Abstract
Introduction: Radiation therapy (RT) is a standard component of breast cancer management; however, treatment planning becomes more complex in patients with cardiac implantable electronic devices (CIEDs), including pacemakers (PMs) and implantable cardioverter-defibrillators (ICDs). Exposure of these devices to therapeutic radiation may lead to malfunction, particularly in pacemaker-dependent individuals, where device failure can have serious clinical consequences. Careful treatment planning is therefore essential when irradiating breast cancer patients with implanted cardiac devices. This report presents our institutional experience in the safe administration of adjuvant RT in a pacemaker-dependent patient undergoing treatment for breast cancer. Materials and Methods: A retrospective review was conducted of breast carcinoma patients treated with adjuvant external beam radiation therapy between January 2023 and December 2024, including one pacemaker-dependent patient with a dual-chamber pacemaker implanted in the left anterior chest wall. Simulation imaging was performed using both free-breathing and deep inspiration breath-hold (DIBH) computed tomography (CT) protocols. Target volumes and organs at risk were delineated according to ESTRO/RTOG contouring guidelines, with the pacemaker generator and leads contoured separately as organs at risk. Treatment planning was performed using 6 MV photon beams with field-in-field and hybrid intensity-modulated radiation therapy (IMRT) techniques. Volumetric modulated arc therapy (VMAT) plans were additionally generated for dosimetric comparison. Pacemaker dose constraints were established in accordance with the recommendations of the American Association of Physicists in Medicine Task Group 203 (AAPM TG-203). Prior to treatment initiation, multidisciplinary evaluation was undertaken, including cardiology consultation, device interrogation before and after treatment, and preparation of emergency pacing support protocols. Results: Adjuvant RT was completed successfully without interruption. Target coverage was clinically acceptable, with 96.8% of the planning target volume (PTV) receiving at least 95% of the prescribed dose (PTV V95% = 96.8%). Use of DIBH contributed to cardiac sparing, resulting in a mean heart dose of 1.9 Gy and a mean dose to the left anterior descending artery (LAD) of 4.1 Gy. The maximum recorded dose to the pacemaker was 0.86 Gy, remaining well below established safety thresholds. No pacemaker malfunction, sensing abnormalities, or cardiac complications were observed during treatment. Acute toxicity was limited to grade 1 radiation dermatitis. Conclusion: Adjuvant breast radiotherapy in pacemaker-dependent patients can be delivered safely with appropriate precautions. The use of low-energy photon beams, DIBH techniques, meticulous dosimetric planning, and multidisciplinary coordination enables effective target coverage while maintaining pacemaker dose within acceptable limits, without compromising oncologic outcomes or device functionality.
|
Published in
|
Journal of Cancer Treatment and Research (Volume 14, Issue 2)
|
|
DOI
|
10.11648/j.jctr.20261402.12
|
|
Page(s)
|
66-74 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Pacemaker-dependent Patients, Breast Cancer Radiotherapy, Cardiac Implantable Electronic Devices,
Deep Inspiration Breath-hold, Intensity-modulated Radiation Therapy, Device Dose Constraints,
Multidisciplinary Treatment Planning
1. Introduction
Worldwide, breast cancer is the most commonly diagnosed type of cancer in women, with about 2.3 million new cases diagnosed each year and being one of the leading causes of cancer-related deaths
| [1] | Zaremba T, Jakobsen AR, Søgaard M, Thøgersen AM, Riahi S. Risk of device malfunction in cancer patients with implantable cardioverter-defibrillators receiving radiotherapy: a population-based cohort study. Pacing Clin Electrophysiol. 2016; 39(9): 880–6. https://doi.org/10.1111/pace.12910 |
[1]
. Radiation therapy (RT) is an important part of breast-conserving treatment and has been shown to decrease the chance of recurrence around the treatment area and increase the rate of long-term survival after both lumpectomies and mastectomies
| [2] | American Association of Physicists in Medicine (AAPM). AAPM TG-203 Report: Management of Patients with CIEDs Undergoing Radiotherapy. Med Phys. 2017; 44(9): e391–e429. https://doi.org/10.1002/mp.12345 |
[2]
. There are several clinical challenges involved in providing RT to patients who have implanted cardiac devices (e.g., pacemakers) that include potential problems that may occur due to the use of ionizing radiation such as electromagnetic interference, reset of device computer systems and permanent malfunction of the device due to the radiation’s effect on the device computer systems during delivery. If a patient is dependent upon a pacemaker for pacing, an interruption in pacing for any time period can lead to potentially devastating hemodynamic instability, making treatment planning for these patients especially complex
| [3] | Hurkmans CW, Scheepers E, Springorum BG, Uiterwaal H. Management of radiation oncology patients with a pacemaker or ICD: a new practical guideline. Radiat Oncol. 2012; 7: 198. https://doi.org/10.1186/1748-717X-7-198 |
[3]
. The location of the pacemaker during placement is typically in the subclavicular region, which is located very close to tangential breast fields when treating the breast, thus increasing the risk for unintentional dose delivery to the device.
The AAPM Task Group 203 made recommendations on how to safely manage RT in patients receiving CIEDs. The recommendations include keeping the cumulative radiation dose to the device with the CIED to as low a value as reasonably achievable (<2 Gy) as well as using only photon beam energies greater than 6 Megavolts to avoid neutron production & potentially malfunctioning of the device with more than 2 Gy of radiation from high-energy photons
. The recent development of newer RT delivery techniques (IMRT, VMAT and DIBH) offers greater dosimetric precision in shaping the dose while reducing unintended exposure to the heart/lung and adjacent CIED structures than was previously possible using traditional techniques
| [5] | International Commission on Non-Ionizing Radiation Protection (ICNIRP). Guidelines on exposure limits to ionizing radiation for patients with CIEDs. Health Phys. 2020; 118(5): 459–71. https://doi.org/10.1097/HP.0000000000001316 |
[5]
. In particular, DIBH demonstrated a significantly lower mean dose to the heart and left anterior descending artery (LAD) than free-breathing techniques when used with left-sided breast irradiation
.
