Background: X-linked dystonia parkinsonism (XDP, DYT3), a disease endemic to Panay Island in the Philippines, is a progressive adult-onset sex-linked neurodegenerative movement disorder with features of both dystonia and parkinsonism. Medical treatment and botulinum toxin injection (BTX) are of limited benefit. Deep brain stimulation (DBS) of the bilateral globus pallidus internus (GPi) is effective but is expensive and requires specialized equipment, training and after care. Posteroventral pallidotomy (PVP) is an older known ablative procedure which has successfully treated cervical and generalized dystonia, but has not been previously used for XDP. Case presentation: Two male adults with genetically-confirmed XDP, presented with progressive and severely disabling dystonias. The mean preoperative Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) was 80.5. Both XDP patients underwent a unilateral posteroventral pallidotomy. In the first case, there was a 38.46% decrease in BFMDRS score at 2 weeks sustained to 41.66% decrease (compared to pre-op BFMDRS at 4 years post-surgery). In the second case, there was a 33.73% decrease in BFMDRS at 2 months post-op, and a decrease of 86.74% in BFMDRS score at 3 years post-surgery. Conclusion: While not as effective as bilateral pallidal DBS, the benefits of a unilateral PVP are still substantial and sustained while also being less costly and resource expensive.
| Published in | International Journal of Neurosurgery (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijn.20250901.13 |
| Page(s) | 17-22 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
XDP, Dystonia, Parkinsonism, Pallidotomy
Timeline of assessment | BFMDRS score | % improvement from baseline |
|---|---|---|
Pre-op | 78 | --- |
Post-op | 80 | -2.56% |
2 weeks | 48 | 38.46% |
1 month | 64 | 17.94% |
2 months | 52 | 33.33% |
4 months | 53 | 32.05% |
1 year | 49 | 37.17% |
2 years | 45.5 | 41.66% |
4 years | 51 | 34.61% |
Components of BFMDRS | Baseline | Post-op | 2 weeks | 1 month | 2 months | 4 months | 1 year | 2 years | 4 years |
|---|---|---|---|---|---|---|---|---|---|
Eyes | 8 | 8 | 6 | 8 | 6 | 0 | 3 | 6 | 2 |
Mouth | 8 | 6 | 4 | 8 | 6 | 6 | 6 | 4 | 8 |
Speech & swallowing | 12 | 12 | 9 | 9 | 8 | 4 | 8 | 2 | 8 |
Neck | 8 | 6 | 8 | 8 | 6 | 6 | 6 | 4.5 | 6 |
Right arm | 9 | 9 | 8 | 4 | 8 | 6 | 4 | 1 | 6 |
Left arm | 12 | 12 | 4 | 9 | 4 | 9 | 6 | 8 | 6 |
Right leg | 3 | 6 | 1 | 1 | 1 | 1 | 4 | 0 | 6 |
Left leg | 6 | 9 | 0 | 1 | 0 | 3 | 6 | 8 | 6 |
Trunk | 12 | 12 | 8 | 16 | 12 | 12 | 6 | 12 | 3 |
TOTAL | 78 | 80 | 48 | 64 | 52 | 53 | 49 | 45.5 | 51 |
% Improvement compared to baseline | - | -2.5% | 38.46% | 17.94% | 33.33% | 32.05% | 37.17% | 41.66% | 34.61% |
Timeline of assessment | BFMDRS score | % improvement from baseline |
|---|---|---|
Pre-op | 83 | --- |
2 months | 55 | 33.73% |
3 months | 34 | 59.03% |
1 year | 25 | 69.87% |
3 years | 11 | 86.74% |
Components of BFMDRS | Pre-op | 2 months | 3 months | 1 year | 3 years |
