Abstract
Severe Acute Malnutrition (SAM) is a critical condition often seen in children from low-resource settings. While its common presentations include edema, growth failure, and immune dysfunction, rare complications such as pericardial effusion and elevated liver enzymes can significantly impact management and outcomes. To highlight unusual presentations of SAM and emphasize the importance of early recognition and comprehensive management. This case series describes two pediatric patients with SAM and rare complications. The first case involved a 1-year 9-month-old girl with edematous SAM, presenting with generalized pitting edema, fever, and loose stools, accompanied by mild anemia, elevated liver enzymes, and a minimal pericardial effusion. The second case featured a 29-day-old neonate with Pierre Robin Syndrome and failure to thrive, presenting with feeding difficulties, respiratory symptoms, elevated liver enzymes, and a small pericardial effusion. Both children were managed according to WHO guidelines, including nutritional rehabilitation, antibiotics, and supportive care, resulting in stabilization and recovery. Pericardial effusion in SAM is a rare but significant complication linked to fluid retention and systemic inflammation, while elevated liver enzymes suggest hepatic dysfunction due to malnutrition and infection. These cases underline the critical need for multidisciplinary care, early detection, and tailored interventions to address such complications. Healthcare providers managing SAM should be vigilant for atypical presentations like pericardial effusion and elevated liver enzymes. Prompt recognition and comprehensive management can lead to improved outcomes, as demonstrated in these cases
Keywords
Severe Acute Malnutrtion, Pleural Effussion, Liver Enzymes, Systemic Inflammation, Nutritional Rehabilitation
1. Introduction
Severe Acute Malnutrition (SAM) is a life-threatening condition primarily affecting children in low-resource settings, often presenting with edema, growth failure, and weakened immunity.
| [1] | Anato A. Severe acute malnutrition and associated factors among children under-five years: A community based-cross sectional study in Ethiopia. Heliyon. 2022 Sep 29; 8(10): e10791. https://doi.org/10.1016/j.heliyon 2022. e10791 . PMID: 36203897; PMCID: PMC9529577. |
| [2] | Benjamin O, Lappin SL. Kwashiorkor. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507876/ |
| [3] | Briend A. Kwashiorkor - New evidence in the puzzle of oedema formation. EBioMedicine. 2022 Jun; 80: 104070. https://doi.org/10.1016/j.ebiom.2022.104070 Epub 2022 May 19. PMID: 35598438; PMCID: PMC9126987. |
| [4] | Gonzales GB, Njunge JM, Gichuki BM, Wen B, Ngari M, Potani I, Thitiri J, Laukens D, Voskuijl W, Bandsma R, Vanmassenhove J, Berkley JA. The role of albumin and the extracellular matrix on the pathophysiology of oedema formation in severe malnutrition. EBio Medicine. 2022 May; 79: 103991. https://doi.org/10.1016/j.ebiom.2022.103991 Epub 2022 Apr 7. |
| [5] | Allison SP, Lobo DN. The clinical significance of hypoalbuminaemia. Clin Nutr. 2024 Apr; 43(4): 909-914. https://doi.org/10.1016/j.clnu.2024.02.018 Epub 2024 Feb 22. PMID: 38394971. |
| [6] | Dipasquale V, Cucinotta U, Romano C. Acute Malnutrition in Children: Pathophysiology, Clinical Effects and Treatment. Nutrients. 2020 Aug 12; 12(8): 2413. https://doi.org/10.3390/nu12082413 |
| [7] | Chiabi A, Malangue B, Nguefack S, Dongmo FN, Fru F, Takou V, Angwafo F 3rd. The clinical spectrum of severe acute malnutrition in children in Cameroon: a hospital-based study in Yaounde, Cameroon. Transl Pediatr. 2017 Jan; 6(1): 32-39. https://doi.org/10.21037/tp.2016.07.05 |
[1-7]
In rare cases, SAM can be complicated by pericardial effusion and elevated liver enzymes, which are uncommon but important clinical findings.
