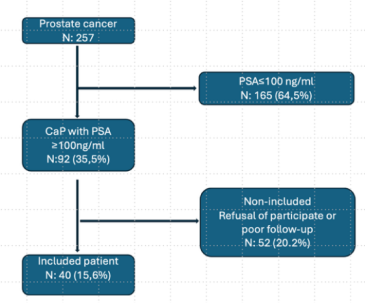
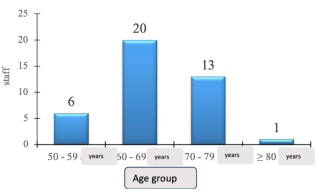
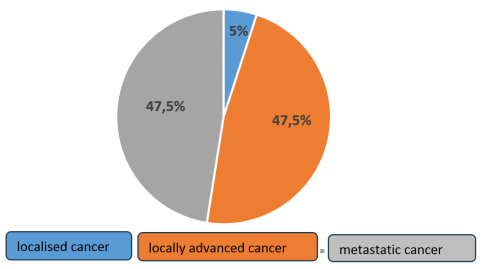
Objective: To study the epidemiological, diagnostic, therapeutic and progressive aspects of prostate cancer with PSA ≥ 100 ng/ml at Owendo University Hospital. Methodology: Prospective, descriptive study with progressive inclusion of cases, conducted from November 2021 to October 2024. It involved 40 patients admitted to the general surgery department of Owendo University Hospital. The variables studied were age, medical history, comorbidities, reason for consultation, duration of symptoms, PSA kinetics, nadir time, castration resistance time, Gleason score and duration of treatment. Results: The prevalence was 35.5% of CaP cases. The average age was 66.9 ± 6.1 years. All patients had lower urinary tract symptoms and 95% of cases had a pathological prostate on digital rectal examination. Stages T2 and T3 accounted for 32.5% and 55% of cases. Forty-seven per cent of cancers were low grade. CT-TAP revealed 47.5% of metastatic cancers with 45.0% of bone metastases. Treatment consisted of first-generation hormone therapy, chemotherapy, and radical prostatectomy in 95%, 20%, and 5% of cases, respectively. Symptoms regressed in 60% of cases, and the nadir time was 10.9 months. During the 24-month follow-up period, 11 patients achieved a PSA level below 4 ng/ml and 6 cases showed resistance to castration after an average of 15 months of treatment. The mortality rate was 20%. Conclusion: Prostate cancer with PSA levels above 100 ng/ml is common in our country. A PSA level ≥100 ng/ml does not necessarily indicate high-grade prostate cancer, let alone metastasis. Treatment with hormone therapy and even definitive local treatment allows for effective control of the disease.
| Published in | International Journal of Clinical Urology (Volume 10, Issue 1) |
| DOI | 10.11648/j.ijcu.20261001.23 |
| Page(s) | 71-76 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Prostate Cancer, High PSA, Hormone Therapy, Mortality
Reason for consultation | Staff | Purcentage |
|---|---|---|
Dysuria | 13 | 32,5 |
Pollakiuria | 7 | 17,5 |
Urunary retention | 7 | 17,5 |
Low back pain | 6 | 15 |
Paraplegia | 3 | 7,5 |
deterioration in overall health | 2 | 5 |
Hematuria | 2 | 5 |
Total | 40 | 100 |
initial PSA level. | Staff | Purcentage |
|---|---|---|
100 à 500 | 24 | 60 |
501 à 1000 | 3 | 7,5 |
1001 à 1500 | 3 | 7,5 |
1501 à 2000 | 5 | 12,5 |
>2000 | 5 | 12,5 |
Total | 40 | 100 |
CT-TAP | Chest, Abdomen and Pelvis CT Scan |
PSA | Protate Specific Antigen |
MRI | Magnetic Resonance Imaging |
CaP | Cancer Prostate |
HBP | High Blood Pressure |
| [1] | Bray F, Laversanne M, Sung H et al. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2024; 74(3): 229-63. |
| [2] | Ntama A, Owon’Abessolo P, Sango AJF et al. Epidemiology and Diagnosis of Prostate Cancer in the City of Douala (Cameroon). Health Sci. Dis. 2023; 24(7): 33-38. |
| [3] | Salmi F, Jouhadi H. A study of the epidemiological profile of prostate cancer in a Moroccan population. Journal of Epidemiology and Public Health. 2018; 66(3): 157-8. |
| [4] | Mbethe D, Mougougou A, Ndang Ngou Milama S et al. Incidence of Prostate Cancer in Gabon: Blue November 2020 Cases. Health Res. Afr. 2024; 2(6): 38-42. |
| [5] | Darré T, Djiwa T, Kpatcha TM et al. Prostate cancers in men under the age of 50: about a series in Togo, Sub-Saharan Africa. BMC Cancer. 2022; 22(1): 1341-6. |
| [6] | Mougougou A, Massande Mouyendi J, Ndang Ngou Milama S et al Prostate cancer in young patients at the urology-andrology department of Aristide le Dantec University Hospital: 12 cases. Bull Med Owendo. 2019; 17(46) 17-24. |
