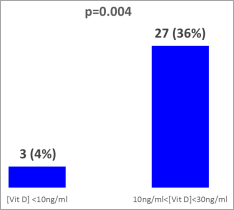
In addition to its role in phosphocalcic and bone metabolism, vitamin D also plays a global role in health. Despite high levels of sunshine, vitamin D deficiency remains a public health problem in sub-Saharan Africa, where sickle cell disease predominates. This study aimed to investigate an association between serum vitamin D (25(OH)D) levels and the occurrence of clinical and biological complications. The study was carried out in children with SS sickle cell disease aged 1 to 17 years (75 patients) matched to 17 AA controls. Plasma 25(OH)D concentration was obtained by immunoassay. The clinical complications studied were caso-occlusive crisis, osteomyelitis, osteonecrosis, acute chest syndrome, and priapism. Biological parameters included blood count, ionized calcium, and phosphorus. Statistical analysis was performed using R Studio 4.1.2 software. The significance threshold was 5%. Our study revealed a high prevalence of vaso-occlusive crisis (97%). Vitamin D deficiency was found in 4% of patients (3 SS patients) and 36% (27 SS patients) had a plasma concentration between 10 and 30 ng/ml. The association study revealed a negative association between vitamin D and the number of vaso-occlusive crises (r = -0.51; p < 0.001). We noted a positive association between vitamin D and blood calcium (r = 0.347; p < 0.002), phosphatemia (r = 0.347; p < 0.002), and hemoglobin (r = 0.243; p < 0.035). Vitamin D is correlated with certain clinical and biological complications. Vitamin D supplementation in children with sickle cell disease (SS) would therefore be relevant for better management of this disease.
| Published in | Advances in Biochemistry (Volume 12, Issue 2) |
| DOI | 10.11648/j.ab.20241202.15 |
| Page(s) | 85-91 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Sickle Cell Disease, Vitamin D, CVO, Ionized Calcium, Hemoglobin
Clinical manifestations | Effective (N) | Percentage (%) |
|---|---|---|
VOCs | 73 | 97.33 |
ACS | 05 | 6.66 |
Osteonecrosis | 15 | 20 |
Osteomyelitis | 15 | 20 |
Priapism | 01 | 1.33 |
Parameters | Case (N=75) | Controls AA (N=17) | p |
|---|---|---|---|
GB (103/mm3) | 17.42±6.34 | 9.15±5.27 | 0.03* |
Hb (g/dl) | 7.94±1.54 | 10.97±1.49 | 0.003* |
MCV (fl) | 85.06±7.88 | 80.12±7.7 | 0.0109* |
MCH (pg) | 28.75±3.35 | 24.24±3.15 | 0.05 |
MCHC (g/dl) | 33.77±1.96 | 30.09±2.20 | 0.120 |
Vitamin D (ng/ml) | 37.91±13.41 | 35.16±13.33 | 0.44 |
Ionized calcium (mmol/l) | 0.86±0.12 | 1.0 ±0.11 | 0.0094* |
Phosphatemia (mg/l) | 51.80±16.87 | 38.33±10.19 | 0.0022* |
25(OH)D (ng/mL) | ||
|---|---|---|
VOC | r | 0,51 |
p-value | < 0,001** | |
Osteomyelitis | r | 1 |
p-value | ||
Osteonecrosis | r | 1 |
p-value | ||
Ca2+ (mmol/L) | r | 0,347** |
p-value | 0,002** | |
Phosphatemia (mg/l) | r | 0,347** |
p-value | 0,002** | |
Hb (mg/dl) | r | 0,243* |
p-value | 0,035* | |
VOC | Vaso-Occlusive Crisis |
ACS | Acute Chest Syndrome |
BMD | Bone Mineral Density |
ABMD | Apparent Bone Mineral Density |
| [1] | Mogire RM, Mutua A, Kimita W, Kamau A, Bejon P, Pettifor JM, et al. Articles Prevalence of vitamin D deficiency in Africa: a systematic review and meta-analysis. Lancet Glob Heal. 2019; 25(19): 1–9. |
| [2] | Aude Tonson, Alexndre Wilhelm, Elsa Gonzalez EG. Le point sur la vitamine D [Vitamin D update]. Paediatrica. 2012 ; 23(409): 18–9. |