| [8] | Surak A, Bravo G, McMurray A, Altamirano-Diaz L, and Taheri S (2019) An unusual case of pericardial effusion. Cardiology in the Young, page 1 of 4. https://doi.org/10.1017/S1047951119002129 |
| [9] | Gibson D, Mehler PS (2023) Cardiac Tamponade in Anorexia Nervosa: An Argument for Conservative Management. Ann Case Report. 8: 1406. https://doi.org/10.29011/2574-7754.101406 |
| [10] | Carey MN, Cameron LH, Rider NL, et al. What Came First: Malnutrition or Severe Disease? Pediatrics. 2023; 152(3): e2022060983. |
| [11] | Sueblinvong V, Varavithya C, Snidvongs D. Pericardial effusion in infants. J Med Assoc Thai. 1971 Mar; 54(3): 198-201. PMID: 5554350. |
| [12] | Spina G, Clemente A, Roversi M, Marchili MR, Silvestri P, Mascolo C, Zanna V, Diamanti A, Reale A, Villani A, Raucci U, Ammirati A. Early echocardiographic evaluation of children admitted to the emergency department for anorexia nervosa during the COVID-19 pandemic. Eat Weight Disord. 2022 Dec; 27(8): 3409-3417. https://doi.org/10.1007/s40519-022-01474-8 Epub 2022 Sep 2. |
| [13] | Karajibani M, Montazerifar F, Hosseini R, Suni F, Dashipour A R, et al. The Relationship Between Malnutrition and Liver Enzymes in Hospitalized Children in Zahedan: A Case-control Study. Zahedan J Res Med Sci. 2021; 23(1): e102994. https://doi.org/10.5812/zjrms.102994 |
[8-13]
This case series highlights these unusual complications, showcasing two pediatric cases where SAM was accompanied by both pericardial effusion and liver enzyme elevation. The aim is to draw attention to these complications, emphasizing the need for comprehensive management of SAM and the importance of early detection and intervention
2. Case Series
2.1. Severe Acute Oedematous Malnutrition
A 1-year 9-month-old girl presented with a two-week history of generalized pitting edema, a five-day history of intermittent low-grade fever, and non-bloody loose stools. Her mother also reported facial puffiness in the mornings, which resolved by midday. The child was born at term via spontaneous vaginal delivery with a birth weight of 2.8 kg and good Apgar scores. There were no antenatal or postnatal complications, but the child was not exclusively breastfed, as complementary feeding with water and local meal preparations was introduced at birth. Her immunizations were up to date. She is the first child of parents with no formal education, living in a mud house, and relying on water from a borehole located 20 meters from their home.
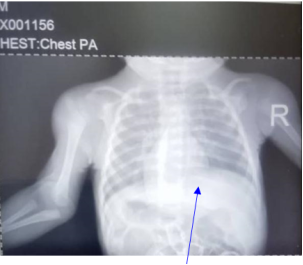
On examination, she appeared apathetic and febrile (37.7°C) with mouth sores, flaky skin, and grade three pitting pedal edema. Her weight was 8 kg, which is low for her age, even considering the edema. Systemic examination was unremarkable except for tachycardia (169 beats per minute). Laboratory investigations revealed mild anemia (Hb 9.9 g/dL), elevated liver enzymes, a chest X-ray showing loss of cardiac contour
Figure 1, and a minimal (<1 mm) pericardial effusion around the left ventricle on echocardiography.
Figure 1. Chest X-ray of a 1-year 9-month-old girl showing loss of cardiac contour suggesting intracardiac pathology possibly Pericardial effusion.
