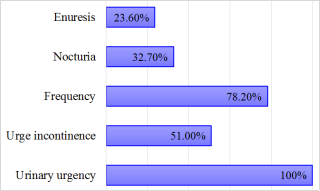
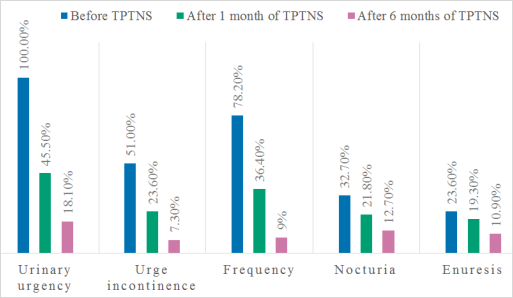
Background: Transcutaneous posterior tibial nerve stimulation (TPTNS) is a promising treatment modality for idiopathic overactive bladder (OAB) in the pediatric population. Objective: To evaluate the efficacy of TPTNS in children suffering from idiopathic OAB refractory to conventional therapies. Method: It is a retrospective study including children with clinical OAB syndrome refractory to treatment. The TPTNS protocol consisted of a daily 20-minute session (5 times per week, frequency 10 Hz, pulse width 200 µsec). All patients and family were instructed on how to use the device at home. Treatment efficacy was assessed based on perceived clinical improvement or success using a 3-day voiding diary and visual analog scale (VAS). The evaluation of treatment effectiveness was done after 1 and 6 months. Result: A total of 55 children were included in the study (31 girls and 24 boys), with a mean age of 10.6 ± 3.1 years. All patients experienced urinary urgency, 78.2% had frequency and 51% urge incontinence. 32.7% exhibited both daytime and nighttime symptoms. After one month of TPTNS, clinical outcomes showed improvement in 52 patients. The perceived improvement was more pronounced for daytime symptoms. After 6 months, 65.5% were considered cured while the remaining patients showed continued improvement. On the VAS, 72.7% assessed the improvement in symptoms as between 9/10 and 10/10. Conclusion: TPTNS represents a potentially effective and noninvasive treatment strategy for idiopathic OAB in children, showing significant symptom improvement without adverse effects. However, further research is needed to determine optimal treatment parameters.
| Published in | Rehabilitation Science (Volume 10, Issue 1) |
| DOI | 10.11648/j.rs.20251001.12 |
| Page(s) | 16-20 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Transcutaneous Posterior Tibial Nerve Stimulation, Neuromodulation, Overactive Bladder, Children
GABA | Gamma-aminobutyric Acid |
ICCS | International Children’s Continence Society |
OAB | Overactive Bladder |
ODC | Overactive Detrusor Contraction |
PTNS | Posterior Tibial Nerve Stimulation |
TENS | Transcutaneous Electrical Nerve Stimulation |
TPTNS | Transcutaneous Posterior Tibial Nerve Stimulation |
VAS | Visual Analog Scale |
| [1] | Austin PF, Bauer SB, Bower W, Chase J, Franco I, Hoebeke P, et al. The standardization of terminology of lower urinary tract function in children and adolescents: update report from the Standardization Committee of the International Children’s Continence Society. Neurourol Urodyn. 2016; 35(4): 471-81. |
| [2] | Franco I. Overactive bladder in children. Part 1: Pathophysiology. J Urol. 2007; 178(3): 761-8. |
| [3] | Ramsay S, Bolduc S. Overactive bladder in children. Can Urol Assoc J. 2017; 11(1-2 Suppl 1): S74-S79. |
| [4] | Chung JM, Lee SD, Kang DI, Kwon DD, Kim KS, Kim JH. Prevalence and associated factors of overactive bladder in Korean children 5-13 years old: a nationwide multicenter study. Urology. 2009; 73(1): 63-7. |
| [5] | Snow-Lisy DC. Management of overactive bladder in children. Curr Bladder Dysfunct Rep. 2018; 13(2): 38-45. |
| [6] | Fall M, Lindström S. Electrical stimulation: a physiologic approach to the treatment of urinary incontinence. Urol Clin North Am. 1991; 18(2): 393-407. |
| [7] | Parodi S, Kendall HJ, Terrone C, Heesakkers JPFA. What is in the pipeline on investigational neuromodulation techniques for lower urinary tract dysfunction: a narrative review. Neuromodulation. 2024; 27(2): 267-72. |
