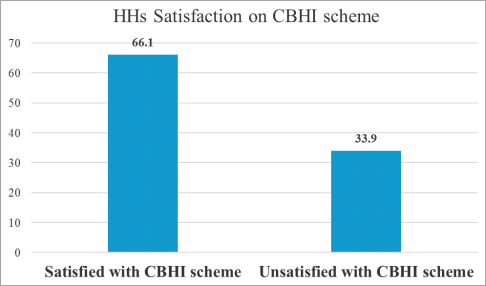
Understanding the level of satisfaction and factors associated with it is essential to ensure the sustainability of the community- based health insurance (CBHI) program. Therefore, this study aimed to assess household satisfaction with a community-based health insurance scheme and its associated factors in the Adama district. A community-based cross-sectional study was conducted in households of Adama district from February 15-30, 2023. The Systematic random sampling technique under multi-stage sampling was used to select study participants. A face-to-face interview with a total of 620 households was conducted by using a pre-tested structured questionnaire. Descriptive analysis, bivariable, and multivariable logistic regression analysis were conducted. Variables with p-value < 0.05 were considered statistically significant to determine independent predictors of household satisfaction with the CBHI scheme. The level of household satisfaction with the CBHI scheme was found to be 61.1%. Satisfaction was found significantly associated with male household heads (AOR=0.545; 95% C.I 0.358-0.831), households with the educational level of able to read and write, grade 1-4 and grade 5-8,(AOR=0.281; 95% C.I 0.131-0.603; AOR=0.533; 95% C.I 0.311-0.915 and, AOR=0.409; 95% C.I 0.191-0.877) respectively, followers of waqefeta religion (AOR=2.123; 95% C.I 0.858-5.262), occupation of government employment (AOR=3.493; 95% C.I 1.949-6.262), those who strongly agreed with immediate care (AOR=0.508; 95% C.I 0.270-0.957), those who strongly agree and disagree with CBHI scheme office opining time (AOR=0.157; 95% C.I 0.044-0.556; AOR=-0.049; 95% C.I 0.006-0.384) and those who disagree with payment of premium schedule (AOR=150.66; 95% C.I 6.171-3678.207). This study showed that the overall satisfaction of households in the Adama district with the CBHI scheme was very good. Male households, waqefeta region followers, occupation of government employees, educational level, immediate care, BBHI office opening time, and premium schedule paying were significant factors of satisfaction with CBHI. Consideration should be given to increasing the accessibility of immediate health care, improving the educational level of households, and improving enrollee’s knowledge of CBHI benefit packages.
| Published in | International Journal of Science, Technology and Society (Volume 12, Issue 6) |
| DOI | 10.11648/j.ijsts.20241206.13 |
| Page(s) | 178-195 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Community Based Health Scheme (CBHI), Household Satisfaction, Factors, Adama
Variables | Frequency | Percentage | Mean |
|---|---|---|---|
Age | 48.15 | ||
Gender | |||
Male | 364 | 58.7 | |
Female | 256 | 41.3 | |
Marital status | |||
Married | 308 | 49.7 | |
Single | 207 | 33.4 | |
Divorced | 46 | 7.4 | |
Widowed | 59 | 9.5 | |
Household size | |||
>3 | 290 | 46.8 | |
4-7 | 268 | 43.2 | |
<8 | 62 | 10 | |
Education level | |||
Not able to write and read | 336 | 54.2 | |
Able to read and write | 69 | 11.1 | |
Grade 1-4 | 116 | 18.7 | |
Grade 5-8 | 76 | 12.3 | |
Secondary school | 21 | 3.4 | |
Diploma and above | 2 | 3 | |
Religion | |||
Orthodox | 409 | 66 | |
Muslim | 88 | 14.2 | |
Protestant | 82 | 13.2 | |
Wakefeta | 41 | 6.6 | |
HH occupation | |||
Farming | 483 | 77.9 | |
Merchant | 15 | 2.4 | |
