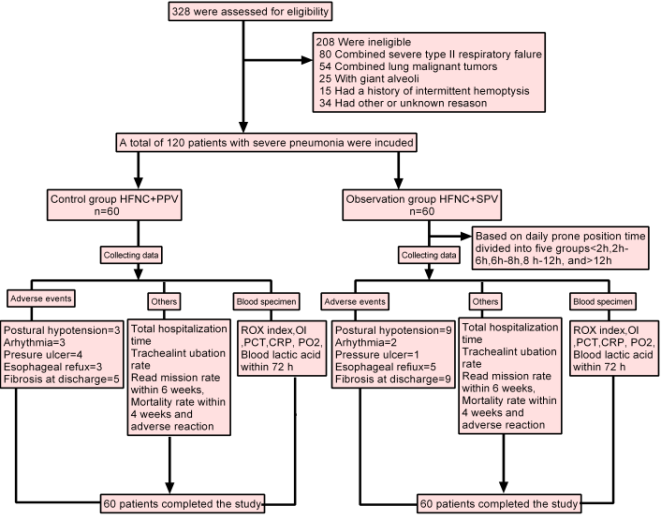
Objective: This study aims to evaluate the effect of high-flow nasal cannula (HFNC) oxygen therapy combined with awake prone position ventilation (APPV) vs. supine position ventilation (SPV) in patients with severe pneumonia. Methods: This is a quasi-experimental study enrolled patients diagnosed with severe pneumonia from the Department of Respiratory and Critical Care Medicine of the Fourth People's Hospital of Zigong City between November 2021 and January 2023. The primary endpoint was the treatment effectiveness, and the secondary endpoints included 72 h respiratory rate oxygenation index, oxygenation index, procalcitonin within 72 h, C-reactive protein within 72 h and partial pressure of oxygen within 24 h, blood lactate within 24 h, total length of hospital stay, endotracheal intubation rate within 2 weeks, readmission rate within 6 weeks, mortality rate within 4 weeks and incidence of adverse events. Results: A total of 120 patients with severe pneumonia were enrolled, evenly divided with 60 patients receiving HFNC+APPV and the other 60 receiving HFNC+SPV. The HFNC+APPV group demonstrated higher efficacy (90.0% vs. 76.7%, P=0.040) and shorter length of hospital stay (11.00(9.00,13.00) vs. 12.00(10.00,16.00), P=0.004) compared to the HFNC+SPV group. There was no significant difference in ROX index, CRP, PCT, lactate, PO2 and the onset of days, times of transferred to ICU within 1 week, times of transferred to ICU within 2 weeks, endotracheal intubation rate within 2 weeks, readmission rate within 6 weeks and mortality rate within 4 weeks between the HFNC+APPV group and HFNC+SPV group (P>0.05). The generalized estimation equation showed that the OI index at 12h, 24h, 48h and 72h was significantly higher than that at 0h (P<0.001), however, there was no significant difference in the change between HFNC+APPV group and HFNC+SPV group (P=0.604). There was no significant difference in the rate of adverse events between the HFNC+APPV group and HFNC+SPV group (P>0.05). Conclusion: The findings suggest that combining HFNC with APPV can enhance treatment efficacy and reduce hospitalization duration in severe pneumonia patients, offering valuable guidance for ventilation treatment positioning.