These patients were provided with an adjuvant RT to a left-sided breast carcinoma, had a left-sided dual-chamber device and were Pacemaker-Dependent. Multidisciplinary collaboration, individualised dosimetric planning and device-dose verification in real time were all important to the success of RT. Therefore, this case illustrates that proper adherence to current AAPM TG-203 guidelines, along with modern RT techniques, can provide effective oncologic treatment while maintaining both the patient’s and the device’s safety.
2. Materials and Methods
A retrospective observational study was conducted to include five consecutive female patients who were diagnosed with breast carcinoma, confirmed by histopathology, and received adjuvant external beam radiation therapy at Apex Hospital, Varanasi, India, between January 2023 and December 2024. All patients underwent CT simulation using the GE SOMATOM scanner (GE Healthcare, USA). Patients were positioned supinely on a breast board with both arms raised, and axial images were acquired from the mandible to the upper abdomen using 3-5 mm slices acquired during both free breathing (FB) and deep inspiration breath hold (DIBH). In the patient with the CIED, the pacemaker was marked with radiopaque wires at the time of simulation. Before radiotherapy planning, comprehensive documents were obtained documenting all device specifications, including model, pacing dependency, baseline interrogation parameters, and magnet response and mandatory cardiology clearance was obtained prior to radiotherapy planning.
Target delineation was done according to ESTRO and RTOG contouring guidelines. Clinical target volume (CTV) included the whole breast or chest wall and, where applicable, the regional nodal basins. An additional margin of 5-7 mm was used to create the planning target volume (PTV) and a 3 mm trim from the skin surface. Organs at risk (OAR) include: heart, left anterior descending artery (LAD), IPSI and contralateral lung, contralateral breast, spinal cord, and, if applicable to the CIED pulse generator and pacing leads.
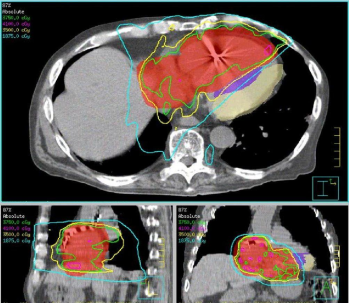
The Monaco Treatment Planning System (Elekta AB, Sweden) was used to create the treatment plan and delivered by a Versa HD linear accelerator (Elekta, England) with 6 MV photon beams according to the AAPM TG-203 guidelines for neutron production and to minimise the dose to the CIED. Treatment planning methodology used the field-in-field technique with forward planning shown in (
Figure 1).
Figure 1. Axial, coronal, and sagittal CT views showing target volume coverage with isodose distribution. Adequate dose conformity to the planning target volume is achieved while limiting dose exposure to adjacent organs at risk, including the pacemaker region.
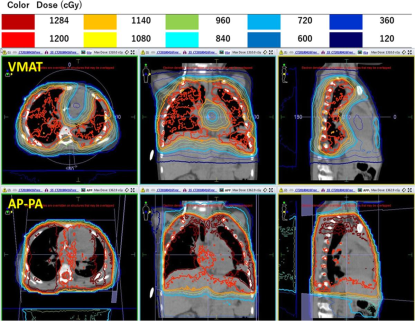
Five pacemaker patients received dosimetric comparisons of hybrid IMRT and VMAT planning and were treated with each of these planning techniques. Pacemaker-specific criteria for treatment included the following: to deliver <2 Gy cumulative dose to the pacemaker, to avoid any direct beams through the pulse generator, and to maximise the distance from the pacemaker to the field edge as much as possible. In addition to PTV metrics (D95%, V95%, and D-mean), an assessment of OARs included metrics specific to heart with mean dose, heart V5 and V10 and mean dose and maximum dose to LAD; metrics specific to ipsilateral lung included V20 and V10; device-specific metrics for the pacemaker case included Dmax, D-mean, distance from the edge of beam; and dose to the pacing leads. All treatment plans were reviewed in a multidisciplinary manner by an experienced radiation oncologist, medical physicist, and experienced radiation technologist. Pre-treatment patient-specific quality assurance for IMRT/VMAT treatment plans was performed on an Octavius II 2D ion-chamber array, requiring a minimum gamma passing rate of ≥95% at 3%/3 mm Shown in
Figure 2,
Figure 3.
Figure 2. Comparison of VMAT and AP–PA plans in a pacemaker-dependent breast cancer patient. VMAT demonstrates superior dose conformity and reduced exposure to the pacemaker and surrounding organs at risk compared to the AP–PA technique.
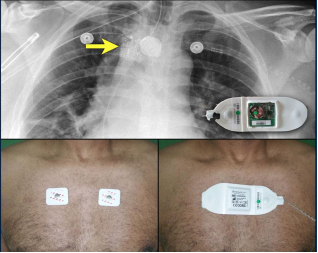
Figure 3. Chest radiograph showing the implanted pacemaker (Yellow arrow) and external dosimetry setup. In vivo dosimeters are positioned over the chest, with a wireless dosimetry device used for real-time dose monitoring during radiotherapy.
Before initiating treatment on the pacemaker-dependent patient, safety readiness included coordinating with the cardiologist prior to treatment to ensure emergency pacing equipment was available, that a magnet would be on standby, and that asynchronous pacing mode would be used bedside as appropriate. The outcome of radiotherapy and pacemaker function (per patient) was assessed at time of treatment completion for each of the five patients.
