The purpose of this study is to examine the effects of the COVID-19 pandemic and the ensuing lockdown on children's mental health in four Kerala districts. During the second wave of the COVID-19 pandemic, from May 16 to June 4, 2021, 400 parents with at least one child between the ages of 5 and 15 participated in an online cross-sectional study using a non-probability sampling technique. Children were classified according to their mental health scores using discriminant analysis, and the association between parental behavior and children's mental health was identified using confirmatory factor analysis (CFA). The chi-square test was also used to evaluate these correlations. Four levels of mental health difficulties were identified in children: 43% had minimal difficulties (mean MDD-10: 2.8), 30.5% had emerging difficulties (mean MDD-10: 8.9), 19.3% had significant difficulties (mean MDD-10: 15.9), and 7.2% had high-risk or severe difficulties (mean MDD-10: 25.2). Children whose parents were required to continue working on-site, had relatives infected with COVID-19, had higher levels of education, or exhibited abnormal behaviors were found to have a higher percentage of mental health disorders. In contrast, children whose parents did not experience these difficulties. The results show that during the second wave of COVID-19, especially during the lockdown period between May and June 2021, a significant percentage of children in Kerala had mental health issues. Children's psychological well-being may be improved by putting psychological intervention techniques into practice, increasing parental literacy, strengthening job security, ensuring appropriate childcare, and improving household financial stability. Children's psychological wellbeing may improve as a result of increased security. The study's conclusions, according to the authors, will help Kerala make progress toward the Sustainable Development Goals (SDGs) pertaining to health.
| Published in | International Journal of Statistical Distributions and Applications (Volume 12, Issue 1) |
| DOI | 10.11648/j.ijsda.20261201.12 |
| Page(s) | 13-23 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
COVID-19, Psychological Impact, Confirmatory Factor Analysis, Statistical Models
Group | Variable | Number | Percentage (%) |
|---|---|---|---|
Sex | Female | 287 | 74.7 |
Sex | Male | 94 | 24.5 |
Sex | Other | 3 | 0.8 |
Age | < 25 years | 14 | 3.6 |
Age | 26–35 years | 118 | 30.7 |
Age | 36–45 years | 135 | 35.2 |
Age | 46–55 years | 117 | 30.5 |
Age | > 55 years | 0 | 0.0 |
Education | S.S.C / H.S.C | 224 | 58.3 |
Education | Graduation | 85 | 22.1 |
Education | Primary | 46 | 12.0 |
Education | Post-Graduation | 29 | 7.6 |
Education | PhD | 0 | 0.0 |
Place of Living | Urban | 179 | 46.6 |
Place of Living | Rural | 173 | 45.1 |
Place of Living | Semi-urban | 32 | 8.3 |
Job Status | No | 168 | 43.7 |
Job Status | Yes | 216 | 56.3 |
Financial Tension | No | 124 | 32.3 |
Financial Tension | Yes | 260 | 67.7 |
Need to Go to Workplace | No | 287 | 74.7 |
Need to Go to Workplace | Yes | 97 | 25.3 |
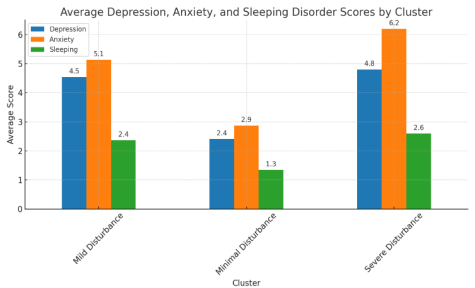
Variables | Minimal Disturbance (n = 357) | Mild Disturbance (n = 22) | Severe Disturbance (n = 5) | p-value |