| [8] | Barroso U Jr, Lordêlo P. Electrical nerve stimulation for overactive bladder in children. Nat Rev Urol. 2011; 8(7): 402-7. |
| [9] | Cui H, Yao Y, Xu Z, Gao Z, Wu J, Zhou Z. Role of transcutaneous electrical nerve stimulation in treating children with overactive bladder from pooled analysis of 8 randomized controlled trials. Int Neurourol J. 2020; 24(2): 84-94. |
| [10] | Barroso U Jr, Viterbo W, Bittencourt J, Barroso DV, Lordêlo P. Posterior tibial nerve stimulation vs parasacral transcutaneous neuromodulation for overactive bladder in children. J Urol. 2013; 190(2): 673-7. |
| [11] | O'Sullivan H, Kelly G, Toale J, Cascio S. Comparing the outcomes of parasacral transcutaneous electrical nerve stimulation for the treatment of lower urinary tract dysfunction in children: a systematic review and meta-analysis of randomized controlled trials. Neurourol Urodyn. 2021; 40(2): 570-581. |
| [12] | Lombardo AM, Alpert SA. Third-line therapeutic interventions for non-neurogenic bladder dysfunction in children. Curr Urol Rep. 2024; 25: 331-8. |
| [13] | Wang ZH, Liu ZH. Treatment for overactive bladder: a meta-analysis of tibial versus parasacral neuromodulation. Medicine (Baltimore). 2022; 101(41): e31165. |
| [14] | Bower WF, Moore KH, Adams RD. A pilot study of the home application of transcutaneous neuromodulation in children with urgency or urge incontinence. J Urol. 2001; 166(6): 2420-2. |
| [15] | Hoebeke P, Van Laecke E, Everaert K, Renson C, De Paepe H, Raes A, Vande Walle J. Transcutaneous neuromodulation for the urge syndrome in children: a pilot study. J Urol. 2001; 166(6): 2416-9. |
| [16] | Lordêlo P, Soares PV, Maciel I, Macedo A Jr, Barroso U Jr. Prospective study of transcutaneous parasacral electrical stimulation for overactive bladder in children: long-term results. J Urol. 2009; 182(6): 2900-4. |
| [17] | Hagstroem S, Mahler B, Madsen B, Toft L, Djurhuus JC. Transcutaneous electrical nerve stimulation for refractory daytime urinary urge incontinence. J Urol. 2009; 182(4 Suppl): 2072-8. |
| [18] | Lordêlo P, Teles A, Veiga ML, Correia LC, Barroso U Jr. Transcutaneous electrical nerve stimulation in children with overactive bladder: a randomized clinical trial. J Urol. 2010; 184(2): 683-9. |
| [19] | De Paula LIDS, De Oliveira LF, Cruz BP, De Oliveira DM, Miranda LM, De Moraes Ribeiro M, et al. Parasacral transcutaneous electrical neural stimulation (PTENS) once a week for the treatment of overactive bladder in children: a randomized controlled trial. J Pediatr Urol. 2017; 13(3): 263. e 1-6. |
| [20] | Hoffmann A, Sampaio C, Nascimento AA, Lopes AA, Lordêlo P, Barroso U Jr. Predictors of outcome in children and adolescents with overactive bladder treated with parasacral transcutaneous electrical nerve stimulation. J Pediatr Urol. 2018; 14(1): 54. e 1-6. |
| [21] | De Gennaro M, Capitanucci ML, Mastracci P, Silveri M, Gatti C, Mosiello G. Percutaneous tibial nerve neuromodulation is well tolerated in children and effective for treating refractory vesical dysfunction. J Urol. 2004; 171(5): 1911-3. |
| [22] | Malm-Buatsi E, Nepple KG, Boyt MA, Austin JC, Cooper CS. Efficacy of transcutaneous electrical nerve stimulation in children with overactive bladder refractory to pharmacotherapy. Urology. 2007; 70(5): 980. e 3. |
| [23] | Tugtepe H, Thomas DT, Ergun R, Kocak T, Erdem E. The effectiveness of transcutaneous electrical neural stimulation therapy in patients with urinary incontinence resistant to initial medical treatment or biofeedback. J Pediatr Urol. 2015; 11(3): 137. e 1-5. |