3. Results
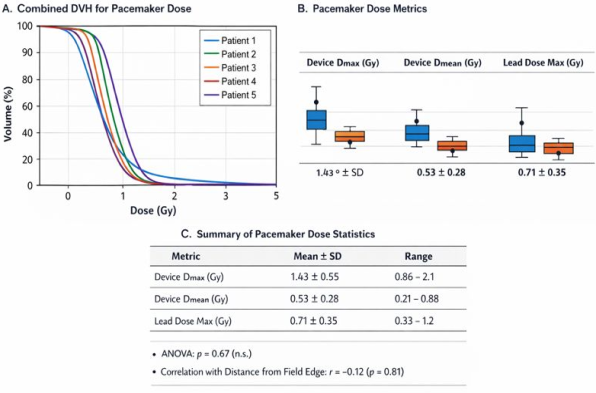
In a Pacemaker-Dependent patient diagnosed with breast cancer, radiation therapy was administered with no interruption to treatment or adverse effects to the patient. The target area (PTV) had excellent treatment coverage (PTV V95% = 96.8%; mean dose 49.6 Gy; prescribed dose of 50.0 Gy). Radiation exposure to the heart during treatment was minimised with the use of deep inspiration breath-hold (DIBH): CT scan (3.2 Gy); mean dose to heart (1.9 Gy); mean dose to left anterior descending artery (4.1 Gy). The maximum dose received by the pacemaker was also low (Dmax = 0.86 Gy) and was less than the recommended maximum dose of 2.0 Gy outlined in the American Association of Physicists in Medicine's (AAPM) Task Group (TG) #203; no device-related malfunctions, sensing abnormalities, resets, or battery/lead issues occurred in this patient. No cardiac complications arose from treatment of this patient, and only mild Grade I skin erythema due to acute toxicity was observed (
Figure 4)
Table 1.
Figure 4. Dose–volume histograms and summarised pacemaker dose metrics across patients. Results demonstrate low device and lead dose exposure within clinically acceptable limits, with no significant variability observed.
Table 1. Baseline Patient Characteristics, Treatment Planning, OAR Metrics, and Pacemaker Dose Parameters.
Parameter | P1 (Breast, Dependent) | P2 (Lung, Dependent) | P3 (Prostate, Non-Dependent) | P4 (Esophagus, Dependent) | P5 (Lymphoma, Partial) |
Age (years) | 68 | 72 | 65 | 75 | 70 |
Diagnosis | Left IDC | RUL NSCLC | Prostate Adenocarcinoma | Mid-esophageal SCC | Classical Hodgkin Lymphoma |
Stage (TNM) | pT2N1M0 | cT3N2M0 | cT2bN0M0 | cT3N1M0 | Stage IIA |
Laterality | Left Breast | Right Lung | Midline | Midline | Mediastinum |
Comorbidities | HTN, CHB | COPD, CAD, CHB | DM, HTN | AF, CHF | HTN |
Pacemaker Type | Dual chamber | Single chamber | Dual chamber | Single chamber | Dual chamber |
Pacing Dependency | 100% | 100% | No | 100% | ~40% |
Device Location | Left pectoral | Right pectoral | Left pectoral | Right pectoral | Left pectoral |
Distance from Field Edge (cm) | 2.1 | 3.4 | 8.2 | 4.0 | 2.8 |
ECOG Status | 1 | 2 | 0 | 2 | 1 |
CT Slice Thickness (mm) | 3 | 2.5 | 3 | 2.5 | 3 |
Immobilization | Breast board | Vac-Lok | Pelvic support | Vac-Lok | Wing board |
Scans Acquired | FB + DIBH | FB + 4D-CT | FB | FB + 4D-CT | FB + DIBH |
Treatment Technique | Field-in-field (DIBH) | VMAT | IMRT | 3D-CRT | VMAT |
Photon Energy | 6 MV | 6 MV | 6 MV | 6 MV | 6 MV |
Prescription Dose | 50 Gy / 25# | 60 Gy / 30# | 78 Gy / 39# | 50.4 Gy / 28# | 30 Gy / 15# |
PTV Coverage (V95%) | 96.8% | 97.2% | 98.1% | 95.6% | 98.4% |
Heart Mean Dose (Gy) | 1.9 | 8.6 | — | 9.8 | 5.4 |
Heart V10 / V20 | 1.2% | 14.3% (V20) | — | — | — |
LAD Mean (Gy) | 4.1 | — | — | — | — |
Lung V20 (%) | 13.6 | 28.7 | — | 22 | 12 |
Spinal Cord Dmax (Gy) | — | — | — | 41 | — |
Rectum V70 (%) | — | — | 14 | — | — |
Device Dmax (Gy) | 0.86 | 1.8 | 0.9 | 2.1 | 1.5 |
Device Dmean (Gy) | 0.32 | 0.74 | 0.21 | 0.88 | 0.52 |
Lead Dose Max (Gy) | 0.45 | 0.92 | 0.33 | 1.2 | 0.63 |
Pre-Treatment QA | Gamma>97% | 96.5% | >98% | 95% | 97% |
Acute Toxicity | G1 erythema | G2 esophagitis | G1 GU | G2 esophagitis | G1 fatigue |
4. Discussion
An individualized and risk-stratified plan should be developed for the patient requiring radiotherapy with an implantable cardiac device, primarily for the purpose of achieving both the goals of the patient’s oncologic care and the safety of the device(s). There are many previous publications and consensus statements describing issues related to patients requiring pacemakers and the fact that they are very sensitive to ionizing radiation, electromagnetic interference and scatter from neutrons. It is known that just a fraction of a Gy with a pacemaker as part of the therapy plan can be sufficient to cause short- or long-term malfunctioning of the device (oversensing, failure to sense or pacing inhibition or inappropriate mode switching or damage to the circuitry), due to direct exposure from radiation, secondary neutrons or other mechanical disruptions. The higher the energy of the beam (>10 MV), the more significant and greater the risk of malfunctioning of the pacemaker, due to secondary neutrons being produced, and therefore it is contraindicated for a patient dependent on a pacemaker.
