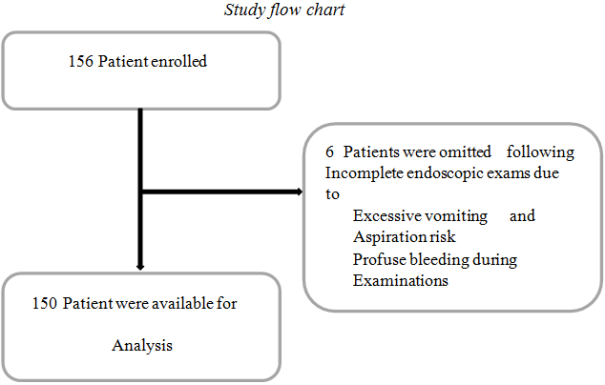
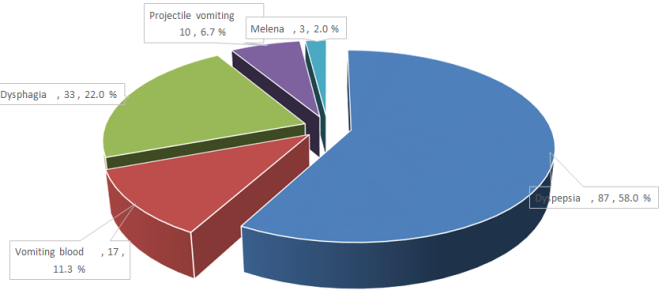
Background: Upper Gastrointestinal endoscopy is a safe procedure, and widely available technique for investigation of upper GI conditions. The demand for the investigation continues resulting in an increase number of endoscopic procedures. This observation little information is available in BMC regarding the profile of patients attending for endoscopic examination. The study aim to determine the endoscopic and clinicopathological patterns of upper GI tract conditions and establish agreement between biopsied endoscopic findings and histopathological findings of upper GI tract conditions among patients attending BMC. Methodology: This was a cross-sectional study involving patients with upper gastrointestinal tract conditions receiving endoscopic examination with or without biopsy at BMC between January and May 2020. Recruitment of patient based on serial technique and endoscopic examination done under short sedation. Biopsy were taken on the same sit in eligible patient and preserved in 10% formalin for further histology evaluation. Results: Total of 150 participants were included in the study,139 (92.7%) were attended from outpatient clinics and 11 (7.3%) from inpatients. The median age was 50[IQR 34-65] years. Dyspepsia was the leading clinical presentation 87 (58.0%). In the study population, 141 (94.0%) had abnormal endoscopic findings. Gastritis was the leading finding in both endoscopic and histopathological finding with 41(29.1%) and 36(32.1%). Among patients with abnormal histopathological findings, 23 were esophageal malignancies, 10 gastric malignancies, and 1 duodenal malignancy. The Kappa value 0.778 considered a substantial agreement between endoscopic findings and histopathological findings where K value interpreted as <0.4 as fair, 0.4 to 0.6 as moderate, 0.6 to 0.8 substantial and >0.8 near perfect. Conclusion: Dyspepsia was the commonest clinical presentation among the study participants while gastritis was the leading finding on both endoscopic and histopathological results, followed by esophageal and gastric malignancy. There is substantial agreement between endoscopic and histopathological findings; therefore endoscopy is incomplete without biopsy and histopathology as the gold standard for the diagnosis of upper gastrointestinal conditions.