Government Employee | 75 | 12.1 | |
Daily laborer | 47 | 7.6 | |
Residence of Households | |||
Rural | 519 | 83.7 | |
Urban | 88 | 14.2 | |
Both | 13 | 2.1 |
Variables | HHs satisfaction with CBHI scheme (N=410 | HHs unsatisfied with CBHI scheme (N=210) | Sig. (2-tailed) | ||
|---|---|---|---|---|---|
Mean | Std | Mean | Std | ||
Age | 47.69 | 12.220 | 49.06 | 12.250 | 0.045* |
Variables | Frequency | Percentage |
|---|---|---|
Health institution visited | ||
Health center | 214 | 34.5 |
Hospital | 203 | 32.7 |
Both | 203 | 32.7 |
Got requested laboratory services | ||
Yes | 536 | 86.5 |
No | 84 | 13.5 |
CBHI benefited households | ||
Yes | 586 | 94.5 |
No | 34 | 5.5 |
Discussion with CBHI managers | ||
Yes | 480 | 77.4 |
No | 140 | 22.6 |
Got prescribed drugs | ||
Yes | 479 | 77.4 |
No | 141 | 22.7 |
Satisfied with visited healthcare institution | ||
Yes | 450 | 72.6 |
No | 170 | 27.7 |
Times premium paid | ||
Once | 41 | 6.6 |
Twice | 69 | 11.1 |
3 times | 138 | 22.3 |
Greater than 3 times | 372 | 60 |
Times healthcare visited | ||
Once | 76 | 12.3 |
Twice | 366 | 59 |
3 times | 178 | 28.7 |
Schedule of payment | ||
Monthly | 330 | 53.2 |
Quarterly | 114 | 18.4 |
Twice per year | 134 | 21.6 |
Once a year | 42 | 6.8 |
Participation of CBHI-related meeting | ||
Yes | 4 | 0.6 |
No | 616 | 99.4 |
Variables | Frequency | Percentages |
|---|---|---|
CBHI is good way of helping clients to relieve health expenditure | ||
Yes | 525 | 84.7 |
No | 95 | 15.3 |
CBHI covers only care from public health institutions | ||
Yes | 517 | 83.4 |
No | 103 | 16.6 |
CBHI does not cover transportation fee | ||
Yes | 535 | 86.3 |
No | 85 | 13.7 |
CBHI covers inpatient care | ||
Yes | 435 | 70.2 |
No | 185 | 29.8 |
CBHI covers outpatient care | ||
Yes | 103 | 16.6 |
No | 517 | 83.4 |
CBHI does not cover medical care for cosmetic value | ||
Yes | 581 | 93.7 |
No | 39 | 6.3 |
Answered more than the four of CBHI benefit packages | ||
Yes | 346 | 55.8 |
No | 274 | 44.2 |
Categorical variables | Category | satisfaction with CBHI scheme (N=410) | unsatisfied with CBHI scheme (N=210) | Chi-Square (χ2) |
|---|---|---|---|---|
Gender | Male | 226 | 138 | 0.011** |
Female | 184 | 72 | ||
Participation in CBHI related meeting | Yes | 4 | 0 | 0.0151** |
No | 406 | 210 | ||
Helps clients to health expenditure | Yes | 353 | 172 | 0.170 |
No | 57 | 38 | ||
Only care from public institution | Yes | 349 | 168 | 0.105 |
No | 61 | 42 | ||
Does not cover transportation fee | Yes | 354 | 181 | 0.000*** |
No | 56 | 29 | ||
CBHI covers inpatient care | Yes | 286 | 149 | 0.046** |
No | 124 | 61 | ||
CBHI covers outpatient care | Yes | 63 | 40 | 0.244 |
No | 347 | 170 | ||
Members got the prescribed drug | Yes | 317 | 162 | 0.0200** |
No | 93 | 48 | ||
Got the requested laboratory services | Yes | 351 | 185 | 0.730 |
No | 59 | 25 | ||
Sat. with visited health institution | Yes | 292 | 158 | 0.280 |
No | 118 | 52 | ||
Discussion with CBHI managers | Yes | 317 | 163 | 0.000*** |
No | 93 | 47 | ||
CBHI benefited HHs | Yes | 389 | 197 | 0.048** |
No | 21 | 13 | ||
Answered >4 of benefit packages | Yes | 235 | 111 | 0.290 |
No | 410 | 99 | ||
Not cover medical care for cosmetics | Yes | 388 | 193 | 0.185 |
No | 22 | 17 |
Statements | Five point Likert scales (1-5) | ||||||
|---|---|---|---|---|---|---|---|
1 | 2 | 3 | 4 | 5 | Mean | SD | |