| [24] | Hoebeke P, Renson C, Petillon L, Vande Walle J, De Paepe H. Percutaneous electrical nerve stimulation in children with therapy-resistant nonneuropathic bladder sphincter dysfunction: a pilot study. J Urol. 2002; 168(6): 2605-7; discussion 2607-8. |
| [25] | Capitanucci ML, Camanni D, Demelas F, Mosiello G, Zaccara A, De Gennaro M. Long-term efficacy of percutaneous tibial nerve stimulation for different types of lower urinary tract dysfunction in children. J Urol. 2009; 182(4 Suppl): 2056-61. |
| [26] | Boudaoud N, Binet A, Line A, Guys JM, Moscovici J, Moscovici L, et al. Management of refractory overactive bladder in children by transcutaneous posterior tibial nerve stimulation: a controlled study. J Pediatr Urol. 2015; 11(3): 138. e 1-10. |
| [27] | Bouali O, Even L, Mouttalib S, Moscovici J, Galinier P, Game X. Tibial nerve transcutaneous stimulation for refractory idiopathic overactive bladder in children and adolescents. Prog Urol. 2015; 25(11): 665-72. |
| [28] | Patidar N, Mittal V, Kumar M, Sureka SK, Arora S, Ansari MS. Transcutaneous posterior tibial nerve stimulation in pediatric overactive bladder: a preliminary report. J Pediatr Urol. 2015; 11(6): 377-82. |
| [29] | Barroso U Jr, Carvalho MT, Veiga ML, Moraes MM, Cunha CC, Lordêlo P. Urodynamic outcome of parasacral transcutaneous electrical neural stimulation for overactive bladder in children. Int Braz J Urol. 2015; 41(4): 739-43. |
| [30] | Humphreys MR, Vandersteen DR, Slezak JM, Hollatz P, Smith CA, Smith JE, et al. Preliminary results of sacral neuromodulation in 23 children. J Urol. 2006; 176(5): 2227-31. |
APA Style
Kyal, N., Beloui, R. E., Boutalja, H., Rsaissi, K., Lmidmani, F., et al. (2025). Effectiveness of Transcutaneous Posterior Tibial Nerve Stimulation for Refractory Idiopathic Overactive Bladder in Children. Rehabilitation Science, 10(1), 16-20. https://doi.org/10.11648/j.rs.20251001.12
ACS Style
Kyal, N.; Beloui, R. E.; Boutalja, H.; Rsaissi, K.; Lmidmani, F., et al. Effectiveness of Transcutaneous Posterior Tibial Nerve Stimulation for Refractory Idiopathic Overactive Bladder in Children. Rehabil. Sci. 2025, 10(1), 16-20. doi: 10.11648/j.rs.20251001.12
@article{10.11648/j.rs.20251001.12,
author = {Nada Kyal and Ryme El Beloui and Hasnaa Boutalja and Khawla Rsaissi and Fatima Lmidmani and Abdellatif El Fatimi},
title = {Effectiveness of Transcutaneous Posterior Tibial Nerve Stimulation for Refractory Idiopathic Overactive Bladder in Children
},
journal = {Rehabilitation Science},
volume = {10},
number = {1},
pages = {16-20},
doi = {10.11648/j.rs.20251001.12},
url = {https://doi.org/10.11648/j.rs.20251001.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.rs.20251001.12},
abstract = {Background: Transcutaneous posterior tibial nerve stimulation (TPTNS) is a promising treatment modality for idiopathic overactive bladder (OAB) in the pediatric population. Objective: To evaluate the efficacy of TPTNS in children suffering from idiopathic OAB refractory to conventional therapies. Method: It is a retrospective study including children with clinical OAB syndrome refractory to treatment. The TPTNS protocol consisted of a daily 20-minute session (5 times per week, frequency 10 Hz, pulse width 200 µsec). All patients and family were instructed on how to use the device at home. Treatment efficacy was assessed based on perceived clinical improvement or success using a 3-day voiding diary and visual analog scale (VAS). The evaluation of treatment effectiveness was done after 1 and 6 months. Result: A total of 55 children were included in the study (31 girls and 24 boys), with a mean age of 10.6 ± 3.1 years. All patients experienced urinary urgency, 78.2% had frequency and 51% urge incontinence. 