Introduction: Penile gangrene is rare and can pose difficulties in management. Although the penis have a rich arterial supply, they are basically end arteries and arterial occlusion will invariably cause distal necrosis similar to ischemic gangrene often noted in the digits of extremities. It is estimated that around 8–18% of cancer patients have diabetes. Diabetes and multiple myeloma are two overwhelming conditions for both patients and clinicians. In this paper we described our experience with managing penile gangrene in a diabetic patient with multiple myeloma on chemotherapy. Our patient had partial penectomy with refashioning of the penile stump and neo-meatus. Case report: He is OND, a 54 year old male patient who presented to our facility with difficulty in passing urine and progressive discoloration of glans penis for a week duration. These symptoms were insidious in onset and progressed to involve the penis up to the mid penile shaft. He is a known type 2 diabetic patient with poor control and was recently managed for diabetic ketoacidosis (DKA) by our endocrinologist. He was also diagnosed of multiple myeloma 6 weeks prior to presentation and had commenced his chemotherapy protocol. External genitalia revealed penile swelling with features of gangrene. He was counseled on partial penile amputation with refashioning of penile stump and neo meatus. The immediate postoperative condition was satisfactory. The histological diagnosis was that of benign calcinosis to rule out metastatic calcifications. Conclusion: Penile gangrene is a hallmark of severe systemic vascular disease. It is rare in clinical practice. Early presentation can result in penile salvage. However with late presentation partial or total penile loss becomes inevitable.
| Published in | International Journal of Clinical Urology (Volume 9, Issue 1) |
| DOI | 10.11648/j.ijcu.20250901.19 |
| Page(s) | 55-61 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Penile, Gangrene, Multiple Myeloma, Diabetes Mellitus, Fournier's Gangrene, Benign Calcinosis, Phalloplasty, Neo-Meatus
QoL | Quality of Life |
DM | Diabetes Mellitus |
DKA | Diabetic Ketoacidosis |
LUTS | Lower Urinary Tract Symptoms |
| [1] | Ntia IO, Mungadi IA. The Pattern of Penile Gangrene in Sokoto, Nigeria. Afr J Urol. 2007; 13(4): 255-261. |
| [2] | Ashutosh T, Neerja P, Majhail S. Fournier’s Gangrene of the Penis: A Rare Entity. J Cutan Aesthet Surg. 2010; 3(1): 41–44. |
| [3] | Khanh NP, Mitchell HS, charles AS. Severe Gangrene at the Glans Penis Requiring Penectomy as the First Major Complication of Buerger’s Disease. Am J Clin Exp Urol. 2016; 4(1): 9–11. |
| [4] | Vijayan P. Gangrene of the Penis in a Diabetic Male with Multiple Amputations and Follow up. Indian J Urol. 2009 Jan-Mar; 25(1): 123–125. |
| [5] | Vikas KP, Ravimohan SM, Sudheer KD, Kim V, Girdhar SB. Priapism with Penile Gangrene: An Unusual Presentation of Multiple Myeloma. Indian J Urol. 2017 Jul-Sep; 33(3): 251–252. |
| [6] | Ogbonna C. N. Management of Multiple Myeloma in Developing Countries. IntechOpen. 2018: 61996. |
| [7] | Zeinab AI, Mira SZ, Sami TA. Multiple Myeloma and Diabetes. ISRN Endocrinol. 2011 Nov 17; 2011: 815013. |
| [8] | Urvi AS, Erin M, Andriy D, Yuanhui H, Sham M, Carlyn R et al. Prevalence and Impact of Diabetes on Survival of Patients with Multiple Myeloma in Different Racial Groups. Blood Adv. 2024; 8(1): 236–247. |
| [9] | Mohamed AA, Yasar AA, Abubaker I. Clinical Challenges: Myeloma and Concomitant Type 2 Diabetes. South Asian J Cancer. 2013 Oct-Dec; 2(4): 290–295. |
| [10] | Odunukwe NN, Madu JA, Nnodu OE, Okocha OE, Akingbola TS, Asuquo IM et al. Multiple Myeloma in Nigeria: A Multi-centre Epidemiological and Biomedical Study. PAM J. 2015; 22: 292. |
| [11] | Abdulla MC, Nair LK, Narayan R, Das A. Multiple Myeloma Presenting as Extensive Limb Gangrene. J. Appl. Hematol. 2014 Jul-Sep; 5(3): 107-110. |
| [12] | Nwabuko CC, Igbigbi EE, Chukwuonye II, Nnoli MA. Multiple Myeloma in Niger Delta, Nigeria: Complications and Outcome of Palliative Interventions. CMAR. 2017; 9: 189-196. |
| [13] | Weiner DM, Lowe FC. Surgical Management of Ischemic Penile Gangrene in Diabetics with End Stage Atherosclerosis. J Urol. 1996; 155: 926–929. |
| [14] | Suleiman A, Michael AN, Helina KT, Nahom GM, Yishak A, Mesfin TW. Management of Total Penile Amputation Following Circumcision in a Resource Limited Setting: A Case Report. J. Pediatr. Surg. Case Rep. 2025; 113: 102939. |
| [15] | Olaomi OO. Penile Gangrene Following Cavernoglandular Shunt for Priapism: Case Report. Nig. J. of Surgical Research. 2002; 4(3-4): 112-114. |
| [16] | I-Ni Chiang, Shang-Jen Chang, Yuh-Chen Kuo, Shih-Ping Liu, Hong-Jeng Yu, Ju-Ton Hsieh, Management of Ischemic Penile Gangrene: Prompt Partial Penectomy and Other Treatment Options, The Journal of Sexual Medicine, Volume 5, Issue 11, November 2008, Pages 2725–2733. |
| [17] | Benjamin E Ayres. Psychosocial Impact of Penile Cancer: An Unmet Need. Urol Clin North Am 2024 Aug; 51(3): 327-334. |
APA Style
Kenenna, O., Christopher, O., E, M. F., Chinemezu, A., Emeka, O. (2025). Penile Gangrene Leading to Penile Amputation: An Unusual Complication of Diabetes in a Patient with Multiple Myeloma. International Journal of Clinical Urology, 9(1), 55-61. https://doi.org/10.11648/j.ijcu.20250901.19
ACS Style
Kenenna, O.; Christopher, O.; E, M. F.; Chinemezu, A.; Emeka, O. Penile Gangrene Leading to Penile Amputation: An Unusual Complication of Diabetes in a Patient with Multiple Myeloma. Int. J. Clin. Urol. 2025, 9(1), 55-61. doi: 10.11648/j.ijcu.20250901.19