| [7] | Mougola P, Kumbading G, Montcho CJ et al. Prostate Specific Antigen and the Risk of Prostate Cancer on Prostate Biopsies in Libreville, 2018-2020. Health Sci. Dis. 2023 (24): 28-34. |
| [8] | Ndoye M, Niang L, Gandaho KI et al. Advanced prostate cancer in Senegal. Diagnostic aspects at Grand Yoff Hospital. Prog Urol. 2014; 24(5): 271-275. |
| [9] | Jang JY, Kim YS. Is prostate biopsy essential to diagnose prostate cancer in the older patient with extremely high prostate-specific antigen? Kor J Urol. 2012; 53: 82. |
| [10] | Izumi K, Lin WJ, Miyamoto H et al. Outcomes and predictive factors in patients with prostate cancer presenting with extremely high prostate-specific antigen levels. J Cancer Res Clin Oncol. 2014; 140(8): 1413 – 9. |
| [11] | Lillard JW Jr, Moses KA, Mahal BA, George DJ et al. Racial disparities in Black men with prostate cancer: A literature review. Cancer. 2022; 128(21): 3787-95. |
| [12] | Tean O, Bras Da Silva C, Vega Toro P et al. Epidemiology of prostate cancer in French Guiana – Preliminary data. Prog Urol. 2020; 30: 456-62. |
| [13] | Huang CY, Chen CH. Clinical characteristics and survival outcomes in patients with a high PSA and non-metastatic prostate cancer. Journal of the Formosan Medical Association. 2022; 121: 181-6. |
| [14] | Ang M, Rajcic B, Foreman D et al. Men presenting with prostate-specific antigen (PSA) values of over 100 ng/mL. BJU Int. 2016; 117 Suppl 4: 68-75. |
| [15] | Ngoungou EB, Aboyans V, Kouna P et al. Prevalence of cardiovascular disease in Gabon: a population study. Arch Cardiovasc Dis. 2012; 105(2): 77-83. |
| [16] | Wingo PA, Tong T, Bolden S. Cancer statistics. CA Cancer J Clin. 1995; 45(1): 8-30. |
| [17] | Koo KC, Park SU, Kim KH et al. Predictors of survival in prostate cancer patients with bone metastasis and extremely high prostate-specific antigen levels. Prostate Int. 2015; 3(1): 10-5. |
| [18] | Tengue K, Kpatcha T. M., Botchoa G et al. Epidemiological, diagnostic, therapeutic and prognostic profile of prostate cancer in Togo. African Journal of Urology. 2016; 22: 76-82. |
APA Style
Adrien, M., Dimitri, M., Felicite, A. M. E., Steevy, N. N. M., Ted, B. I. I., et al. (2026). Epidemiological, Diagnostic, Therapeutic and Evolutionary Aspects of Prostate Cancer with PSA Greater Than 100ng/ml. International Journal of Clinical Urology, 10(1), 71-76. https://doi.org/10.11648/j.ijcu.20261001.23
ACS Style
Adrien, M.; Dimitri, M.; Felicite, A. M. E.; Steevy, N. N. M.; Ted, B. I. I., et al. Epidemiological, Diagnostic, Therapeutic and Evolutionary Aspects of Prostate Cancer with PSA Greater Than 100ng/ml. Int. J. Clin. Urol. 2026, 10(1), 71-76. doi: 10.11648/j.ijcu.20261001.23
@article{10.11648/j.ijcu.20261001.23,
author = {Mougougou Adrien and Mbethe Dimitri and Adande Menest Elvire Felicite and Ndang Ngou Milama Steevy and Bissiriou Isoudine Idoukou Ted and Mbadinga Nzamba Ghislain and Nzalimbaninenou Mboula Pauline and Allogho Mbouye Gloire and Nguyen Akendengue Leslie},
title = {Epidemiological, Diagnostic, Therapeutic and Evolutionary Aspects of Prostate Cancer with PSA Greater Than 100ng/ml},
journal = {International Journal of Clinical Urology},
volume = {10},
number = {1},
pages = {71-76},
doi = {10.11648/j.ijcu.20261001.23},
url = {https://doi.org/10.11648/j.ijcu.20261001.23},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20261001.23},