| [3] | Garrido C, Bardón-Cancho EJ, Fajardo-Sánchez V de los Á, Cascón-Pérez-Teijón ME, García-Morín M, Cela E, et al. Evaluation of the effectiveness of prophylactic oral vitamin D (cholecalciferol) in children with sickle cell disease. Bone. avr 2020; 133: 115228. |
| [4] | García Chumillas V, Borrego García E, González Martínez MÁ. Severe hyperphosphatemia and hypernatremia induced by sodium phosphate enemas. Med Clin (Barc). 2023 Aug 9. |
| [5] | Thiam L, Dramé A, Coly IZ, Diouf FN, Seck N, Boiro D, Ndongo AA, Basse I, Niang B, Deme/Ly I, Sylla A, Diagne I, Ndiaye O. Profils épidémiologiques, cliniques et hématologiques de la drépanocytose homozygote SS en phase inter critique chez l’enfant à Ziguinchor, Sénégal. [Epidemiological, clinical and hematological profiles of SS homozygous sickle cell disease in the intercritical phase in children in Ziguinchor, Senegal]. Pan Afr Med J. 2017 Nov 7; 28: 208. |
| [6] | Boiro D, Guèye M, Thiongane A, Ndongo A, Houngbadji M, Keita Y, et al. Drépanocytose chez l’enfant, profils clinique et évolutif: à propos de 138 cas suivis au service de pédiatrie de l’hôpital Abass Ndao de Dakar.[Sickle cell disease in children, clinical and evolutionary profiles: about 138 cases followed at the pediatric department of Abass Ndao Hospital, Dakar]. Médecine Afr Noire. 1 juin 2016; 63: 326‑32. |
| [7] | Yé Diarra, Koueta F, Dao L, Kaboret S, Sawadogo A. Prise en charge de la drépanocytose en milieu pédiatrique : expérience du centre hospitalier universitaire pédiatrique Charles-De-Gaulle de Ouagadougou (Burkina Faso). [Management of sickle cell disease in the pediatric setting: experience of the Charles-De-Gaulle pediatric university hospital in Ouagadougou (Burkina Faso)]. Cahiers santé. 2008 Avril-Mai-Juin; 18(2): 71-5. |
| [8] | Labie D. La drépanocytose est de moins en moins monogénique. [Sickle cell disease is becoming less and less monogenic]. Hématologie. 2009 Janvier-Février; 15(1): 98-9. |
| [9] | Kedy Koum, D., Penda, C. I., Mbiki Yema, R., Eposse, C., Endale Mangamba, L. M. and Koki Ndombo, P. 2018. Statut Vaccinal des Enfants Drépanocytaires Homozygotes À l’Hôpital Laquintinie de Douala, Cameroun. [Vaccination Status of Homozygous Sickle Cell Children at Laquintinie Hospital, Douala, Cameroon]. HEALTH SCIENCES AND DISEASE. 19, 4 (Oct. 2018). |
| [10] | I. Diagne, N. R. Diagne-Guèye, A. L. Fall, I. Déme, A. Sylla, J. I. Coly, B. Camara, H. D. Sow. Aspects épidémiologiques et évolutifs de la splénomégalie chez les enfants et adolescents porteurs de syndromes drépanocytaires majeurs au Sénégal. [Epidemiological and evolutionary aspects of splenomegaly in children and adolescents with major sickle cell syndromes in Senegal]. Archives de Pédiatrie, Volume 17, Issue 7, 2010, Pages 1017-1025. |
| [11] | Isabelle M. N., Ngo Njock, V., Alima Yanda, A.., Kamo Doka, H.., Mbono betoko, R.., Nengom, T.., Epee Ngoue, J., Ngo Um Sap,. S., & Chelo, D. (2021). Corrélation entre le Taux Sanguin de la 25(OH)D et les Crises Vaso-Occlusives chez les Enfants Drépanocytaires SS. [Correlation between 25(OH)D Blood Level and Vaso-Occlusive Crisis in SS Sickle Cell Children] HEALTH SCIENCES AND DISEASE, 22(10). |
