Background: The postnatal phase is a critical time for women to rest and to recover after giving birth, and the hospital environment can influence the wellbeing experiences of new mothers. Existing research found aspects of the physical environments that are supportive of women during labour and birth, but research focusing on the environmental factors in postnatal environments, where women recover after birth, is limited and important. Purpose: The study investigated environmental factors and spatial features in postnatal environments that make an impact on women’s physical recovery and wellbeing following birth. Methods: Data were collected through online survey questionnaires from 229 postnatal women who gave birth in New Zealand hospitals and from 58 midwives (N = 287) who worked in postnatal settings. Midwives recruited women and their colleagues using a snowball sampling method and provided dedicated links to women and midwives to access the online survey questionnaires. Midwives filled out identical questionnaires as women; the only difference was data related to their demographic characteristics. Descriptive statistics and the independent-samples t-test were used to analyse the data... Results: Women’s and midwives’ have strong preferences for single-occupancy rooms, visual or physical connection to the outdoors, and views of nature, all of which were ranked significantly high, indicating both women and midwives desire personal control in the space, as well as connections to the outside during postnatal hospitalisation. The study participants also indicated a strong preference for air quality and room freshness, adequate daylight in the room, art and nature images and the presence of colours in the interior spaces. These design features were thought to be critical design elements for promoting rest, recovery and psychological wellbeing in postnatal settings. Conclusions: The results of this study highlight the importance of several key environmental design features, providing beneficial insights into women’s psychological recovery and wellbeing and suggesting the need for awareness by architects, and healthcare providers for creating restorative postnatal healthcare settings for women following birth.
| Published in | International Journal of Architecture, Arts and Applications (Volume 11, Issue 2) |
| DOI | 10.11648/j.ijaaa.20251102.14 |
| Page(s) | 85-95 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Environmental Factors, Healthcare Environment, Postnatal, Recovery, Wellbeing
Women | Midwives | ||||
|---|---|---|---|---|---|
Category | Mean | SD | Mean | SD | P |
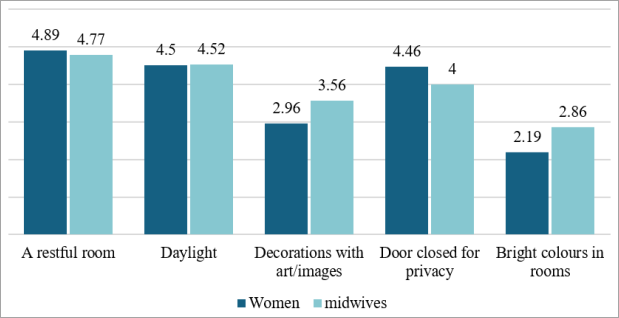
Interior features | |||||
A restful room is important to recovery | 4.89 | 0.38 | 4.77 | 0.52 | 0.158† |
A room daylight can enter | 4.50 | 0.62 | 4.52 | 0.58 | 0.796† |
Decoration in a room (nature art & images) | 2.96 | 1.05 | 3.56 | 1.07 | 0.001* |
Be in a room where the door is closed for privacy | 4.46 | 0.85 | 4. 00 | 0.97 | 0.001* |
Bright colours in a room | 2.19 | 0.91 | 2.86 | 1.03 | 0.001* |
Women | Midwives | ||||
|---|---|---|---|---|---|
Category | Mean | SD | Mean | SD | P |
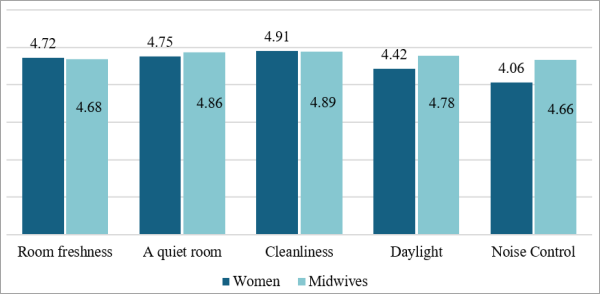
Sensory comfort | |||||
Air quality and room freshness | 4.72 | 0.53 | 4.68 | 0.59 | 0.620† |
Provision of a quiet room | 4.75 | 0.62 | 4.86 | 0.35 | 0.080** |
Hygiene/clean environment | 4.91 | 0.34 | 4.89 | 0.38 | 0.796† |
Adequate daylight in the room | 4.42 | 0.73 | 4.78 | 0.47 | 0.001* |
Noise control from equipment | 4.06 | 1.03 | 4.66 | 0.48 | 0.001* |
Women | Midwives | ||||
|---|---|---|---|---|---|
Category | Mean | SD | Mean | SD | P |
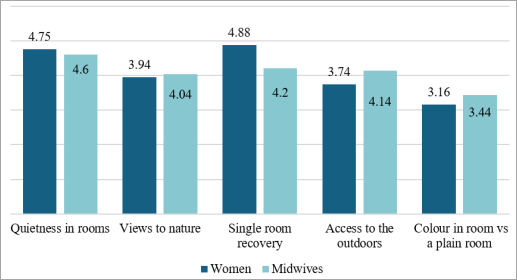
Room features | |||||
Quietness in rooms | 4.75 | 0.61 | 4.60 | 0.61 | 0.11† |
Views to nature | 3.94 | 0.73 | 4.04 | 0.61 | 0.39† |
A single room recovery | 4.88 | 0.37 | 4.20 | 0.97 | <.001* |
Access of room to the outdoors | 3.74 | 1.13 | 4.14 | 070 | <.002* |
Colours in room vs a plain room | 3.16 | 0.72 | 3.44 | 0.71 | 0.012** |
EBD | Evidence-Based Design |