|---|---|---|---|---|---|
Eyes | 8 | 2 | 2 | 0 | 0.5 |
Mouth | 8 | 6 | 2 | 2 | 0.5 |
Speech & swallowing | 12 | 6 | 6 | 2 | 1 |
Neck | 8 | 8 | 6 | 6 | 6 |
Right arm | 8 | 6 | 4 | 1 | 0 |
Left arm | 12 | 12 | 6 | 4 | 2 |
Right leg | 6 | 0 | 0 | 0 | 0 |
Left leg | 9 | 3 | 2 | 1 | 0 |
Trunk | 12 | 12 | 6 | 9 | 1 |
TOTAL | 83 | 55 | 34 | 25 | 11 |
% Improvement compared to baseline | --- | 33.73% | 59.03% | 69.87% | 86.74% |
ADL | Activities of Daily Living |
BTX | Botulinum Toxin |
BFMDRS | Burke-Fahn-Marsden Dystonia Rating Scale |
CT | Computerized Tomography |
DBS | Deep Brain Stimulation |
GPi | Globus Pallidus Internus |
MRI | Magnetic Resonance Imaging |
PVP | Posteroventral Pallidotomy |
SVA | SINE-VNTR-Alus |
XDP | X-linked Dystonia Parkinsonism |
| [1] | Lee LV, Maranon E, Demaisip C, Peralta O, Borres-Icasiano R, Arancillo J, ... Reyes MT. The natural history of sex-linked recessive dystonia parkinsonism of Panay, Philippines (XDP)*. Parkinsonism Relat Disord. 2002; 9(1): 29-38. |
| [2] | Jamora RDG, Diesta CCE, Pasco PMD, Lee LV. Oral pharmacological treatment of X-linked dystonia parkinsonism: successes and failures. Int J Neurosci. 2011; 121 Suppl: 18-21. |
| [3] | Badillo SPJ, Jamora RDG. Zolpidem for the treatment of dystonia. Front Neurol. 2019. |
| [4] | Aguilar JA, Vesagas TS, Jamora RD, Teleg RA, Ledesma L, Rosales RL, ... Lee LV. The promise of deep brain stimulation in X-linked dystonia parkinsonism. Int J Neurosci. 2011; 121(Suppl 1): 57-63. |
| [5] | Hariz M. Pallidotomy for dystonia: a neglected procedure? Mov Disord. 2021; 36(3): 533-4. |
| [6] | Vitek JL. Surgery for dystonia. Neurosurg Clin N Am. 1998; 9(2): 345-366. Available from: |
| [7] | Gross RE. What happened to posteroventral pallidotomy for Parkinson’s disease and dystonia? Neurotherapeutics. 2008; 5(2): 281-293. |
| [8] | Centen LM, Oterdoom DLM, Tijssen MAJ, Lesman-Leegte I, van Egmond ME, van Dijk JMC. Bilateral pallidotomy for dystonia: a systematic review. Mov Disord. 2021; 36. |
| [9] | De Roxas R, Jamora RDG. Cost-analysis of the different treatment modalities in X-linked dystonia-parkinsonism. Front Neurol. 2019; 10: 500. |
| [10] | Rosales RL. X-linked dystonia parkinsonism: clinical phenotype, genetics and therapeutics. J Mov Disord. 2010. |
| [11] | Brüggemann N, Domingo A, Rasche D, Moll CKE, Rosales RL, Jamora RDG, ... Klein C. Association of pallidal neurostimulation and outcome predictors with X-linked dystonia parkinsonism. JAMA Neurol. 2019. |
| [12] | Abejero JEE, Jamora RDG, Vesagas TS, Teleg RA, Rosales RL, Anlacan JP, ... Aguilar JA. Long-term outcomes of pallidal deep brain stimulation in X-linked dystonia parkinsonism (XDP): up to 84 months follow-up and review of literature. Parkinsonism Relat Disord. 2019. |
| [13] | Dannug AT, Gabriel FGC, Macias MCYL, Diesta CCE. Impact of deep brain stimulation on quality of life and motor symptoms in Parkinson's disease and X-linked dystonia parkinsonism: The Philippine experience. Parkinsonism Relat Disord. 2021; 87: 92-7. |