There are many factors affecting how a pacemaker will affect how the planning of radiotherapy will be planned. The angles of the treatment beams will be somewhat restricted, since they will avoid directly entering through the generator. The restriction will also prohibit the use of higher-energy beams in the treatment plan. This restriction will lead to limitations in the treatment plans for patients being treated for left-sided breast cancer, where the pulse generator is very close to the tangential fields. These types of clinical and technical restrictions to the treatment plans may prolong the time to develop the treatment plans, in addition to requiring much greater detail in the dosimetric evaluation for both the pulse generator and the lead wires. There are also special considerations when treating the patient, including using continuous ECG or pulse monitoring throughout treatment delivery; using frequent verification imaging; and ensuring that the treatment delivery is performed in a reproducible manner to maximise the effectiveness of the respiratory control techniques, such as DIBH.
Table 2.
Table 2. Consolidated Clinical Assessment Outcomes Supporting Safe Radiotherapy Delivery.
Clinical Parameter | P1 | P2 | P3 | P4 | P5 |
Overall Clinical Status | Stable | Stable | Stable | Stable | Stable |
Pacemaker Function | Normal | Normal | Normal | Normal | Normal |
Device Reset/Inhibition | None | None | None | None | None |
In-Vivo Dose Verification | <8% deviation | <10% | <5% | <8% | <7% |
Setup Reproducibility | ≤2 mm | ≤3 mm | ≤2 mm | ≤3 mm | ≤2 mm |
Cardiac Monitoring | Stable ECG | Stable ECG | No events | Stable ECG | No arrhythmia |
Post-Treatment Recovery | Complete | Improved | Complete | Improved | Complete |
Follow-Up Impression | Safe RT | Safe RT | Safe RT | Safe RT | Safe RT |
Advancements in radiotherapy have made it more effective and safer to treat patients with cardiac implantable electronic devices (CIEDs). Patients using the DIBH technique achieve greater separation between their heart, chest wall, and CIED; this technique results in lower radiation doses to the heart and pacemaker. This study found that the mean dose delivered to the heart and left anterior descending artery is much lower when patients are treated using DIBH, and the dose delivered to the CIED potentially falls within acceptable thresholds. The results of this case are consistent with previous studies that concluded that DIBH can improve the protection of the heart from radiation therapy and reduce the risk to the CIED during treatment. Techniques such as IMRT and VMAT help tailor radiation therapy dose distributions away from the CIED while providing adequate tumour coverage. However, the increased low dose to surrounding tissue with these techniques requires careful tracking of the contribution from scattered radiation. Treating a patient with breast cancer who uses a CIED requires balancing two competing demands: adequately treating the cancer and limiting the potential for loss of the pacemaker. The best practice today is to contour the CIED (pacemaker and leads) as separate organs at risk (OARs) and impose very low dose (such as 1–2 Gy) constraints on them. Both aspects were performed in this case. Treating a pacemaker-dependent breast cancer patient on the left side requires balancing the need to control the cancer with the immediate risk to the patient’s life from loss of pacemaking. Current guidelines stress individualised, multidisciplinary planning across radiation oncology, medical physics, and electrophysiology in order to minimise the radiation dose delivered to the CIED, estimate the risk of failure of the CIED, and anticipate how to safely manage a potential system failure and loss of pacing functionality
| [7] | Miften M, Mihailidis D, Kry SF, Reft C, Esquivel C, Farr J, et al. Management of radiotherapy patients with implanted cardiac pacemakers and defibrillators: a report of the AAPM TG-203. Med Phys. 2019; 46(12): e757–88.
https://doi.org/10.1002/mp.13838 |
[7]
.
The stratification of risk will determine the workflow for these cases. The risk for device malfunction is greater for patients with implants when they receive high doses of radiation to their devices. This risk increases with the patient's cumulative dose to their pacemaker/ICD (Implantable Cardioverter Defibrillator), and additionally, with the neutron-producing energy of the therapeutic radiation beam. For example, in patients who are pacing-dependent (relying on a pacemaker for heart function), even transient software glitches or resets can lead to hemodynamic instability, so they will be handled with a higher level of risk and subjected to tighter controls
| [8] | Zaremba T, Jakobsen AR, Søgaard M, Thøgersen AM, Riahi S. Radiotherapy in patients with pacemakers and implantable cardioverter defibrillators: a literature review. Europace. 2016; 18(4): 479–91. https://doi.org/10.1093/europace/euv135 |
[8]
.
To ensure patient safety in these at-risk patients, the following practical and technical dose recommendations should be adhered to when developing a breast treatment plan: (1) Keep the cumulative absorbed dose to the CIED device as low as possible in accordance with the AAPM TG-203 recommendations - the maximum dose (Dmax) should be carefully calculated to limit exposure; 2. Avoid directing beams through the pace maker/ICD and, when feasible, adjust beam arrangements (tangential, partial arc(s) or IMRT segments), if feasible, to avoid exposing high dose areas to the pacemaker/ICD; 3. Limit the use of high-energy (greater than 10 MV) photon beams because of neutron production, as the risk of device failure increases with increased neutron production. If the expected dose of the device will exceed the institution's high-risk dosing threshold (many guidelines indicate significant caution when doses exceed approximately 5 - 10 Gy and consider reassessing device placement/alternative therapy when doses exceed 10 Gy) then, before treatment, discuss with the patient and the cardiology team the potential for generator relocation versus use of modified radiation therapy techniques.
