Background: Unsafe abortion continues to be a serious public health problem worldwide, especially in developing countries it is one of the leading preventable causes of maternal death and disabilities. Evidence-based programs have paramount importance in women's health improvement. However, only limited information about unsafe abortion and its determinants are available in the study setting. We aimed to assess magnitude and factors of unsafe abortion among reproductive-age women who underwent post-abortion care at Public Hospitals in West Arsi Zone of Ethiopia, 2018. A cross-sectional study employed to involve 399 women. Data collected by using an interviewer-applied questionnaire then entered into EPI-Info and exported to SPSS software for analysis. Bivariate and multivariate regression analysis was done to get OR and its 95% CI at p < 0.05. Response rate was 99 percent. Unsafe abortion practice was 41 percent. Key risk factors including younger age group 16-19 ((adjusted OR (95% CI); 9.23 (2.1, 40.17)), unplanned pregnancy ((adjusted OR (95% CI); 3.26 (1.39, 7.69)), increase the risk while having had previous experience of abortion ((adjusted OR (95% CI); 0.32 (0.13, 0.81)) and low monthly family income ((adjusted OR (95% CI); 0.20 (0.07, 0.60)) were the preventives of unsafe abortion. This study showed unsafe abortion is yet women’s health challenge. Being in a younger age group, and those with unplanned pregnancy, were among the key risky while those who have repeated experiences of abortion previously, and those who are from a lower monthly income group were less likely do unsafe abortion in the study setting. Health programmers and implementers expected to address them and a more explorative study recommended.
| Published in | Science Futures (Volume 2, Issue 2) |
| DOI | 10.11648/j.scif.20260202.16 |
| Page(s) | 158-168 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Abortion, Maternal Mortality, Unwanted Pregnancy, Unintended Pregnancy, Ethiopia
Variables | Categories | Frequency | Percent |
|---|---|---|---|
Age | |||
15-19 | 53 | 13.41 | |
20-24 | 97 | 24.56 | |
25-29 | 100 | 25.32 | |
30-34 | 67 | 16.96 | |
35-44 | 78 | 19.75 | |
Religion | |||
Orthodox | 100 | 25.32 | |
Muslim | 191 | 48.35 | |
Protestant | 58 | 14.68 | |
Catholic | 29 | 7.34 | |
Others* | 17 | 4.31 | |
Ethnic group | |||
Oromo | 282 | 71.39 | |
Amhara | 64 | 16.20 | |
Guragie | 35 | 8.87 | |
Others** | 14 | 3.54 | |
Marital status | |||
Single | 73 | 18.48 | |
Married currently | 276 | 69.87 | |
Divorced | 29 | 7.34 | |
Widowed | 8 | 2.03 | |
Separated | 9 | 2.27 | |
Age at first pregnancy (years) | |||
15-18 | 120 | 30.40 | |
>18 | 275 | 69.60 | |
Residence | |||
Urban | 267 | 67.60 | |
Rural | 128 | 32.40 | |
Occupation | |||
Student | 73 | 18.48 | |
Housewife | 137 | 34.68 | |
Self Employed | 101 | 25.57 | |
Governmental employed | 67 | 16.96 | |
Daily laborers | 17 | 4.31 | |
Monthly income of the respondent (Ethiopian birr) | |||
Dependent on family | 55 | 13.92 | |
<1000 | 91 | 23.04 | |
1001-2000 | 100 | 25.32 | |
>2000 | 149 | 37.72 | |
The completed education level of the woman | |||
Cannot read and write | 64 | 16.20 | |
Read and write | 50 | 12.70 | |
Elementary school | 85 | 21.50 | |
Secondary school | 79 | 20.00 | |
College and above | 117 | 29.60 | |
The completed education level of partner (n=321) | |||
Cannot read and write | 25 | 7.79 | |
Reading and writing | 38 | 13.84 | |
Elementary school | 58 | 18.07 | |
