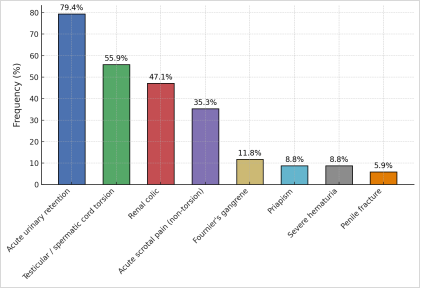
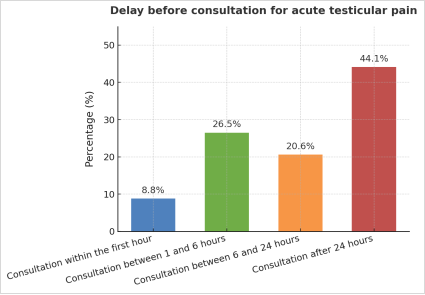
Urological emergencies account for a significant proportion of medical consultations, with acute scrotal pain and testicular torsion being common and high-risk causes. Rapid treatment is essential to preserve testicular function. In Chad, general practitioners are the first point of contact, but their practices had never been studied. Methods: A descriptive, cross-sectional study was conducted in July 2025 among 136 general practitioners in Chad working in public and mixed, urban and rural settings. Participants completed an online questionnaire on urological emergencies, their management, and complications. The analysis was performed using Excel and presented in proportions and absolute values. A total of 136 general practitioners participated in the survey, the majority of whom were men (87.5%) aged 28 to 44. More than half had been practicing for less than five years, and the majority worked in public facilities (65.4%) or in urban areas (53.7%). The most frequently reported urological emergencies were acute urinary retention (79.4%), acute scrotal pain (55.9%), and renal colic (47.1%). Almost all respondents (94.1%) reported seeing young patients with sudden unilateral scrotal pain; 20.6% encountered this at least once a month. The consultation time varied, with 8.8% of patients consulting within an hour and 20.6% after 24 hours. When faced with a painful scrotum without fever, 26.5% of doctors suspected testicular torsion, while 20.6% suggested epididymitis. The majority (97.1%) had already suspected or diagnosed testicular torsion. Management was mainly based on immediate referral to a specialized center (50%), sometimes combined with the prescription of analgesics (50%) or a scrotal ultrasound (14.7%). Testicular necrosis was the most feared complication (94.1%). No physician performed exploratory scrototomy. Chadian general practitioners recognize testicular torsion but have limited surgical skills and face prolonged delays in consultation, increasing the risk of testicular loss. Enhanced training, the development of standardized protocols, clinical simulation, and improved access to specialized centers are essential to optimize care and reduce morbidity.
| Published in | International Journal of Clinical Urology (Volume 10, Issue 1) |
| DOI | 10.11648/j.ijcu.20261001.25 |
| Page(s) | 85-91 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Urological Emergencies, Acute Scrotal Pain, Testicular Torsion, General Practitioners, Emergency Management, Chad
Characteristic | Category | Number (n) | Percentage (%) |
|---|---|---|---|
Sex | Male | 120 | 88 |
Female | 16 | 12 | |
Age (years) | Age moyen: 31 (extremes: 28 et 44) | ||
Work Experience (years) | 2 | 24 | 18 |
5 | 16 | 12 | |
Structure type | Public | 60 | 44 |
Public-private | 64 | 47 | |
Private | 12 | 9 | |
Exercise area | Urban | 106 | 78 |
Rurale | 30 | 22 | |
Variable | Category | Number (n) | Percentage (%) |
|---|---|---|---|
Diagnostic suspicion | Spermatic cord torsion | 72 | 52,9 |
Epididymitis / Orchiepididymitis | 28 | 20,6 | |
Others | 36 | 26,5 | |
Previous experience of testicular torsion | Yes | 132 | 97,1 |
No | 4 | 2,9 | |
Initial conduct | Prescription for painkillers | 48 | 35,3 |
Request for scrotal ultrasound | 20 | 14,7 | |
Immediate referral to a specialist center | 68 | 50 | |
Feared complications | Testicular necrosis | 128 | 94,1 |
Others | 8 | 5,9 |
| [1] | Kinnear N, Herath M, Barnett D, Hennessey D, Dobbins C, Sammour T, Moore J. A systematic review of dedicated models of care for emergency urological patients. Asian J Urol. 2021 Jul; 8(3): 315-323. |
| [2] | Talreja S, Banerjee I, Teli R, Agarwal N, Vyas N, Priyadarshi S, Yadav S, Tomar V. A Spectrum of Urological Emergency Reported at a Tertiary Care Teaching Hospital: An Experience. J Clin Diagn Res. 2015 Nov; 9(11): PC12-5. |