Monitoring pre-treatment and making contingency plans are important. For patients who are pacemaker-dependent, this includes pre-treatment device interrogation (reprogramming if necessary) and continuous A/V monitoring during fractions. Staff members trained in advanced cardiac life support should be available and have quick access to external pacing/defibrillation equipment, and they must have rapid access to a pacemaker technician/electrophysiologist. Post-treatment interrogation should be completed as soon as possible post-treatment and at the time intervals defined by the physician because some radiation effects do not occur until later
| [7] | Miften M, Mihailidis D, Kry SF, Reft C, Esquivel C, Farr J, et al. Management of radiotherapy patients with implanted cardiac pacemakers and defibrillators: a report of the AAPM TG-203. Med Phys. 2019; 46(12): e757–88.
https://doi.org/10.1002/mp.13838 |
[7]
. Precautions must also be taken when planning a stereotactic or hypofractionated regimen (including partial breast or regional nodal boost), since high doses delivered in each fraction and steep gradients can theoretically lead to the accumulation of high doses near a device generator and may increase the risk associated with a single fraction. If dose cannot be avoided, a formal, multidisciplinary risk-benefit discussion should take place, and a specific form of informed consent to document the potential for device malfunction or the change in pacing strategy (temporary external pacing or generator revision) should be signed by the patient
| [8] | Zaremba T, Jakobsen AR, Søgaard M, Thøgersen AM, Riahi S. Radiotherapy in patients with pacemakers and implantable cardioverter defibrillators: a literature review. Europace. 2016; 18(4): 479–91. https://doi.org/10.1093/europace/euv135 |
[8]
. Lastly, all institutions should implement formal, local protocols designed from consensus documents (e.g., AAPM TG-203, JASTRO/JCS) and established multidisciplinary reviews. Regular training, clear delineation of responsibilities and audits of CIED cases will help to reduce variability and improve the safety of patients with a pacemaker who receive radiotherapy for breast cancer
| [7] | Miften M, Mihailidis D, Kry SF, Reft C, Esquivel C, Farr J, et al. Management of radiotherapy patients with implanted cardiac pacemakers and defibrillators: a report of the AAPM TG-203. Med Phys. 2019; 46(12): e757–88.
https://doi.org/10.1002/mp.13838 |
[7]
.
Delivering radiotherapy to patients with cardiac implantable electronic devices (CIEDs) is a significant clinical problem given that patients who rely on pacemaker support are at risk of malfunctioning or complete failure of their pacemakers due to radiation exposure
. In the past, it was recommended that practitioners limit irradiation to the pacemaker device to decrease the potential risk of malfunctioning as well as to limit the dose delivered during the radiation treatment planning for individual patients
. Subsequent studies have shown that cumulative doses above the manufacturer-approved maximum cumulative dose can contribute to malfunction due to the malfunction frequency increasing when neutron-producing high-energy photon beams are used and the cumulative dose increases
| [11] | Elders J, Kunze-Busch M, Jan S, et al. High incidence of cardiac device malfunctions caused by radiation therapy in patients with pacemakers and implantable cardioverter-defibrillators. Heart Rhythm. 2013; 10(5): 699-705.
https://doi.org/10.1016/j.hrthm.2013.01.037 |
| [13] | Grant JD, Jensen GL, Tang C, et al. Radiotherapy-induced malfunction in contemporary cardiovascular implantable electronic devices: clinical incidence and predictors. JAMA Oncol. 2015; 1(5): 624-632.
https://doi.org/10.1001/jamaoncol.2015.1787 |
[11, 13]
. In light of these findings, current guidelines for delivering radiotherapy to pacemaker patients should include using low-energy photon beams and performing a risk assessment for each patient in addition to using a multidisciplinary approach in managing the patient and providing continuous monitoring of the pacemaker throughout radiotherapy
| [9] | Gauter-Fleckenstein B, Israel CW, Dorenkamp M, et al. DEGRO/DGK guideline for radiotherapy in patients with cardiac implantable electronic devices. Strahlenther Onkol. 2015; 191(5): 393-404. https://doi.org/10.1007/s00066-015-0807-0 |
| [12] | Uiterwaal H, Hurkmans CW, Knegjens JL, et al. Radiotherapy in patients with a pacemaker or ICD: practical recommendations of the Dutch Society of Radiotherapy and Oncology. Radiat Oncol. 2012; 7: 198. |
[9, 12]
.
This study delivered effective radiotherapy via 6 MV photon beams using deep inspiration breath-hold techniques, with excellent target dose coverage achieved while limiting the dose to the pacemaker within acceptable limits (Dmax 0.86 Gy). The breath hold technique provided considerable cardiac sparing and increased separation between the heart, chest wall, and pacemaker generator, which have been described by other authors in the current clinical setting and have demonstrated that utilizing advanced radiotherapy techniques can be utilized to achieve significant reductions in dose to the heart and pacemaker device without adversely affecting oncological outcomes
| [15] | Hudson FZ, Coulshed DS, D’Souza DP, et al. Radiation therapy in patients with cardiac implantable electronic devices: contemporary practice and clinical outcomes. Clin Oncol (R Coll Radiol). 2021; 33(2): e74-e82.
https://doi.org/10.1016/j.clon.2020.09.011 |
[15]
.
These findings are supporting developing evidence that appropriate dosimetric planning by the radiation oncology staff, strict adherence to published dose constraints by both the radiation oncology staff and the treating physician(s), and a coordinated multidisciplinary approach to the management of pacemaker patients allows for the safe delivery of breast radiotherapy to patients dependent on pacemaker support
| [9] | Gauter-Fleckenstein B, Israel CW, Dorenkamp M, et al. DEGRO/DGK guideline for radiotherapy in patients with cardiac implantable electronic devices. Strahlenther Onkol. 2015; 191(5): 393-404. https://doi.org/10.1007/s00066-015-0807-0 |
| [12] | Uiterwaal H, Hurkmans CW, Knegjens JL, et al. Radiotherapy in patients with a pacemaker or ICD: practical recommendations of the Dutch Society of Radiotherapy and Oncology. Radiat Oncol. 2012; 7: 198. |
| [15] | Hudson FZ, Coulshed DS, D’Souza DP, et al. Radiation therapy in patients with cardiac implantable electronic devices: contemporary practice and clinical outcomes. Clin Oncol (R Coll Radiol). 2021; 33(2): e74-e82.
https://doi.org/10.1016/j.clon.2020.09.011 |
[9, 12, 15]
.