SPR | Semi-Private Room/Single Private Room |
DHB | District Health Board |
LMC | Lead Maternity Carer |
SPSS | Statistical Package for the Social Sciences |
| [1] | Payam, S., Hossaini, J., Zaschka, K., Friedmann, A., & Mall, V. (2023). Designing Well-Being: A Qualitative Investigation of Young Patients’ Perspectives on the Material Hospital Environment. HERD: Health Environments Research & Design Journal, 16(3), 168-181. |
| [2] | Ulrich, R. S., Zimring, C., Zhu, X., DuBose, J., Seo, H. B., Choi, Y. S., & Joseph, A. (2008). A review of the research literature on evidence-based healthcare design. HERD: Health Environments Research & Design Journal, 1(3), 61-125. |
| [3] | Foureur, M., Davis, D., Fenwick, J., Leap, N., Iedema, R., Forbes, I., & Homer, C. S. (2010). The relationship between birth unit design and safe, satisfying birth: developing a hypothetical model. Midwifery, 26(5), 520-525. |
| [4] | Nilvér, H., & Berg, M. (2023). The birth companions’ experience of the birthing room and how it influences the supportive role: A qualitative study. HERD: Health Environments Research & Design Journal, 16(3), 156-167. |
| [5] | Sands, G., Evans, K., Spiby, H., Eldridge, J., Pallotti, P., & Evans, C. (2023). Birth environments for women with complex pregnancies: A mixed-methods systematic review. Women and Birth, 36(1), 39-46. |
| [6] | Boucher, D., Bennett, C., McFarlin, B., & Freeze, R. (2009). Staying home to give birth: why women in the United States choose home birth. Journal of midwifery & women’s health, 54(2), 119-126. |
| [7] | Waldenstrom, U., & Nilsson, C. A. (1997). A randomized controlled study of birth center care versus standard maternity care: effects on women’s health. Birth, 24(1), 17-26. |
| [8] | Hodnett, E. D., Downe, S., & Walsh, D. (2012). Alternative versus conventional institutional settings for birth. Cochrane Database of Systematic Reviews, 8. |
| [9] | Phillips, C. R. (1999). Family-centered maternity care: Past, present, future. International Journal childbirth education, 14(4), 6. |
| [10] | Mathews, J. J., & Zadak, (1991). The alternative birth movement in the United States: History and current status. Women & Health, 17(1), 39-56. |
| [11] | Stichler, J. F. (2007). Is Your hospital hospitable?: How physical environment influences patient safety. Nursing for women's health, 11(5), 506-511. |
| [12] | Verderber, S. (2010). Innovations in hospital architecture. Routledge. |
| [13] | Huisman, E. R., Morales, E., Van Hoof, J., & Kort, H. S. (2012). Healing environment: A review of the impact of physical environmental factors on users. Building and environment, 58, 70-80. |
| [14] | Rashid, M. (2013). The question of knowledge in evidence-based design for healthcare facilities: Limitations and suggestions. HERD: Health Environments Research & Design Journal, 6(4), 101-126. |
| [15] | Hansen, M. L., Lorentzen, I. P., Andersen, C. S., Jensen, H. S., Fogsgaard, A., Foureur, M., & Nohr, E. A. (2022). The effect on the birth experience of women and partners of giving birth in a “birth environment room”: A secondary analysis of a randomised controlled trial. Midwifery, 112, 103424. |
| [16] | McLeish, J., Harvey, M., Redshaw, M., Henderson, J., Malouf, R., & Alderdice, F. (2020). First-time mothers’ expectations and experiences of postnatal care in England. Qualitative health research, 30(12), 1876-1887. |
| [17] | Cheng, C. Y., Fowles, E. R., & Walker, L. O. (2006). Postpartum maternal health care in the United States: A critical review. The Journal of perinatal education, 15(3), 34. |
| [18] | MacArthur, C., Winter, H. R., Bick, D. E., Knowles, H., Lilford, R., Henderson, C., & Gee, H. (2002). Effects of redesigned community postnatal care on womens' health 4 months after birth: a cluster randomised controlled trial. The lancet, 359(9304), 378-385. |
| [19] | Boehm, H., & Morast, S. (2009). Quiet time. AJN The American Journal of Nursing, 109(11), 29-32. |