|---|---|---|---|---|
Number (Percentages) | 357 (93.0%) | 22 (5.7%) | 5 (1.3%) | — |
Depression M(SD) (Emotional symptoms) | 2.41 (1.49) | 4.55 (2.26) | 4.80 (1.48) | < 0.001 |
Anxiety M(SD) (Hyperactivity) | 2.87 (1.66) | 5.14 (1.86) | 6.20 (1.30) | < 0.001 |
Sleeping Disturbance M (SD) (Peer problems) | 1.35 (1.14) | 2.36 (1.33) | 2.60 (1.14) | < 0.001 |
Variable | Category | Normal (N,%) | Borderline (N,%) | Abnormal (N,%) | Total | p-value |
|---|---|---|---|---|---|---|
Sex | Female | 269 (93.7%) | 14 (4.9%) | 4 (1.4%) | 287 | 0.7354 |
Sex | Male | 85 (90.4%) | 8 (8.5%) | 1 (1.1%) | 94 | 0.7354 |
Sex | Other | 3 (100.0%) | 0 (0.0%) | 0 (0.0%) | 3 | 0.7354 |
Age | <25 | 13 (92.9%) | 1 (7.1%) | 0 (0.0%) | 14 | 0.7454 |
Age | 26-35 | 111 (94.1%) | 7 (5.9%) | 0 (0.0%) | 118 | 0.7454 |
Age | 36-45 | 126 (93.3%) | 6 (4.4%) | 3 (2.2%) | 135 | 0.7454 |
Age | 46-55 | 107 (91.5%) | 8 (6.8%) | 2 (1.7%) | 117 | 0.7454 |
Education Level | Graduation | 77 (90.6%) | 6 (7.1%) | 2 (2.4%) | 85 | 0.8794 |
Education Level | Post-Graduation | 27 (93.1%) | 2 (6.9%) | 0 (0.0%) | 29 | 0.8794 |
Education Level | Primary | 42 (91.3%) | 3 (6.5%) | 1 (2.2%) | 46 | 0.8794 |
Education Level | S.S.C/H.S.C | 211 (94.2%) | 11 (4.9%) | 2 (0.9%) | 224 | 0.8794 |
Place of Living | Rural | 166 (96.0%) | 5 (2.9%) | 2 (1.2%) | 173 | 0.2413 |
Place of Living | Semi-urban | 29 (90.6%) | 3 (9.4%) | 0 (0.0%) | 32 | 0.2413 |
Place of Living | Urban | 162 (90.5%) | 14 (7.8%) | 3 (1.7%) | 179 | 0.2413 |
Relatives/Neighbor infected | No | 311 (93.4%) | 18 (5.4%) | 4 (1.2%) | 333 | 0.7035 |
Relatives/Neighbor infected | Yes | 46 (90.2%) | 4 (7.8%) | 1 (2.0%) | 51 | 0.7035 |
Average Family Income | 2–3 lakhs | 72 (94.7%) | 4 (5.3%) | 0 (0.0%) | 76 | 0.86 |
Average Family Income | 3–4 lakhs | 56 (93.3%) | 3 (5.0%) | 1 (1.7%) | 60 | 0.86 |
Average Family Income | 4–5 lakhs | 55 (93.2%) | 3 (5.1%) | 1 (1.7%) | 59 | 0.86 |
Average Family Income | 5+ lakhs | 121 (92.4%) | 9 (6.9%) | 1 (0.8%) | 131 | 0.86 |
Average Family Income | < 2 lakhs | 53 (91.4%) | 3 (5.2%) | 2 (3.4%) | 58 | 0.86 |
Need to go Workplace | No | 265 (92.3%) | 18 (6.3%) | 4 (1.4%) | 287 | 0.7025 |
Need to go Workplace | Yes | 92 (94.8%) | 4 (4.1%) | 1 (1.0%) | 97 | 0.7025 |
Chance of losing Job | No | 310 (93.4%) | 17 (5.1%) | 5 (1.5%) | 332 | 0.2994 |
Chance of losing Job | Yes | 47 (90.4%) | 5 (9.6%) | 0 (0.0%) | 52 | 0.2994 |
Feeling bored at Home | No | 52 (91.2%) | 5 (8.8%) | 0 (0.0%) | 57 | 0.6468 |
Feeling bored at Home | Sometimes | 156 (92.3%) | 10 (5.9%) | 3 (1.8%) | 169 | 0.6468 |
Feeling bored at Home | Yes | 149 (94.3%) | 7 (4.4%) | 2 (1.3%) | 158 | 0.6468 |
Smoker | No | 289 (92.0%) | 20 (6.4%) | 5 (1.6%) | 314 | 0.2854 |
Smoker | Yes | 68 (97.1%) | 2 (2.9%) | 0 (0.0%) | 70 | 0.2854 |
Child Cartoon Hours | 2–4 h | 126 (92.6%) | 8 (5.9%) | 2 (1.5%) | 136 | 0.9696 |
Child Cartoon Hours | 4–6 h | 40 (90.9%) | 4 (9.1%) | 0 (0.0%) | 44 | 0.9696 |
Child Cartoon Hours | 6–8 h | 7 (100.0%) | 0 (0.0%) | 0 (0.0%) | 7 | 0.9696 |
Child Cartoon Hours | < 2 h | 183 (93.4%) | 10 (5.1%) | 3 (1.5%) | 196 | 0.9696 |
Child Cartoon Hours | > 8 h | 1 (100.0%) | 0 (0.0%) | 0 (0.0%) | 1 | 0.9696 |