Secondary school | 62 | 19.31 | |
College and above | 138 | 42.99 | |
Family Size of the respondent | |||
Only 1 member | 174 | 44.05 | |
1-5 members | 127 | 32.15 | |
6-10 members | 54 | 13.67 | |
>10 members | 40 | 10.13 | |
Variables | Category | Frequency | Percent |
|---|---|---|---|
Parity of the woman | |||
Para 0-1 | 237 | 60.00 | |
Para >2 | 158 | 40.00 | |
Information heard about family planning | |||
Yes | 286 | 72.40 | |
No | 109 | 27.60 | |
Where contraceptive was available (n=286) | |||
Governmental Health center | 82 | 28.67 | |
Governmental hospital | 83 | 29.02 | |
Private clinic/hospital | 64 | 22.38 | |
Pharmacy | 31 | 10.84 | |
Health Extension Workers | 26 | 9.09 | |
Family planning utilization history (n=286) | |||
Previously used | 212 | 74.13 | |
Currently using | 74 | 25.87 | |
Types of methods used (n=286) | |||
OCP | 127 | 44.41 | |
Depo | 87 | 30.41 | |
Implant | 48 | 16.78 | |
IUCD | 13 | 4.55 | |
Permanent | 11 | 3.85 | |
For what purpose family planning was used (n=286) | |||
For birth spacing | 186 | 65.03 | |
For birth limiting | 100 | 34.97 | |
A reason not used family planning (n=109) | |||
Fear of side effect | 37 | 33.94 | |
Lack of awareness | 25 | 22.94 | |
To have more children | 22 | 20.18 | |
Husband disapproval | 25 | 22.94 | |
Current pregnancy wanted (n=395) | |||
Yes | 254 | 64.30 | |
No | 141 | 35.70 | |
Variable | Category | Frequency | Percent |
|---|---|---|---|
History of previous abortion (n=395) | |||
Yes | 206 | 52.20 | |
No | 189 | 47.80 | |
Number of previous abortion (n=206) | |||
One | 131 | 63.59 | |
Two | 58 | 28.16 | |
≥ Three | 17 | 8.25 | |
Types of previous abortion (n=206) | |||
Induced | 74 | 35.90 | |
Spontaneous | 132 | 64.10 | |
Who performed the abortion? (n=206) | |||
Self | 11 | 5.34 | |
Local abortionist | 23 | 11.17 | |
Skilled health personnel | 172 | 83.49 | |
Gestational age of current abortion (n=395) | |||
Up to 12 weeks | 217 | 54.90 | |
13-28 weeks | 178 | 45.10 | |
Causes of current bleeding/Abortion (n=395) | |||
Self-induced | 156 | 39.50 | |
Spontaneous | 239 | 60.50 | |
Current abortion performed in a health facility or out of a health facility (n=395) | |||
Out of health facility | 162 | 41.00 | |
In a health facility | 233 | 59.00 | |
Types of procedures used for controlling post-abortion bleeding (n=395) | |||
Oral medication | 148 | 37.50 | |
Vaginal procedure | 247 | 62.50 | |
It is better to have a legal or free abortion (n=395) | |||
Strongly agree | 177 | 44.80 | |
Agree | 78 | 19.70 | |
Not agree | 107 | 27.10 | |
I do not know | 33 | 8.40 | |
Status of current abortion | |||
safe | 233 | 58.99% | |
unsafe | 162 | 41.01% | |
Awareness of the presence of safe abortion service in Ethiopia (n=395) | |||
Yes | 229 | 58.00 | |
No | 166 | 42.00 | |
The legality of abortion for any condition in Ethiopia (n=395) | |||
Yes; for all reason | 50 | 12.66 | |
Yes; for some reason | 162 | 41.01 | |
No | 135 | 34.18 | |
Not sure | 48 | 12.15 | |
Aware of unsafe abortion (n=395) | |||
Yes | 218 | 55.20 | |
No | 177 | 44.80 | |
Definitions of unsafe abortion (n=395) | |||
When performed by unskilled personnel | 7 | 1.80 | |
When performed in an unsafe environment | 12 | 3.00 | |
Both | 205 | 51.90 | |
Not know | 171 | 43.30 | |
What happens if abortion is legalized? | |||
It aggravates unsafe abortion | 1 | 0.30 | |
It minimizes unsafe abortion | 200 | 50.60 | |
It neither aggravates nor minimizes it | 43 | 10.90 | |
