Background and Aims: Acute appendicitis is an important and common problem world over. Complications of acute appendicitis are sometimes serious and even lethal. These complications can be presented by diagnosing appendicitis quickly and accurately allowing appendicectomy at earliest along with prevention of negative appendicectomy. Various scoring systems are in use to diagnose acute appendicitis. Nigam’s scoring system is compared here with other common scoring systems in relation to negative appendicectomy. The comparison of Nigam’s scoring system (NSS) and other scoring systems was done with our work on NSS and the work of other workers on other scoring systems. Methods: It is designed as a study of original study of scoring systems of acute appendicitis. Setting of this study was done in a primary care hospital with various specialties. 82 participants of this study attend emergency room and surgical OPDs with acute abdomen and referred to us on suspicious of acute appendicitis. Intervention was carried out as appendicectomy after thorough history taking, physical examinations and basic laboratory tests. Results: Showed high percentage of accuracy with zero incidence of negative appendicectomy. Conclusions: The comparative study of NSS with various other scoring system for diagnosing acute appendicitis shows that the rate of negative appendicectomy by using NSS is zero and no other scoring system compared here have shown this level.
| Published in | International Journal of Gastroenterology (Volume 9, Issue 2) |
| DOI | 10.11648/j.ijg.20250902.17 |
| Page(s) | 142-151 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Appendicitis Appendicectomy, Negative Appendicectomy, Scoring Systems
Variables | Score |
|---|---|
Symptoms | |
Migratory right iliac fossa pain | 1 |
Anorexia | 1 |
Nausea/vomiting | 1 |
Pain precedes vomiting | 1 |
Vomiting precedes pain | -1 |
Signs | |
Tenderness RIF (mild) | 2 |
Tenderness RIF (moderate) | 3 |
Tenderness RIF (severe) | 4 |
Rebound tenderness in RIF | 2 |
Guarding in RIF | 2 |
Elevated temperature | 1 |
Laboratory findings | |
Leucocytosis 10000-12000 per microliter of blood | 2 |
Leucocytosis 12000-15000 per microliter of blood | 3 |
Leucocytosis more than 15000 per microliter of blood | 4 |
Maximum score | 17 |
NSS | Interpretation |
|---|---|
6 and less than 6 score | Probably not acute appendicitis |
7 to 10 score | Probably acute appendicitis |
11 and more score | Confirmed diagnosis of acute appendicitis |
Age (Years) / Sex (Male or Female) / BMI | Number of patients | Percentage (%) of patients |
|---|---|---|
Age | ||
15 – 20 | 04 | 4.8% |
21 – 30 | 23 | 28.0% |
31 – 40 | 31 | 37.8% |
41 – 50 | 16 | 19.5% |
51 – 60 | 06 | 7.4% |
61 and above | 02 | 2.5% |
Male | 66 | 80.5% |
Female | 16 | 19.5% |
BMI – 18.5 to 25 | 76 | 92.7% |
BMI – 25 to 30 | 5 | 6.1% |
BMI – 35 and above | 1 | 1.2% |
Score | Number of patients | Percentage (%) of patients |
|---|---|---|
6 and less than 6 score | 5 | 6.1% |
7 – 10 score | 11 | 13.4% |
11 and above score | 66 | 80.5% |
Number of patients | Percentage (%) of patients | |
|---|---|---|
Negative appendicectomy (Histopathologically -ve, no appendicitis) | 0 | 0% |
Appendicitis (histopathology +ve) | 77 | 100% |
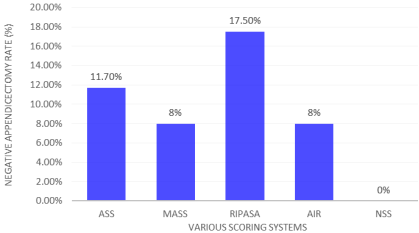
Scoring system | Total number of patients | Negative appendix on HPE number | Percentage |
|---|---|---|---|
Alvarado SS (Francisco et al [18] ) | 324 | 38 | 11.7% |
Modified Alvarado SS (Sulo et al [19] ) | 200 | 16 | 8% |
RIPASA SS (Singh A et al [ 4]) | 120 | 21 | 17.5% |
AIR SS (Suvarchala A et al [2 0]) | 100 | 8 | 8% |
NSS (Nigam VK and Nigam S [2 1]) | 82 | 0 | 0% |
AIR | Appendicitis Inflammatory Response |