| Published in | European Journal of Preventive Medicine (Volume 13, Issue 2) |
| DOI | 10.11648/j.ejpm.20251302.11 |
| Page(s) | 34-42 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Endoscopic, Clinicopathological, Gastrointestinal Conditions, Tanzania
Variable | Frequency(n) | Percent (%) |
|---|---|---|
Age(years) | ||
<55( median 50) | 88 | 58.6 |
≥55(IQR 34-65) | 62 | 41.4 |
Gender | ||
Male | 79 | 52.7 |
Female | 71 | 47.3 |
Attended From | ||
Outpatient | 139 | 92.7 |
Inpatient | 11 | 7.3 |
Residence | ||
Urban | 84 | 56.0 |
Rural | 66 | 44.0 |
Education Level | ||
Primary/Secondary | 95 | 63.3 |
College/University | 55 | 36.7 |
Marital Status | ||
Single | 43 | 28.7 |
Married | 107 | 71.3 |
Occupation | ||
Employed | 57 | 38.0 |
Unemployed | 24 | 16.0 |
Peasant | 69 | 46.0 |
Mode of Cost sharing | ||
Insured | 90 | 60.0 |
Not Insured | 60 | 40.0 |
Risk Factors | ||
Smoking | 14 | 9.5 |
Alcohol | 50 | 33.8 |
Corrosives | 1 | 0.7 |
NSAIDs | 11 | 7.4 |
Stress | 72 | 48.6 |
Endoscopic findings | Frequency(n) | Percentage (%) |
|---|---|---|
Normal | 09 | 6.0 |
Oesophageal mass | 27 | 18.0 |
Gastric mass | 11 | 7.3 |
Gastritis | 41 | 27.3 |
Gastric ulcer | 18 | 12.0 |
Duodenal ulcer | 18 | 12.0 |
Gastroesophageal reflux disease | 07 | 4.7 |
Oesophageal stricture | 01 | 0.7 |
Oesophageal/Gastric varices | 17 | 11.3 |
Gastric outlet obstruction | 01 | 0.7 |
Total | 150 | 100 |
Endoscopic findings | Reasons |
|---|---|
Gastroesophageal reflux disease(GERD) | Erosive esophagitis with LES muscle failure to close tightly |
Esophageal/gastric varices | They are enlarged vein in esophagus and gastrium due to portal vein obstruction. |
Esophageal stricture | Narrowing of lumen due to corrosive ingestion |
Gastric outlet obstruction | An obstruction at the pylorus which is the outlet of the stomach. |
Anatomicalsite | Histopathological results | |||||||
|---|---|---|---|---|---|---|---|---|
SCC | Adenocarcinoma | GIST | Barret Esophagus | Gastritis | Duodenitis | Polyps | Total | |
Oesophagus | 17 | 6 | - | 1 | - | - | - | 24 |
Gastric | 6 | 4 | - | 51 | - | - | 61 | |
Duodenum | - | 1 | - | - | - | 13 | 1 | 15 |
Total | 17 | 13 | 4 | 1 | 51 | 13 | 1 | 100 |
Endoscopic | Histopathology | Kappa | |
|---|---|---|---|
Benign | Malignancy | ||
Benign | 64 | 2 | 0.778 |
Malignancy | 1 | 32 | |
BE | Barrett Esophagus |
BMC | Bugando Medical Center |
CREC | CUHAS BMC Research and Ethics Committee |
CUHAS | Catholic University of Health and Allied Science |
ESGE | European Society of Gastrointestinal Endoscopy |
GERD | Gastro Esophageal Reflux Disease |
GI | Gastro Intestinal |
GIST | Gastro Intestinal Stromal Tumor |
GIT | Gastro Intestinal Tract |
HIV | Human Immunodeficiency Virus |
H.Pylori | Helicobacter Pylori |
IQR | Inter Quartile Range |
NSAIDs | Non-Steroidal Ant inflammatory Drugs |
PI | Principal Investigator |
RA | Research Assistant |
WHO | WorldHealth Organization |
| [1] | Ainapure R, Tanga V. A clinico-endoscopic study of upper GI disorders in rural population. International Surgery Journal. 2018; 5(3): 1111-3. |
| [2] | Caglar E, Baysal B, Dobrucalı A. The changing pattern of upper gastrointestinal disorders by endoscopy: data of the last 40 years. Diagnostic and therapeutic endoscopy. 2014; 2014. |
| [3] | Al-Humayed SM, Mohamed-Elbagir AK, Al-Wabel AA, Argobi YA. The changing pattern of upper gastro-intestinal lesions in southern Saudi Arabia: an endoscopic study. Saudi journal of gastroenterology: official journal of the Saudi Gastroenterology Association. 2010; 16(1): 35. |
| [4] | Memon F, Baloch K, Memon AA. UPPER GASTROINTESTINAL ENDOSCOPIC BIOPSY. The Professional Medical Journal. 2015; 22(12): 1574-9. |
| [5] | Lodenyo H, Rana F, Mutuma GZ, Kabanga JM, Kuria JK, Okoth FA. Patterns of upper gastrointestinal diseases based on endoscopy in the period 1998-2001. African journal of health sciences. 2005; 12(1): 49-54. |