@article{10.11648/j.ijcu.20250901.19,
author = {Obiatuegwu Kenenna and Otabor Christopher and Magnus Felix E and Awuzie Chinemezu and Okonta Emeka},
title = {Penile Gangrene Leading to Penile Amputation: An Unusual Complication of Diabetes in a Patient with Multiple Myeloma
},
journal = {International Journal of Clinical Urology},
volume = {9},
number = {1},
pages = {55-61},
doi = {10.11648/j.ijcu.20250901.19},
url = {https://doi.org/10.11648/j.ijcu.20250901.19},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijcu.20250901.19},
abstract = {Introduction: Penile gangrene is rare and can pose difficulties in management. Although the penis have a rich arterial supply, they are basically end arteries and arterial occlusion will invariably cause distal necrosis similar to ischemic gangrene often noted in the digits of extremities. It is estimated that around 8–18% of cancer patients have diabetes. Diabetes and multiple myeloma are two overwhelming conditions for both patients and clinicians. In this paper we described our experience with managing penile gangrene in a diabetic patient with multiple myeloma on chemotherapy. Our patient had partial penectomy with refashioning of the penile stump and neo-meatus. Case report: He is OND, a 54 year old male patient who presented to our facility with difficulty in passing urine and progressive discoloration of glans penis for a week duration. These symptoms were insidious in onset and progressed to involve the penis up to the mid penile shaft. He is a known type 2 diabetic patient with poor control and was recently managed for diabetic ketoacidosis (DKA) by our endocrinologist. He was also diagnosed of multiple myeloma 6 weeks prior to presentation and had commenced his chemotherapy protocol. External genitalia revealed penile swelling with features of gangrene. He was counseled on partial penile amputation with refashioning of penile stump and neo meatus. The immediate postoperative condition was satisfactory. The histological diagnosis was that of benign calcinosis to rule out metastatic calcifications. Conclusion: Penile gangrene is a hallmark of severe systemic vascular disease. It is rare in clinical practice. Early presentation can result in penile salvage. However with late presentation partial or total penile loss becomes inevitable.
},
year = {2025}
}
TY - JOUR T1 - Penile Gangrene Leading to Penile Amputation: An Unusual Complication of Diabetes in a Patient with Multiple Myeloma AU - Obiatuegwu Kenenna AU - Otabor Christopher AU - Magnus Felix E AU - Awuzie Chinemezu AU - Okonta Emeka Y1 - 2025/03/18 PY - 2025 N1 - https://doi.org/10.11648/j.ijcu.20250901.19 DO - 10.11648/j.ijcu.20250901.19 T2 - International Journal of Clinical Urology JF - International Journal of Clinical Urology JO - International Journal of Clinical Urology SP - 55 EP - 61 PB - Science Publishing Group SN - 2640-1355 UR - https://doi.org/10.11648/j.ijcu.20250901.19 AB - Introduction: Penile gangrene is rare and can pose difficulties in management. Although the penis have a rich arterial supply, they are basically end arteries and arterial occlusion will invariably cause distal necrosis similar to ischemic gangrene often noted in the digits of extremities. It is estimated that around 8–18% of cancer patients have diabetes. Diabetes and multiple myeloma are two overwhelming conditions for both patients and clinicians. In this paper we described our experience with managing penile gangrene in a diabetic patient with multiple myeloma on chemotherapy. Our patient had partial penectomy with refashioning of the penile stump and neo-meatus. Case report: He is OND, a 54 year old male patient who presented to our facility with difficulty in passing urine and progressive discoloration of glans penis for a week duration. These symptoms were insidious in onset and progressed to involve the penis up to the mid penile shaft. He is a known type 2 diabetic patient with poor control and was recently managed for diabetic ketoacidosis (DKA) by our endocrinologist. He was also diagnosed of multiple myeloma 6 weeks prior to presentation and had commenced his chemotherapy protocol. External genitalia revealed penile swelling with features of gangrene. He was counseled on partial penile amputation with refashioning of penile stump and neo meatus. The immediate postoperative condition was satisfactory. The histological diagnosis was that of benign calcinosis to rule out metastatic calcifications. Conclusion: Penile gangrene is a hallmark of severe systemic vascular disease. It is rare in clinical practice. Early presentation can result in penile salvage. However with late presentation partial or total penile loss becomes inevitable. VL - 9 IS - 1 ER -
Department of Surgery, Alliance Hospital and Services Ltd, Abuja, Nigeria; Department of Surgery, Baze University, Abuja, Nigeria; Division of Urology, Department of Surgery, Federal Medical Center, Abuja, Nigeria
Department of Surgery, Alliance Hospital and Services Ltd, Abuja, Nigeria
Department of Surgery, Alliance Hospital and Services Ltd, Abuja, Nigeria; Division of Urology, Department of Surgery, Chivar Specialist Hospital and Urology Center, Abuja, Nigeria
Division of Urology, Department of Surgery, Federal Medical Center, Abuja, Nigeria
Department of Surgery, Alliance Hospital and Services Ltd, Abuja, Nigeria