A well-designed multi-team approach to the safe application of breast radiation therapy to pacemaker-dependent patients is achievable through careful planning, application of low energy (≤ 6 MV), strict dose limits, on-going treatment monitoring and multi-disciplinary collaboration; thus allowing for the continued efficacy of the patient’s breast radiation therapy as well as the durability of his or her pacemaker device. The author also believes that the integration of technological advances with multi-faceted safety protocols could optimise outcomes for patients who will receive breast radiation therapy and have an implanted cardiac implantable electronic device (CIED). Breath-handled (DIBH) radiation delivery methods can be used to minimise breath-hold variability. The patient’s pacemaker was interrogated before, during, and after radiation therapy to detect oversensing, undersensing, reset, and parameter drift; all findings were recorded ○n a shared database for review with the patient’s cardiology team. During the retrospective dose measurement comparisons, the authors were able to create a complete dosimetric record and implement safe breast radiation therapy in a pacemaker-dependent patient and provide comparative data from nine breast patients treated with standard therapy, the authors were able to implement similar protocols and evaluate multiple consensus statements that emphasise that pre-treatment interrogation of the patient device, continuous monitoring during radiotherapy, and periodic post-treatment evaluation are integral aspects of patient safety and typically cited in literature. The authors also recommend obtaining long-term surveillance data to assess for any delayed adverse effects on CIED device integrity and cardiac function. The patient continues to be monitored in cooperation with the patient’s cardiologist, with no reports of adverse events during follow-up.
5. Conclusions
These case studies provide examples of how with careful planning, monitoring, and the involvement of multiple specialities, radiation therapy can be delivered safely to breast cancer patients who require a pacemaker. Radiation exposure to residents implanted with pacemakers and to critical organs was minimised by the implementation of Intensity Modulated Radiation Therapy (IMRT) and the use of Deep Inspiration Breath Hold (DIBH) techniques, while at the same time allowing for optimal management of the patient's tumour. Standardised and individualised approaches to the planning and execution of radiation therapy procedures are imperative to overcome the challenges of delivering cancer care to patients who have CIED devices. Additionally, through the use of appropriate planning (utilizing 6 MV photon beams), DIBH, strict adherence to dose limits, as well as by employing the participation of a multi-disciplinary team in the delivery process, continued monitoring, and monitoring of device integrity throughout the radiation therapy process, the possibility exists to provide radiotherapy treatment that is delivered safely to breast cancer patients who have pacemaker devices while not compromising the quality of the tumor or the device.
Ethics statement
This study was conducted in accordance with ethical guidelines and all applicable local and international ethical guidelines for conducting research involving human subjects. This study used previously consented and de-identified imaging and treatment records of patients who, in turn, provided written consent for their anonymised imaging and treatment records to be used for research by the investigators and published in journals. No additional procedures were performed to patients in this study other than those routinely performed in the delivery of health care to those patients who were part of the study. All patient-related privacy and confidentiality were maintained at all times.
Limitations of the Study: The findings of the study are limited by the fact that there was a very small sample size, with only one Pacemaker-Dependent patient. This limits the amount of generalizability of the findings. The study was conducted at a single institution, the results may not be applicable to other institutions with different technology, infrastructure, or clinical workflows. The follow-up period for this study was limited, which did not allow for an adequate assessment of the long-term performance of pacemakers or late radiation-induced complications on the devices. Evaluation of VMAT has only been done at the dosimetric planning level and was not actual clinical delivery; this limits the conclusion that can be made regarding the real-world safety of VMAT. The study involved a single pacemaker manufacturer and therefore cannot be generalized to any other cardiac implantable electronic devices (CIEDs) such as ICDs. No in-vivo dosimetry was performed over the pacemaker; only treatment planning system calculations were made when estimating the radiation dose.
Abbreviations
AAPM | American Association of Physicists in Medicine |
CIED | Cardiac Implantable Electronic Device |
CT | Computed Tomography |
CTV | Clinical Target Volume |
DIBH | Deep Inspiration Breath Hold |
ECG | Electrocardiogram |
FB | Free Breathing |
ICD | Implantable Cardioverter Defibrillator |
IMRT | Intensity-Modulated Radiation Therapy |
LAD | Left Anterior Descending (Coronary Artery) |
MV | Megavoltage |
OAR | Organ at Risk |
PTV | Planning Target Volume |
QA | Quality Assurance |
RT | Radiotherapy |
TG-203 | Task Group 203 (AAPM Guideline) |
TPS | Treatment Planning System |
VMAT | Volumetric Modulated Arc Therapy |
Acknowledgments
The authors extend their sincere gratitude to the Department of Radiation Oncology and the Radiation Therapy team at our institution for their invaluable technical support and collaboration throughout the course of this study. We deeply appreciate the cooperation of all participating patients and the dedicated efforts of the Radiation Therapists who ensured the accuracy and consistency of data collection during treatment delivery. The authors also thank the medical physicists and oncologists whose expertise in data interpretation significantly enhanced the quality and integrity of this research.