| [12] | Gueye Tall F, Ndour EHM, Cissé F, Gueye PM, Ndiaye Diallo R, Diatta A, Lopez Sall P, Cissé A. Perturbations de paramètres lipidiques au cours de la drépanocytose. [Perturbations of lipid parameters in sickle cell disease. sickle cell disease]. Revue CAMES SANTE. Vol. 2(2), pp. 35-41, Décembre 2014. |
| [13] | Oladipo OO, Temiye EO, Ezeaka VC, Obomanu P. Serum magnesium, phosphate and calcium in Nigerian children with sickle cell disease. West Afr J Med. 2005 Apr-Jun; 24(2): 120-3. |
| [14] | Litosch I, Lee KS. Sickle red cell calcium metabolism: studies on Ca2+-Mg2+ ATPase and Ca-binding properties of sickle red cell membranes. Am J Hematol. 1980; 8(4): 377-87. |
| [15] | Bordbar MR, Haghpanah S, Zarei T, Dabbaghmanesh MH, Omrani GR, Saki F. Evaluation of bone mineral density in children with sickle-cell anemia and its associated factors in the south of Iran: a case-control study. Arch Osteoporos. 2017 Dec; 12(1): 70. |
| [16] | Chapelon E, Garabédian M, Brousse V, Souberbielle JC, Bresson JL, de Montalembert M. Ostéopénie et déficit en vitamine D chez les enfants drépanocytaires. [Osteopenia and vitamin D deficiency in dre-panocytic children]. Arch Pediatr. 2009 Jun; 16(6): 619-21. |
| [17] | Al-Harbi N, Annobil SH, Abbas F, Adzaku F, Bassuni W. Renal reabsorption of phosphate in children with sickle cell anemia. Am J Nephrol. 1999; 19(5): 552-4. |
| [18] | Smith EC, Valika KS, Woo JE, O'Donnell JG, Gordon DL, Westerman MP. Serum phosphate abnormalities in sickle cell anemia. Proc Soc Exp Biol Med. 1981 Nov; 168(2): 254-8. |
| [19] | Nolan VG, Nottage KA, Cole EW, Hankins JS, Gurney JG. Prevalence of vitamin D deficiency in sickle cell disease: a systematic review. PLoS One. 2015 Mar 3; 10(3): e0119908. |
| [20] | Chow LH, Frei JV, Hodsman AB, Valberg LS. Low serum 25-hydroxyvitamin D in hereditary hemochromatosis: relation to iron status. Gastroenterology. 1985 Apr; 88(4): 865-9. |
| [21] | Napoli N, Carmina E, Bucchieri S, Sferrazza C, Rini GB, Di Fede G. Low serum levels of 25-hydroxy vitamin D in adults affected by thalassemia major or intermedia. Bone. 2006 Jun; 38(6): 888-92. |
| [22] | Mahaseth, H., Vercellotti, G. M., Welch, T. E., Bowlin, P. R., Sonbol, K. M., Hsia, C. J. C., Li, M., Bischof, J. C., Hebbel, R. P., and Belcher, J. D. (2005) Polynitroxyl albumin inhibits inflammation and vas occlusion in transgenic sickle mice, J. Lab. Clin. Med 145, 204–211. |
| [23] | Norman AW. From vitamin D to hormone D: fundamentals of the vitamin D endocrine system essential for good health. Am J Clin Nutr. 2008 Aug; 88(2): 491S-499S. |
| [24] | Bikle DD. Vitamin D metabolism, mechanism of action, and clinical applications. Chem Biol. 2014 Mar 20; 21(3): 319-29. |
| [25] | Grégoire-Pelchat P, Alos N, Ribault V, Pastore Y, Robitaille N, Mailhot G. Vitamin D Intake and Status of Children With Sickle Cell Disease in Montreal, Canada. J Pediatr Hematol Oncol. 2018 Nov; 40(8): e531-e536. |
| [26] | Winters AC, Kethman W, Kruse-Jarres R, and Kanter J. Vitamin D Insufficiency is a Frequent Finding in Pediatric and Adult Patients with Sickle Cell Disease and Correlates with Markers of Cell Turnover., J Nutr Disorders Ther 2014, 4: 2. |
| [27] | Adegoke SA, Braga JAP, Adekile AD, Figueiredo MS. The Association of Serum 25-Hydroxyvitamin D With Biomarkers of Hemolysis in Pediatric Patients With Sickle Cell Disease. J Pediatr Hematol Oncol. 2018 Mar; 40(2): 159-162. |
