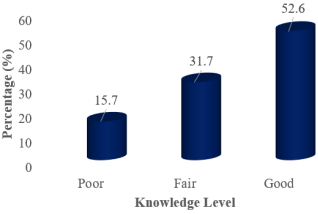
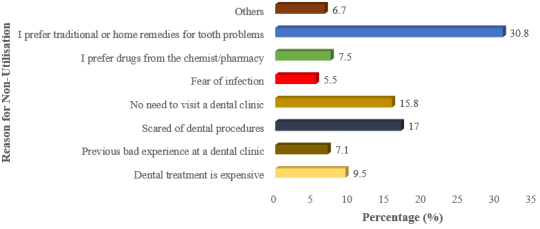
Background: Oral health is essential for overall health and quality of life. Yet, utilisation of professional dental services remains low in many rural communities in developing countries. This study assessed knowledge and determinants of dental care utilisation among rural residents of Ikwerre Local Government Area (LGA), Rivers State, Nigeria. Methods: A community-based, cross-sectional study was conducted among 300 adults selected using multistage sampling. The sample size was calculated using the Cochran formula. Of the 326 distributed questionnaires, 300 were completed, yielding a 92.0% response rate. Data were collected using a validated structured questionnaire (Cronbach’s alpha ≥ 0.7). Descriptive statistics summarised the variables, and Chi-square and binary logistic regression analyses identified factors associated with dental care utilisation. Statistical significance was set at p < 0.05. Results: Over half of respondents (52.6%) demonstrated good knowledge of oral health, and 89.0% were aware of dental services. However, only 15.7% had utilized professional dental care in the past year, mostly for pain or gum problems, while preventive visits were rare. Multivariate analysis showed that educational level, monthly income, and positive attitude towards dental care significantly predicted utilization (p < 0.001). Key barriers included preference for traditional remedies, fear of dental procedures, perceived lack of need, and cost. Conclusion: Despite high awareness, utilization of dental services in Ikwerre LGA remains low. Socio-economic status and attitudes, rather than knowledge alone, largely influence dental care-seeking behaviour. Interventions targeting oral health education, affordability, and attitude change are critical to improving dental service uptake in rural communities.
| Published in | Central African Journal of Public Health (Volume 12, Issue 2) |
| DOI | 10.11648/j.cajph.20261202.12 |
| Page(s) | 64-75 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Dental Care Utilisation, Determinants, Rural Population, Oral Health, Nigeria
Variables | Frequency (n=300) | Percentage (%) | Cumulative Percentage |
|---|---|---|---|
Gender | |||
Male | 122 | 40.7 | 40.7 |
Female | 178 | 59.3 | 100 |
Marital status | |||
Not currently married | 114 | 38.0 | 38.0 |
Married | 186 | 62.0 | 100 |
Age of respondents (years) | |||
18-32 | 78 | 26.0 | 26.0 |
33-47 | 105 | 35.0 | 62.0 |
48-62 | 79 | 26.3 | 88.3 |
63-77 | 38 | 12.7 | 100 |
Mean (SD) | 43.17 (14.67) | ||
Educational level | |||
No formal | 59 | 19.4 | 19.4 |
Primary | 73 | 24.3 | 43.7 |
Secondary | 136 | 45.3 | 89.0 |
Tertiary | 32 | 11.0 | 100 |
Source of household income | |||
Unemployed | 32 | 10.7 | 10.7 |
Farmer | 103 | 34.3 | 45.0 |
Business | 75 | 25.0 | 70.0 |
Formal Employment | 34 | 11.3 | 81.3 |
Artisans | 56 | 18.7 | 100 |
Variables | Frequency (n=300) | Percentage (%) | Cumulative Percentage |
|---|---|---|---|
Aware of Dental Clinic | |||
Yes | 267 | 89.0 | 89.0 |
No | 33 | 11.0 | 100 |
Dental visit within the past 1 year | |||
Yes | 47 | 15.7 | 15.7 |
No | 253 | 84.3 | 100 |
Frequency of Dental Visits | |||
Only if I have a dental problem | 30 | 63.8 | 63.8 |
Once every 6 months | 7 | 14.9 | 78.7 |
Once every year | 10 | 21.3 | 100 |
Reason for Visit | |||
Tooth pain | 16 | 34.0 | 34.0 |
Gum problem | 13 | 27.7 | 61.7 |
Routine check-up | 5 | 10.6 | 72.3 |
Tooth extraction | 7 | 14.9 | 87.2 |
Others | 6 | 12.8 | 100 |
Where care Received | |||
Government facility | 38 | 80.9 | 80.9 |
Private facility | 9 | 19.1 | 100 |
Satisfaction | |||