The child was managed according to WHO guidelines for Severe Acute Malnutrition (SAM). During the stabilization phase, she was treated with intravenous ampicillin (400 mg TDS) and gentamicin (40 mg OD) for seven days to address suspected sepsis. Resomal was provided after each loose stool to correct dehydration. Nutritional rehabilitation began with F-75 therapeutic food for five days before transitioning to F-100. Zinc (20 mg OD for 10 days) and syrup folic acid (1 mg OD for 10 days) were also administered. Her weight initially dropped from 8 kg to 7.5 kg due to the resolution of edema but later improved to 8.2 kg by discharge.
The discharge plan included continued nutritional rehabilitation with ready-to-use therapeutic food (RUTF), syrup folic acid, multivitamins, and ferrous sulfate (3 mg/kg OD) to address anemia. A follow-up appointment was scheduled for two weeks to monitor progress. Counseling was provided on proper feeding practices, improved hygiene, and regular follow-up care to prevent recurrence.
This case highlights the classic presentation of edematous SAM (Kwashiorkor) with its associated complications, including mild anemia and pericardial effusion. Management per WHO guidelines, incorporating nutritional rehabilitation, infection treatment, and micronutrient supplementation, resulted in successful stabilization and recovery. The child’s condition emphasizes the importance of addressing underlying risk factors such as poor breastfeeding practices, inadequate nutrition, and suboptimal living conditions to reduce the burden of malnutrition.
2.2. Peirre Robin Syndrome with Failure to Thrive
A 29-day-old male infant was admitted to the Emergency Pediatric Unit with a one-week history of nighttime cough, noisy breathing, and low-grade fever. Since birth, he struggled to breastfeed and was switched to Lactogen formula twice daily after one week. He was born at term via spontaneous vaginal delivery, weighing 3.0 kg, with Apgar scores of 7 and 10 at one and five minutes, respectively.
At birth, the baby had a low-pitched cry and was unable to sustain breastfeeding. The mother had an uncomplicated pregnancy with no history of herbal medication use or febrile illness. Immunizations were up to date, and there was no family history of cleft palate or congenital anomalies. This is the parents' first child; the father is a businessman, and the mother, a senior secondary school graduate, is a housewife. The family lives in a cement house with access to water and electricity from the national supply.
On examination, the baby appeared non-pale, non-icteric, afebrile (temperature 37.6°C), and without cyanosis, pedal oedema, or signs of dehydration. Notably, the infant had microcephaly, low-set eyes, micrognathia, and a cleft lip and palate. The systemic examination revealed no abnormalities except for a weight below the birth weight of 3.0 kg. A chest X-ray showed a loss of cardiac contour (
Figure 2) and a 0.4 mm pericardial effusion around the left ventricle. Laboratory findings included elevated liver enzymes, and a white blood cell count of 11.6 × 10⁹/L.
Figure 2. Chest X-ray of a 29-day-old infant showing a "leather bottle" heart appearance subjective of pericardial effusion.
The infant was managed with gentamicin at a dose of 15 mg once daily for seven days and intravenous ampicillin at 150 mg four times daily for 12 days. Feeding was initiated with expressed breast milk (EBM) at 60 mL every three hours. Intravenous frusemide was administered at 1.3 mg twice daily for 10 days to manage fluid retention. During the course of treatment, the infant’s weight initially dropped to 2.5 kg but improved to 3.0 kg by the 10th day of hospitalization.
He was subsequently discharged with a scheduled follow-up involving both the pediatric and maxillofacial surgery teams. The parents were counseled extensively on feeding techniques and the importance of adequate nutrition to support growth and development.
This case highlights the challenges of feeding and weight management in neonates with congenital anomalies, such as cleft lip and palate, compounded by underlying nutritional and respiratory issues. Early multidisciplinary involvement, including pediatric and surgical teams, was crucial in optimizing care and improving the infant’s condition.
3. Result
In this case series, two pediatric patients with Severe Acute Malnutrition (SAM) presented with rare complications, including pericardial effusion and elevated liver enzymes. Both cases demonstrated the importance of early recognition and management of such complications.
