressively worsening abdominal pain, generalized body swelling, progressive abdominal distension, low blood pressure and difficulty in breathing. He had poor performance status with suboptimal oxygen saturation probably due to splinting of the diaphragm from the progressive abdominal distension and was immediately transferred to intensive care unit for close monitoring. Ultrasound scan revealed a huge right renal mass with turbulent internal flow paving way for suspicion of a giant renal artery aneurysm. Subsequent CT angiogram confirmed a giant saccular aneurysm emanating from the proximal main right renal artery with evidence of surrounding hematoma signifying recent rupture. There was significant mass effect on adjacent structures including the inferior vena cava which was nearly completely collapsed. Following a multidisciplinary discussion with interventional radiology, he was transferred to a facility equipped with a catheterization laboratory. Procedure: Real-time ultrasound was used to gain access into the right radial artery and a 6French sheath placed. A 5 Fr Vertebral curve catheter was advanced successfully from the right radial artery access into the right renal artery over a 0.035 guidewire. Following arteriograms and confirmation of site of aneurysm being the proximal main renal artery, considerations for treatment included stent graft placement or sacrifice of the right renal artery. Due to unavailability of an appropriately sized stent graft, we elected to sacrifice the right renal artery. Through the 5 French catheter, multiple 0.035 detachable and nondetectable coils were deployed proximal to the aneurysm sac and distal to the aneurysm sac to completely occlude the right renal artery. Post embolization arteriogram showed complete exclusion of flow within the aneurysm sac. Conclusion: Endovascular embolization as a minimal invasive technique is an ideal treatment option for the treatment of giant complex renal artery aneurysms especially in patients in a poor clinical state.
| Published in | International Journal of Clinical Urology (Volume 8, Issue 2) |
| DOI | 10.11648/j.ijcu.20240802.16 |
| Page(s) | 44-50 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Renal Artery, Aneurysms, Embolization, Interventional Radiology, Arteriogram
RAAs | Renal Artery Aneurysms |
MRA | Magnetic Resonance Angiography |
CT | Computed Tomography |
| [1] | Coleman DM, Stanley JC. Renal artery aneurysms. J Vasc Surg. 2015 Sep. 62 (3): 779-85. |
| [2] | Stanley JC, Rhodes EL, Gewertz BL, Chang CY, Walter JF, Fry WJ. Renal artery aneurysms. Significance of macroaneurysms exclusive of dissections and fibrodysplastic mural dilations. Arch Surg. 1975; 110(11): 1327-1333. |
| [3] | Zhang LJ, Yang GF, Qi J, Shen W. Renal artery aneurysm: diagnosis and surveillance with multidetector-row computed tomography. Acta Radiol. 2007; 48(3): 274-279. |
| [4] | Tham G, Ekelund L, Herrlin K, et al. Renal artery aneurysms natural history and prognosis. Ann Surg. 1983; 197: 348–352. |
| [5] | Henriksson C, Lukes P, Nilson AE. Angiographically discovered, non-operated renal artery aneurysms. Scand J Urol Neprol. 1984; 18: 59–62. |
| [6] | Deterling RA., Jr Aneurysm of the visceral arteries. J Cardiovasc Surg (Torino) 1971; 12: 309–322. |
| [7] | Sedat J, Chau Y, Baque J. Endovascular treatment of renal aneurysms: a series of 18 cases. Eur J Radiol. 2012; 81: 3973–3978. |
| [8] | Down LA, Papavassiliou DV, O'Rear EA. Arterial deformation with renal artery aneurysm as a basis for secondary hypertension. Biorheology. 2013. 50 (1-2): 17-31. |