Child Gaming Hours | 2–4 h | 81 (91.0%) | 6 (6.7%) | 2 (2.2%) | 89 | 0.9338 |
Child Gaming Hours | 4–6 h | 30 (93.8%) | 1 (3.1%) | 1 (3.1%) | 32 | 0.9338 |
Child Gaming Hours | 6–8 h | 4 (100.0%) | 0 (0.0%) | 0 (0.0%) | 4 | 0.9338 |
Child Gaming Hours | < 2 h | 240 (93.4%) | 15 (5.8%) | 2 (0.8%) | 257 | 0.9338 |
Child Gaming Hours | > 8 h | 2 (100.0%) | 0 (0.0%) | 0 (0.0%) | 2 | 0.9338 |
Child Fights | No | 192 (92.3%) | 12 (5.8%) | 4 (1.9%) | 208 | 0.5049 |
Child Fights | Yes | 165 (93.8%) | 10 (5.7%) | 1 (0.6%) | 176 | 0.5049 |
Keep Child Busy | No | 87 (91.6%) | 6 (6.3%) | 2 (2.1%) | 95 | 0.6951 |
Keep Child Busy | Yes | 270 (93.4%) | 16 (5.5%) | 3 (1.0%) | 289 | 0.6951 |
Child Acting Normal | No | 61 (95.3%) | 3 (4.7%) | 0 (0.0%) | 64 | 0.374 |
Child Acting Normal | Not noticeable | 93 (89.4%) | 8 (7.7%) | 3 (2.9%) | 104 | 0.374 |
Child Acting Normal | Yes | 203 (94.0%) | 11 (5.1%) | 2 (0.9%) | 216 | 0.374 |
Child Complains Parent Busy | No | 238 (92.6%) | 16 (6.2%) | 3 (1.2%) | 257 | 0.797 |
Child Complains Parent Busy | Yes | 119 (93.7%) | 6 (4.7%) | 2 (1.6%) | 127 | 0.797 |
Calling Child Bad Names | No | 254 (92.7%) | 15 (5.5%) | 5 (1.8%) | 274 | 0.3459 |
Calling Child Bad Names | Yes | 103 (93.6%) | 7 (6.4%) | 0 (0.0%) | 110 | 0.3459 |
Threatening Child | No | 216 (91.5%) | 16 (6.8%) | 4 (1.7%) | 236 | 0.3602 |
Threatening Child | Yes | 141 (95.3%) | 6 (4.1%) | 1 (0.7%) | 148 | 0.3602 |
Screaming at Child | No | 207 (95.4%) | 7 (3.2%) | 3 (1.4%) | 217 | 0.0551 |
Screaming at Child | Yes | 150 (89.8%) | 15 (9.0%) | 2 (1.2%) | 167 | 0.0551 |
Hitting Child | No | 287 (92.6%) | 19 (6.1%) | 4 (1.3%) | 310 | 0.7879 |
Hitting Child | Yes | 70 (94.6%) | 3 (4.1%) | 1 (1.4%) | 74 | 0.7879 |
Hitting with Object | No | 297 (92.5%) | 19 (5.9%) | 5 (1.6%) | 321 | 0.5638 |
Hitting with Object | Yes | 60 (95.2%) | 3 (4.8%) | 0 (0.0%) | 63 | 0.5638 |
Common Abuse Type | Emotional abuse | 112 (91.8%) | 8 (6.6%) | 2 (1.6%) | 122 | 0.4616 |
Common Abuse Type | Family violence | 69 (90.8%) | 6 (7.9%) | 1 (1.3%) | 76 | 0.4616 |
Common Abuse Type | Neglect abuse | 52 (96.3%) | 2 (3.7%) | 0 (0.0%) | 54 | 0.4616 |
Common Abuse Type | Physical abuse | 95 (96.9%) | 2 (2.0%) | 1 (1.0%) | 98 | 0.4616 |
Common Abuse Type | Sexual abuse | 29 (85.3%) | 4 (11.8%) | 1 (2.9%) | 34 | 0.4616 |
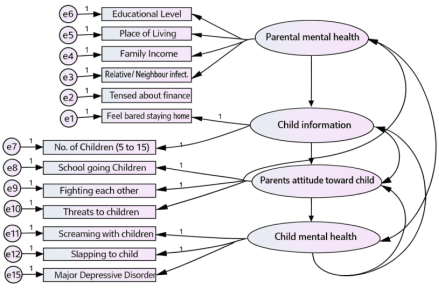
Latent Variables | Parental MH | Child Info | Parent Attitude | Child MH |
|---|---|---|---|---|
Parental MH | 1.000 | 0.005 | –0.022 | 0.100 |
Child Info | 0.005 | 1.000 | 0.099 | 0.043 |
Parent Attitude | –0.022 | 0.099 | 1.000 | –0.014 |
Child MH | 0.100 | 0.043 | –0.014 | 1.000 |
CFA | Confirmatory Factor Analysis |
MDD | Major Depressive Disorder |
SDGs | Sustainable Development Goals |
SDQ-P | Strengths and Difficulties Questionnaire–Parent Version |
PHQ-A | Patient Health Questionnaire for Adolescents |
SCARED-P | Screen for Child Anxiety Related Disorders–Parent Version |
PSC | Pediatric Symptom Checklist |
CSHQ-A | Abridged Children’s Sleep Habits Questionnaire |
SEM | Structural Equation Modelling |
MH | Mental Health |
| [1] | Brooks, S. K., Webster, R. K., Smith, L. E., et al. (2020). The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. The Lancet, 395(10227), 912–920. |