BMI | Body Mass Index |
CRP | C-reactive Protein |
CT | Computed Tomography |
FN | False Negative |
FP | False Positive |
MAS | Modified Alvarado Score |
MASS | Modified Alvarado Scoring System |
MRI | Magnetic Resonance Imaging |
NPV | Negative Predictive Value |
NSS | Nigam’s Scoring System |
OPD | Outpatient Department |
PPV | Positive Predictive Value |
RIF | Right Iliac Fossa |
RIPASA | Raja Isteri Pengiran Anak Saleha Appendicitis |
TN | True Negative |
TP | True Positive |
USG | Ultrasonography |
| [1] | Khan MS, Chaudhary MBH, Shahzad N, Tariq M, Memon WA, Alvi AR, Risk of appendicitis in patients with incidentally discovered appendicoliths. J Surg Res. 2018 Jan; 221: 84-87. |
| [2] | Stringer MD. Acute appendicitis, J Paediatr Child Health. 2017 Nov; 53(11): 1071-10. |
| [3] | Addis DG, Shaffer N, Fowler BS, Tauxe RV. The epidemiology of appendicitis and appendectomy in the United States. Am J Epidemiol. 1990; 132(5): 910-925. |
| [4] | Singh A, Parihar US, Kumwat G, Samota R, Chaudhary R. To determine validation of RIPASA score in diagnosis of suspected acute appendicitis and histopathological correction with applicability of Indian population: A single institute study. Ind J Surg. 2018; 80(2): 113-117. |
| [5] | Shobha S, Sushrutha G, Goudar BV. Diagnostic Accuracy of the RIPASA score is suspected Acute Appendicitis in Adults: A Cross-sectional Study Comparing it with Histopathological Findings from Bagalkot, India. Int J Anat Radiol Surg 2023; 12(5): 5035-5038. |
| [6] | Jones MW, Lopez RA, Deppen JG. Appendicitis. StatPearls.ed.Treasure Island: StatPearls Publishing; 2020. |
| [7] | Schwerk WB, Wichtrup B, Rothmund M, Ruschoff J. Ultrasonography in the diagnosis of acute appendicitis: a prospective study. Gastroenterology. 1989; 97: 630-9. |
| [8] | Chishti MM, Surendran AK, Narayan JT. RIPASA and air scoring systems are superior to Alvarado scoring in acute appendicitis: diagnostic accuracy study. Ann Med Surg. 2020; 59: 138-42. |
| [9] | Seetahal SA, Bolorunduro OB, Sookdeo TC, Oyetunji TA, Greene WR, Frederick W, et al. Negative appendectomy: a 10-year review of a nationally representative sample. Am J Surg. 2011; 201(4): 433-7. |
| [10] | Shah AA, Al-Zoubi RM, Al-Qudimat AR, Almine Rijeb M, Kumar Ojha L, Abdulzem S, et al. Daytime versus night time laparoscopic appendectomy in term of complications and clinical outcomes. Heliyon. 2022; 8(12). |
| [11] | Alvarado A. A practical score for the early diagnostic of acute appendicitis. Annals of Emergency Medicine. 1986; 15(5): 557-564. |
| [12] | Kalan M, Talbot D, Cunliffe WJ, Rich AJ. Evaluations of the modified Alvarado score in the diagnosis of acute appendicitis. A perspective study. Annals of the Royal College of Surgeons of England 1994; 76: 418-419. |
| [13] | Alvarado A. Diagnostic Scores in Acute Appendicitis Nov 5; 2018, Current Issues in the Diagnostics and Treatment of Acute Appendicitis. Dmitry Victorovich Grabuzenko June 2018. |
| [14] | Fenyo G, Lindberg G, Blind P, Enochsson L, Oberga A. Diagnostic decision support in suspected acute appendicitis: validation of simplified scoring system. Eur J Surg Med. 1997; 11: 831-8. |
| [15] | Chong CF, Adi MI, Thien A, Sieyoi A, Mackie AJ, Tin AS, et al. Development of RIPASA score a new appendicitis scoring system for the diagnosis of acute appendicitis. Singapore Med J. 2010; 51(3): 220-5. |
| [16] | M Hassan, Sree GS, Vakka-lagadda NP etal. The RIPASA scoring system: A new era in appendicitis diagnosis. Ann Med Surg. 2022 Aug; 80: 104174. |
| [17] | Wani MM, Yousaf MN, Khan MA. Usefulness of the Alvarado scoring system with respect to age, sex and time of presentation with regression analysis of individual parameters. Internet J Surg. 2007; 11(2). |