Satisfaction with the opining hours of CBHI offices | 13 (2.1%) | 23 (3.7%) | 22 (3.5%) | 261 (42.1%) | 301 (48.5%) | 4.31 | 0.87 |
satisfied with the time to make use of the CBHI after payment of registration fee | 14 (2.3%) | 8 (1.3%) | 10 (1.6%) | 253 (40.8%) | 335 (54%) | 4.44 | 0.75 |
satisfied with the collection process of insurance cards | 2 (.5%) | 12 (1.9%) | 46 (7.4%) | 205 (33.1%) | 354 (57.1%) | 4.43 | 0.79 |
satisfied with the schedule for paying the premium | 8 (1.5%) | 13 (2.1%) | 29 (4.7%) | 212 (34.2%) | 358 (57.7%) | 4.45 | 0.78 |
Note: 1= Strongly Disagree 2= Disagree 3= Neutral 4=Agree 5=strongly Agree (in terms of level of satisfaction), out off and in the bracket shows frequency and percentage respectively. | |||||||
variables | Frequency | Percentages |
|---|---|---|
Satisfied with laboratory services | ||
Strongly disagree | 41 | 6.6 |
Disagree | 93 | 15 |
Neutral | 29 | 4.7 |
Agree | 177 | 28.5 |
Strongly agree | 280 | 45.2 |
Service providers friendly | ||
Strongly disagree | 80 | 12.9 |
Disagree | 51 | 8.2 |
Neutral | 20 | 3.2 |
Agree | 205 | 33.1 |
Strongly agree | 264 | 42.6 |
Can get immediate care when visiting health facility | ||
Strongly disagree | 52 | 8.4 |
Disagree | 94 | 15.2 |
Neutral | 31 | 5 |
Agree | 242 | 39 |
Strongly agree | 201 | 32.4 |
Respect from services providers | ||
Strongly disagree | 69 | 11.1 |
Disagree | 102 | 16.5 |
Neutral | 18 | 2.9 |
Agree | 206 | 33.2 |
Strongly agree | 225 | 36.3 |
Variables | Five point Likert scales (1-5) | ||||||
|---|---|---|---|---|---|---|---|
1 | 2 | 3 | 4 | 5 | Mean | SD | |
Satisfaction laboratory services | 41 (6.6%) | 93 (15%) | 29 (4.7%) | 177 (28.5%) | 280 (45.2) | 3.91 | 1.299 |
Services providers friendly | 80 (12.9%) | 51 (8.2%) | 20 (3.2%) | 205 (33.1%) | 264 (42.6%) | 3.84 | 1.388 |
Can get immediate care | 52 (8.4%) | 94 (15.2%) | 31 (5%) | 242 (39%) | 201 (32.4%) | 3.72 | 1.288 |
Respect from services providers | 69 (11.1%) | 102 (16.5%) | 18 (2.9%) | 206 (33.2) | 225 (36.3) | 3.67 | 1.395 |
Note: 1= Strongly Disagree 2= Disagree 3= Neutral 4=Agree 5=strongly Agree (in terms of level of satisfaction), out off and in the bracket shows frequency and percentage respectively. | |||||||
Statements | Five point Likert scales (1-5) | Mean | SD | ||||
|---|---|---|---|---|---|---|---|
1 | 2 | 3 | 4 | 5 | |||
Local CBHI management is trustworthy | 16 (2.6%) | 12 (1.9%) | 43 (6.9%) | 250 (40.3%) | 299 (48.2%) | 4.3 | 0.88 |
satisfied with benefit packages of the CBHI scheme | 13 (2.9%) | 20 (3.2%) | 58 (9.4%) | 225 (36.3%) | 304 (49%) | 4.27 | 0.911 |
satisfied with the information provided with CBHI scheme | 18 (2.9%) | 25 (4%) | 77 (12.4%) | 228 (36.8%) | 272 (43.9%) | 4.15 | 0.983 |
Do not want to stay enrolled in the CBHI scheme | 20 (3.2%) | 31 (5%) | 17 (2.7%) | 234 (37.7%) | 318 (51.3%) | 4.29 | 0.974 |
Being enrolled in the scheme did not benefit the household | 10 (1.6%) | 18 (2.9%) | 93 (15%) | 210 (33.9) | 289 (46.6) | 4.21 | 0.914 |
Recommending CBHI scheme scale up to other settings/woredas | 3 (.5%) | 12 (1.9%) | 47 (7.6%) | 320 (51.6%) | 238 (38.6%) | 4.25 | 0.719 |
Note: 1= Strongly Disagree 2= Disagree 3= Neutral 4=Agree 5=strongly Agree (in terms of level of satisfaction), out off and in the bracket shows frequency and percentage respectively. | |||||||
variables | No (%) | P-value | Unst (B) | Stan (B) | COR with 95% CIs for B | AOR with 95% CIs for B |