| [20] | Eberhard-Gran, M., Eskild, A., Opjordsmoen, S., & Schei, B. (2000). Postnatal care--sleep, rest and satisfaction. Tidsskrift for den Norske laegeforening: tidsskrift for praktisk medicin, ny raekke, 120(12), 1405-1409. Retrieved at: |
| [21] | Hammond, A. D., Homer, C. S., & Foureur, M. (2014). Messages from space: an exploration of the relationship between hospital birth environments and midwifery practice. HERD: Health Environments Research & Design Journal, 7(4), 81-95. |
| [22] | Hammond, A., Foureur, M., Homer, C. S., & Davis, D. (2013). Space, place and the midwife: exploring the relationship between the birth environment, neurobiology and midwifery practice. Women and Birth, 26(4), 277-281. |
| [23] | Symon, A., Paul, J., Butchart, M., Carr, V., & Dugard, P. (2008). Maternity unit design study part 3: environmental comfort and control. British Journal of Midwifery, 16(3), 167-171. |
| [24] | Adatia, S., Law, S., & Haggerty, J. (2014). Room for improvement: noise on a maternity ward. BMC health services research, 14, 1-3. |
| [25] | Driver, R. L., & Colbert, T. (2010). Shhh… Implementation of quiet time on the mother/Infant Unit. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 39(s1). |
| [26] | Nicholas, D., Connell, J. E., & Plumb, J. (2015). Sensory informed design: Human processes and emerging sensory tools. Architectural Research, 472. |
| [27] | van Hoof, J., & Verkerk, M. J. (2013). Developing an integrated design model incorporating technology philosophy for the design of healthcare environments: A case analysis of facilities for psychogeriatric and psychiatric care in The Netherlands. Technology in Society, 35(1), 1-13. |
| [28] | Li, Y., Lin, X., Li, S., Huang, M., Ren, Z., & Song, Q. (2025). Restorative Environment Design Drives Well-Being in Sustainable Elderly Day Care Centres. Buildings, 15(5), 757. |
| [29] | Aries, M. B. C., Aarts, M. P. J., & van Hoof, J. (2015). Daylight and health. A review of the evidence and consequences for the built environment. Lighting Research and Technology, 47(1), 6-27. |
| [30] | Boyce, P., Hunter, C., & Howlett, O. (2003). The benefits of daylight through windows. Troy, New York: Rensselaer Polytechnic Institute. |
| [31] | Tan, X., van Egmond, L., Partinen, M. Lange, T., & Benedict, C. (2019). A narrative review of interventions for improving sleep and reducing circadian disruption in medical inpatients. Sleep medicine, 59, 42-50. |
| [32] | Loupa, G. (2020). Influence of noise on patient recovery. Current Pollution Reports, 6, 1-7. |
| [33] | Devlin, A. S., Anderson, A., Hession-Kunz, S., Kelly, M., Noble, L., & Zou, A. (2019). Magnitude matters: Art image size and waiting time impact perceived quality of care. HERD: Health Environments Research & Design Journal, 13(3), 140-153. |
| [34] | Schafthuizen, L., Ista, E., van der Heijden, M., van Heel, L., Maben, J., van Rosmalen, J., & van Dijk, M. (2023). Hospitalized patients’ Sleep Quality compared between multioccupancy rooms and single-patient rooms. HERD: Health Environments Research & Design Journal, 16(3), 119-133. |
| [35] | Nejati, A., Shepley, M., Rodiek, S., Lee, C., & Varni, J. (2016). Restorative design features for hospital staff break areas: A multi-method study. HERD: Health Environments Research & Design Journal, 9(2), 16-35. |
| [36] | Elnaklah, R., & AlWaer, H. (2025). Impact of window views on cognitive functions and perceived comfort in healthcare environments. Building and Environment, 270, 112482. |
| [37] | Gharaveis, A., Shepley, M. M., & Gaines, K. (2016). The role of daylighting in skilled nursing short term rehabilitation facilities. HERD: Health Environments Research & Design Journal, 9(2), 105-118. |
| [38] | Halperin, D. (2014). Environmental noise and sleep disturbances: A threat to health? Sleep science, 7(4), 209-212. |
| [39] | Foureur, M. J., & Harte, J. D. (2017). Salutogenic design for birth. In Health and well-being for interior architecture (pp. 108-122). Routledge. |
| [40] | Igarashi, T., Wakita, M., Miyazaki, K., & Nakayama, T. (2014). Birth environment facilitation by midwives assisting in non-hospital births: A qualitative interview study. Midwifery, 30(7), 877-884. |