| [18] | Francisco AR; Carlos ER, Julio CN et al. Assessment of negative appendectomy in acute appendicitis diagnosis 8% NAR with MASS. |
| [19] | (Sulo etal) Sulo, Suzan Safar, Al-Atrakchi, Ahmad H. The modified Alvarado score versus Alvarado Score in the Diagnosis of Acute Appendicitis. Med J Babglon. 2019 Jul-Sep; 16(3): 203-206. |
| [20] | Suvarchala A, Chandralekha J, Sudha YK, Praveena M, Samanth M. To Compare the Performance of AIR score in Reducing Negative Appendicectomies with Histopathological Correlation. Int. J Curr Phar Rev and Res 2025; 17(6): 745-752. |
| [21] | Nigam VK, Nigam S. Nigam’s Scoring System for acute appendicitis with high accuracy surpassing Alvarado Scoring System. Int Surg J 2022; 9(4): 835-840. |
| [22] | Andersson M, Andersson RE. The appendicitis inflammatory response score: a tool for the diagnosis of acute appendicitis that outperforms the Alvarado Score. World Journal of Surgery 2008 Aug; 32(8): 1843-1849. |
| [23] | deCastro SMM, Unlu C, Steller EP, van Wagensveld BA, Vrouenraels BC. Evaluation of the Appendicitis. Inflammatory Response Score for Patients with Acute Appendicitis. World Journal of Surgery 2012 Jul; 36(7): 1540-1545. |
| [24] | Kollar D, McCartan DP, Boorke M, Cross KS, Dowdall J. Predicting Acute Appendicitis? A comparison of the Alvarado Score, the Appendicitis Inflammatory Response Score and clinical assessment World Journal of Surgery. 2014 Sep; 39(1): 104-109. |
| [25] | Martinez JP. Evaluation and Management of the Patients with Abdominal Pain. In Mattu A, Goyal D (eds) Emergency Medicine. Malden, Massachusetts: Blackwell (BMJ Books) 2007; p 28. |
| [26] | Ohle R, O’Reilly F, O’Brien KK, Fahey T, Dimitrov BD. The Alvarado score for predicting acute appendicitis: a systematic review. BMC Med. 2011; 9(1): 139. |
| [27] | Deiters A, Drozd A, Parikh P, Markest R, Shein JK. Use of Alvarado score in Elderly Patients with complicated and uncomplicated Appendicitis. Am Surg. 2019; 85(4): 397-402. |
| [28] | Bai S, Hv S, Zhang Y, Guo S, Zhu R, Zeng J. The value of the Alvarado score for the diagnosis of acute appendicitis in children: A systematic review and meta-analysis. J Pediatr Surg. 2023; 58(10): 1886-1892. |
| [29] | Karakas SP, Guelfguat M, Leonidas JC, Springer S, Singh SP. Acute appendicitis in children: comparison of clinical diagnosis with ultrasound and CT imaging. Pediatr Radiol 2000; 30: 94-98. |
| [30] | Jose T, Rajesh PS. Appendicitis Inflammatory Response score in Comparison to Alvarado Score in Acute Appendicitis. Surg J (NY). 2001 Jul 19; 7(3): e127-e131. |
| [31] | Owen TD, Williams, H, Stiff G, Jenkinson LR, Rees BI: Evolution of the Alvarado score in acute appendicitis. JRSOC Med 1992; 85: 87-88. |
| [32] | Arain GM, Sohu KM, Ahmad E, Haidar W, Nagi SA: Role of Alvarado score in diagnosis of acute appendicitis. Pak J Surg 2001; 17: 41-46. |
| [33] | Khan I, urRehman A: Application of Alvarado scoring system in diagnosis of acute appendicitis. J Ayb Med Coll, Abottabad 2005; 17: 41-44. |
| [34] | Singh SK, Gupta S, Pargal P. Application of Alvarado scoring system in diagnosis of acute appendicitis JK Sci 2008; 10: 84-86. |
| [35] | Yuksel Y, Dine B, Yuksel D, etal. How reliable is the Alvarado score in acute appendicitis? Ulus Jravma Acil Cerrahi Derg. 2014; 20: 12-18. |
| [36] | Chong CF, Thien A, Mackie AJ et al. Comparison of RIPASA and Alvarado scores for the diagnosis of acute appendicitis Singapore Med J. 2011; 52: 340-345. |
| [37] | Lintula H, Pesonen E, Kokki H, et al. A diagnostic score for children with suspected appendicitis. Langenbecks Arch Surg. 2005; 390: 164-170. |