|---|---|---|---|---|---|---|
Gender | ||||||
Male | 364 (58.7) | 005 | 641 | 545 | 454 to 905 | .358 to .831** |
Female | 256 (41.3) | R | R | |||
Edu level | ||||||
Not write & read | 336 (54.2) | 004 | R | R | ||
Able to read & write | 69 (11.1) | 001 | 310 | 281 | 160 to 599 | .131 to .603** |
Grade 1-4 | 116 (18.7) | 023 | 662 | 533 | 422 to 1.037 | .311 to .915** |
Grade 5-8 | 76 (12.3) | 022 | 362 | 409 | 197 to 662 | .191 to .877** |
Secondary school | 21 (3.4) | 848 | 1.337 | 1.106 | 553 to 3.235 | .392 to 3.122 |
Diploma and above | 2 (3) | 486 | 1.471 | 2.710 | 091 to 23.713 | .486 to 44.846 |
Religion | ||||||
Orthodox | 409 (66) | R | R | |||
Muslim | 88 (14.2) | 687 | 932 | 886 | 574 to 1.513 | .491 to 1.597 |
Protestant | 82 (13.2) | 984 | 702 | 1.007 | 416 to 1.184 | .543 to 1.866 |
Waqefeta | 41 (6.6) | 013 | 661 | -2.123 | 322 to 1.357 | .858 to 5.262** |
Occupation | ||||||
Farmers | 483 (77.9) | R | R | |||
Merchant | 15 (2.4) | 998 | 2.228 | 000 | 1.363 to 3.642 | .000 to |
Employment | 75 (12.1) | 000 | 2.228 | 3.493 | 1.363 to 3.642 | 1.949 to 6.262*** |
Daily laborer | 47 (7.6) | 810 | 786 | 911 | 404 to 1.532 | .426 to 1.947 |
Immediate care | ||||||
Strongly disagree | 52 (8.4) | 182 | R | R | ||
Disagree | 94 (15.2) | 1330 | .714 | .707 | .358 to 1.425 | .353 to 1.419 |
Neutral | 31 (5) | 950 | 1.038 | .972 | .425 to 2.540 | .394 to 2.398 |
Agree | 242 (39) | 121 | .623 | .614 | .339 to 1.145 | .332 to 1.138 |
Strongly agree | 201 (32.4) | 036 | .524 | .508 | .280 to .980 | .270 to .957** |
Happy with CBHI offices opening times | ||||||
Strongly disagree | 13 (2.1) | R | R | |||
Disagree | 23 (3.7) | 0004 | .303 | -.049 | .072 to 1.269 | .006 to .384** |
Neutral | 22 (3.5) | 751 | 1.837 | 1.306 | .448 to 7.539 | .252 to 6.778 |
Agree | 261 (42.1) | 310 | .877 | .520 | .287 to 2.680 | .147 to 1.838 |
Strongly agree | 301 (48.5) | 004 | .171 | .157 | .055 to .530 | .044 to .556** |
Satisfied with paying premium schedule | ||||||
Strongly disagree | 8 (1.3) | R | R | |||
Disagree | 13 (2.1) | 002 | 196.00 | 150.66 | 10.86 to 3536.9 | 6.171 to 3678.207** |
Neutral | 29 (4.7) | 160 | 5.79 | 5.155 | .700 to 47.911 | .523 to 50.794 |
Agree | 212 (34.2) | 208 | 1.793 | 4.384 | .214 to 14.60 | .438 to 43.852 |
Strongly agree | 358 (57.7) | 1.000 | .000 | .000 | .000 to | .000 to |
AOR | Adjusted Odd Ratio |
CI | Confidence Interval |
CBHI | Community Based Health Insurance |
UHC | Universal Health Coverage |
EHIA | Ethiopia Health Insurance Agency |
OOPs | Out of Pocket Payments |
SNNPR | Southern Nation Nationality People Representative Region |
SPSS | Statistical Package for the Social Sciences |
STATA | Software for Statistics and Data Science |
| [1] | Addise, T., & Erkalo, D. (2021). The Magnitude of Satisfaction and Associated Factors Among Household Heads Who Visited Health Facilities with Community-Based Health Insurance Scheme in Anilemo District, Hadiya Zone, Southern Ethiopia. Risk Management and Healthcare Policy, 14, 145–154. |
| [2] | AWoHO. (2023). Adama Woreda Health Offices. Annual Report. Adama, Oromia. |
| [3] | Awosika, L. (2007). Health insurance and managed care in Nigeria. In Annals of Ibadan Postgraduate Medicine (Vol. 3, Issue 2). |
| [4] | Badacho AS, Tushune K, Ejigu Y,.(2016). Household satisfaction with a community-based health insurance scheme in Ethiopia. BMC Res Notes 2016; 9(1): 424. |