3.1. Case 1 (Severe Acute Oedematous Malnutrition)
The 1-year 9-month-old girl exhibited generalized edema, mild anemia, and minimal pericardial effusion, confirmed by echocardiography. Management according to WHO SAM guidelines, including nutritional rehabilitation and infection control, resulted in recovery and weight gain at discharge.
3.2. Case 2 (Pierre Robin Syndrome with Failure to Thrive)
The 29-day-old male infant presented with cleft lip and palate, microcephaly, and significant weight loss. Management included specialized feeding, antibiotic use, and fluid regulation, leading to an improved clinical condition and stabilization of weight. The cases highlight the utility of a multidisciplinary approach in addressing complex presentations of SAM. Both patients showed marked improvement with appropriate interventions, emphasizing the critical role of timely detection and tailored treatment strategies.
4. Discussion
Pericardial effusion in severe acute malnutrition (SAM) is uncommon but can occur due to fluid retention, immune dysfunction, and systemic inflammation
| [11] | Sueblinvong V, Varavithya C, Snidvongs D. Pericardial effusion in infants. J Med Assoc Thai. 1971 Mar; 54(3): 198-201. PMID: 5554350. |
[11]
. It is often associated with inadequate protein intake and, in severe cases, may lead to cardiac tamponade
| [13] | Karajibani M, Montazerifar F, Hosseini R, Suni F, Dashipour A R, et al. The Relationship Between Malnutrition and Liver Enzymes in Hospitalized Children in Zahedan: A Case-control Study. Zahedan J Res Med Sci. 2021; 23(1): e102994. https://doi.org/10.5812/zjrms.102994 |
| [14] | Mariana Parenti, Shannon MClorry, Elizabeth A. Maga, Carolyn M. Slupsky. Metabolomic changes in severe acute malnutrition suggest hepatic oxidative stress: a secondary analysis, Nutrition Research, Volume 91, 2021, Pages 44-56, ISSN 0271-5317, https://doi.org/10.1016/j.nutres.2021.05.005 |
| [15] | Nishioka H, Yoshizaki A, Imai Y, Higashibeppu N. Starvation-induced Liver Enzyme Elevation after Initiation of Feeding. Intern Med. 2019 Mar 1; 58(5): 749-753. https://doi.org/10.2169/internalmedicine.1663-18 Epub 2018 Oct 17. |
| [16] | Su A, Choe M, Birkness JE, Limketkai B, Chen PH. Two Acute Liver Injuries in a Patient With Malnutrition. J Med Cases. 2021 Aug; 12(8): 315-318. https://doi.org/10.14740/jmc3713 Epub 2021 Jul 3. |
| [17] | Imaeda M, Tanaka S, Fujishiro H, Kato S, Ishigami M, Kawano N, Katayama H, Kohmura K, Ando M, Nishioka K, Ozaki N. Risk factors for elevated liver enzymes during refeeding of severely malnourished patients with eating disorders: a retrospective cohort study. J Eat Disord. 2016 Dec 7; 4: 37. https://doi.org/10.1186/s40337-016-0127-x |
| [18] | Rao A, Cherian A, Onuora CU, Suvarnabai PC. Serum aminotransferases and gamma-glutamyl transferase in protein energy malnutrition. Trop Geogr Med. 1985 Mar; 37(1): 11-4. PMID: 2861677. |
| [19] | Costa JM, Pinto SM, Santos-Silva E, Moreira-Silva H. Incidental hypertransaminasemia in children-a stepwise approach in primary care. Eur J Pediatr. 2023 Apr; 182(4): 1601-1609. https://doi.org/10.1007/s00431-023-04825-4 Epub 2023 Jan 26. |
[13-19].