32.7% exhibited both daytime and nighttime symptoms. After one month of TPTNS, clinical outcomes showed improvement in 52 patients. The perceived improvement was more pronounced for daytime symptoms. After 6 months, 65.5% were considered cured while the remaining patients showed continued improvement. On the VAS, 72.7% assessed the improvement in symptoms as between 9/10 and 10/10. Conclusion: TPTNS represents a potentially effective and noninvasive treatment strategy for idiopathic OAB in children, showing significant symptom improvement without adverse effects. However, further research is needed to determine optimal treatment parameters.},
year = {2025}
}
TY - JOUR T1 - Effectiveness of Transcutaneous Posterior Tibial Nerve Stimulation for Refractory Idiopathic Overactive Bladder in Children AU - Nada Kyal AU - Ryme El Beloui AU - Hasnaa Boutalja AU - Khawla Rsaissi AU - Fatima Lmidmani AU - Abdellatif El Fatimi Y1 - 2025/07/31 PY - 2025 N1 - https://doi.org/10.11648/j.rs.20251001.12 DO - 10.11648/j.rs.20251001.12 T2 - Rehabilitation Science JF - Rehabilitation Science JO - Rehabilitation Science SP - 16 EP - 20 PB - Science Publishing Group SN - 2637-594X UR - https://doi.org/10.11648/j.rs.20251001.12 AB - Background: Transcutaneous posterior tibial nerve stimulation (TPTNS) is a promising treatment modality for idiopathic overactive bladder (OAB) in the pediatric population. Objective: To evaluate the efficacy of TPTNS in children suffering from idiopathic OAB refractory to conventional therapies. Method: It is a retrospective study including children with clinical OAB syndrome refractory to treatment. The TPTNS protocol consisted of a daily 20-minute session (5 times per week, frequency 10 Hz, pulse width 200 µsec). All patients and family were instructed on how to use the device at home. Treatment efficacy was assessed based on perceived clinical improvement or success using a 3-day voiding diary and visual analog scale (VAS). The evaluation of treatment effectiveness was done after 1 and 6 months. Result: A total of 55 children were included in the study (31 girls and 24 boys), with a mean age of 10.6 ± 3.1 years. All patients experienced urinary urgency, 78.2% had frequency and 51% urge incontinence. 32.7% exhibited both daytime and nighttime symptoms. After one month of TPTNS, clinical outcomes showed improvement in 52 patients. The perceived improvement was more pronounced for daytime symptoms. After 6 months, 65.5% were considered cured while the remaining patients showed continued improvement. On the VAS, 72.7% assessed the improvement in symptoms as between 9/10 and 10/10. Conclusion: TPTNS represents a potentially effective and noninvasive treatment strategy for idiopathic OAB in children, showing significant symptom improvement without adverse effects. However, further research is needed to determine optimal treatment parameters. VL - 10 IS - 1 ER -
Department of Physical and Rehabilitation Medicine, University Hospital of Ibn Rochd, Casablanca, Morocco
Department of Physical and Rehabilitation Medicine, University Hospital of Ibn Rochd, Casablanca, Morocco
Department of Physical and Rehabilitation Medicine, University Hospital of Ibn Rochd, Casablanca, Morocco
Department of Physical and Rehabilitation Medicine, University Hospital of Ibn Rochd, Casablanca, Morocco
Department of Physical and Rehabilitation Medicine, University Hospital of Ibn Rochd, Casablanca, Morocco
Department of Physical and Rehabilitation Medicine, University Hospital of Ibn Rochd, Casablanca, Morocco
Information