I don't know | 151 | 38.20 | |
Your decision for future unwanted pregnancy (n=395) | |||
Giving birth | 149 | 37.72 | |
Abort | 176 | 44.56 | |
Leave the place of residence | 37 | 9.37 | |
Self-suicide | 33 | 8.35 | |
Heard about the safe termination of unwanted pregnancy? | |||
Yes | 218 | 55.20 | |
No | 177 | 44.80 | |
Who told you heard about the safe termination of unwanted pregnancy? (n=218) | |||
Health professionals | 154 | 38.99 | |
TV or radio | 28 | 7.09 | |
Family or friends | 22 | 5.57 | |
School or health facility | 14 | 3.54 | |
The nearest health center has necessary facilities to provide abortion services (n=395) | |||
Yes | 220 | 55.70 | |
No | 175 | 44.30 | |
Variables | Categories | Current Abortion type | Crude OR (95% CI) | Adjusted OR (95% CI) | |
|---|---|---|---|---|---|
Unsafe | Safe | ||||
Age | |||||
15-19 | 26 | 27 | 0.46(.22,0.95)* | 9.23(2.1,40.17)** | |
20-24 | 42 | 55 | 0.58(0.31,1.09) | 1.66(0.54,5.12) | |
25-29 | 43 | 57 | 0.59(0.32,2.00) | 2.22(0.75,6.63) | |
30-34 | 27 | 40 | 0.66(0.33,1.31) | 1.00(0.30,3.31) | |
35-44 | 24 | 54 | 1.00 | 1.00 | |
Women's educational status | |||||
cannot read and write | 18 | 46 | 3.31(1.72,6.37)* | 0.86(0.22,3.37) | |
reading and write | 16 | 34 | 2.75(1.37,5.52)* | 0.43(0.13,1.47) | |
elementary school | 37 | 48 | 1.68(0.96,2.95) | 1.27(0.45,3.59) | |
secondary school | 25 | 54 | 2.80(1.54,5.09)* | 0.50(0.18,1.39) | |
college and above | 66 | 51 | 1.00 | 1.00 | |
Family's monthly income | |||||
dependent on family | 29 | 26 | 0.89(0.48,1.64) | 1.70(0.52,5.58) | |
<1000 birr | 19 | 72 | 3.74(2.05,6.81)* | 0.20(0.07,0.60)** | |
1001-2000 birr | 40 | 60 | 1.480(0.89,2.47) | 1.42(0.55,3.68) | |
>2000 birr | 74 | 75 | 1.00 | 1.00 | |
Number of pregnancy | |||||
The first | 73 | 74 | 0.57(0.38,0.86)* | 2.02(0.45,9.04) | |
The second and above | 89 | 159 | 1.00 | 1.00 | |
Parity | |||||
Para 0-1 | 109 | 128 | 0.59(0.39,0.90)* | 0.88(0.3,2.59) | |
Para >2 | 53 | 105 | 1.98 | 1.00 | |
History of previous abortion | |||||
Yes | 71 | 135 | 1.77(1.18,2.65)* | 0.32(0.13,0.81)** | |
No | 91 | 98 | 1.00 | 1.00 | |
Status of current pregnancy | |||||
Unplanned | 54 | 102 | 1.56(1.03,2.36)* | 3.26(1.39,7.69)** | |
Planned | 108 | 131 | 1.00 | 1.00 | |
OR | Odds Ratio |
EDHS | Ethiopia Demographic and Health Survey |
SPSS | Statistical Package for Social Science |
WHO | World Health Organization |
| [1] |
WHO. Global and regional estimates of the incidence of unsafe abortion and associated mortality in 2008. World Health Organization, 2011. 6th ed.
https://apps.who.int/iris/bitstream/10665/44529/1/9789241501118_eng.pdf |
| [2] |
WHO. Clinical practice handbook for safe abortion. World Health Organization. 2014.
https://www.who.int/reproductivehealth/publications/unsafe_abortion/clinical-pr |
| [3] | Lisa B, Haddad M, Nawal M. Unsafe Abortion: Unnecessary Maternal Mortality. Reviews in obstetrics and gynecology. 2009; 2(2). |
| [4] | Mishra V, Gaigbe-Togbe MV, Ferre MJ. Abortion policies and reproduction health around the World. 2014. |
| [5] | Dibaba SDY, Fetters T, Moore A, Gebreselassie H, Gebrehiwot Y, Bonson J. A decade of progress providing safe abortion services in Ethiopia: Results of national assessments in 2008 and 2014. BMC pregnancy and childbirth. 2017. |
| [6] |
Demtsu B, Bugssa G, Alemu A. Assessment of Quality and determinant Factors of Post-Abortion are in Governmental Hospitals of Tigray, Ethiopia, 2013. Family Medicine and Medical Science Research. 2014.