Very satisfied | 8 | 17.0 | 17.0 |
Satisfied | 18 | 38.4 | 55.4 |
Neutral | 9 | 19.1 | 74.5 |
Dissatisfied | 5 | 10.6 | 85.1 |
Very dissatisfied | 7 | 14.9 | 100 |
Variable | Dental Care Utilisation | Unadjusted Odds Ratio (uOR) | Adjusted Odds Ratio (aOR) | p-value | |
|---|---|---|---|---|---|
Yes | No | ||||
n (%) | n (%) | ||||
Age (years) | |||||
18-32 | 13 (20.3) | 65 (27.5) | 0.321 | ||
33-47 | 22 (34.4) | 83 (35.2) | 0.491 (0.196-1.232) | 0.542 (0.162-1.812) | 0.320 |
48-62 | 18 (28.1) | 61 (25.8) | 0.651 (0.280-1.513) | 0.346 (0.112-1.068) | 0.065 |
63-77 | 11 (17.2) | 27 (11.4) | 0.724 (0.302-1.740) | 0.587 (0.197-1.750) | 0.339 |
Sex of Respondents | |||||
Male | 27 (42.2) | 95 (40.3) | |||
Female | 37 (57.8) | 141 (59.7) | 1.083 (0.619-1.896) | 1.072 (0.512-2.244) | 0.855 |
Marital Status | |||||
Not currently married | 21 (32.8) | 93 (39.4) | |||
Married | 43 (67.2) | 143 (60.6) | 0.751 (0.419-1.346) | 0.865 (0.371-2.015) | 0.736 |
Level of Education | |||||
No formal education | 6 (9.4) | 53 (22.5) | <0.001* | ||
Primary | 9 (14.1) | 64 (27.1) | 0.038 (0.012-0.121) | 0.060 (0.014-0.252) | <0.001* |
Secondary | 25 (39.1) | 111 (47.0) | 0.047 (0.016-0.136) | 0.058 (0.015-0.220) | <0.001* |
Tertiary | 24 (37.5) | 8 (3.4) | 0.075 (0.030-0.187) | 0.076 (0.024-0.239) | <0.001* |
Occupation | |||||
Unemployed | 3 (4.7) | 29 (12.3) | 0.539 | ||
Farmer | 15 (23.4) | 87 (36.9) | 0.379 (0.098-1.462) | 0.465 (0.103-2.101) | 0.320 |
Business | 14 (21.9) | 62 (26.3) | 0.632 (0.273-1.466) | 0.842 (0.313-2.266) | 0.734 |
Formal employment | 20 (31.3) | 14 (5.9) | 0.828 (0.350-1.961) | 0.471 (0.163-1.356) | 0.163 |
Artisans | 12 (18.8) | 44 (18.6) | 5.238 (2.057-13.340) | 0.929 (0.261-3.302) | 0.909 |
Monthly Income | |||||
<₦20,000 | 7 (10.9) | 90 (38.1) | 0.000* | ||
₦20,000–₦49,999 | 18 (28.1) | 104 (44.1) | 0.041 (0.013-0.131) | 0.048 (0.013-0.186) | 0.000* |
₦50,000–₦99,999 | 24 (37.5) | 34 (14.4) | 0.092 (0.034-0.249) | 0.138 (0.043-0.439) | 0.001* |
₦100,000 and above | 15 (23.4) | 8 (3.4) | 0.376 (0.138-1.028) | 0.343 (0.103-1.147) | 0.082 |
Level of Knowledge | |||||
Good | 57 (89.1) | 196 (83.1) | |||
Poor | 7 (10.9) | 40 (16.9) | 0.602 (0.256-1.416) | 0.572 (0.194-1.685) | 0.572 |
Attitude towards dental care services | |||||
Positive | 53 (82.8) | 56 (23.7) | 0.065 (0.032-0.132) | 0.070 (0.033-0.152) | <0.001* |
Negative | 11 (17.2) | 180 (76.3) | |||
LGA | Local Government Area |
UOR | Unadjusted Odds Ratio |
AOR | Adjusted Odds Ratio |
CI | Confidence Interval |
SD | Standard Deviation |
WHO | World Health Organisation |
| [1] | Abodunrin, O. R., Adebayo, E. T., Adewole, I. E., Olagunju, M. T., Ekeh, C., Samuel, I. O., Zamba, E., Gbaja-Biamila, T., Akinsolu, F. T., Eleje, G. U., Tantawi, M. E., Ezechi, O. C., Foláyan, M. O. Factors associated with the dental service utilisation by enrollees on the Lagos State health insurance scheme, Nigeria. BMC Health Services Research. 2025, 25(1), 14. |
| [2] | Aborisade, A., Okolo, C., Aminu, R., Moghalu, H., Aminu, N., Bamgbose, B. Pattern of dental services utilisation among adolescents and adults in Kano, Northern Nigeria. Pyramid Journal of Medicine. 2024, 7(1). |
| [3] | Adeniyi, A. A., Oyapero, A. Predisposing, enabling and need factors influencing dental service utilisation among a sample of adult Nigerians. Population Medicine. 2020, 2(December), 1-9. |
| [4] | Akinyamoju, A. O., Dairo, D. M., Adeoye, I. A. Oral health knowledge and practices among adults in rural Nigeria. African Journal of Oral Health. 2018, 7(2), 45–53. |
| [5] | Akinyamoju, C. A., Taiwo, J. O., Uwadia, E., Agbogidi, J. M., Ambeke, A. ORAL HEALTH KNOWLEDGE AND PRACTICE AMONG TRADERS IN IBADAN. Annals of Ibadan postgraduate medicine. 2018, 16(2), 150–156. |