Figure 1. Showing obvious macroscopic death of distal penis and glans.

Figure 2. Firm proximal penile shaft.

Figure 3. Patient draped to expose the surgical field.

Figure 4. Showing the ventral part of the penis with obvious urethral meatal stenosis.

Figure 5. Incision placed 1cm proximal to the gangrenous part and extended in an oblique manner toward ventral penis.

Figure 6. Prior to placement of incision we applied a tourniquet to reduce bleeding. This diagram also shows dead distal urethral covered with slough.
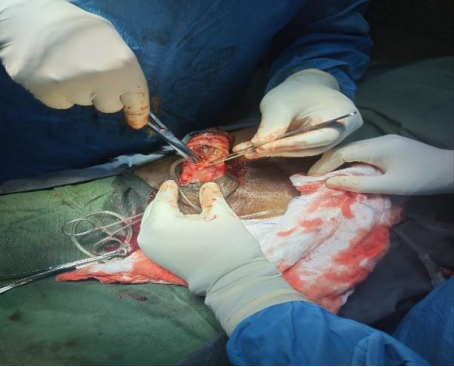
Figure 7. Incision extended obliquely and proximally to the viable part of the mid urethra.

Figure 8. Penile skin degloved, viable urethra stump dissected and a feeding tube advanced to ascertain patency.

Figure 9. Partial penectomy done with the viable corpora bodies and urethral exposed.

Figure 10. Gangrenous distal penis that was sent for histological analysis.
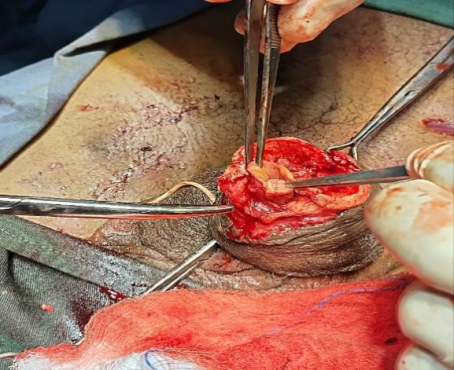
Figure 11. Amputated stump with bleeding edges and properly dissected urethra which was subsequently everted to prevent stenosis.
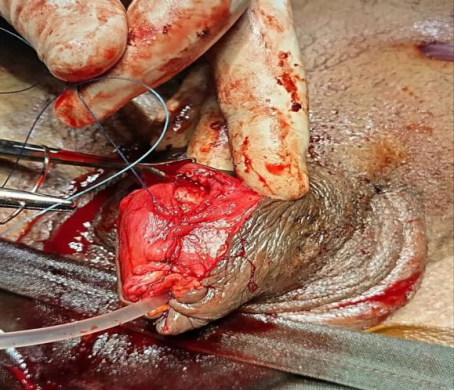
Figure 12. The tunica albuginea was repaired over the copora bodies in a water tight fashion longitudinally after the neo-urethra stump was refashioned and everted.

Figure 13. Closure of the penile skin. The tunica albuginea was first closed longitudinally in a water tight fashion over the copora bodies after the edges ot the urethra stump was everted to prevent stenosis.

Figure 14. Size 16 French urethral catheter was inserted to keep the neo-meatus patent during healing as well as for urinary drainage and monitoring. The SPC was removed after 72hours and urethral catheter removed after 4 weeks.
Information