https://www.longdom.org/open-access/assessment-of-quality-and-determina |
| [7] |
Gebeyehu D, Admassu B, Sinega M, Haile M. Assessment of prevalence and reasons for termination of pregnancy at Jimma University Teaching Hospital, Ethiopia. Universal Journal of Public Health. 2015; 3(6).
https://www.researchgate.net/publication/285538193_Assessment_of_Prevalen |
| [8] | Fantahun MA, Yeneneh H, Seid A, Belete S, Yimer B, Gizaw A, et al. Acceptability of the involvement of health extension workers (HEWs) in medical abortion (MA): the perspectives of clients, service providers and trained HEWs in East Shoa and Arsi Zones, Oromia Region, Ethiopia. Ethiop Med J. 2015, 53(1). |
| [9] |
Barot S. The roadmap to Safe Abortion Worldwide: Lesson from New Global Trends on Incidence, Legality, and Safety. Guttmacher Policy Review, 2018; 21.
https://www.guttmacher.org/gpr/2018/03/roadmap-safe-abortion-worldwide-less |
| [10] |
Singh S, Zimet M. Facility-based treatment for medical complications resulting from unsafe pregnancy termination in the developing world, 2012: a review of evidence from 26 countries. BJOG An International Journal of Obstetrics and Gynecology. 2015.
https://obgyn.onlinelibrary.wiley.com/doi/abs/10.1111/1471-0528.13552 |
| [11] |
Rocca CH, Puri M, Dulal B, Bajracharya L, Harper CC, Blum M, et al. Unsafe abortion after legalization in Nepal: a cross-sectional study of women presenting to hospitals, Internationa Journal of Obstetrics and Gynaecology. 2013; 120.
https://obgyn.onlinelibrary.wiley.com/doi/abs/10.1111/1471-0528.12242 |
| [12] | Gerdts C, Vohra D, Ahern J. Measuring Unsafe Abortion-Related Mortality: A systematic review of the Existing Methods. PLOS ONE2013; 8(1) |
| [13] |
Guttmacher Institute. Abortion in Africa. Guttmacher Institute, FACT SHEET March 2018. 125 Maiden lane New York, 10038, USA 212.248.1111.
https://www.guttmacher.org/sites/default/files/factsheet/ib_aww-africa.pdf |
| [14] | Ziraba AK, Izigbara C, Levandowski BA, Geberesilassie H, Mutua M, Mohamed SF, et al. Unsafe abortion in Kenya: a cross-sectional study of abortion complication severity and associated factors. BMC Pregnancy and Childbirth. 2015; 15(34). |
| [15] | Central Statistical Authority. Demographic and Health survey 2016 Key Indicators Report. Federal Democratic Republic of Ethiopia, Addis Ababa. 2016; 4. |
| [16] | Tessema GA, Laurence CO, Melaku YA, Misganaw A, Woldie SA, Hiruye A, et al.: Trends and causes of maternal mortality in Ethiopia during 1990–2013: findings from the Global Burden of Diseases study 2013. BMC Public Health (2017) 17: 160. |
| [17] |
WHO. Sustainable Development Goals. The Global Health Observatory Data. World Health Orgnanization, 2015.
https://repositorio.cepal.org/bitstream/handle/11362/40156/S1801140 en.pdf |
| [18] |
Guttmacher Institute. Induced Abortion and Postabortion Care in Ethiopia. Fact Sheet Guttmacher Institute. JANUARY 2017. 125 Maiden lane New York, 10038, USA 212.248.1111.
https://www.ipas.org/resource/induced-abortion-and-postabortion-care-in-ethiopia/ |
| [19] |
Charie N, Asmerom B. Proportion of safe abortion and associated factors among women who seek abortion care services in Family Guidance and Marie Stopes International Clinic in Dessie Town, North East Ethiopia. Journal of Public Health and Epidemiology. 2017; 9(10).
http://academicjournals.org/journal/JPHE/how-to-cite-article/F182B7C66417 |
| [20] |
Federal Democratic Republic of Ethiopia Population Census Commission. Summary and Statistical Report of the 2007 Population and Housing Census: Population size by Sex and age. UNFPA, December 2008, Addis Ababa, Ethiopia.