| [2] | Singh, S., Roy, D., Sinha, K., Parveen, S., Sharma, G., & Joshi, G. (2020). Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review. Psychiatry Research, 293, 113429. |
| [3] | Government of Kerala. (2021). Kerala COVID-19 daily updates. Department of Health Services. |
| [4] | Jiao, W. Y., Wang, L. N., Liu, J., et al. (2020). Behavioral and emotional disorders in children during the COVID-19 epidemic. The Journal of Pediatrics, 221, 264–266. |
| [5] | Kline, R. B. (2016). Principles and practice of structural equation modeling (4th ed.). Guilford Press. |
| [6] | Kroenke, K., Spitzer, R. L., & Williams, J. (2001). The PHQ-9: Validity of a brief depression severity measure. Journal of General Internal Medicine, 16(9), 606–613. |
| [7] | Orgilés, M., Morales, A., Delvecchio, E., et al. (2020). Immediate psychological effects of the COVID-19 quarantine in youth from Italy and Spain. Frontiers in Psychology, 11, 579038. |
| [8] | Panda, P. K., Gupta, J., Chowdhury, S. R., et al. (2021). Psychological and behavioral impact of lockdown and quarantine measures for COVID-19 pandemic on children, adolescents and caregivers: A systematic review. Psychiatry Research, 293, 113429. |
| [9] | Pillai, Swapna K; Nair, Rekha S; Sundeep, S1 (2023). Study of Impact of COVID-19 Infection and Lockdown on Mental Health, Nutrition, and Lifestyle Practices in Children: A Cross-sectional Study in a Tertiary Hospital in Kerala. Journal of Applied Sciences and Clinical Practice 4(3): p 202-210 |
| [10] | Singh, S., Roy, D., Sinha, K., et al. (2020). Impact of COVID-19 and lockdown on mental health of children and adolescents: A narrative review. Psychiatry Research, 293, 113429. |
| [11] | Spinelli, M., Lionetti, F., Pastore, M., & Fasolo, M. (2020). Parents’ stress and children’s psychological problems in families facing the COVID-19 outbreak in Italy. Frontiers in Psychology, 11, 1713. |
| [12] | United Nations. (2015). Transforming our world: The 2030 Agenda for Sustainable Development. |
| [13] | Dunleavy, B. P. (2020). 20% of children on lockdown in China suffer depression, anxiety, study finds. United Press International. |
| [14] | Francesconi, M., & Ermisch, J. (2000). The Effect of Parents’ Employment on Children’s Educational Attainment. IZA Discussion Paper, 215. |
| [15] | Galvin, G. (2020). With Schools Closed, Chinese Primary School Students Show Signs of Depression, Anxiety. U.S. News. |
| [16] | Jagoda Grzejszczak, Dominik Strzelecki, Agata Gabryelska, Magdalena Kotlicka-Antczak, J. Clin. Med. 2024, 13(3), 744; |
| [17] | Yosep, I.; Purnama, H.; Lindayani, L.; Chen, Y.-C.; Sudrajat, D. A.; Firdaus, M. R. The Relationship Between Bullying and Risk of Suicide Among Adolescents During the COVID-19 Pandemic in Indonesia. J. Korean Acad. Child Adolesc. Psychiatry 2024, 35, 75–81. |
| [18] | Ruishuai Miao, Chang Liu, Jiarong Zhang, Hui Jin (2023). Impact of the COVID-19 pandemic on the mental health of children and adolescents: A systematic review and meta-analysis of longitudinal studies. Journal of Affective Disorders, 914-922, |