| [28] | Bouillon R, Okamura WH, Norman AW. Structure-function relationships in the vitamin D endocrine system. Endocr Rev. 1995 Apr; 16(2): 200-57. |
| [29] | Haussler MR, Whitfield GK, Haussler CA, Hsieh JC, Thompson PD, Selznick SH, Dominguez CE, Jurutka PW. The nuclear vitamin D receptor: biological and molecular regulatory properties revealed. J Bone Miner Res. 1998 Mar; 13(3): 325-49. |
APA Style
Tall, F. G., Kandji, P. M., Ndour, E. H. M., Mbancké, S. S., Djité, M., et al. (2024). Association Between Serum 25(OH)D Concentration and Clinical and Biological Complications in Pediatric Patients with Sickle Cell Disease. Advances in Biochemistry, 12(2), 85-91. https://doi.org/10.11648/j.ab.20241202.15
ACS Style
Tall, F. G.; Kandji, P. M.; Ndour, E. H. M.; Mbancké, S. S.; Djité, M., et al. Association Between Serum 25(OH)D Concentration and Clinical and Biological Complications in Pediatric Patients with Sickle Cell Disease. Adv. Biochem. 2024, 12(2), 85-91. doi: 10.11648/j.ab.20241202.15
@article{10.11648/j.ab.20241202.15,
author = {Fatou Gueye Tall and Pape Matar Kandji and El Hadji Malick Ndour and Serigne Saliou Mbancké and Moustapha Djité and Oumou Kesso Barry and Aynina Cissé and Philoméne Lopez Sall and Papa Madièye Gueye},
title = {Association Between Serum 25(OH)D Concentration and Clinical and Biological Complications in Pediatric Patients with Sickle Cell Disease
},
journal = {Advances in Biochemistry},
volume = {12},
number = {2},
pages = {85-91},
doi = {10.11648/j.ab.20241202.15},
url = {https://doi.org/10.11648/j.ab.20241202.15},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ab.20241202.15},
abstract = {In addition to its role in phosphocalcic and bone metabolism, vitamin D also plays a global role in health. Despite high levels of sunshine, vitamin D deficiency remains a public health problem in sub-Saharan Africa, where sickle cell disease predominates. This study aimed to investigate an association between serum vitamin D (25(OH)D) levels and the occurrence of clinical and biological complications. The study was carried out in children with SS sickle cell disease aged 1 to 17 years (75 patients) matched to 17 AA controls. Plasma 25(OH)D concentration was obtained by immunoassay. The clinical complications studied were caso-occlusive crisis, osteomyelitis, osteonecrosis, acute chest syndrome, and priapism. Biological parameters included blood count, ionized calcium, and phosphorus. Statistical analysis was performed using R Studio 4.1.2 software. The significance threshold was 5%. Our study revealed a high prevalence of vaso-occlusive crisis (97%). Vitamin D deficiency was found in 4% of patients (3 SS patients) and 36% (27 SS patients) had a plasma concentration between 10 and 30 ng/ml. The association study revealed a negative association between vitamin D and the number of vaso-occlusive crises (r = -0.51; p < 0.001). We noted a positive association between vitamin D and blood calcium (r = 0.347; p < 0.002), phosphatemia (r = 0.347; p < 0.002), and hemoglobin (r = 0.243; p < 0.035). Vitamin D is correlated with certain clinical and biological complications. Vitamin D supplementation in children with sickle cell disease (SS) would therefore be relevant for better management of this disease.