| [3] | Osmancevic A, Petersson A, Duverin A, Merzaai B, Hedlund E, Porras GM, Albinsson I, Al-Hadad J, Olsson S, Vestberg D, Sagen E, Abuhasanein S. Epidemiology and management of urological emergencies in a tertiary care setting in Scandinavia. Int J Emerg Med. 2025 Apr 15; 18(1): 79. |
| [4] | Diabaté I, Ondo CZ, Sow I, et al. Urgences urologiques au Centre Hospitalier de Louga, Sénégal: aspects épidémiologiques et évaluation de la prise en charge. African J Urol 21 (2015): 181-186. |
| [5] | Girgin R, Erdem K. Epidemiologic Analysis of Urological Cases Admitted to an Emergency Department of a Tertiary Care Center. J Urol Surg. 2020 Aug 20; 7(3): 227-231. |
| [6] | Boissier R, Savoie PH, Long JA. Épidémiologie des urgences urologiques en France [Epidemiology of urological emergencies in France]. Prog Urol. 2021 Nov; 31(15): 945-955. French. |
| [7] | Okpani C. P., and Kufre U. 2024. “Urological Emergencies; Spectrum of Cases Seen Over a Three Year Period in a Tertiary Care Teaching Hospital in West Africa”. Asian Journal of Research and Reports in Urology 7(1): 20-27. |
| [8] | Davis JE, Silverman M. Scrotal emergencies. Emerg Med Clin North Am. 2011 Aug; 29(3): 469-84. |
| [9] | Gordhan CG, Sadeghi-Nejad H. Scrotal pain: evaluation and management. Korean J Urol. 2015 Jan; 56(1): 3-11. |
| [10] | Burgher SW. Acute scrotal pain. Emerg Med Clin North Am. 1998 Nov; 16(4): 781-809, vi. |
| [11] | Long-Depaquit T, Chiron P, Bourgouin S, Hardy J, Deledalle FX, Laroche J, Molimard B, Savoie PH. Prise en charge de la torsion du testicule par un chirurgien généraliste isolé en Afrique [Management of testicular torsion by a general surgeon isolated in Africa]. Med Trop Sante Int. 2022 Apr 4; 2(2): mtsi.v2i2.2022.230. French. |
| [12] | Ngueringem, O., Mahamat, M. A., Abakar, M. N., & Gondjé, A. (2014). Épidémiologie des urgences urologiques en chirurgie pédiatrique à l’Hôpital de la Mère et de l’Enfant de N’Djamena. Revue scientifique du Tchad. |
| [13] | Diallo TO, Diabaté I, Barry M, Bah OR. Le profil des urgences urologiques dans un hôpital régional au Sénégal: étude rétrospective de 20 mois [Urological emergencies in a regional hospital in Senegal: a 20-month retrospective study]. Pan Afr Med J. 2022 Aug 22; 42: 302. French. |
| [14] | Owon’Abessolo, P. F., Mayopa, C. F., Mekeme, J., Fouda, J. C., Biyouma, M. D. C., Dongmo, G. Sosso, M. A. (2020). Urgences Urologiques: Aspects Épidémiologiques, Cliniques et Thérapeutiques à l’Hôpital Central de Yaoundé. HEALTH SCIENCES AND DISEASE, 21(8). |
| [15] | Vadandi V, Mahamat A, Temga O, Minguemadji A, Vounouzia B, Abdelmamoud C, et al. Urological Emergencies at the Abeche University Teaching Hospital: Epidemioclinicial Pattern and Management: Les Urgences Urologiques au Centre Hospitalier Universitaire d’Abeche: Profil Épidémiologique, Clinique et Thérapeutique. Health Sci. Dis. 2024 Apr. 28 [cited 2025 Jul. 29]; 25(5). Available from: |
| [16] | Kaboré, F. A., Zango, B., Yaméogo, C., Sanou, A., Kirakoya, B., & Traoré, S. S. (2011). Les torsions du cordon spermatique chez l’adulte au CHU Yalgado Ouédraogo de Ouagadougou. Basic and Clinical Andrology, 21(4), 254-259. |
| [17] | Obi AO, Okeke CJ, Ugwuidu EI. Acute testicular torsion: A critical analysis of presentation, management and outcome in southeast Nigeria. Niger J Clin Pract. 2020 Nov; 23(11): 1536-1541. |
| [18] | Rampaul MS, Hosking SW. Testicular torsion: most delay occurs outside hospital. Ann R Coll Surg Engl. 1998 May; 80(3): 169-72. |
| [19] | Kabore FA, Kabore KK, Kabore M, Kirakoya B, Yameogo C, Ky BD, Zango B. Predictive factors for orchiectomy in adult's spermatic cord torsion: a case-control study. Basic Clin Androl. 2021 Jan 21; 31(1): 2. |
| [20] | Diabaté I, Ouédraogo B, Thiam M. Les grosses bourses aiguës au centre hospitalier de Louga, Sénégal: aspects épidémiologiques, étiologiques et thérapeutiques [Acute scrotal swellings at Louga Regional Hospital, Senegal: epidemiologic, etiologic and therapeutic aspects]. Pan Afr Med J. 2016 Jul 12; 24: 214. French. |