abstract = {Objective: To study the epidemiological, diagnostic, therapeutic and progressive aspects of prostate cancer with PSA ≥ 100 ng/ml at Owendo University Hospital. Methodology: Prospective, descriptive study with progressive inclusion of cases, conducted from November 2021 to October 2024. It involved 40 patients admitted to the general surgery department of Owendo University Hospital. The variables studied were age, medical history, comorbidities, reason for consultation, duration of symptoms, PSA kinetics, nadir time, castration resistance time, Gleason score and duration of treatment. Results: The prevalence was 35.5% of CaP cases. The average age was 66.9 ± 6.1 years. All patients had lower urinary tract symptoms and 95% of cases had a pathological prostate on digital rectal examination. Stages T2 and T3 accounted for 32.5% and 55% of cases. Forty-seven per cent of cancers were low grade. CT-TAP revealed 47.5% of metastatic cancers with 45.0% of bone metastases. Treatment consisted of first-generation hormone therapy, chemotherapy, and radical prostatectomy in 95%, 20%, and 5% of cases, respectively. Symptoms regressed in 60% of cases, and the nadir time was 10.9 months. During the 24-month follow-up period, 11 patients achieved a PSA level below 4 ng/ml and 6 cases showed resistance to castration after an average of 15 months of treatment. The mortality rate was 20%. Conclusion: Prostate cancer with PSA levels above 100 ng/ml is common in our country. A PSA level ≥100 ng/ml does not necessarily indicate high-grade prostate cancer, let alone metastasis. Treatment with hormone therapy and even definitive local treatment allows for effective control of the disease.},
year = {2026}
}
TY - JOUR T1 - Epidemiological, Diagnostic, Therapeutic and Evolutionary Aspects of Prostate Cancer with PSA Greater Than 100ng/ml AU - Mougougou Adrien AU - Mbethe Dimitri AU - Adande Menest Elvire Felicite AU - Ndang Ngou Milama Steevy AU - Bissiriou Isoudine Idoukou Ted AU - Mbadinga Nzamba Ghislain AU - Nzalimbaninenou Mboula Pauline AU - Allogho Mbouye Gloire AU - Nguyen Akendengue Leslie Y1 - 2026/04/07 PY - 2026 N1 - https://doi.org/10.11648/j.ijcu.20261001.23 DO - 10.11648/j.ijcu.20261001.23 T2 - International Journal of Clinical Urology JF - International Journal of Clinical Urology JO - International Journal of Clinical Urology SP - 71 EP - 76 PB - Science Publishing Group SN - 2640-1355 UR - https://doi.org/10.11648/j.ijcu.20261001.23 AB - Objective: To study the epidemiological, diagnostic, therapeutic and progressive aspects of prostate cancer with PSA ≥ 100 ng/ml at Owendo University Hospital. Methodology: Prospective, descriptive study with progressive inclusion of cases, conducted from November 2021 to October 2024. It involved 40 patients admitted to the general surgery department of Owendo University Hospital. The variables studied were age, medical history, comorbidities, reason for consultation, duration of symptoms, PSA kinetics, nadir time, castration resistance time, Gleason score and duration of treatment. Results: The prevalence was 35.5% of CaP cases. The average age was 66.9 ± 6.1 years. All patients had lower urinary tract symptoms and 95% of cases had a pathological prostate on digital rectal examination. Stages T2 and T3 accounted for 32.5% and 55% of cases. Forty-seven per cent of cancers were low grade. CT-TAP revealed 47.5% of metastatic cancers with 45.0% of bone metastases. Treatment consisted of first-generation hormone therapy, chemotherapy, and radical prostatectomy in 95%, 20%, and 5% of cases, respectively. Symptoms regressed in 60% of cases, and the nadir time was 10.9 months. During the 24-month follow-up period, 11 patients achieved a PSA level below 4 ng/ml and 6 cases showed resistance to castration after an average of 15 months of treatment. The mortality rate was 20%. Conclusion: Prostate cancer with PSA levels above 100 ng/ml is common in our country. A PSA level ≥100 ng/ml does not necessarily indicate high-grade prostate cancer, let alone metastasis. Treatment with hormone therapy and even definitive local treatment allows for effective control of the disease. VL - 10 IS - 1 ER -
Owendo University Hospital Center, University of Health Science, Owendo, Gabon
Information