| [38] | Limpawattanasiri C. Alvarado score for the acute appendicitis in a provincial hospital. J Med Ass Thai. 2011; 94: 441-448. |
| [39] | Takada T, Yasuda H, Uchiyama K, Hasegawa H, Shikata JL. Ultrasonographic diagnosis of acute appendicitis in surgical indication Int Surg. 1986; 71(1): 9-13. |
| [40] | Mittal GS, Goel M, Singh J, Kshirsagar MB. Evaluation of modified Alvarado scoring system as a diagnostic tool for acute appendicitis and its correlation with Histo-pathological examination: A prospective study. IPJ Surg Allied Sci. 2025; 7(1): 35-39. |
| [41] | Favara G, Maugeri A, Barchitta M, Ventara A, Basile G, Agodi A. Comparison of RIPASA and Alvarado scores for risk assessment of acute appendicitis. A systematic review and meta analysis. PLoS ONE 17(9): e0275427. |
| [42] | Frountzas M, Sterigios K, Kopsini D, et al. Alvarado or RIPASA score for diagnosis of acute appendicitis? A meta-analysis of randomized trials. Int J Surg. 2018 Aug; 56: 307-314. |
| [43] | Chong CF, Thien A, Mackie AJ, Tin AS, Tripathi S, Ahmad MA, Tan LT, Daud FM, Tan C, Telisinghe PV, Ang SH. Evolution of RIPASA score – a new scoring system for the diagnosis of acute appendicitis. Brueni Int Med J. 2010; 6(1): 17-26. |
| [44] | Stephens PL, Mazzucco JJ. Comparison of ultrasound and the Alvarado score for the diagnosis of acute appendicitis. Conn Med J. 1999; 63: 137-140. |
| [45] | Lim J, Pang Q, Alexander R. One year negative appendicectomy rates at a district general hospital: a retrospective cohort study. Int J Surg. 2016; 31: 1-4. |
| [46] | Singh V, Jaiswal SS. Risk stratification using Appendicitis Inflammatory Response score, A useful tool to reduce negative appendicectomy rate: our experience. Int J Sci Res. 2019 May; 8(5): 2277-8179. |
| [47] | Scott AJ, Mason SE, Arunakirinathan M, Reissis Y, Kinross JM, Smith JJ. Risk stratification by the Appendicitis Inflammatory Response score to guide decision-making in patients with suspected appendicitis. Br J Surg. 2015; 102(5): 563-572. |
| [48] | Anderson M, Kolodziej B, Andersson RE. Randomized clinical trial of Appendicitis Inflammatory Response score-based management of patients with suspected appendicitis. Br. J Surg. 2017 Oct; 104(11): 1451-1461. |
| [49] | Nigam VK, Nigam S. Guidelines for handling neglected and complicated cases of acute appendicitis: A case scores in relation to Nigam’s scoring system (NSS). Int J Surg Sci. 2024; 8(4): 101-104 |
| [50] | Laxmandas VM, Karthik N, Joshi SS. A comparison Between Modified Alvarado Scoring System and Tzanaki’s Scoring System in Pre-Operative Evaluation of Acute Appendicitis, Operated and Confirmed with Hpr – An Observational Study. European J. Cardiovas Med. 2024 Jul-Aug; 14(4): 903-909. |
APA Style
Nigam, V. K., Nigam, S. (2025). Negative Appendicectomy – Relevance of Scoring Systems – Alvarado, Modified Alvarado, Ripasa, Air and Nigam’s Scoring System (NSS). International Journal of Gastroenterology, 9(2), 142-151. https://doi.org/10.11648/j.ijg.20250902.17
ACS Style
Nigam, V. K.; Nigam, S. Negative Appendicectomy – Relevance of Scoring Systems – Alvarado, Modified Alvarado, Ripasa, Air and Nigam’s Scoring System (NSS). Int. J. Gastroenterol. 2025, 9(2), 142-151. doi: 10.11648/j.ijg.20250902.17
@article{10.11648/j.ijg.20250902.17,
author = {Vinod Kumar Nigam and Siddharth Nigam},
title = {Negative Appendicectomy – Relevance of Scoring Systems – Alvarado, Modified Alvarado, Ripasa, Air and Nigam’s Scoring System (NSS)},
journal = {International Journal of Gastroenterology},
volume = {9},
number = {2},
pages = {142-151},
doi = {10.11648/j.ijg.20250902.17},
url = {https://doi.org/10.11648/j.ijg.20250902.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijg.20250902.17},