| [6] | Aroyehun, A. R., Onyenma, G. C., Abuta, C. M. A., Garshon, W. B. Effects of Coronavirus on Food Systems in Ikwerre Local Government Area of Rivers State, Nigeria. Journal of Agriculture. 2024, 7(2), 125-131. |
| [7] | Balogun, A. O., Taiwo, J. O., Ipeaiyeda, O. J., Lawal, F. B., Ibiyemi, O. A report on oral health delivery to rural underserved communities Oyo state using the mobile dental clinic. African Journal of Oral Health. 2018, 7(2), 5-10. |
| [8] | Chikuni, W., Amalimeh, B. E., Agholor, C. N. Utilisation of oral health services and associated factors in a sub-urban population in Western Uganda. International Journal of Medical Sciences and Pharma Research. 2023, 9(2), 1-12. |
| [9] | Deolia, S. G., Kela, K. S., Sawhney, I. M., Sonavane, P. A., Nimbulkar, G., Reche, A. Evaluation of oral health care seeking behavior in rural population of central India. Journal of family medicine and primary care. 2020, 9(2), 886–891. |
| [10] | Foláyan, M. O., Ishola, A. G., Bhayat, A., El Tantawi, M., Ndembi, N. Strengthening health systems to tackle oral diseases in Africa: Africa centers for Disease Control and Prevention's role. Frontiers in public health. 2025, 13, 1539805. |
| [11] | Foláyan, M. O., Olagunju, M. T., Abodunrin, O. R., Alade, O. T. A scoping review on the use of traditional medicine and oral health in Africa. PloS one. 2024, 19(5), e0297570. |
| [12] | Folorunsho, S., Ajayi, V., Sanmori, M., Suleiman, M., Abdullateef, R., Abdulganiyu, A. Access to and Utilisation of Dental Care Services by Older Adults in Nigeria: Barriers and Facilitators. Special care in dentistry: official publication of the American Association of Hospital Dentists, the Academy of Dentistry for the Handicapped, and the American Society for Geriatric Dentistry. 2025, 45(3), e70040. |
| [13] | Gallione, C., Bassi, E., Cattaneo, A., Busca, E., Basso, I., & Dal Molin, A. Oral Health Care: A Systematic Review of Clinical Practice Guidelines. Nursing & Health Sciences. 2025, 27(1), e70027. |
| [14] | Gbolahan, O. O., Fasola, A. O., Aladelusi, T. O. Attitude and Behavior to Oral Health of 456 Patients Who Presented for Tooth Extraction at 2 Health Facilities in Southwestern Nigeria. Journal of Patient Experience. 2019, 6(2), 157–163. |
| [15] | Geda, Z. T., Asefa, K. Z., Gonfa, A. N., Assefa, M. Oral health-related knowledge, attitudes, and practices among high school students in Robe Town, Ethiopia: a cross-sectional study. BMC Public Health. 2025, 25(1), 3848. |
| [16] | Hewlett, S. A., Blankson, P. K., Aheto, J. M. K., Anto, F., Danso-Appiah, T., Sackeyfio, J., Koram, K., Amoah, A. G. B. Assessment of oral health status in a Ghanaian population: rationale, methods, and population characteristics. BMC oral health. 2022, 22(1), 67. |
| [17] | Jönsson, B., Holde, G. E., Baker, S. R. The role of psychosocial factors and treatment need in dental service use and oral health among adults in Norway. Community dentistry and oral epidemiology. 2020, 48(3), 215–224. |
| [18] | Lawal, F. B., Taiwo, J. O., Oke, G. A. Factors influencing awareness and attendance of traditional oral health care practices by residents of a peri-urban community in Ibadan, Nigeria. African health sciences. 2015, 15(1), 233-239. |
| [19] | Lawal, F. B., Taiwo, J. O., Arowojolu, M. O., Howitt, L. Factors influencing utilisation of oral health care services in Nigeria. BMC Oral Health. 2020, 20(1), 1–9. |
| [20] | Luo, H., Wu, Q., Bell, R. A., Wright, W., Quandt, S. A., Basu, R., Moss, M. E. Rural-Urban Differences in Dental Service Utilisation and Dental Service Procedures Received Among US Adults: Results From the 2016 Medical Expenditure Panel Survey. The Journal of rural health: official journal of the American Rural Health Association and the National Rural Health Care Association. 2021, 37(3), 655–666. |