Elevated liver enzymes are frequently observed in SAM, reflecting liver damage caused by toxic proteins generated by the liver in response to malnutrition and oxidative stress because of infections
In the two cases presented, children with edematous SAM exhibited pericardial effusion and elevated liver enzymes. These complications were effectively managed through supportive care, nutritional rehabilitation, and antibiotic use
| [19] | Costa JM, Pinto SM, Santos-Silva E, Moreira-Silva H. Incidental hypertransaminasemia in children-a stepwise approach in primary care. Eur J Pediatr. 2023 Apr; 182(4): 1601-1609. https://doi.org/10.1007/s00431-023-04825-4 Epub 2023 Jan 26. |
| [20] | Kulkarni B, Mamidi RS. Nutrition rehabilitation of children with severe acute malnutrition: Revisiting studies undertaken by the National Institute of Nutrition. Indian J Med Res. 2019 Aug; 150(2): 139-152. https://doi.org/10.4103/ijmr.IJMR_1905_18 |
| [21] | Cameron R, Kogan-Liberman D. Nutritional considerations in pediatric liver disease. Pediatr Rev. 2014 Nov; 35(11): 493-6. https://doi.org/10.1542/pir.35-11-493 |
[19-21]
. Both children showed significant improvement with timely and appropriate treatment, underscoring the importance of early recognition and multidisciplinary care.
This case series emphasizes the need for healthcare providers to remain vigilant for rare complications when managing SAM. Early identification and comprehensive treatment are crucial to achieving optimal outcomes and minimizing morbidity and mortality in affected children.
5. Conclusion
This case series underscores the importance of recognizing and managing rare complications of Severe Acute Malnutrition (SAM), such as pericardial effusion and elevated liver enzymes. These findings highlight the multifaceted nature of SAM, requiring a comprehensive, multidisciplinary approach to care. Early detection and adherence to WHO management guidelines played a pivotal role in the successful recovery of both cases. Addressing underlying factors, including poor nutrition, feeding practices, and living conditions, is critical in mitigating the burden of SAM and its complications. This series emphasizes the need for ongoing vigilance and tailored interventions to improve outcomes in vulnerable pediatric populations.
6. Recommendations
To improve outcomes in children with Severe Acute Malnutrition (SAM), especially those presenting with rare complications like pericardial effusion and elevated liver enzymes, several measures are recommended. Early detection through routine screening, including echocardiography and liver function tests, should be prioritized for atypical cases. Comprehensive management adhering to WHO guidelines, such as phased nutritional rehabilitation and prompt infection control, is essential. A multidisciplinary approach involving pediatricians, cardiologists, nutritionists, and surgeons is critical for addressing complex cases.
Parent and caregiver education on proper breastfeeding practices, complementary feeding, and hygiene should be emphasized to prevent malnutrition. Community-level public health initiatives, such as food security programs and maternal education, can help mitigate the root causes of SAM. Strengthening follow-up systems for discharged children is vital to monitor growth and prevent relapses.
Further research is needed to understand the prevalence and mechanisms of rare complications in SAM and to gather longitudinal data on outcomes. Training healthcare workers to recognize and manage these complications will also enhance care quality. By implementing these strategies, the burden of SAM and its severe complications can be significantly reduced, improving survival and long-term health outcomes in vulnerable populations.
Abbreviations
SAM | Severe Acute Malnutrition |
Acknowledgments
We would like to thank the medical and nursing staff for their assistance in the care of the patient and the surgical team for their expertise in managing this case.
Author Contributions
Lamin Makalo: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Orlianys Ruiz Perez: Investigation, Visualization, Writing – original draft, Writing – review & editing
Momodou Lamin Jobarteh: Investigation, Writing – original draft
Fatoumatta Jitteh: Investigation, Writing – original draft
Isatou Bah: Data curation, Investigation, Writing – original draft
Conflict of Interest
The authors declare no conflicts of interest.