| Published in | International Journal of Biomedical Science and Engineering (Volume 13, Issue 1) |
| DOI | 10.11648/j.ijbse.20251301.12 |
| Page(s) | 16-23 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Severe Pneumonia, High-Flow Nasal Cannula, Awake Prone Position Ventilation, Supine Position Ventilation, Quasi-Experimental Study
Variable | HFNC+APPV group (n=60) | HFNC+SPV group (n=60) | P |
|---|---|---|---|
Sex, male, n/% | 23 (38.3%) | 22 (36.7%) | 0.850 |
Age, Mean ± SD | 63.68±6.15 | 63.55±6.07 | 0.905 |
BMI, kg/m2, Mean ± SD, | 19.93±1.77 | 19.79±1.55 | 0.643 |
Type 2 diabetes, n/% | 22 (36.7%) | 14 (23.3%) | 0.111 |
Hypertension, n/% | 27 (45.0%) | 26 (43.3%) | 0.854 |
History of the underlying pulmonary disease, n/% | 22 (36.7%) | 25 (41.7%) | 0.575 |
History of Heart Disease, n/% | 16 (26.7%) | 18 (30.0%) | 0.685 |
Variable | HFNC+APPV group (n=60) | HFNC+SPV group (n=60) | P |
|---|---|---|---|
Efficacy, n/% | 54 (90.0%) | 46 (76.7%) | 0.040 |
ROX index, Mean ± SD | 0.305 | ||
0h | 4.89±0.43 | 4.89±0.22 | |
72h | 5.50±0.65 | 5.24±0.46 | |
CRP, Mean ± SD | 0.478 | ||
0h | 55.81±39.87 | 43.18±21.14 | |
72h | 25.76±32.49 | 27.65±27.97 | |
PCT, Mean ± SD | 0.916 | ||
0h | 1.72±1.24 | 2.19±1.20 | |
72h | 1.02±1.61 | 1.46±1.52 | |
Lactate, Mean ± SD | 0.604 | ||
0h | 4.62±2.26 | 3.43±1.75 | |
24h | 2.77±2.84 | 2.76±3.49 | |
PO2, Mean ± SD | 0.454 | ||
0h | 76.17±4.68 | 77.62±4.01 | |
24h | 84.02±5.06 | 82.78±4.14 | |
The onset of days, medians (IQR) | 5.00 (4.00,6.00) | 5.00 (4.00,5.00) | 0.681 |
Length of hospital stay (days), medians (IQR) | 11.00 (9.00,13.00) | 12.00 (10.00,16.00) | 0.004 |
Times of transferred to ICU within 2 weeks, n/% | 6 (10.0%) | 8 (13.3%) | 0.570 |
Times of transferred to ICU within 1 week, n/% | 3 (5.0%) | 2 (3.3%) | 1.000 |
Endotracheal intubation rate within 2 weeks, n/% | 3 (5.0%) | 0 (0.0%) | 0.245 |
Readmission rate within 6 weeks, n/% | 4 (7.4%) | 9 (16.4%) | 0.149 |
Mortality rate within 4 weeks, n/% | 4 (6.7) | 5 (8.3%) | 1.000 |
group | 0h | 12h | 24h | 48h | 72h |
|---|---|---|---|---|---|
HFNC+APPV group | 252.89±34.86 | 284.18±39.00* | 315.96±49.81* | 344.41±56.24* | 370.55±64.30* |
HFNC+SPV group | 263.06±21.04 | 285.68±26.79* | 311.41±37.18* | 338.58±45.06* | 364.27±57.90* |
P time | - | <0.001 | <0.001 | <0.001 | <0.001 |
P group | 0.604 | ||||
variable | HFNC+APPV group (n=60) | HFNC+SPV group (n=60) | P |
|---|---|---|---|
Pressure ulcer | 1 (1.7%) | 4 (6.7%) | 0.361 |
Postural hypotension | 9 (15.0%) | 3 (5.0%) | 0.068 |
Arhythmia | 2 (3.3%) | 3 (5.0%) | 0.648 |
Esophageal reflux | 5 (8.3%) | 3 (5.0%) | 0.714 |
Fibrosis at discharge | 9 (15.0%) | 5 (8.3%) | 0.237 |
HFNC | High-flow Nasal Cannula |
APPV | Awake Prone Position Ventilation |
SPV | Supine Position Ventilation |
ICU | Intensive Care Unit |
PPV | Prone Position Ventilation |
ROX | Rate Oxygenation |
OI | Oxygenation Index |
PCT | Procalcitonin |
ARDS | Acute Respiratory Distress Syndrome |
| [1] |
Huang, C.; Zhang, J.; Zhang, C.; Zhang, P.; Mo, L. Heparin-Binding Protein in Bronchoalveolar Lavage Fluid as a Biomarker for Discriminating Severe Bacterial and Viral Pneumonia in Critically Ill Children. Mediators of inflammation 2023, 2023, 6123911.