| [21] | Maia, A. C., Marques, M. J., Goes, A. R., Gama, A., Osborne, R., Dias, S. Health literacy strengths and needs among migrant communities from Portuguese-speaking African countries in Portugal: a cross-sectional study. Frontiers in Public Health. 2024, 12, 1415588. |
| [22] | Naavaal, S., Griffin, S. O., Jones, J. A. Impact of Making Dental Care Affordable on Quality of Life in Adults Aged 45 Years and Older. Journal of aging and health. 2020, 32(7-8), 861–870. |
| [23] | Northridge, M. E., Kumar, A., & Kaur, R. (2020). Disparities in Access to Oral Health Care. Annual review of public health, 41, 513–535. |
| [24] | Okeigbemen, S. A., & Nnawuihe, C. U. (2015). Oral health trends and service utilisation at a rural outreach dental clinic, Udo, Southern Nigeria. Journal of International Society of Preventive & Community Dentistry, 5(2), 123-130. |
| [25] | Okoroafor, C. C., Okobi, O. E., Owodeha-Ashaka, M., Okobi, E., Oluseye, B., Ekpang, O. B., Aya, L. E., Owolabi, O. J., Oru-Betem, T. E., Nwafor, J. N. Dental Health Knowledge, Attitude, and Practice among University of Calabar Students. Cureus. 2023, 15(6), e40055. |
| [26] | Olabisi, A. A., Udo, U. A., Ehimen, U. G., Bashiru, B. O., Gbenga, O. O., Adeniyi, A. O. Prevalence of dental caries and oral hygiene status of a screened population in Port Harcourt, Rivers State, Nigeria. Journal of International Society of Preventive & Community Dentistry. 2015, 5(1), 59–63. |
| [27] | Omitola, O. G., Arigbede, A. O. Inequalities in oral health care utilisation in Nigeria. Journal of Oral Science. 2012, 54(1), 65–71. |
| [28] | Omotoso, K. O., Adesina, J., Adewole, O. G., Gbadegesin, T. F. Factors influencing healthcare-seeking behaviour of South African adolescents. Journal of Public Health. 2022, 30(10), 2427-2439. |
| [29] | Onuoha, O. O., Okereke, O. J., Ngwoke, G. O., Ekpechu, J. O. A. Influence of Cultural Factors on Health Seeking Behavior in Ebonyi State, South East, Nigeria. Nigerian Journal of Social Psychology. 2024, 7(2). |
| [30] | Opoku, P., Salu, S., Azornu, C. K., Komesuor, J. Oral health knowledge, practice, and associated factors among Junior High School students of Koforidua, Ghana: a cross-sectional study. BMC oral health. 2024, 24(1), 449. |
| [31] | Osadolor, O. O., Akaji, E. A., Otakhoigbogie, U., Amuta, H. C., Obi, D. I., Osadolor, A. J. Dental service utilisation of a rural population in Nigeria. International Journal of Dentistry Research. 2019, 4(2), 62-5. |
| [32] | Peres, M. A., Macpherson, L. M. D., Weyant, R. J., Daly, B., Venturelli, R., Mathur, M. R., Listl, S., Celeste, R. K., Guarnizo-Herreño, C. C., Kearns, C., Benzian, H., Allison, P., Watt, R. G. Oral diseases: a global public health challenge. Lancet (London, England). 2019, 394(10194), 249–260. |
| [33] | Petersen, P. E. The World Oral Health Report 2020: Continuous improvement of oral health in the 21st century. World Health Organization. 2020. |
| [34] | Robinson, V., Chidinma, D. Roles of Cooperatives in Rural Development in Ikwerre and Emohua Local Government Areas, Rivers State. International Journal of Applied Educational Research (IJAER). 2025, 3(6), 371-382. |
| [35] | Shomuyiwa, D. O., Bridge, G. Oral health of adolescents in West Africa: prioritizing its social determinants. Global health research and policy. 2023, 8(1), 28. |
| [36] | Soroye, M. O., Aikins, E. A., Eigbobo, J. O., Umanah, A. U. Utilisation of dental services among a selected population in a rural community in South-South, Nigeria. The Nigerian Health Journal. 2021, 21(1), 20-27. |