abstract = {Background and Aims: Acute appendicitis is an important and common problem world over. Complications of acute appendicitis are sometimes serious and even lethal. These complications can be presented by diagnosing appendicitis quickly and accurately allowing appendicectomy at earliest along with prevention of negative appendicectomy. Various scoring systems are in use to diagnose acute appendicitis. Nigam’s scoring system is compared here with other common scoring systems in relation to negative appendicectomy. The comparison of Nigam’s scoring system (NSS) and other scoring systems was done with our work on NSS and the work of other workers on other scoring systems. Methods: It is designed as a study of original study of scoring systems of acute appendicitis. Setting of this study was done in a primary care hospital with various specialties. 82 participants of this study attend emergency room and surgical OPDs with acute abdomen and referred to us on suspicious of acute appendicitis. Intervention was carried out as appendicectomy after thorough history taking, physical examinations and basic laboratory tests. Results: Showed high percentage of accuracy with zero incidence of negative appendicectomy. Conclusions: The comparative study of NSS with various other scoring system for diagnosing acute appendicitis shows that the rate of negative appendicectomy by using NSS is zero and no other scoring system compared here have shown this level.},
year = {2025}
}
TY - JOUR T1 - Negative Appendicectomy – Relevance of Scoring Systems – Alvarado, Modified Alvarado, Ripasa, Air and Nigam’s Scoring System (NSS) AU - Vinod Kumar Nigam AU - Siddharth Nigam Y1 - 2025/12/31 PY - 2025 N1 - https://doi.org/10.11648/j.ijg.20250902.17 DO - 10.11648/j.ijg.20250902.17 T2 - International Journal of Gastroenterology JF - International Journal of Gastroenterology JO - International Journal of Gastroenterology SP - 142 EP - 151 PB - Science Publishing Group SN - 2640-169X UR - https://doi.org/10.11648/j.ijg.20250902.17 AB - Background and Aims: Acute appendicitis is an important and common problem world over. Complications of acute appendicitis are sometimes serious and even lethal. These complications can be presented by diagnosing appendicitis quickly and accurately allowing appendicectomy at earliest along with prevention of negative appendicectomy. Various scoring systems are in use to diagnose acute appendicitis. Nigam’s scoring system is compared here with other common scoring systems in relation to negative appendicectomy. The comparison of Nigam’s scoring system (NSS) and other scoring systems was done with our work on NSS and the work of other workers on other scoring systems. Methods: It is designed as a study of original study of scoring systems of acute appendicitis. Setting of this study was done in a primary care hospital with various specialties. 82 participants of this study attend emergency room and surgical OPDs with acute abdomen and referred to us on suspicious of acute appendicitis. Intervention was carried out as appendicectomy after thorough history taking, physical examinations and basic laboratory tests. Results: Showed high percentage of accuracy with zero incidence of negative appendicectomy. Conclusions: The comparative study of NSS with various other scoring system for diagnosing acute appendicitis shows that the rate of negative appendicectomy by using NSS is zero and no other scoring system compared here have shown this level. VL - 9 IS - 2 ER -
Department of General and Minimal Access Surgery, Max Hospital, Gurugram, India
Department of General and Minimal Access Surgery, Max Hospital, Gurugram, India
Information