https://doi.org/10.1155/2023/6123911 eCollection 2023. |
| [2] | Martin-Loeches, I.; Torres, A.; Nagavci, B.; Aliberti, S.; Antonelli, M.; Bassetti, M.; Bos, L. D.; Chalmers, J. D.; Derde, L.; de Waele, J.; et al. ERS/ESICM/ESCMID/ALAT guidelines for the management of severe community-acquired pneumonia. Intensive care medicine 2023, 49, 615-632. |
| [3] | Assanto, G. M.; Di Rocco, A.; Malfona, F.; Capriata, M.; Del Giudice, I.; Petrucci, L.; Girardi, P.; D'Elia, G. M.; Martelli, M.; Gentile, G.; et al. Impact of anti-SARS-CoV-2 monoclonal antibodies in the management of patients with lymphoma and COVID19: A retrospective study. Hematological oncology 2023, 41, 343-353. |
| [4] |
Ferrer, M.; Travierso, C.; Cilloniz, C.; Gabarrus, A.; Ranzani, O. T.; Polverino, E.; Liapikou, A.; Blasi, F.; Torres, A. Severe community-acquired pneumonia: Characteristics and prognostic factors in ventilated and non-ventilated patients. PloS one 2018, 13, e0191721.
https://doi.org/10.1371/journal.pone.0191721 eCollection 2018. |
| [5] | Coppola, S.; Caccioppola, A.; Froio, S.; Formenti, P.; De Giorgis, V.; Galanti, V.; Consonni, D.; Chiumello, D. Effect of mechanical power on intensive care mortality in ARDS patients. Critical care (London, England) 2020, 24, 246. |
| [6] | Sheikh, M.; Ahmad, H.; Ibrahim, R.; Nisar, I.; Jehan, F. Pulse oximetry: why oxygen saturation is still not a part of standard pediatric guidelines in low-and-middle-income countries (LMICs). Pneumonia (Nathan Qld.) 2023, 15, 3. |
| [7] | Walter, J. M.; Corbridge, T. C.; Singer, B. D. Invasive Mechanical Ventilation. Southern medical journal 2018, 111, 746-753. |
| [8] | Junhai, Z.; Jing, Y.; Beibei, C.; Li, L. The value of ROX index in predicting the outcome of high flow nasal cannula: a systematic review and meta-analysis. Respiratory research 2022, 23, 33. |
| [9] | Beduneau, G.; Boyer, D.; Guitard, P. G.; Gouin, P.; Carpentier, D.; Grangé, S.; Veber, B.; Girault, C.; Tamion, F. Covid-19 severe hypoxemic pneumonia: A clinical experience using high-flow nasal oxygen therapy as first-line management. Respiratory medicine and research 2021, 80, 100834. |
| [10] | Setten, M.; Plotnikow, G. A.; Accoce, M. Prone position in patients with acute respiratory distress syndrome. Revista Brasileira de terapia intensiva 2016, 28, 452-462. |
| [11] | Chua, E. X.; Zahir, S.; Ng, K. T.; Teoh, W. Y.; Hasan, M. S.; Ruslan, S. R. B.; Abosamak, M. F. Effect of prone versus supine position in COVID-19 patients: A systematic review and meta-analysis. Journal of clinical anesthesia 2021, 74, 110406. |
| [12] | Alviar, C. L.; Miller, P. E.; McAreavey, D.; Katz, J. N.; Lee, B.; Moriyama, B.; Soble, J.; van Diepen, S.; Solomon, M. A.; Morrow, D. A. Positive Pressure Ventilation in the Cardiac Intensive Care Unit. Journal of the American College of Cardiology 2018, 72, 1532-1553. |
| [13] | Alhazzani, W.; Parhar, K. K. S.; Weatherald, J.; Al Duhailib, Z.; Alshahrani, M.; Al-Fares, A.; Buabbas, S.; Cherian, S. V.; Munshi, L.; Fan, E.; et al. Effect of Awake Prone Positioning on Endotracheal Intubation in Patients With COVID-19 and Acute Respiratory Failure: A Randomized Clinical Trial. Jama 2022, 327, 2104-2113. |
| [14] | Mandell, L. A.; Wunderink, R. G.; Anzueto, A.; Bartlett, J. G.; Campbell, G. D.; Dean, N. C.; Dowell, S. F.; File, T. M., Jr.; Musher, D. M.; Niederman, M. S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America 2007, 44 Suppl 2, S27-72. |