| [19] | Stipe Vidović, Slavica Kotromanović, Zenon Pogorelić (2024). Depression, Anxiety, and Stress Symptoms Among Students in Croatia During the COVID-19 Pandemic: A Systematic Review, Journal of Clinical Medicine, |
| [20] | Du, Xiayu (2025). Trend of Chinese adolescent anxiety symptoms before and after COVID-19: A cross-temporal meta-analysis with segmented regression, Journal of Research on Adolescence. |
APA Style
Ramachandran, D. V., Senthilkumar, B., Bhat, M., Mathews, A. J. (2026). Psychological Impact of the COVID-19 Pandemic on Children in Kerala: A Cross-sectional Analysis. International Journal of Statistical Distributions and Applications, 12(1), 13-23. https://doi.org/10.11648/j.ijsda.20261201.12
ACS Style
Ramachandran, D. V.; Senthilkumar, B.; Bhat, M.; Mathews, A. J. Psychological Impact of the COVID-19 Pandemic on Children in Kerala: A Cross-sectional Analysis. Int. J. Stat. Distrib. Appl. 2026, 12(1), 13-23. doi: 10.11648/j.ijsda.20261201.12
@article{10.11648/j.ijsda.20261201.12,
author = {Divya Valiyattil Ramachandran and Balan Senthilkumar and Mohini Bhat and Ashok Jacob Mathews},
title = {Psychological Impact of the COVID-19 Pandemic on Children in Kerala: A Cross-sectional Analysis},
journal = {International Journal of Statistical Distributions and Applications},
volume = {12},
number = {1},
pages = {13-23},
doi = {10.11648/j.ijsda.20261201.12},
url = {https://doi.org/10.11648/j.ijsda.20261201.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijsda.20261201.12},
abstract = {The purpose of this study is to examine the effects of the COVID-19 pandemic and the ensuing lockdown on children's mental health in four Kerala districts. During the second wave of the COVID-19 pandemic, from May 16 to June 4, 2021, 400 parents with at least one child between the ages of 5 and 15 participated in an online cross-sectional study using a non-probability sampling technique. Children were classified according to their mental health scores using discriminant analysis, and the association between parental behavior and children's mental health was identified using confirmatory factor analysis (CFA). The chi-square test was also used to evaluate these correlations. Four levels of mental health difficulties were identified in children: 43% had minimal difficulties (mean MDD-10: 2.8), 30.5% had emerging difficulties (mean MDD-10: 8.9), 19.3% had significant difficulties (mean MDD-10: 15.9), and 7.2% had high-risk or severe difficulties (mean MDD-10: 25.2). Children whose parents were required to continue working on-site, had relatives infected with COVID-19, had higher levels of education, or exhibited abnormal behaviors were found to have a higher percentage of mental health disorders. In contrast, children whose parents did not experience these difficulties. The results show that during the second wave of COVID-19, especially during the lockdown period between May and June 2021, a significant percentage of children in Kerala had mental health issues. Children's psychological well-being may be improved by putting psychological intervention techniques into practice, increasing parental literacy, strengthening job security, ensuring appropriate childcare, and improving household financial stability. Children's psychological wellbeing may improve as a result of increased security. The study's conclusions, according to the authors, will help Kerala make progress toward the Sustainable Development Goals (SDGs) pertaining to health.},