},
year = {2024}
}
TY - JOUR T1 - Association Between Serum 25(OH)D Concentration and Clinical and Biological Complications in Pediatric Patients with Sickle Cell Disease AU - Fatou Gueye Tall AU - Pape Matar Kandji AU - El Hadji Malick Ndour AU - Serigne Saliou Mbancké AU - Moustapha Djité AU - Oumou Kesso Barry AU - Aynina Cissé AU - Philoméne Lopez Sall AU - Papa Madièye Gueye Y1 - 2024/06/19 PY - 2024 N1 - https://doi.org/10.11648/j.ab.20241202.15 DO - 10.11648/j.ab.20241202.15 T2 - Advances in Biochemistry JF - Advances in Biochemistry JO - Advances in Biochemistry SP - 85 EP - 91 PB - Science Publishing Group SN - 2329-0862 UR - https://doi.org/10.11648/j.ab.20241202.15 AB - In addition to its role in phosphocalcic and bone metabolism, vitamin D also plays a global role in health. Despite high levels of sunshine, vitamin D deficiency remains a public health problem in sub-Saharan Africa, where sickle cell disease predominates. This study aimed to investigate an association between serum vitamin D (25(OH)D) levels and the occurrence of clinical and biological complications. The study was carried out in children with SS sickle cell disease aged 1 to 17 years (75 patients) matched to 17 AA controls. Plasma 25(OH)D concentration was obtained by immunoassay. The clinical complications studied were caso-occlusive crisis, osteomyelitis, osteonecrosis, acute chest syndrome, and priapism. Biological parameters included blood count, ionized calcium, and phosphorus. Statistical analysis was performed using R Studio 4.1.2 software. The significance threshold was 5%. Our study revealed a high prevalence of vaso-occlusive crisis (97%). Vitamin D deficiency was found in 4% of patients (3 SS patients) and 36% (27 SS patients) had a plasma concentration between 10 and 30 ng/ml. The association study revealed a negative association between vitamin D and the number of vaso-occlusive crises (r = -0.51; p < 0.001). We noted a positive association between vitamin D and blood calcium (r = 0.347; p < 0.002), phosphatemia (r = 0.347; p < 0.002), and hemoglobin (r = 0.243; p < 0.035). Vitamin D is correlated with certain clinical and biological complications. Vitamin D supplementation in children with sickle cell disease (SS) would therefore be relevant for better management of this disease. VL - 12 IS - 2 ER -
Pharmaceutical Biochemistry Laboratory, Faculty of Medicine and Pharmacy, Cheikh Anta Diop University, Dakar, Senegal; Medical Biology Analysis Laboratory, Hôpital Alber Royer, Dakar, Senegal
Pharmaceutical Biochemistry Laboratory, Faculty of Medicine and Pharmacy, Cheikh Anta Diop University, Dakar, Senegal
Pharmaceutical Biochemistry Laboratory, Faculty of Medicine and Pharmacy, Cheikh Anta Diop University, Dakar, Senegal; Medical Biology Analysis Laboratory, Hôpital Alber Royer, Dakar, Senegal
Medical Biology Analysis Laboratory, Hôpital Alber Royer, Dakar, Senegal
Pharmaceutical Biochemistry Laboratory, Faculty of Medicine and Pharmacy, Cheikh Anta Diop University, Dakar, Senegal
Pharmaceutical Biochemistry Laboratory, Faculty of Medicine and Pharmacy, Cheikh Anta Diop University, Dakar, Senegal
Pharmaceutical Biochemistry Laboratory, Faculty of Medicine and Pharmacy, Cheikh Anta Diop University, Dakar, Senegal
Information