| [15] | Ehrmann, S.; Li, J.; Ibarra-Estrada, M.; Perez, Y.; Pavlov, I.; McNicholas, B.; Roca, O.; Mirza, S.; Vines, D.; Garcia-Salcido, R.; et al. Awake prone positioning for COVID-19 acute hypoxaemic respiratory failure: a randomised, controlled, multinational, open-label meta-trial. The Lancet. Respiratory medicine 2021, 9, 1387-1395. |
| [16] | Kang, H.; Gu, X.; Tong, Z. Effect of Awake Prone Positioning in non-Intubated COVID-19 Patients with Acute Hypoxemic Respiratory Failure: A Systematic Review and Meta-Analysis. Journal of intensive care medicine 2022, 37, 1493-1503. |
| [17] | Lehingue, S.; Allardet-Servent, J.; Ferdani, A.; Hraeich, S.; Forel, J. M.; Arnal, J. M.; Prud'homme, E.; Penaranda, G.; Bourenne, J.; Monnet, O.; et al. Physiologic Effects of the Awake Prone Position Combined With High-Flow Nasal Oxygen on Gas Exchange and Work of Breathing in Patients With Severe COVID-19 Pneumonia: A Randomized Crossover Trial. Critical care explorations 2022, 4, e0805. |
| [18] | Guérin, C.; Reignier, J.; Richard, J. C.; Beuret, P.; Gacouin, A.; Boulain, T.; Mercier, E.; Badet, M.; Mercat, A.; Baudin, O.; et al. Prone positioning in severe acute respiratory distress syndrome. The New England journal of medicine 2013, 368, 2159-2168. |
| [19] | Munshi, L.; Del Sorbo, L.; Adhikari, N. K. J.; Hodgson, C. L.; Wunsch, H.; Meade, M. O.; Uleryk, E.; Mancebo, J.; Pesenti, A.; Ranieri, V. M.; et al. Prone Position for Acute Respiratory Distress Syndrome. A Systematic Review and Meta-Analysis. Annals of the American Thoracic Society 2017, 14, S280-s288. |
| [20] | Al-Dorzi, H. M.; Kress, J.; Arabi, Y. M. High-Flow Nasal Oxygen and Noninvasive Ventilation for COVID-19. Critical care clinics 2022, 38, 601-621. |
| [21] | Bertaina, M.; Nuñez-Gil, I. J.; Franchin, L.; Fernández Rozas, I.; Arroyo-Espliguero, R.; Viana-Llamas, M. C.; Romero, R.; Maroun Eid, C.; Uribarri, A.; Becerra-Muñoz, V. M.; et al. Non-invasive ventilation for SARS-CoV-2 acute respiratory failure: a subanalysis from the HOPE COVID-19 registry. Emergency medicine journal: EMJ 2021, 38, 359-365. |
| [22] | Kaur, R.; Vines, D. L.; Mirza, S.; Elshafei, A.; Jackson, J. A.; Harnois, L. J.; Weiss, T.; Scott, J. B.; Trump, M. W.; Mogri, I.; et al. Early versus late awake prone positioning in non-intubated patients with COVID-19. Critical care (London, England) 2021, 25, 340. |
| [23] | Papazian, L.; Munshi, L.; Guérin, C. Prone position in mechanically ventilated patients. Intensive care medicine 2022, 48, 1062-1065. |
| [24] | Froese, A. B. Gravity, the belly, and the diaphragm: you can't ignore physics. Anesthesiology 2006, 104, 193-196. |
| [25] | Chiumello, D.; Taccone, P.; Berto, V.; Marino, A.; Migliara, G.; Lazzerini, M.; Gattinoni, L. Long-term outcomes in survivors of acute respiratory distress syndrome ventilated in supine or prone position. Intensive care medicine 2012, 38, 221-229. |
APA Style
Zheng, A., Sun, K., Ma, S., Liu, P., Shen, Y., et al. (2025). Effect of High-Flow Nasal Cannula Oxygen Therapy with Awake Prone Position Ventilation vs. Supine Position Ventilation in Patients with Severe Pneumonia: A Quasi-Experimental Study. International Journal of Biomedical Science and Engineering, 13(1), 16-23. https://doi.org/10.11648/j.ijbse.20251301.12