| [21] | Gatti JM, Patrick Murphy J. Current management of the acute scrotum. Semin Pediatr Surg. 2007; 16(1): 58-63. |
| [22] | Nedjim, S. A., Biyouma, M. D. C., Mahamat, M. A. et al. Testicular torsion in Sub-Saharan Africa: a scoping review. Afr J Urol 29, 50 (2023). |
| [23] | Tree K, Buckland BC, Huynh R, Baskaranathan S, Fisher D, Indrajit B. Testicular Torsion: An Analysis of Rural Geography and Socioeconomic Status. Société Internationale d’Urologie Journal. 2023; 4(4): 257-264. |
| [24] |
Practical Urology for the Rural General Surgeon – CAGS. Available from:
https://cags-accg.ca/urology-program/ (accessed December 8, 2025). |
| [25] | Cummings JM, Boullier JA, Sekhon D, Bose K. Adult testicular tor- sion. J Urol 2002; 167: 2109–10. |
| [26] | Audenet F. Torsion du cordon spermatique et des annexes testiculaires: physiopathologie, diagnostic et principes du traitement. EMC Urologie 2012; 5(2): 1-7 [Article 18-622-A-10]. |
| [27] | Anderson MJ, Dunn JK, Lipshultz LI, Coburn M. Semen quality and endocrine parameters after acute testicular torsion. J Urol. 1992; 147: 1545–50. |
APA Style
Nedjim, S. A., Mahamat, M. A., Kouldjim, A., Allah-Syengar, N., Younous, S., et al. (2026). A Cross-sectional Survey of Urological Emergency Management by General Practitioners, with a Focus on Acute Scrotal Pain and Testicular Torsion in Chad. International Journal of Clinical Urology, 10(1), 85-91. https://doi.org/10.11648/j.ijcu.20261001.25
ACS Style
Nedjim, S. A.; Mahamat, M. A.; Kouldjim, A.; Allah-Syengar, N.; Younous, S., et al. A Cross-sectional Survey of Urological Emergency Management by General Practitioners, with a Focus on Acute Scrotal Pain and Testicular Torsion in Chad. Int. J. Clin. Urol. 2026, 10(1), 85-91. doi: 10.11648/j.ijcu.20261001.25
AMA Style
Nedjim SA, Mahamat MA, Kouldjim A, Allah-Syengar N, Younous S, et al. A Cross-sectional Survey of Urological Emergency Management by General Practitioners, with a Focus on Acute Scrotal Pain and Testicular Torsion in Chad. Int J Clin Urol. 2026;10(1):85-91. doi: 10.11648/j.ijcu.20261001.25
@article{10.11648/j.ijcu.20261001.25,
author = {Saleh Abdelkerim Nedjim and Mahamat Ali Mahamat and Adoumadji Kouldjim and Ndormadjita Allah-Syengar and Seid Younous and Sadié Ismael and Moussa Kalli and Choua Ouchemi},
title = {A Cross-sectional Survey of Urological Emergency Management by General Practitioners, with a Focus on Acute Scrotal Pain and Testicular Torsion in Chad},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {85-91},
doi = {10.11648/j.ijcu.20261001.25},
url = {https://doi.org/10.11648/j.ijcu.20261001.25},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.25},
abstract = {Urological emergencies account for a significant proportion of medical consultations, with acute scrotal pain and testicular torsion being common and high-risk causes. Rapid treatment is essential to preserve testicular function. In Chad, general practitioners are the first point of contact, but their practices had never been studied. Methods: A descriptive, cross-sectional study was conducted in July 2025 among 136 general practitioners in Chad working in public and mixed, urban and rural settings. Participants completed an online questionnaire on urological emergencies, their management, and complications. The analysis was performed using Excel and presented in proportions and absolute values. A total of 136 general practitioners participated in the survey, the majority of whom were men (87.5%) aged 28 to 44. More than half had been practicing for less than five years, and the majority worked in public facilities (65.4%) or in urban areas (53.7%). The most frequently reported urological emergencies were acute urinary retention (79.4%), acute scrotal pain (55.9%), and renal colic (47.1%). Almost all respondents (94.1%) reported seeing young patients with sudden unilateral scrotal pain; 20.6% encountered this at least once a month. The