References
| [1] |
Anato A. Severe acute malnutrition and associated factors among children under-five years: A community based-cross sectional study in Ethiopia. Heliyon. 2022 Sep 29; 8(10): e10791.
https://doi.org/10.1016/j.heliyon 2022. e10791
. PMID: 36203897; PMCID: PMC9529577.
|
| [2] |
Benjamin O, Lappin SL. Kwashiorkor. [Updated 2023 Jul 17]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from:
https://www.ncbi.nlm.nih.gov/books/NBK507876/
|
| [3] |
Briend A. Kwashiorkor - New evidence in the puzzle of oedema formation. EBioMedicine. 2022 Jun; 80: 104070.
https://doi.org/10.1016/j.ebiom.2022.104070
Epub 2022 May 19. PMID: 35598438; PMCID: PMC9126987.
|
| [4] |
Gonzales GB, Njunge JM, Gichuki BM, Wen B, Ngari M, Potani I, Thitiri J, Laukens D, Voskuijl W, Bandsma R, Vanmassenhove J, Berkley JA. The role of albumin and the extracellular matrix on the pathophysiology of oedema formation in severe malnutrition. EBio Medicine. 2022 May; 79: 103991.
https://doi.org/10.1016/j.ebiom.2022.103991
Epub 2022 Apr 7.
|
| [5] |
Allison SP, Lobo DN. The clinical significance of hypoalbuminaemia. Clin Nutr. 2024 Apr; 43(4): 909-914.
https://doi.org/10.1016/j.clnu.2024.02.018
Epub 2024 Feb 22. PMID: 38394971.
|
| [6] |
Dipasquale V, Cucinotta U, Romano C. Acute Malnutrition in Children: Pathophysiology, Clinical Effects and Treatment. Nutrients. 2020 Aug 12; 12(8): 2413.
https://doi.org/10.3390/nu12082413
|
| [7] |
Chiabi A, Malangue B, Nguefack S, Dongmo FN, Fru F, Takou V, Angwafo F 3rd. The clinical spectrum of severe acute malnutrition in children in Cameroon: a hospital-based study in Yaounde, Cameroon. Transl Pediatr. 2017 Jan; 6(1): 32-39.
https://doi.org/10.21037/tp.2016.07.05
|
| [8] |
Surak A, Bravo G, McMurray A, Altamirano-Diaz L, and Taheri S (2019) An unusual case of pericardial effusion. Cardiology in the Young, page 1 of 4.
https://doi.org/10.1017/S1047951119002129
|
| [9] |
Gibson D, Mehler PS (2023) Cardiac Tamponade in Anorexia Nervosa: An Argument for Conservative Management. Ann Case Report. 8: 1406.
https://doi.org/10.29011/2574-7754.101406
|
| [10] |
Carey MN, Cameron LH, Rider NL, et al. What Came First: Malnutrition or Severe Disease? Pediatrics. 2023; 152(3): e2022060983.
|
| [11] |
Sueblinvong V, Varavithya C, Snidvongs D. Pericardial effusion in infants. J Med Assoc Thai. 1971 Mar; 54(3): 198-201. PMID: 5554350.
|
| [12] |
Spina G, Clemente A, Roversi M, Marchili MR, Silvestri P, Mascolo C, Zanna V, Diamanti A, Reale A, Villani A, Raucci U, Ammirati A. Early echocardiographic evaluation of children admitted to the emergency department for anorexia nervosa during the COVID-19 pandemic. Eat Weight Disord. 2022 Dec; 27(8): 3409-3417.
https://doi.org/10.1007/s40519-022-01474-8
Epub 2022 Sep 2.
|
| [13] |
Karajibani M, Montazerifar F, Hosseini R, Suni F, Dashipour A R, et al. The Relationship Between Malnutrition and Liver Enzymes in Hospitalized Children in Zahedan: A Case-control Study. Zahedan J Res Med Sci. 2021; 23(1): e102994.
https://doi.org/10.5812/zjrms.102994
|
| [14] |
Mariana Parenti, Shannon MClorry, Elizabeth A. Maga, Carolyn M. Slupsky. Metabolomic changes in severe acute malnutrition suggest hepatic oxidative stress: a secondary analysis, Nutrition Research, Volume 91, 2021, Pages 44-56, ISSN 0271-5317,
https://doi.org/10.1016/j.nutres.2021.05.005
|
| [15] |
Nishioka H, Yoshizaki A, Imai Y, Higashibeppu N. Starvation-induced Liver Enzyme Elevation after Initiation of Feeding. Intern Med. 2019 Mar 1; 58(5): 749-753.