| [41] | Jenkinson, B., Josey, N., & Kruske, S. (2014). BirthSpace: An evidence-based guide to birth environment design. |
| [42] | Newburn, M., & Singh, D. (2005). Are women getting the birth environment they need: Report of a national survey of women's experiences. London: National Childbirth Trust. |
| [43] | Rayner, J. A., McLachlan, H. L., Peters, L., & Forster, D. A. (2013). Care providers’ views and experiences of postnatal care in private hospitals in Victoria, Australia. Midwifery, 29(6), 622-627. |
| [44] | Rayner, J. A., Forster, D., McLachlan, H., Yelland, J., & Davey, M. A. (2008). A state-wide review of hospital postnatal care in Victoria, Australia: the views and experiences of midwives. Midwifery, 24(3), 310-320. |
| [45] | Reyhan, F. A., Sayiner, F. D., & Ozen, H. (2023). A mixed-design study on the development of birth unit assessment scale. Midwifery, 123, 103708. |
| [46] | Forster, D. A., McLachlan, H. L., Yelland, J., Rayner, J., Lumley, J., & Davey, M. A. (2006). Staffing in postnatal units: is it adequate for the provision of quality care? Staff perspectives from a state-wide review of postnatal care in Victoria, Australia. BMC health services research, 6, 1-14. |
| [47] | Martell, L. K. (2003). Postpartum women's perceptions of the hospital environment. Journal of Obstetric, Gynecologic, & Neonatal Nursing, 32(4), 478-485. |
| [48] | Setola, N., Naldi, E., Cocina, G. G., Eide, L. B., Iannuzzi, L., & Daly, D. (2019). The impact of the physical environment on intrapartum maternity care: identification of eight crucial building spaces. HERD: Health Environments Research & Design Journal, 12(4), 67-98. |
| [49] | Ulrich, R. S. (1991, January). Effects of interior design on wellness: theory and recent scientific research. In Journal of Health Care Interior Design: Proceedings from the... Symposium on Health Care Interior Design. Symposium on Health Care Interior Design (Vol. 3, pp. 97-109). |
| [50] | Stichler, J. F. (2001). Creating healing environments in critical care units. Critical care nursing quarterly 24(3), 1-20. |
| [51] | Mann, D. (2016). Design, implementation, and early outcome indicators of a new family integrated neonatal unit. Nursing for women’s health, 20(2), 158-166. |
| [52] | Ulrich, R. S. (2001). Effects of healthcare environmental design on medical outcomes. In Design and Health: Proceedings of the Second International Conference on Health and Design. Stockholm, Sweden: Svensk Byggtjanst vol.49, 59. |
| [53] | Andrade, C. C., & Devlin, A. S. (2015). Stress reduction in the hospital room: Applying Ulrich's theory of supportive design. Journal of environmental psychology, 41, 125-134. |
| [54] | Nightingale, F. (1863). Notes on hospital. Longman, Green, Longman, Roberts, and Green. |
| [55] | Douglas, C., & Douglas, M. R. (2005). Patient-centred improvements in health-care built environments: perspectives and design indicators. Health expectations, 8(3), 264-276. |
| [56] | Quan, X., Joseph, A., & Ensign, J. C. (2012). Impact of imaging room environment: Staff job stress and satisfaction, patient satisfaction, and willingness to recommend. HERD: Health Environments Research & Design Journal, 5(2), 61-79. |
| [57] | Watts, G., Khan, A. & Pheasant, R. (2015). Influence of soundscape and interior design on anxiety and perceived tranquillity of patients in a healthcare setting. Applied Acoustics, 104, 135-141Choiniere, D. B. (2010). The effects of hospital noise. Nursing administration quarterly, 34(4), 327-333. |
| [58] | Hauck, Y., Rivers, C., & Doherty, K. (2008). Women's experiences of using a Snoezelen room during labour in Western Australia. Midwifery, 24(4), 460-470. |
| [59] | Lepori, B., Foureur, M., & Hastie, C. (2008). Mindbodyspirit architecture: creating birth space. Birth territory and midwifery guardianship: Theory for practice, education and research, 95-112. |
| [60] | Zeisel, J. (2006). Inquiry by design: Environment/behavior/neuroscience in architecture, interiors, landscape, and planning. WW Norton & Co. |