https://www.ethiopianreview.com/pdf/001/Cen2007_firstdraft(1).pdf |
| [21] | West Arsi Zone Health Office. Unpublished West Arsi Zone Health Office Report. 2017/18. |
| [22] | Tadesse LW, Tejineh SM, Kisi TB. Unsafe abortion and associated factors among women in the reproductive age group in Arsi Zone, Central Ethiopia. International Journal of Nursing and Midwifery. 2017; 9(10). |
| [23] |
Paul M, Gebreselassie H, Samai M, Benson J, Kargbo S, Lazzarino MM. Unsafe Abortion in Sieraleone: An Examination of Costs and Burden of Treatment on Health care Resources. Journal of Women's Health Care. 2015; 4(2).
https://www.longdom.org/abstract/unsafe-abortion-in-sierra-leone-an-examina |
| [24] |
Abinath Yogi A, Prakash K. C and Neupane S. Prevalence and factors associated with abortion and unsafe abortion in Nepal: a nationwide cross-sectional study. BMC Pregnancy and Childbirth, (2018) 18: 376.
https://bmcpregnancychildbirth.biomedcentral.com/articles/10.1186/s12884-0 |
| [25] |
Feyisso M, Girma A, Yimam H, Hailu S. Magnitude of unintended pregnancy and its determinants among pregnant women visiting Dilla University Referral Hospital, South Ethiopia. Journal of Women's Health Care. 2017; 6(4).
https://www.longdom.org/open-access/magnitude-of-unintended-pregnancy-and-its-determinants-a |
| [26] | Abebe Feyissa Amare, Dereje Gobena Alemayehu, Alemtsehay Adam Bogale. Factors associated with Unsafe Induced abortion among women who attended Fichie Hospital, Oromia, Ethiopia: Cross-sectional study. |
APA Style
Kasiye, T., Wodajo, L. T., Kare, Y., Gemechu, T. (2026). Magnitude and Factors Affecting Unsafe Abortion Among Reproductive-age Women Underwent Post-abortion Care at Public Hospitals in West Arsi Zone of Ethiopia. Science Futures, 2(2), 158-168. https://doi.org/10.11648/j.scif.20260202.16
ACS Style
Kasiye, T.; Wodajo, L. T.; Kare, Y.; Gemechu, T. Magnitude and Factors Affecting Unsafe Abortion Among Reproductive-age Women Underwent Post-abortion Care at Public Hospitals in West Arsi Zone of Ethiopia. Sci. Futures 2026, 2(2), 158-168. doi: 10.11648/j.scif.20260202.16
AMA Style
Kasiye T, Wodajo LT, Kare Y, Gemechu T. Magnitude and Factors Affecting Unsafe Abortion Among Reproductive-age Women Underwent Post-abortion Care at Public Hospitals in West Arsi Zone of Ethiopia. Sci Futures. 2026;2(2):158-168. doi: 10.11648/j.scif.20260202.16
@article{10.11648/j.scif.20260202.16,
author = {Tirune Kasiye and Legesse Tadesse Wodajo and Yalemwork Kare and Teshome Gemechu},
title = {Magnitude and Factors Affecting Unsafe Abortion Among Reproductive-age Women Underwent Post-abortion Care at Public Hospitals in West Arsi Zone of Ethiopia},
journal = {Science Futures},
volume = {2},
number = {2},
pages = {158-168},
doi = {10.11648/j.scif.20260202.16},
url = {https://doi.org/10.11648/j.scif.20260202.16},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.scif.20260202.16},
abstract = {Background: Unsafe abortion continues to be a serious public health problem worldwide, especially in developing countries it is one of the leading preventable causes of maternal death and disabilities. Evidence-based programs have paramount importance in women's health improvement. However, only limited information about unsafe abortion and its determinants are available in the study setting. We aimed to assess magnitude and factors of unsafe abortion among reproductive-age women who underwent post-abortion care at Public Hospitals in West Arsi Zone of Ethiopia, 2018. A cross-sectional study employed to involve 399 women. Data collected by using an interviewer-applied questionnaire then entered into EPI-Info and exported to SPSS software for analysis. Bivariate and multivariate regression analysis was done to get OR and its 95% CI at p < 0.05. Response rate was 99 