ACS Style
Zheng, A.; Sun, K.; Ma, S.; Liu, P.; Shen, Y., et al. Effect of High-Flow Nasal Cannula Oxygen Therapy with Awake Prone Position Ventilation vs. Supine Position Ventilation in Patients with Severe Pneumonia: A Quasi-Experimental Study. Int. J. Biomed. Sci. Eng. 2025, 13(1), 16-23. doi: 10.11648/j.ijbse.20251301.12
AMA Style
Zheng A, Sun K, Ma S, Liu P, Shen Y, et al. Effect of High-Flow Nasal Cannula Oxygen Therapy with Awake Prone Position Ventilation vs. Supine Position Ventilation in Patients with Severe Pneumonia: A Quasi-Experimental Study. Int J Biomed Sci Eng. 2025;13(1):16-23. doi: 10.11648/j.ijbse.20251301.12
@article{10.11648/j.ijbse.20251301.12,
author = {Aibo Zheng and Kai Sun and Shengjun Ma and Ping Liu and Yibo Shen and Li Gu and Juan Peng},
title = {Effect of High-Flow Nasal Cannula Oxygen Therapy with Awake Prone Position Ventilation vs. Supine Position Ventilation in Patients with Severe Pneumonia: A Quasi-Experimental Study},
journal = {International Journal of Biomedical Science and Engineering},
volume = {13},
number = {1},
pages = {16-23},
doi = {10.11648/j.ijbse.20251301.12},
url = {https://doi.org/10.11648/j.ijbse.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijbse.20251301.12},
abstract = {Objective: This study aims to evaluate the effect of high-flow nasal cannula (HFNC) oxygen therapy combined with awake prone position ventilation (APPV) vs. supine position ventilation (SPV) in patients with severe pneumonia. Methods: This is a quasi-experimental study enrolled patients diagnosed with severe pneumonia from the Department of Respiratory and Critical Care Medicine of the Fourth People's Hospital of Zigong City between November 2021 and January 2023. The primary endpoint was the treatment effectiveness, and the secondary endpoints included 72 h respiratory rate oxygenation index, oxygenation index, procalcitonin within 72 h, C-reactive protein within 72 h and partial pressure of oxygen within 24 h, blood lactate within 24 h, total length of hospital stay, endotracheal intubation rate within 2 weeks, readmission rate within 6 weeks, mortality rate within 4 weeks and incidence of adverse events. Results: A total of 120 patients with severe pneumonia were enrolled, evenly divided with 60 patients receiving HFNC+APPV and the other 60 receiving HFNC+SPV. The HFNC+APPV group demonstrated higher efficacy (90.0% vs. 76.7%, P=0.040) and shorter length of hospital stay (11.00(9.00,13.00) vs. 12.00(10.00,16.00), P=0.004) compared to the HFNC+SPV group. There was no significant difference in ROX index, CRP, PCT, lactate, PO2 and the onset of days, times of transferred to ICU within 1 week, times of transferred to ICU within 2 weeks, endotracheal intubation rate within 2 weeks, readmission rate within 6 weeks and mortality rate within 4 weeks between the HFNC+APPV group and HFNC+SPV group (P>0.05). The generalized estimation equation showed that the OI index at 12h, 24h, 48h and 72h was significantly higher than that at 0h (P0.05). Conclusion: The findings suggest that combining HFNC with APPV can enhance treatment efficacy and reduce hospitalization duration in severe pneumonia patients, offering valuable guidance for ventilation treatment positioning.},
year = {2025}
}