| [9] | Chung R, Touska P, Morgan R, Belli AM. Endovascular management of true renal arterial aneurysms: results from a single center. Cardiovasc Intervent Radiol. 2016; 39: 36–43. |
| [10] | Shigehiro Karashima, Mitsuhiro Kometani, Daisuke Aono, Takuya Higashitani, Yuya Nishimoto, Seigoh Konishi, Masashi Demura, Yoshiyu Takeda, and Takashi Yoneda. Renal artery aneurysm due to fenestration of a branch of the renal artery: A case study. J Endocri Soc. 2021 Feb 1; 5(2): bvaa189. |
| [11] | Augustin G, Kulis T, Kello N, Ivkovic V. Ruptured renal artery aneurysm in pregnancy and puerperium: literature review of 53 cases. Arch Gynecol Obstet. 2019 Apr. 299(4): 923-931. |
| [12] | Bastounis E, Pikoulis E, Georgopoulos S, Alexiou D, Leppäniemi A, Boulafendis D. Surgery for renal artery aneurysms: a combined series of two large centers. Eur Urol. 1998. 33 (1): 22-7. |
| [13] | Adeyemi J, Johnson J, Rits Y, Akingba AG, Rubin J. Ex Vivo Reconstruction and Autotransplantation for Hilar Renal Artery Aneurysms in Patients with Congenital Anomalies. Ann Vasc Surg. 2018 Feb. 47: 280. e5-280.e8. |
| [14] | Wu Q, Yang X, Yuan B, Cai L, Zhuang J, Feng D, et al. Robot-Assisted Laparoscopic Retroperitoneal Renal Artery Aneurysm Repair: A Rare Case Report and Literature Review. Urol Int. 2021 Aug 5. 1-6. |
| [15] | Grandhomme J, Lejay A, Gogeneata I, Steinmetz L, Georg Y, Chakfé N, et al. Robotic Surgery For in situ Renal Artery Aneurysm Repair: Technical Note and Literature Review About a Mini- Invasive Alternative. Ann Vasc Surg. 2021 Jul. 74: 526. e7-526.e12. |
| [16] | Etezadi V, Gandhi RT, Beneati JF, et al. Endovascular treatment of visceral and renal artery aneurysms. J Vasc Interv Radiol. 2011; 22: 1246–1253. |
| [17] | Klein GE, Szolar DH, Breinl E, Raith J, Schreyer HH. Endovascular treatment of renal artery aneurysms with conventional non-detachable microcoils and Guglielmi detachable coils. Br J Urol. 1997 Jun. 79 (6): 852-60. |
| [18] | Belli AM, Markose G, Morgan R. The role of interventional radiology in the treatment of abdominal visceral artery aneuryms. Cardiovasc Intervent Radiol. 2012; 35: 234–243. |
| [19] | Chaer RA, Abularrage CJ, Coleman DM, Eslami MH, Kashyap VS, Rockman C, et al. The society for vascular surgery clinical practice guidelines on the management of visceral aneurysms. J Vasc Surg. (2020) 72(1s): 3s–39. |
| [20] | Henke PK, Cardneau JD, Welling TH, 3rd, Upchurch GR, Jr, Wakefield TW, Jacobs LA, et al. Renal artery aneurysms: a 35-year clinical experience with 252 aneurysms in 168 patients. Ann Surg. (2001) 234(4): 454–62; discussion 462–3. |
| [21] | González J, Esteban M, Andrés G, Linares E, Martínez-Salamanca JI. Renal artery aneurysms. Curr Urol Rep. (2014) 15(1): 376. |
| [22] | Dzsinich C, Gloviczki P, McKusick MA, et al. Surgical management of renal artery aneurysm. Cardiovasc Surg 1993; 1: 243–247. |
APA Style
Kenenna, O., Hammed, N., Terkaa, A., Obed, D., Felix, M. (2024). Endovascular Coil Occlusion of Right Renal Artery Aneurysm with Embolization of the Right Kidney: A Case Report. International Journal of Clinical Urology, 8(2), 44-50. https://doi.org/10.11648/j.ijcu.20240802.16
ACS Style
Kenenna, O.; Hammed, N.; Terkaa, A.; Obed, D.; Felix, M. Endovascular Coil Occlusion of Right Renal Artery Aneurysm with Embolization of the Right Kidney: A Case Report. Int. J. Clin. Urol. 2024, 8(2), 44-50. doi: 10.11648/j.ijcu.20240802.16
AMA Style
Kenenna O, Hammed N, Terkaa A, Obed D, Felix M. Endovascular Coil Occlusion of Right Renal Artery Aneurysm with Embolization of the Right Kidney: A Case Report. Int J Clin Urol. 2024;8(2):44-50. doi: 10.11648/j.ijcu.20240802.16