| [37] | Uguru, N., Onwujekwe, O., Uguru, C. C., Ogu, U. U. Achieving universal health coverage in Nigeria: the dilemma of accessing dental care in Enugu state, Nigeria, a mixed methods study. Heliyon. 2021, 7(1), e05977. |
| [38] | Ugwuanyi, G., Omale, J., Emaimo, J., Nweze, M., Hussain, B., Oladoja, M. Knowledge, Oral Hygiene Practices, and Barriers to Compliance among Adult Residents of Adankolo Community, Lokoja, Kogi State. International Journal of Research and Innovation in Social Science. 2025, 9(4), 3436-3443. |
| [39] | Umanah, A. U., Braimoh, O. B. Oral health-related knowledge, attitude and practices of adult residents in a rural community in Nigeria. Journal of Dentistry and Oral Hygiene. 2017, 9(6), 65–72. |
| [40] | Umanah, A. U., Eigbobo, J. O., Soroye, M. O. Awareness and utilisation of oral health services in rural communities of Southern Nigeria. Nigerian Journal of Clinical Practice. 2020, 23(6), 789–795. |
| [41] | Vundavalli, S., Babburi, S., Manyam, R., Indiran, M. A., Doppalapudi, R., Baig, M. N. Use of oral healthcare facilities for the screening of hyperglycaemia in dental patients with undiagnosed type-2 diabetes mellitus in Andhra Pradesh, India. Journal of Oral and Maxillofacial Pathology. 2025, 29(2), 274-280. |
| [42] | World Health Organization. Global oral health status report: Towards universal health coverage for oral health by 2030. WHO Press. 2022. |
| [43] | Zardak, A. N., Amini-Rarani, M., Abdollahpour, I., Eslamipour, F., Tahani, B. Utilisation of dental care among adult populations: a scoping review of applied models. BMC Oral Health. 2023, 23(1), 596. |
APA Style
Wegbom, A. I., Ndudim, O. M., Atuzie, Q. D., Ike-Wegbom, S. A., Emordi, N. A. (2026). Assessment of Professional Dental Care Utilisation Among Rural Dwellers in Ikwerre Local Government Area, Rivers State, Nigeria. Central African Journal of Public Health, 12(2), 64-75. https://doi.org/10.11648/j.cajph.20261202.12
ACS Style
Wegbom, A. I.; Ndudim, O. M.; Atuzie, Q. D.; Ike-Wegbom, S. A.; Emordi, N. A. Assessment of Professional Dental Care Utilisation Among Rural Dwellers in Ikwerre Local Government Area, Rivers State, Nigeria. Cent. Afr. J. Public Health 2026, 12(2), 64-75. doi: 10.11648/j.cajph.20261202.12
@article{10.11648/j.cajph.20261202.12,
author = {Anthony Ike Wegbom and Oluchi Mildred Ndudim and Queen Desmond Atuzie and Salome Amarachi Ike-Wegbom and Nnenna Ali Emordi},
title = {Assessment of Professional Dental Care Utilisation Among Rural Dwellers in Ikwerre Local Government Area, Rivers State, Nigeria},
journal = {Central African Journal of Public Health},
volume = {12},
number = {2},
pages = {64-75},
doi = {10.11648/j.cajph.20261202.12},
url = {https://doi.org/10.11648/j.cajph.20261202.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20261202.12},
abstract = {Background: Oral health is essential for overall health and quality of life. Yet, utilisation of professional dental services remains low in many rural communities in developing countries. This study assessed knowledge and determinants of dental care utilisation among rural residents of Ikwerre Local Government Area (LGA), Rivers State, Nigeria. Methods: A community-based, cross-sectional study was conducted among 300 adults selected using multistage sampling. The sample size was calculated using the Cochran formula. Of the 326 distributed questionnaires, 300 were completed, yielding a 92.0% response rate. Data were collected using a validated structured questionnaire (Cronbach’s alpha ≥ 0.7). Descriptive statistics summarised the variables, and Chi-square and binary logistic regression