| [14] | Fenoy AJ, Simpson RK. Risks of common complications in deep brain stimulation surgery: management and avoidance—clinical article. J Neurosurg. 2014. |
APA Style
Cataniag, P., Diesta, C. C., Gamboa, J. A., Oropilla, J. Q. (2025). Sustained Effect of Posteroventral Pallidotomy for X-Linked Dystonia Parkinsonism. International Journal of Neurosurgery, 9(1), 17-22. https://doi.org/10.11648/j.ijn.20250901.13
ACS Style
Cataniag, P.; Diesta, C. C.; Gamboa, J. A.; Oropilla, J. Q. Sustained Effect of Posteroventral Pallidotomy for X-Linked Dystonia Parkinsonism. Int. J. Neurosurg. 2025, 9(1), 17-22. doi: 10.11648/j.ijn.20250901.13
@article{10.11648/j.ijn.20250901.13,
author = {Paulo Cataniag and Cid Czarina Diesta and Julie Anne Gamboa and Jean Quint Oropilla},
title = {Sustained Effect of Posteroventral Pallidotomy for X-Linked Dystonia Parkinsonism},
journal = {International Journal of Neurosurgery},
volume = {9},
number = {1},
pages = {17-22},
doi = {10.11648/j.ijn.20250901.13},
url = {https://doi.org/10.11648/j.ijn.20250901.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijn.20250901.13},
abstract = {Background: X-linked dystonia parkinsonism (XDP, DYT3), a disease endemic to Panay Island in the Philippines, is a progressive adult-onset sex-linked neurodegenerative movement disorder with features of both dystonia and parkinsonism. Medical treatment and botulinum toxin injection (BTX) are of limited benefit. Deep brain stimulation (DBS) of the bilateral globus pallidus internus (GPi) is effective but is expensive and requires specialized equipment, training and after care. Posteroventral pallidotomy (PVP) is an older known ablative procedure which has successfully treated cervical and generalized dystonia, but has not been previously used for XDP. Case presentation: Two male adults with genetically-confirmed XDP, presented with progressive and severely disabling dystonias. The mean preoperative Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) was 80.5. Both XDP patients underwent a unilateral posteroventral pallidotomy. In the first case, there was a 38.46% decrease in BFMDRS score at 2 weeks sustained to 41.66% decrease (compared to pre-op BFMDRS at 4 years post-surgery). In the second case, there was a 33.73% decrease in BFMDRS at 2 months post-op, and a decrease of 86.74% in BFMDRS score at 3 years post-surgery. Conclusion: While not as effective as bilateral pallidal DBS, the benefits of a unilateral PVP are still substantial and sustained while also being less costly and resource expensive.},
year = {2025}
}