consultation time varied, with 8.8% of patients consulting within an hour and 20.6% after 24 hours. When faced with a painful scrotum without fever, 26.5% of doctors suspected testicular torsion, while 20.6% suggested epididymitis. The majority (97.1%) had already suspected or diagnosed testicular torsion. Management was mainly based on immediate referral to a specialized center (50%), sometimes combined with the prescription of analgesics (50%) or a scrotal ultrasound (14.7%). Testicular necrosis was the most feared complication (94.1%). No physician performed exploratory scrototomy. Chadian general practitioners recognize testicular torsion but have limited surgical skills and face prolonged delays in consultation, increasing the risk of testicular loss. Enhanced training, the development of standardized protocols, clinical simulation, and improved access to specialized centers are essential to optimize care and reduce morbidity.},
year = {2026}
}
TY - JOUR T1 - A Cross-sectional Survey of Urological Emergency Management by General Practitioners, with a Focus on Acute Scrotal Pain and Testicular Torsion in Chad AU - Saleh Abdelkerim Nedjim AU - Mahamat Ali Mahamat AU - Adoumadji Kouldjim AU - Ndormadjita Allah-Syengar AU - Seid Younous AU - Sadié Ismael AU - Moussa Kalli AU - Choua Ouchemi Y1 - 2026/05/12 PY - 2026 N1 - https://doi.org/10.11648/j.ijcu.20261001.25 DO - 10.11648/j.ijcu.20261001.25 T2 - International Journal of Clinical Urology JF - International Journal of Clinical Urology JO - International Journal of Clinical Urology SP - 85 EP - 91 PB - Science Publishing Group SN - 2640-1355 UR - https://doi.org/10.11648/j.ijcu.20261001.25 AB - Urological emergencies account for a significant proportion of medical consultations, with acute scrotal pain and testicular torsion being common and high-risk causes. Rapid treatment is essential to preserve testicular function. In Chad, general practitioners are the first point of contact, but their practices had never been studied. Methods: A descriptive, cross-sectional study was conducted in July 2025 among 136 general practitioners in Chad working in public and mixed, urban and rural settings. Participants completed an online questionnaire on urological emergencies, their management, and complications. The analysis was performed using Excel and presented in proportions and absolute values. A total of 136 general practitioners participated in the survey, the majority of whom were men (87.5%) aged 28 to 44. More than half had been practicing for less than five years, and the majority worked in public facilities (65.4%) or in urban areas (53.7%). The most frequently reported urological emergencies were acute urinary retention (79.4%), acute scrotal pain (55.9%), and renal colic (47.1%). Almost all respondents (94.1%) reported seeing young patients with sudden unilateral scrotal pain; 20.6% encountered this at least once a month. The consultation time varied, with 8.8% of patients consulting within an hour and 20.6% after 24 hours. When faced with a painful scrotum without fever, 26.5% of doctors suspected testicular torsion, while 20.6% suggested epididymitis. The majority (97.1%) had already suspected or diagnosed testicular torsion. Management was mainly based on immediate referral to a specialized center (50%), sometimes combined with the prescription of analgesics (50%) or a scrotal ultrasound (14.7%). Testicular necrosis was the most feared complication (94.1%). No physician performed exploratory scrototomy. Chadian general practitioners recognize testicular torsion but have limited surgical skills and face prolonged delays in consultation, increasing the risk of testicular loss. Enhanced training, the development of standardized protocols, clinical simulation, and improved access to specialized centers are essential to optimize care and reduce morbidity. VL - 10 IS - 1 ER -
Faculty of Medicine, Adam Barka University of Abeche, Abeche, Chad
Information