@article{10.11648/j.ijcu.20240802.16,
author = {Obiatuegwu Kenenna and Ninalowo Hammed and Atim Terkaa and Dades Obed and Magnus Felix},
title = {Endovascular Coil Occlusion of Right Renal Artery Aneurysm with Embolization of the Right Kidney: A Case Report},
journal = {International Journal of Clinical Urology},
volume = {8},
number = {2},
pages = {44-50},
doi = {10.11648/j.ijcu.20240802.16},
url = {https://doi.org/10.11648/j.ijcu.20240802.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20240802.16},
abstract = {Introduction: Renal artery aneurysm is rare and has reported incidence of 0.09% of the general population. The occurrence of a giant renal artery aneurysm from the main renal artery has even been more rarely reported. Endovascular intervention is ideal for the treatment of patients with vascular anomalies of the renal artery especially in cases where surgical morbidity is high. This article reports our experience in the treatment of giant complex renal artery aneurysm by endovascular techniques in a young man with poor performance status. Case report: A 25-year-old male with no significant past medical history presented with progressively worsening abdominal pain, generalized body swelling, progressive abdominal distension, low blood pressure and difficulty in breathing. He had poor performance status with suboptimal oxygen saturation probably due to splinting of the diaphragm from the progressive abdominal distension and was immediately transferred to intensive care unit for close monitoring. Ultrasound scan revealed a huge right renal mass with turbulent internal flow paving way for suspicion of a giant renal artery aneurysm. Subsequent CT angiogram confirmed a giant saccular aneurysm emanating from the proximal main right renal artery with evidence of surrounding hematoma signifying recent rupture. There was significant mass effect on adjacent structures including the inferior vena cava which was nearly completely collapsed. Following a multidisciplinary discussion with interventional radiology, he was transferred to a facility equipped with a catheterization laboratory. Procedure: Real-time ultrasound was used to gain access into the right radial artery and a 6French sheath placed. A 5 Fr Vertebral curve catheter was advanced successfully from the right radial artery access into the right renal artery over a 0.035 guidewire. Following arteriograms and confirmation of site of aneurysm being the proximal main renal artery, considerations for treatment included stent graft placement or sacrifice of the right renal artery. Due to unavailability of an appropriately sized stent graft, we elected to sacrifice the right renal artery. Through the 5 French catheter, multiple 0.035 detachable and nondetectable coils were deployed proximal to the aneurysm sac and distal to the aneurysm sac to completely occlude the right renal artery. Post embolization arteriogram showed complete exclusion of flow within the aneurysm sac. Conclusion: Endovascular embolization as a minimal invasive technique is an ideal treatment option for the treatment of giant complex renal artery aneurysms especially in patients in a poor clinical state.},
year = {2024}
}