| [5] | Badacho, A. S., Tushune, K., Ejigu, Y., & Berheto, T. M. (2016). Household satisfaction with a community ‑ based health insurance scheme in Ethiopia. BMC Research Notes, 1–10. |
| [6] | Barnett, I., & Tefera, B. (2010). Poor Households’ Experiences and Perception of User Fees for Healthcare: a mixed-method study from Ethiopia. 59. |
| [7] | Begashaw, B., Tessema, F., & Gesesew, H. A. (2016). Health Care Seeking Behavior in Southwest Ethiopia. 1–13. |
| [8] | Dandesa, T. (2020). Seasonal And Annual Climate Profile of Adama. 7(2). |
| [9] | Devadasan N, Criel B, Damme WV, Lefevre P, Manoharan S, der Stuyft PV (2011). Community based health Insurance and patient satisfaction—evidence from India. Indian J Med Res; 133(1): 40–9. |
| [10] | E. Gujarati, D. N. (1995). Basic Econometrics. 3rd Edition, McGraw-Hill Inc., New York. |
| [11] | Ethiopian Health Insurance Agency.(2015). Evaluation of Community-Based Health Insurance Pilot Schemes in Ethiopia: Final Report. Addis Ababa, Ethiopia. |
| [12] | Feleke S, Mitiku W, Zelelew H, A. T. (2015). Ethiopia’s community-based health insurance: a step on the road to universal health coverage. |
| [13] | FMOH. (2003). Health Sector Development Programme IV Annual Performance Report EFY. Addis Ababa, Ethiopia. |
| [14] | FMOH. (2015). Health and Health Related Indicators of 2015. Addis Ababa, Ethiopia. |
| [15] | Jadoo S, Puteh SEW, Ahme Z and Jawdat (2012) A: Level of Patients’ Satisfaction Toward National Health Insurance in Istanbul City (Turkey). World Applied Sciences Journal, 17(8), 976–985. |
| [16] | Kebede, K. M., & Geberetsadik, S. M. (2019). Household satisfaction with community-based health insurance scheme and associated factors in piloted Sheko district, Southwest Ethiopia. PLOS ONE, 14(5), e0216414. |
| [17] | Lenth, R. V. (2001). Some Practical Guidelines for Effective Sample-Size Determination. 1–11. |
| [18] | Mcintyre, D. (2007). Learning from Experience: Health Care Financing in Low- and Middle-Income Countries. Global Forum for Health Research. Retrieved January 11. |
| [19] | Mitiku Kebede K, Geberetsadik SM (2019) Household satisfaction with community-based health insurance scheme and associated factors in piloted Sheko district; Southwest Ethiopia. PLoS ONE 14(5): e0216411. |
| [20] | Mukangendo, M., Nzayirambaho, M., Hitimana, R., & Yamuragiye, A. (2018). Factors contributing to low adherence to community-based health insurance in rural Rwanda: a mixed-methods study. Journal of Global Health, 8(2), 020801. |
| [21] | Shibesh S.(2017). Assessment of factors affecting uptake of community-based health insurance among Sabata Hawas district, Oromiya Region. Thesis, Addis Ababa University. |
| [22] | Tien TV, Holst J, Brandrup-Lukanow A: The inclusion of the poor in a social health insurance frame work: The strategies applied in Vietnam. Extending social protection in health GTZ version, Frankfurt am Main 2005: 63–70. |
| [23] | WHO. (2010). The World Health organization. World Health Report – Health Systems Financing: The Path to Universal Coverage. Geneva, Switzerland: WHO Press. |
APA Style
Nebi, J. M., Tadesse, B. R. (2024). Household Satisfaction with Community Health Insurance Scheme and Associated Factors in Adama Woreda, East Shewa Zone, Ethiopia. International Journal of Science, Technology and Society, 12(6), 178-195. https://doi.org/10.11648/j.ijsts.20241206.13