Author Contributions
Rajiv Kumar Singh: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration
Subrata Roy: Formal Analysis, Investigation, Methodology, Software, Supervision, Writing – original draft
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
| [1] |
Zaremba T, Jakobsen AR, Søgaard M, Thøgersen AM, Riahi S. Risk of device malfunction in cancer patients with implantable cardioverter-defibrillators receiving radiotherapy: a population-based cohort study. Pacing Clin Electrophysiol. 2016; 39(9): 880–6.
https://doi.org/10.1111/pace.12910
|
| [2] |
American Association of Physicists in Medicine (AAPM). AAPM TG-203 Report: Management of Patients with CIEDs Undergoing Radiotherapy. Med Phys. 2017; 44(9): e391–e429.
https://doi.org/10.1002/mp.12345
|
| [3] |
Hurkmans CW, Scheepers E, Springorum BG, Uiterwaal H. Management of radiation oncology patients with a pacemaker or ICD: a new practical guideline. Radiat Oncol. 2012; 7: 198.
https://doi.org/10.1186/1748-717X-7-198
|
| [4] |
Solan AN, Solan MJ, Bednarz G, Goodkin MB. Treatment of patients with cardiac pacemakers and ICDs during radiotherapy. Int J Radiat Oncol Biol Phys. 2004; 59(3): 897–904.
https://doi.org/10.1016/j.ijrobp.2004.02.005
|
| [5] |
International Commission on Non-Ionizing Radiation Protection (ICNIRP). Guidelines on exposure limits to ionizing radiation for patients with CIEDs. Health Phys. 2020; 118(5): 459–71.
https://doi.org/10.1097/HP.0000000000001316
|
| [6] |
Heart Rhythm Society (HRS). HRS Expert Consensus Statement on MRI and radiation exposure in patients with CIEDs. Heart Rhythm. 2017; 14(7): e97–e153.
https://doi.org/10.1016/j.hrthm.2017.04.025
|
| [7] |
Miften M, Mihailidis D, Kry SF, Reft C, Esquivel C, Farr J, et al. Management of radiotherapy patients with implanted cardiac pacemakers and defibrillators: a report of the AAPM TG-203. Med Phys. 2019; 46(12): e757–88.
https://doi.org/10.1002/mp.13838
|
| [8] |
Zaremba T, Jakobsen AR, Søgaard M, Thøgersen AM, Riahi S. Radiotherapy in patients with pacemakers and implantable cardioverter defibrillators: a literature review. Europace. 2016; 18(4): 479–91.
https://doi.org/10.1093/europace/euv135
|
| [9] |
Gauter-Fleckenstein B, Israel CW, Dorenkamp M, et al. DEGRO/DGK guideline for radiotherapy in patients with cardiac implantable electronic devices. Strahlenther Onkol. 2015; 191(5): 393-404.
https://doi.org/10.1007/s00066-015-0807-0
|
| [10] |
Last A. Radiotherapy in patients with cardiac pacemakers. Br J Radiol. 1998; 71(841): 4-10.
https://doi.org/10.1259/bjr.71.841.9536892
|
| [11] |
Elders J, Kunze-Busch M, Jan S, et al. High incidence of cardiac device malfunctions caused by radiation therapy in patients with pacemakers and implantable cardioverter-defibrillators. Heart Rhythm. 2013; 10(5): 699-705.
https://doi.org/10.1016/j.hrthm.2013.01.037
|
| [12] |
Uiterwaal H, Hurkmans CW, Knegjens JL, et al. Radiotherapy in patients with a pacemaker or ICD: practical recommendations of the Dutch Society of Radiotherapy and Oncology. Radiat Oncol. 2012; 7: 198.
|
| [13] |
Grant JD, Jensen GL, Tang C, et al. Radiotherapy-induced malfunction in contemporary cardiovascular implantable electronic devices: clinical incidence and predictors. JAMA Oncol. 2015; 1(5): 624-632.
https://doi.org/10.1001/jamaoncol.2015.1787
|
| [14] |
Marbach JR, Sontag MR, Van Dyk J, Wolbarst AB. Management of radiation oncology patients with implanted cardiac pacemakers: report of AAPM Task Group No. 34. Med Phys. 1994; 21(1): 85-90.
https://doi.org/10.1118/1.597316
|
| [15] |
Hudson FZ, Coulshed DS, D’Souza DP, et al. Radiation therapy in patients with cardiac implantable electronic devices: contemporary practice and clinical outcomes. Clin Oncol (R Coll Radiol). 2021; 33(2): e74-e82.