TY - JOUR T1 - Sustained Effect of Posteroventral Pallidotomy for X-Linked Dystonia Parkinsonism AU - Paulo Cataniag AU - Cid Czarina Diesta AU - Julie Anne Gamboa AU - Jean Quint Oropilla Y1 - 2025/03/18 PY - 2025 N1 - https://doi.org/10.11648/j.ijn.20250901.13 DO - 10.11648/j.ijn.20250901.13 T2 - International Journal of Neurosurgery JF - International Journal of Neurosurgery JO - International Journal of Neurosurgery SP - 17 EP - 22 PB - Science Publishing Group SN - 2640-1959 UR - https://doi.org/10.11648/j.ijn.20250901.13 AB - Background: X-linked dystonia parkinsonism (XDP, DYT3), a disease endemic to Panay Island in the Philippines, is a progressive adult-onset sex-linked neurodegenerative movement disorder with features of both dystonia and parkinsonism. Medical treatment and botulinum toxin injection (BTX) are of limited benefit. Deep brain stimulation (DBS) of the bilateral globus pallidus internus (GPi) is effective but is expensive and requires specialized equipment, training and after care. Posteroventral pallidotomy (PVP) is an older known ablative procedure which has successfully treated cervical and generalized dystonia, but has not been previously used for XDP. Case presentation: Two male adults with genetically-confirmed XDP, presented with progressive and severely disabling dystonias. The mean preoperative Burke-Fahn-Marsden Dystonia Rating Scale (BFMDRS) was 80.5. Both XDP patients underwent a unilateral posteroventral pallidotomy. In the first case, there was a 38.46% decrease in BFMDRS score at 2 weeks sustained to 41.66% decrease (compared to pre-op BFMDRS at 4 years post-surgery). In the second case, there was a 33.73% decrease in BFMDRS at 2 months post-op, and a decrease of 86.74% in BFMDRS score at 3 years post-surgery. Conclusion: While not as effective as bilateral pallidal DBS, the benefits of a unilateral PVP are still substantial and sustained while also being less costly and resource expensive. VL - 9 IS - 1 ER -
Section of Movement Disorders, Department of Neurosciences, MakatiMed Institute of Neurological, Neurosurgical and Behavioral Sciences (M.I.N.D.S.), Makati Medical Center, Makati City, Philippines; Department of Neurosciences, Baguio General Hospital and Medical Center, Baguio City, Philippines
Section of Movement Disorders, Department of Neurosciences, MakatiMed Institute of Neurological, Neurosurgical and Behavioral Sciences (M.I.N.D.S.), Makati Medical Center, Makati City, Philippines
Section of Movement Disorders, Department of Neurosciences, MakatiMed Institute of Neurological, Neurosurgical and Behavioral Sciences (M.I.N.D.S.), Makati Medical Center, Makati City, Philippines
Section of Movement Disorders, Department of Neurosciences, MakatiMed Institute of Neurological, Neurosurgical and Behavioral Sciences (M.I.N.D.S.), Makati Medical Center, Makati City, Philippines
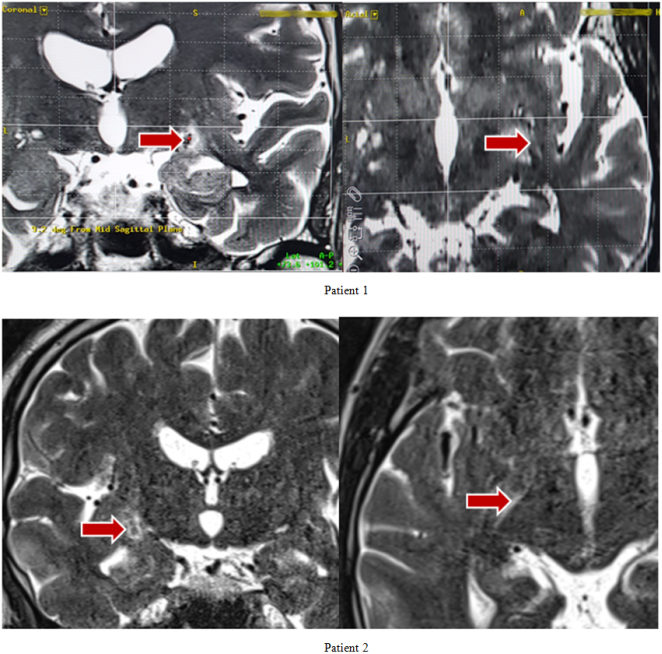
Figure 1. Coronal and axial views of post-pallidotomy MRI showing the lesions in the left and right GPi (red arrow) of Patients 1 and 2, respectively.
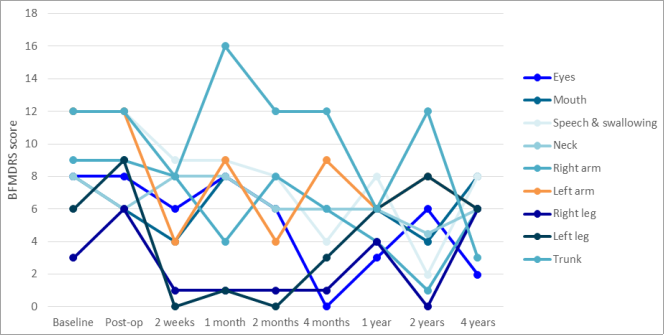
Figure 2. Regional changes in the BFMDRS of Patient 1 after left unilateral PVP.
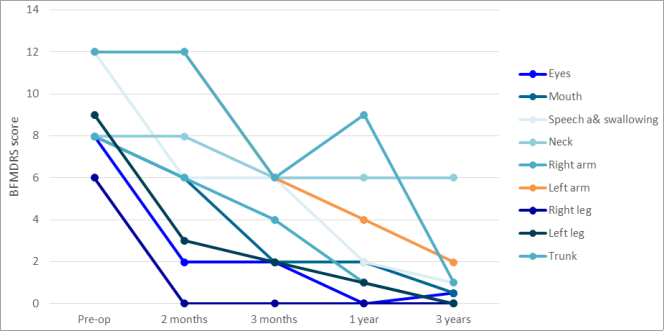
Figure 3. Regional changes in the BFMDRS of Patient 2 after right unilateral PVP.
Information