TY - JOUR T1 - Endovascular Coil Occlusion of Right Renal Artery Aneurysm with Embolization of the Right Kidney: A Case Report AU - Obiatuegwu Kenenna AU - Ninalowo Hammed AU - Atim Terkaa AU - Dades Obed AU - Magnus Felix Y1 - 2024/12/30 PY - 2024 N1 - https://doi.org/10.11648/j.ijcu.20240802.16 DO - 10.11648/j.ijcu.20240802.16 T2 - International Journal of Clinical Urology JF - International Journal of Clinical Urology JO - International Journal of Clinical Urology SP - 44 EP - 50 PB - Science Publishing Group SN - 2640-1355 UR - https://doi.org/10.11648/j.ijcu.20240802.16 AB - Introduction: Renal artery aneurysm is rare and has reported incidence of 0.09% of the general population. The occurrence of a giant renal artery aneurysm from the main renal artery has even been more rarely reported. Endovascular intervention is ideal for the treatment of patients with vascular anomalies of the renal artery especially in cases where surgical morbidity is high. This article reports our experience in the treatment of giant complex renal artery aneurysm by endovascular techniques in a young man with poor performance status. Case report: A 25-year-old male with no significant past medical history presented with progressively worsening abdominal pain, generalized body swelling, progressive abdominal distension, low blood pressure and difficulty in breathing. He had poor performance status with suboptimal oxygen saturation probably due to splinting of the diaphragm from the progressive abdominal distension and was immediately transferred to intensive care unit for close monitoring. Ultrasound scan revealed a huge right renal mass with turbulent internal flow paving way for suspicion of a giant renal artery aneurysm. Subsequent CT angiogram confirmed a giant saccular aneurysm emanating from the proximal main right renal artery with evidence of surrounding hematoma signifying recent rupture. There was significant mass effect on adjacent structures including the inferior vena cava which was nearly completely collapsed. Following a multidisciplinary discussion with interventional radiology, he was transferred to a facility equipped with a catheterization laboratory. Procedure: Real-time ultrasound was used to gain access into the right radial artery and a 6French sheath placed. A 5 Fr Vertebral curve catheter was advanced successfully from the right radial artery access into the right renal artery over a 0.035 guidewire. Following arteriograms and confirmation of site of aneurysm being the proximal main renal artery, considerations for treatment included stent graft placement or sacrifice of the right renal artery. Due to unavailability of an appropriately sized stent graft, we elected to sacrifice the right renal artery. Through the 5 French catheter, multiple 0.035 detachable and nondetectable coils were deployed proximal to the aneurysm sac and distal to the aneurysm sac to completely occlude the right renal artery. Post embolization arteriogram showed complete exclusion of flow within the aneurysm sac. Conclusion: Endovascular embolization as a minimal invasive technique is an ideal treatment option for the treatment of giant complex renal artery aneurysms especially in patients in a poor clinical state. VL - 8 IS - 2 ER -
Division of Urology, Department of Surgery, Federal Medical Center Jabi, Abuja, Nigeria; Division of Urology, Department of Surgery, Cedarcrest Hospitals Limited, Abuja, Nigeria
Figure 1. Introduction of guidewire via the right femoral artery under fluoroscopic guidance.
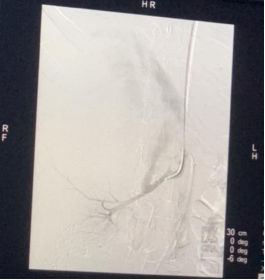
Figure 2. Arteriogram of the right renal artery.

Figure 3. Cannulation of right radial artery.
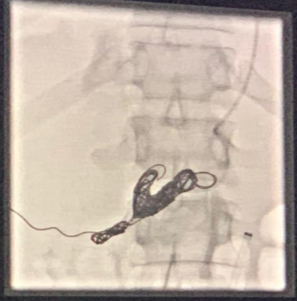
Figure 4. Coils deployed proximal and distal to the aneurysm sac to completely occluded the right renal artery.

Figure 5. Venogram following deployment of coil occlusion.
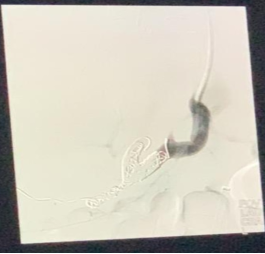
Figure 6. Venogram also demonstrates occlusion of the distal inferior vena cava with patency of the right renal vein.
Information