ACS Style
Nebi, J. M.; Tadesse, B. R. Household Satisfaction with Community Health Insurance Scheme and Associated Factors in Adama Woreda, East Shewa Zone, Ethiopia. Int. J. Sci. Technol. Soc. 2024, 12(6), 178-195. doi: 10.11648/j.ijsts.20241206.13
AMA Style
Nebi JM, Tadesse BR. Household Satisfaction with Community Health Insurance Scheme and Associated Factors in Adama Woreda, East Shewa Zone, Ethiopia. Int J Sci Technol Soc. 2024;12(6):178-195. doi: 10.11648/j.ijsts.20241206.13
@article{10.11648/j.ijsts.20241206.13,
author = {Jemal Midekso Nebi and Belay Roba Tadesse},
title = {Household Satisfaction with Community Health Insurance Scheme and Associated Factors in Adama Woreda, East Shewa Zone, Ethiopia
},
journal = {International Journal of Science, Technology and Society},
volume = {12},
number = {6},
pages = {178-195},
doi = {10.11648/j.ijsts.20241206.13},
url = {https://doi.org/10.11648/j.ijsts.20241206.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijsts.20241206.13},
abstract = {Understanding the level of satisfaction and factors associated with it is essential to ensure the sustainability of the community- based health insurance (CBHI) program. Therefore, this study aimed to assess household satisfaction with a community-based health insurance scheme and its associated factors in the Adama district. A community-based cross-sectional study was conducted in households of Adama district from February 15-30, 2023. The Systematic random sampling technique under multi-stage sampling was used to select study participants. A face-to-face interview with a total of 620 households was conducted by using a pre-tested structured questionnaire. Descriptive analysis, bivariable, and multivariable logistic regression analysis were conducted. Variables with p-value < 0.05 were considered statistically significant to determine independent predictors of household satisfaction with the CBHI scheme. The level of household satisfaction with the CBHI scheme was found to be 61.1%. Satisfaction was found significantly associated with male household heads (AOR=0.545; 95% C.I 0.358-0.831), households with the educational level of able to read and write, grade 1-4 and grade 5-8,(AOR=0.281; 95% C.I 0.131-0.603; AOR=0.533; 95% C.I 0.311-0.915 and, AOR=0.409; 95% C.I 0.191-0.877) respectively, followers of waqefeta religion (AOR=2.123; 95% C.I 0.858-5.262), occupation of government employment (AOR=3.493; 95% C.I 1.949-6.262), those who strongly agreed with immediate care (AOR=0.508; 95% C.I 0.270-0.957), those who strongly agree and disagree with CBHI scheme office opining time (AOR=0.157; 95% C.I 0.044-0.556; AOR=-0.049; 95% C.I 0.006-0.384) and those who disagree with payment of premium schedule (AOR=150.66; 95% C.I 6.171-3678.207). This study showed that the overall satisfaction of households in the Adama district with the CBHI scheme was very good. Male households, waqefeta region followers, occupation of government employees, educational level, immediate care, BBHI office opening time, and premium schedule paying were significant factors of satisfaction with CBHI. Consideration should be given to increasing the accessibility of immediate health care, improving the educational level of households, and improving enrollee’s knowledge of CBHI benefit packages.