https://doi.org/10.2169/internalmedicine.1663-18
Epub 2018 Oct 17.
|
| [16] |
Su A, Choe M, Birkness JE, Limketkai B, Chen PH. Two Acute Liver Injuries in a Patient With Malnutrition. J Med Cases. 2021 Aug; 12(8): 315-318.
https://doi.org/10.14740/jmc3713
Epub 2021 Jul 3.
|
| [17] |
Imaeda M, Tanaka S, Fujishiro H, Kato S, Ishigami M, Kawano N, Katayama H, Kohmura K, Ando M, Nishioka K, Ozaki N. Risk factors for elevated liver enzymes during refeeding of severely malnourished patients with eating disorders: a retrospective cohort study. J Eat Disord. 2016 Dec 7; 4: 37.
https://doi.org/10.1186/s40337-016-0127-x
|
| [18] |
Rao A, Cherian A, Onuora CU, Suvarnabai PC. Serum aminotransferases and gamma-glutamyl transferase in protein energy malnutrition. Trop Geogr Med. 1985 Mar; 37(1): 11-4. PMID: 2861677.
|
| [19] |
Costa JM, Pinto SM, Santos-Silva E, Moreira-Silva H. Incidental hypertransaminasemia in children-a stepwise approach in primary care. Eur J Pediatr. 2023 Apr; 182(4): 1601-1609.
https://doi.org/10.1007/s00431-023-04825-4
Epub 2023 Jan 26.
|
| [20] |
Kulkarni B, Mamidi RS. Nutrition rehabilitation of children with severe acute malnutrition: Revisiting studies undertaken by the National Institute of Nutrition. Indian J Med Res. 2019 Aug; 150(2): 139-152.
https://doi.org/10.4103/ijmr.IJMR_1905_18
|
| [21] |
Cameron R, Kogan-Liberman D. Nutritional considerations in pediatric liver disease. Pediatr Rev. 2014 Nov; 35(11): 493-6.
https://doi.org/10.1542/pir.35-11-493
|
Cite This Article
-
APA Style
Makalo, L., Perez, O. R., Jobarteh, M. L., Jitteh, F., Bah, I. (2025). Pericardial Effusion and Elevated Liver Enzymes as Unusual Presentations of Severe Acute Malnutrition. International Journal of Biomedical Engineering and Clinical Science, 11(1), 1-5. https://doi.org/10.11648/j.ijbecs.20251101.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Makalo, L.; Perez, O. R.; Jobarteh, M. L.; Jitteh, F.; Bah, I. Pericardial Effusion and Elevated Liver Enzymes as Unusual Presentations of Severe Acute Malnutrition. Int. J. Biomed. Eng. Clin. Sci. 2025, 11(1), 1-5. doi: 10.11648/j.ijbecs.20251101.11
Copy
|
Download
AMA Style
Makalo L, Perez OR, Jobarteh ML, Jitteh F, Bah I. Pericardial Effusion and Elevated Liver Enzymes as Unusual Presentations of Severe Acute Malnutrition. Int J Biomed Eng Clin Sci. 2025;11(1):1-5. doi: 10.11648/j.ijbecs.20251101.11
Copy
|
Download
-
@article{10.11648/j.ijbecs.20251101.11,
author = {Lamin Makalo and Orlianys Ruiz Perez and Momodou Lamin Jobarteh and Fatoumatta Jitteh and Isatou Bah},
title = {Pericardial Effusion and Elevated Liver Enzymes as Unusual Presentations of Severe Acute Malnutrition
},
journal = {International Journal of Biomedical Engineering and Clinical Science},
volume = {11},
number = {1},
pages = {1-5},
doi = {10.11648/j.ijbecs.20251101.11},
url = {https://doi.org/10.11648/j.ijbecs.20251101.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijbecs.20251101.11},
abstract = {Severe Acute Malnutrition (SAM) is a critical condition often seen in children from low-resource settings. While its common presentations include edema, growth failure, and immune dysfunction, rare complications such as pericardial effusion and elevated liver enzymes can significantly impact management and outcomes. To highlight unusual presentations of SAM and emphasize the importance of early recognition and comprehensive management. This case series describes two pediatric patients with SAM and rare complications. The first case involved a 1-year 9-month-old girl with edematous SAM, presenting with generalized