year = {2026}
}
TY - JOUR T1 - Psychological Impact of the COVID-19 Pandemic on Children in Kerala: A Cross-sectional Analysis AU - Divya Valiyattil Ramachandran AU - Balan Senthilkumar AU - Mohini Bhat AU - Ashok Jacob Mathews Y1 - 2026/01/26 PY - 2026 N1 - https://doi.org/10.11648/j.ijsda.20261201.12 DO - 10.11648/j.ijsda.20261201.12 T2 - International Journal of Statistical Distributions and Applications JF - International Journal of Statistical Distributions and Applications JO - International Journal of Statistical Distributions and Applications SP - 13 EP - 23 PB - Science Publishing Group SN - 2472-3509 UR - https://doi.org/10.11648/j.ijsda.20261201.12 AB - The purpose of this study is to examine the effects of the COVID-19 pandemic and the ensuing lockdown on children's mental health in four Kerala districts. During the second wave of the COVID-19 pandemic, from May 16 to June 4, 2021, 400 parents with at least one child between the ages of 5 and 15 participated in an online cross-sectional study using a non-probability sampling technique. Children were classified according to their mental health scores using discriminant analysis, and the association between parental behavior and children's mental health was identified using confirmatory factor analysis (CFA). The chi-square test was also used to evaluate these correlations. Four levels of mental health difficulties were identified in children: 43% had minimal difficulties (mean MDD-10: 2.8), 30.5% had emerging difficulties (mean MDD-10: 8.9), 19.3% had significant difficulties (mean MDD-10: 15.9), and 7.2% had high-risk or severe difficulties (mean MDD-10: 25.2). Children whose parents were required to continue working on-site, had relatives infected with COVID-19, had higher levels of education, or exhibited abnormal behaviors were found to have a higher percentage of mental health disorders. In contrast, children whose parents did not experience these difficulties. The results show that during the second wave of COVID-19, especially during the lockdown period between May and June 2021, a significant percentage of children in Kerala had mental health issues. Children's psychological well-being may be improved by putting psychological intervention techniques into practice, increasing parental literacy, strengthening job security, ensuring appropriate childcare, and improving household financial stability. Children's psychological wellbeing may improve as a result of increased security. The study's conclusions, according to the authors, will help Kerala make progress toward the Sustainable Development Goals (SDGs) pertaining to health. VL - 12 IS - 1 ER -
Department of Statistics, Bharathidasan University, Tiruchirappalli, India
Department of Statistics, Thanthai Periyar Government Arts & Science College (Autonomous), Tiruchirappalli, India
Department of Management, Christ Academy Institute for Advanced Studies, Bengaluru, India
Department of Political Science, St. Claret College (Autonomous), Bengaluru, India
Information