},
year = {2024}
}
TY - JOUR T1 - Household Satisfaction with Community Health Insurance Scheme and Associated Factors in Adama Woreda, East Shewa Zone, Ethiopia AU - Jemal Midekso Nebi AU - Belay Roba Tadesse Y1 - 2024/12/19 PY - 2024 N1 - https://doi.org/10.11648/j.ijsts.20241206.13 DO - 10.11648/j.ijsts.20241206.13 T2 - International Journal of Science, Technology and Society JF - International Journal of Science, Technology and Society JO - International Journal of Science, Technology and Society SP - 178 EP - 195 PB - Science Publishing Group SN - 2330-7420 UR - https://doi.org/10.11648/j.ijsts.20241206.13 AB - Understanding the level of satisfaction and factors associated with it is essential to ensure the sustainability of the community- based health insurance (CBHI) program. Therefore, this study aimed to assess household satisfaction with a community-based health insurance scheme and its associated factors in the Adama district. A community-based cross-sectional study was conducted in households of Adama district from February 15-30, 2023. The Systematic random sampling technique under multi-stage sampling was used to select study participants. A face-to-face interview with a total of 620 households was conducted by using a pre-tested structured questionnaire. Descriptive analysis, bivariable, and multivariable logistic regression analysis were conducted. Variables with p-value < 0.05 were considered statistically significant to determine independent predictors of household satisfaction with the CBHI scheme. The level of household satisfaction with the CBHI scheme was found to be 61.1%. Satisfaction was found significantly associated with male household heads (AOR=0.545; 95% C.I 0.358-0.831), households with the educational level of able to read and write, grade 1-4 and grade 5-8,(AOR=0.281; 95% C.I 0.131-0.603; AOR=0.533; 95% C.I 0.311-0.915 and, AOR=0.409; 95% C.I 0.191-0.877) respectively, followers of waqefeta religion (AOR=2.123; 95% C.I 0.858-5.262), occupation of government employment (AOR=3.493; 95% C.I 1.949-6.262), those who strongly agreed with immediate care (AOR=0.508; 95% C.I 0.270-0.957), those who strongly agree and disagree with CBHI scheme office opining time (AOR=0.157; 95% C.I 0.044-0.556; AOR=-0.049; 95% C.I 0.006-0.384) and those who disagree with payment of premium schedule (AOR=150.66; 95% C.I 6.171-3678.207). This study showed that the overall satisfaction of households in the Adama district with the CBHI scheme was very good. Male households, waqefeta region followers, occupation of government employees, educational level, immediate care, BBHI office opening time, and premium schedule paying were significant factors of satisfaction with CBHI. Consideration should be given to increasing the accessibility of immediate health care, improving the educational level of households, and improving enrollee’s knowledge of CBHI benefit packages. VL - 12 IS - 6 ER -
Departement of Sociology and Social Work, Arsi University, Asella, Ethiopia
Ethiopian Institute of Agricultural Research, Melkassa Agricultural Research Center, Melkassa, Ethiopia
Information