| [61] | Lindberg, C. M., & Banasiak, M. (2015). Individual differences as moderators for workspace design and well-being. Paper presented at Academy of Neuroscience for Architecture (ANFA) Conference 2012, (Salk Institute for Biological Studies, La Jolla, CA) Retrieved from: https://www.brikbase.org/search/site/Individual%20differences%20as%20moderators%20for%20workspace%20Design%20and%20wellbeing%20Lindberg |
| [62] | Qualtrics (2017). The online service for questionnaire surveys (used under Victoria University of Wellington account), Retrieved from |
| [63] | Parker, C., Scott, S., & Geddes, A. (2019). Snowball sampling. SAGE research methods foundations. |
| [64] | Verderber, S., & Reuman, D. (1987). Windows, views, and health status in hospital therapeutic environments. Journal of Architectural and Planning Research, 120-133. |
| [65] | Choi, J. H., Beltran, L. O., & Kim, H. S. (2012). Impacts of indoor daylight environments on patient average length of stay (ALOS) in a healthcare facility. Building and environment, 50, 65-75. |
| [66] | Ulrich R. S., Quan, X., Zimring, C., Joseph, A., & Choudhary, R. (2004). The role of the physical environment in the hospital of 21st century: A once-in-a-lifetime opportunity. Concord, CA: The Center for Health Design. |
| [67] | Heerwagen, J. H., & Orians, G. H. (1986). Adaptations to windowlessness: A study of the use of visual decor in windowed and windowless offices. Environment and Behavior, 18(5), 623-639. |
| [68] | Brusaferro, S., Arnoldo, L., Finzi, G., Mura, I., Auxilia, F., Pasquarella, C., & Agodi, A. (2018). Hospital Hygiene and Infection Prevention and Control in Italy: state of the art and perspectives. Annali di Igiene Medicina Preventiva e di Comunita, 30(5 Suppl. 2). |
| [69] | Pattison, H. M., & Robertson, C. E. (1996). The effect of ward design on the well‐being of post operative patients. Journal of advanced nursing, 23(4), 820-826. |
APA Style
Lawal, L. A. (2025). Designing Recovery: Women and Midwives’ Perspectives on Design Factors in the Postnatal Hospital Environment. International Journal of Architecture, Arts and Applications, 11(2), 85-95. https://doi.org/10.11648/j.ijaaa.20251102.14
ACS Style
Lawal, L. A. Designing Recovery: Women and Midwives’ Perspectives on Design Factors in the Postnatal Hospital Environment. Int. J. Archit. Arts Appl. 2025, 11(2), 85-95. doi: 10.11648/j.ijaaa.20251102.14
@article{10.11648/j.ijaaa.20251102.14,
author = {Lateef Ademola Lawal},
title = {Designing Recovery: Women and Midwives’ Perspectives on Design Factors in the Postnatal Hospital Environment
},
journal = {International Journal of Architecture, Arts and Applications},
volume = {11},
number = {2},
pages = {85-95},
doi = {10.11648/j.ijaaa.20251102.14},
url = {https://doi.org/10.11648/j.ijaaa.20251102.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ijaaa.20251102.14},
abstract = {Background: The postnatal phase is a critical time for women to rest and to recover after giving birth, and the hospital environment can influence the wellbeing experiences of new mothers. Existing research found aspects of the physical environments that are supportive of women during labour and birth, but research focusing on the environmental factors in postnatal environments, where women recover after birth, is limited and important. Purpose: The study investigated environmental factors and spatial features in postnatal environments that make an impact on women’s physical recovery and wellbeing following birth. Methods: Data were collected through online survey questionnaires from 229 postnatal women who gave birth in New Zealand hospitals and from 58 midwives (N = 287) who worked in postnatal settings. Midwives recruited women and their colleagues using a snowball sampling method and provided dedicated links to women and midwives to access the online survey questionnaires. Midwives filled out identical questionnaires as women; the only difference was data related to their demographic characteristics. Descriptive statistics and the independent-samples