TY - JOUR T1 - Effect of High-Flow Nasal Cannula Oxygen Therapy with Awake Prone Position Ventilation vs. Supine Position Ventilation in Patients with Severe Pneumonia: A Quasi-Experimental Study AU - Aibo Zheng AU - Kai Sun AU - Shengjun Ma AU - Ping Liu AU - Yibo Shen AU - Li Gu AU - Juan Peng Y1 - 2025/02/17 PY - 2025 N1 - https://doi.org/10.11648/j.ijbse.20251301.12 DO - 10.11648/j.ijbse.20251301.12 T2 - International Journal of Biomedical Science and Engineering JF - International Journal of Biomedical Science and Engineering JO - International Journal of Biomedical Science and Engineering SP - 16 EP - 23 PB - Science Publishing Group SN - 2376-7235 UR - https://doi.org/10.11648/j.ijbse.20251301.12 AB - Objective: This study aims to evaluate the effect of high-flow nasal cannula (HFNC) oxygen therapy combined with awake prone position ventilation (APPV) vs. supine position ventilation (SPV) in patients with severe pneumonia. Methods: This is a quasi-experimental study enrolled patients diagnosed with severe pneumonia from the Department of Respiratory and Critical Care Medicine of the Fourth People's Hospital of Zigong City between November 2021 and January 2023. The primary endpoint was the treatment effectiveness, and the secondary endpoints included 72 h respiratory rate oxygenation index, oxygenation index, procalcitonin within 72 h, C-reactive protein within 72 h and partial pressure of oxygen within 24 h, blood lactate within 24 h, total length of hospital stay, endotracheal intubation rate within 2 weeks, readmission rate within 6 weeks, mortality rate within 4 weeks and incidence of adverse events. Results: A total of 120 patients with severe pneumonia were enrolled, evenly divided with 60 patients receiving HFNC+APPV and the other 60 receiving HFNC+SPV. The HFNC+APPV group demonstrated higher efficacy (90.0% vs. 76.7%, P=0.040) and shorter length of hospital stay (11.00(9.00,13.00) vs. 12.00(10.00,16.00), P=0.004) compared to the HFNC+SPV group. There was no significant difference in ROX index, CRP, PCT, lactate, PO2 and the onset of days, times of transferred to ICU within 1 week, times of transferred to ICU within 2 weeks, endotracheal intubation rate within 2 weeks, readmission rate within 6 weeks and mortality rate within 4 weeks between the HFNC+APPV group and HFNC+SPV group (P>0.05). The generalized estimation equation showed that the OI index at 12h, 24h, 48h and 72h was significantly higher than that at 0h (P0.05). Conclusion: The findings suggest that combining HFNC with APPV can enhance treatment efficacy and reduce hospitalization duration in severe pneumonia patients, offering valuable guidance for ventilation treatment positioning. VL - 13 IS - 1 ER -
Department of Respiratory and Critical Care Medicine, Fourth People's Hospital, Zigong City, China
Department of Respiratory and Critical Care Medicine, Fourth People's Hospital, Zigong City, China
Department of Respiratory and Critical Care Medicine, Fourth People's Hospital, Zigong City, China
Department of Respiratory and Critical Care Medicine, Fourth People's Hospital, Zigong City, China
Department of Respiratory and Critical Care Medicine, Fourth People's Hospital, Zigong City, China
Department of Respiratory and Critical Care Medicine, Fourth People's Hospital, Zigong City, China
Department of Respiratory and Critical Care Medicine, Fourth People's Hospital, Zigong City, China
Information