https://doi.org/10.1016/j.clon.2020.09.011
|
Cite This Article
-
APA Style
Singh, R. K., Roy, S. (2026). Safe Radiotherapy Delivery in a Pacemaker-dependent Breast Cancer Patient: Insights from an Initial Institutional Experience. Journal of Cancer Treatment and Research, 14(2), 66-74. https://doi.org/10.11648/j.jctr.20261402.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Singh, R. K.; Roy, S. Safe Radiotherapy Delivery in a Pacemaker-dependent Breast Cancer Patient: Insights from an Initial Institutional Experience. J. Cancer Treat. Res. 2026, 14(2), 66-74. doi: 10.11648/j.jctr.20261402.12
Copy
|
Download
AMA Style
Singh RK, Roy S. Safe Radiotherapy Delivery in a Pacemaker-dependent Breast Cancer Patient: Insights from an Initial Institutional Experience. J Cancer Treat Res. 2026;14(2):66-74. doi: 10.11648/j.jctr.20261402.12
Copy
|
Download
-
@article{10.11648/j.jctr.20261402.12,
author = {Rajiv Kumar Singh and Subrata Roy},
title = {Safe Radiotherapy Delivery in a Pacemaker-dependent Breast Cancer Patient: Insights from an Initial Institutional Experience},
journal = {Journal of Cancer Treatment and Research},
volume = {14},
number = {2},
pages = {66-74},
doi = {10.11648/j.jctr.20261402.12},
url = {https://doi.org/10.11648/j.jctr.20261402.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.jctr.20261402.12},
abstract = {Introduction: Radiation therapy (RT) is a standard component of breast cancer management; however, treatment planning becomes more complex in patients with cardiac implantable electronic devices (CIEDs), including pacemakers (PMs) and implantable cardioverter-defibrillators (ICDs). Exposure of these devices to therapeutic radiation may lead to malfunction, particularly in pacemaker-dependent individuals, where device failure can have serious clinical consequences. Careful treatment planning is therefore essential when irradiating breast cancer patients with implanted cardiac devices. This report presents our institutional experience in the safe administration of adjuvant RT in a pacemaker-dependent patient undergoing treatment for breast cancer. Materials and Methods: A retrospective review was conducted of breast carcinoma patients treated with adjuvant external beam radiation therapy between January 2023 and December 2024, including one pacemaker-dependent patient with a dual-chamber pacemaker implanted in the left anterior chest wall. Simulation imaging was performed using both free-breathing and deep inspiration breath-hold (DIBH) computed tomography (CT) protocols. Target volumes and organs at risk were delineated according to ESTRO/RTOG contouring guidelines, with the pacemaker generator and leads contoured separately as organs at risk. Treatment planning was performed using 6 MV photon beams with field-in-field and hybrid intensity-modulated radiation therapy (IMRT) techniques. Volumetric modulated arc therapy (VMAT) plans were additionally generated for dosimetric comparison. Pacemaker dose constraints were established in accordance with the recommendations of the American Association of Physicists in Medicine Task Group 203 (AAPM TG-203). Prior to treatment initiation, multidisciplinary evaluation was undertaken, including cardiology consultation, device interrogation before and after treatment, and preparation of emergency pacing support protocols. Results: Adjuvant RT was completed successfully without interruption. Target coverage was clinically acceptable, with 96.8% of the planning target volume (PTV) receiving at least 95% of the prescribed dose (PTV V95% = 96.8%). Use of DIBH contributed to cardiac sparing, resulting in a mean heart dose of 1.9 Gy and a mean dose to the left anterior descending artery (LAD) of 4.1 Gy. The maximum recorded dose to the pacemaker was 0.86 Gy, remaining well below established safety thresholds. No pacemaker malfunction, sensing abnormalities, or cardiac complications were observed during treatment. Acute toxicity was limited to grade 1 radiation dermatitis. Conclusion: Adjuvant breast radiotherapy in pacemaker-dependent patients can be delivered safely with appropriate precautions. The use of low-energy photon beams, DIBH techniques, meticulous dosimetric planning, and multidisciplinary coordination enables effective target coverage while maintaining pacemaker dose within acceptable limits, without compromising oncologic outcomes or device functionality.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Safe Radiotherapy Delivery in a Pacemaker-dependent Breast Cancer Patient: Insights from an Initial Institutional Experience
AU - Rajiv Kumar Singh
AU - Subrata Roy
Y1 - 2026/05/27
PY - 2026
N1 - https://doi.org/10.11648/j.jctr.20261402.12
DO - 10.11648/j.jctr.20261402.12
T2 - Journal of Cancer Treatment and Research
JF - Journal of Cancer Treatment and Research
JO - Journal of Cancer Treatment and Research
SP - 66
EP - 74
PB - Science Publishing Group
SN - 2376-7790
UR - https://doi.org/10.11648/j.jctr.20261402.12
AB - Introduction: Radiation therapy (RT) is a standard component of breast cancer management; however, treatment planning becomes more complex in patients with cardiac implantable electronic devices (CIEDs), including pacemakers (PMs) and implantable cardioverter-defibrillators (ICDs). Exposure of these devices to therapeutic radiation may lead to malfunction, particularly in pacemaker-dependent individuals, where device failure can have serious clinical consequences. Careful treatment planning is therefore essential when irradiating breast cancer patients with implanted cardiac devices. This report presents our institutional experience in the safe administration of adjuvant RT in a pacemaker-dependent patient undergoing treatment for breast cancer. Materials and Methods: A retrospective review was conducted of breast carcinoma patients treated with adjuvant external beam radiation therapy between January 2023 and December 2024, including one pacemaker-dependent patient with a dual-chamber pacemaker implanted in the left anterior chest wall. Simulation imaging was performed using both free-breathing and deep inspiration breath-hold (DIBH) computed tomography (CT) protocols. Target volumes and organs at risk were delineated according to ESTRO/RTOG contouring guidelines, with the pacemaker generator and leads contoured separately as organs at risk. Treatment planning was performed using 6 MV photon beams with field-in-field and hybrid intensity-modulated radiation therapy (IMRT) techniques. Volumetric modulated arc therapy (VMAT) plans were additionally generated for dosimetric comparison. Pacemaker dose constraints were established in accordance with the recommendations of the American Association of Physicists in Medicine Task Group 203 (AAPM TG-203). Prior to treatment initiation, multidisciplinary evaluation was undertaken, including cardiology consultation, device interrogation before and after treatment, and preparation of emergency pacing support protocols. Results: Adjuvant RT was completed successfully without interruption. Target coverage was clinically acceptable, with 96.8% of the planning target volume (PTV) receiving at least 95% of the prescribed dose (PTV V95% = 96.8%). Use of DIBH contributed to cardiac sparing, resulting in a mean heart dose of 1.9 Gy and a mean dose to the left anterior descending artery (LAD) of 4.1 Gy. The maximum recorded dose to the pacemaker was 0.86 Gy, remaining well below established safety thresholds. No pacemaker malfunction, sensing abnormalities, or cardiac complications were observed during treatment. Acute toxicity was limited to grade 1 radiation dermatitis. Conclusion: Adjuvant breast radiotherapy in pacemaker-dependent patients can be delivered safely with appropriate precautions. The use of low-energy photon beams, DIBH techniques, meticulous dosimetric planning, and multidisciplinary coordination enables effective target coverage while maintaining pacemaker dose within acceptable limits, without compromising oncologic outcomes or device functionality.
VL - 14
IS - 2
ER -
Copy
|
Download