t-test were used to analyse the data... Results: Women’s and midwives’ have strong preferences for single-occupancy rooms, visual or physical connection to the outdoors, and views of nature, all of which were ranked significantly high, indicating both women and midwives desire personal control in the space, as well as connections to the outside during postnatal hospitalisation. The study participants also indicated a strong preference for air quality and room freshness, adequate daylight in the room, art and nature images and the presence of colours in the interior spaces. These design features were thought to be critical design elements for promoting rest, recovery and psychological wellbeing in postnatal settings. Conclusions: The results of this study highlight the importance of several key environmental design features, providing beneficial insights into women’s psychological recovery and wellbeing and suggesting the need for awareness by architects, and healthcare providers for creating restorative postnatal healthcare settings for women following birth.
},
year = {2025}
}
TY - JOUR T1 - Designing Recovery: Women and Midwives’ Perspectives on Design Factors in the Postnatal Hospital Environment AU - Lateef Ademola Lawal Y1 - 2025/06/18 PY - 2025 N1 - https://doi.org/10.11648/j.ijaaa.20251102.14 DO - 10.11648/j.ijaaa.20251102.14 T2 - International Journal of Architecture, Arts and Applications JF - International Journal of Architecture, Arts and Applications JO - International Journal of Architecture, Arts and Applications SP - 85 EP - 95 PB - Science Publishing Group SN - 2472-1131 UR - https://doi.org/10.11648/j.ijaaa.20251102.14 AB - Background: The postnatal phase is a critical time for women to rest and to recover after giving birth, and the hospital environment can influence the wellbeing experiences of new mothers. Existing research found aspects of the physical environments that are supportive of women during labour and birth, but research focusing on the environmental factors in postnatal environments, where women recover after birth, is limited and important. Purpose: The study investigated environmental factors and spatial features in postnatal environments that make an impact on women’s physical recovery and wellbeing following birth. Methods: Data were collected through online survey questionnaires from 229 postnatal women who gave birth in New Zealand hospitals and from 58 midwives (N = 287) who worked in postnatal settings. Midwives recruited women and their colleagues using a snowball sampling method and provided dedicated links to women and midwives to access the online survey questionnaires. Midwives filled out identical questionnaires as women; the only difference was data related to their demographic characteristics. Descriptive statistics and the independent-samples t-test were used to analyse the data... Results: Women’s and midwives’ have strong preferences for single-occupancy rooms, visual or physical connection to the outdoors, and views of nature, all of which were ranked significantly high, indicating both women and midwives desire personal control in the space, as well as connections to the outside during postnatal hospitalisation. The study participants also indicated a strong preference for air quality and room freshness, adequate daylight in the room, art and nature images and the presence of colours in the interior spaces. These design features were thought to be critical design elements for promoting rest, recovery and psychological wellbeing in postnatal settings. Conclusions: The results of this study highlight the importance of several key environmental design features, providing beneficial insights into women’s psychological recovery and wellbeing and suggesting the need for awareness by architects, and healthcare providers for creating restorative postnatal healthcare settings for women following birth. VL - 11 IS - 2 ER -
Department of Architecture, School of Architectural Technology, Federal University of Technology, Minna, Nigeria
Information