pitting edema, fever, and loose stools, accompanied by mild anemia, elevated liver enzymes, and a minimal pericardial effusion. The second case featured a 29-day-old neonate with Pierre Robin Syndrome and failure to thrive, presenting with feeding difficulties, respiratory symptoms, elevated liver enzymes, and a small pericardial effusion. Both children were managed according to WHO guidelines, including nutritional rehabilitation, antibiotics, and supportive care, resulting in stabilization and recovery. Pericardial effusion in SAM is a rare but significant complication linked to fluid retention and systemic inflammation, while elevated liver enzymes suggest hepatic dysfunction due to malnutrition and infection. These cases underline the critical need for multidisciplinary care, early detection, and tailored interventions to address such complications. Healthcare providers managing SAM should be vigilant for atypical presentations like pericardial effusion and elevated liver enzymes. Prompt recognition and comprehensive management can lead to improved outcomes, as demonstrated in these cases
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Pericardial Effusion and Elevated Liver Enzymes as Unusual Presentations of Severe Acute Malnutrition
AU - Lamin Makalo
AU - Orlianys Ruiz Perez
AU - Momodou Lamin Jobarteh
AU - Fatoumatta Jitteh
AU - Isatou Bah
Y1 - 2025/02/07
PY - 2025
N1 - https://doi.org/10.11648/j.ijbecs.20251101.11
DO - 10.11648/j.ijbecs.20251101.11
T2 - International Journal of Biomedical Engineering and Clinical Science
JF - International Journal of Biomedical Engineering and Clinical Science
JO - International Journal of Biomedical Engineering and Clinical Science
SP - 1
EP - 5
PB - Science Publishing Group
SN - 2472-1301
UR - https://doi.org/10.11648/j.ijbecs.20251101.11
AB - Severe Acute Malnutrition (SAM) is a critical condition often seen in children from low-resource settings. While its common presentations include edema, growth failure, and immune dysfunction, rare complications such as pericardial effusion and elevated liver enzymes can significantly impact management and outcomes. To highlight unusual presentations of SAM and emphasize the importance of early recognition and comprehensive management. This case series describes two pediatric patients with SAM and rare complications. The first case involved a 1-year 9-month-old girl with edematous SAM, presenting with generalized pitting edema, fever, and loose stools, accompanied by mild anemia, elevated liver enzymes, and a minimal pericardial effusion. The second case featured a 29-day-old neonate with Pierre Robin Syndrome and failure to thrive, presenting with feeding difficulties, respiratory symptoms, elevated liver enzymes, and a small pericardial effusion. Both children were managed according to WHO guidelines, including nutritional rehabilitation, antibiotics, and supportive care, resulting in stabilization and recovery. Pericardial effusion in SAM is a rare but significant complication linked to fluid retention and systemic inflammation, while elevated liver enzymes suggest hepatic dysfunction due to malnutrition and infection. These cases underline the critical need for multidisciplinary care, early detection, and tailored interventions to address such complications. Healthcare providers managing SAM should be vigilant for atypical presentations like pericardial effusion and elevated liver enzymes. Prompt recognition and comprehensive management can lead to improved outcomes, as demonstrated in these cases
VL - 11
IS - 1
ER -
Copy
|
Download