analyses identified factors associated with dental care utilisation. Statistical significance was set at p < 0.05. Results: Over half of respondents (52.6%) demonstrated good knowledge of oral health, and 89.0% were aware of dental services. However, only 15.7% had utilized professional dental care in the past year, mostly for pain or gum problems, while preventive visits were rare. Multivariate analysis showed that educational level, monthly income, and positive attitude towards dental care significantly predicted utilization (p < 0.001). Key barriers included preference for traditional remedies, fear of dental procedures, perceived lack of need, and cost. Conclusion: Despite high awareness, utilization of dental services in Ikwerre LGA remains low. Socio-economic status and attitudes, rather than knowledge alone, largely influence dental care-seeking behaviour. Interventions targeting oral health education, affordability, and attitude change are critical to improving dental service uptake in rural communities.},
year = {2026}
}
TY - JOUR T1 - Assessment of Professional Dental Care Utilisation Among Rural Dwellers in Ikwerre Local Government Area, Rivers State, Nigeria AU - Anthony Ike Wegbom AU - Oluchi Mildred Ndudim AU - Queen Desmond Atuzie AU - Salome Amarachi Ike-Wegbom AU - Nnenna Ali Emordi Y1 - 2026/03/04 PY - 2026 N1 - https://doi.org/10.11648/j.cajph.20261202.12 DO - 10.11648/j.cajph.20261202.12 T2 - Central African Journal of Public Health JF - Central African Journal of Public Health JO - Central African Journal of Public Health SP - 64 EP - 75 PB - Science Publishing Group SN - 2575-5781 UR - https://doi.org/10.11648/j.cajph.20261202.12 AB - Background: Oral health is essential for overall health and quality of life. Yet, utilisation of professional dental services remains low in many rural communities in developing countries. This study assessed knowledge and determinants of dental care utilisation among rural residents of Ikwerre Local Government Area (LGA), Rivers State, Nigeria. Methods: A community-based, cross-sectional study was conducted among 300 adults selected using multistage sampling. The sample size was calculated using the Cochran formula. Of the 326 distributed questionnaires, 300 were completed, yielding a 92.0% response rate. Data were collected using a validated structured questionnaire (Cronbach’s alpha ≥ 0.7). Descriptive statistics summarised the variables, and Chi-square and binary logistic regression analyses identified factors associated with dental care utilisation. Statistical significance was set at p < 0.05. Results: Over half of respondents (52.6%) demonstrated good knowledge of oral health, and 89.0% were aware of dental services. However, only 15.7% had utilized professional dental care in the past year, mostly for pain or gum problems, while preventive visits were rare. Multivariate analysis showed that educational level, monthly income, and positive attitude towards dental care significantly predicted utilization (p < 0.001). Key barriers included preference for traditional remedies, fear of dental procedures, perceived lack of need, and cost. Conclusion: Despite high awareness, utilization of dental services in Ikwerre LGA remains low. Socio-economic status and attitudes, rather than knowledge alone, largely influence dental care-seeking behaviour. Interventions targeting oral health education, affordability, and attitude change are critical to improving dental service uptake in rural communities. VL - 12 IS - 2 ER -
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Department of Public Health Sciences, Rivers State University, Port Harcourt, Nigeria
Information