percent. Unsafe abortion practice was 41 percent. Key risk factors including younger age group 16-19 ((adjusted OR (95% CI); 9.23 (2.1, 40.17)), unplanned pregnancy ((adjusted OR (95% CI); 3.26 (1.39, 7.69)), increase the risk while having had previous experience of abortion ((adjusted OR (95% CI); 0.32 (0.13, 0.81)) and low monthly family income ((adjusted OR (95% CI); 0.20 (0.07, 0.60)) were the preventives of unsafe abortion. This study showed unsafe abortion is yet women’s health challenge. Being in a younger age group, and those with unplanned pregnancy, were among the key risky while those who have repeated experiences of abortion previously, and those who are from a lower monthly income group were less likely do unsafe abortion in the study setting. Health programmers and implementers expected to address them and a more explorative study recommended.},
year = {2026}
}
TY - JOUR T1 - Magnitude and Factors Affecting Unsafe Abortion Among Reproductive-age Women Underwent Post-abortion Care at Public Hospitals in West Arsi Zone of Ethiopia AU - Tirune Kasiye AU - Legesse Tadesse Wodajo AU - Yalemwork Kare AU - Teshome Gemechu Y1 - 2026/01/30 PY - 2026 N1 - https://doi.org/10.11648/j.scif.20260202.16 DO - 10.11648/j.scif.20260202.16 T2 - Science Futures JF - Science Futures JO - Science Futures SP - 158 EP - 168 PB - Science Publishing Group SN - 3070-6289 UR - https://doi.org/10.11648/j.scif.20260202.16 AB - Background: Unsafe abortion continues to be a serious public health problem worldwide, especially in developing countries it is one of the leading preventable causes of maternal death and disabilities. Evidence-based programs have paramount importance in women's health improvement. However, only limited information about unsafe abortion and its determinants are available in the study setting. We aimed to assess magnitude and factors of unsafe abortion among reproductive-age women who underwent post-abortion care at Public Hospitals in West Arsi Zone of Ethiopia, 2018. A cross-sectional study employed to involve 399 women. Data collected by using an interviewer-applied questionnaire then entered into EPI-Info and exported to SPSS software for analysis. Bivariate and multivariate regression analysis was done to get OR and its 95% CI at p < 0.05. Response rate was 99 percent. Unsafe abortion practice was 41 percent. Key risk factors including younger age group 16-19 ((adjusted OR (95% CI); 9.23 (2.1, 40.17)), unplanned pregnancy ((adjusted OR (95% CI); 3.26 (1.39, 7.69)), increase the risk while having had previous experience of abortion ((adjusted OR (95% CI); 0.32 (0.13, 0.81)) and low monthly family income ((adjusted OR (95% CI); 0.20 (0.07, 0.60)) were the preventives of unsafe abortion. This study showed unsafe abortion is yet women’s health challenge. Being in a younger age group, and those with unplanned pregnancy, were among the key risky while those who have repeated experiences of abortion previously, and those who are from a lower monthly income group were less likely do unsafe abortion in the study setting. Health programmers and implementers expected to address them and a more explorative study recommended. VL - 2 IS - 2 ER -
Asasa Health Center, Asasa, Ethiopia
Department of Public Health, Arsi University, Asella, Ethiopia
Department of Public Health, Arsi University, Asella, Ethiopia
Kula District Hospital, Kula, Ethiopia
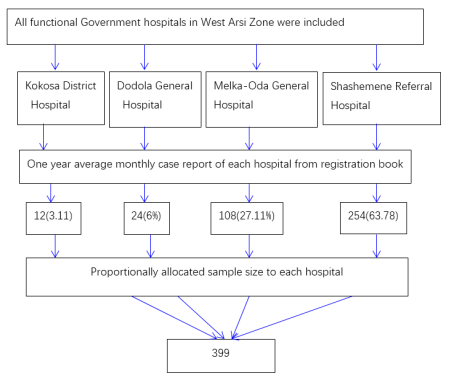
Figure 1. Schematic presentation of sampling procedure and Proportional allocation of total sample size to each functional Governmental Hospitals in West Arsi Zone, Oromia Region, Ethiopia, 2018.
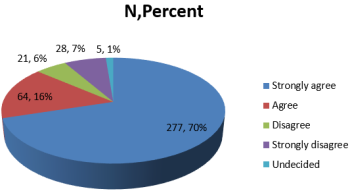
Figure 2. Serious problems can happen if a woman performs an abortion outside a health facility (n=395).
Information