| [6] | Kalebi A, Rana F, Mwanda W, Lule G, Hale M. Histopathological profile of gastritis in adult patients seen at a referral hospital in Kenya. World Journal of Gastroenterology: WJG. 2007; 13(30): 4117. |
| [7] | Sonnenberg A. historic changes of Helicobacter pylori associated diseases. Alimentary pharmacology & therapeutics. 2013; 38(4): 329-42. |
| [8] | Mohamed FA, Lule G, Nyong’o A, Bwayo J, Rana F. Prevalence of Helicobacter pylori and endoscopic findings in HIV seropositive patients with upper gastrointestinal tract symptoms at Kenyatta National Hospital, Nairobi. East African medical journal. 2002; 79(5): 226-31. |
| [9] | Goldacre MJ. Demography of aging and the epidemiology of gastrointestinal disorders in the elderly. Best practice & research Clinical gastroenterology. 2009; 23(6): 793-804. |
| [10] | Rustgi AK, El-Serag HB. Esophageal carcinoma. New England Journal of Medicine. 2014; 371(26): 2499-509. |
| [11] | Loffeld RJLF, Liberov B, Dekkers PEP. The changing prevalence of upper gastrointestinal endoscopic diagnoses: a single-centre study. Neth J Med. 2012; 70(5): 222-6. |
| [12] | Vyse A, Gay N, Hesketh L, Andrews N, Marshall B, Thomas H, et al. The burden of Helicobacter pylori infection in England and Wales. Epidemiology & Infection. 2002; 128(3): 411-7. |
| [13] | Pennathur A, Gibson MK, Jobe BA, Luketich JD. Oesophageal carcinoma. The Lancet. 2013; 381(9864): 400-12. |
| [14] | Mchembe MD, Rambau PF, Chalya PL, Jaka H, Koy M, Mahalu W. Endoscopic and clinicopathological patterns of esophageal cancer in Tanzania: experiences from two tertiary health institutions. World journal of surgical oncology. 2013; 11(1): 257. |
| [15] | Saul C, Teixeira CR, Pereira-Lima JC, Torresini RJS. Prevalence reduction of duodenal ulcer: a Brazilian study. (retrospective analysis in tha last decade: 19962005). Arquivos de gastroenterologia. 2007; 44(4): 320-4. |
| [16] | Shepherd NA, Valori RM. The effective use of gastrointestinal histopathology: guidance for endoscopic biopsy in the gastrointestinal tract. Frontline gastroenterology. 2014; 5(2): 84-7. |
| [17] | Kibiki G, Hauser M, Lyamuya S, Lyaruu I, Ole-Nguyaine S, Dolmans W. Causes of upper gastrointestinal bleeding in Tanzania. Tanzania Medical Journal. 2003; 18: 28. |
| [18] | Suba MR, Ayana SM, Mtabho CM, Kibiki GS. The aetiology, management and clinical outcome of upper gastrointestinal bleeding among patients admitted at the Kilimanjaro Christian Medical Centre in Moshi, Tanzania. Tanzania journal of health research. 2010; 12(4): 286-9. |
| [19] | Ayana SM, Swai B, Maro V, Kibiki GS. Upper gastrointestinal endoscopic findings and prevalence of Helicobacter pylori infection among adult patients with dyspepsia in northern Tanzania. Tanzania journal of health research. 2014; 16(1). |
| [20] | Muhumba E, Magafu MG, Mwita JC, Mkongo E, Mwandri MB. Gastrointestinal endoscopy at Amana Municipal Referral Hospital in Tanzania: reasons for referral and findings. Tanzania Journal of Health Research. 2015; 17(2). |
| [21] | Jaka H, Koy M, Liwa A, Kabangila R, Mirambo M, Scheppach W, et al. A fibreoptic endoscopic study of upper gastrointestinal bleeding at Bugando Medical Centre in northwestern Tanzania: a retrospective review of 240 cases. BMC research notes. 2012; 5(1): 200. |
| [22] | Krishnappa R, Horakerappa M, Ali K, Gouri M. A study on histopathological spectrum of upper gastrointestinal tract endoscopic biopsies. International Journal of Medical Research & Health Sciences. 2013; 2(3): 418-24. |
| [23] | Rani D, Bhuvan S, Gupta A. A study of morphological spectrum of upper gastrointestinal tract lesions by endoscopy and correlation between endoscopic and histopathological findings. Indian Journal of Pathology and Oncology. 2019; 6(1). |
| [24] | Padma S, Murugan R. Disease pattern by upper gastrointestinal endoscopy in rural areas of Tiruchirappalli district carried out at CMCH and RC Irungalur, retrospective study and comparative analysis with other contemporary studies in India. International Surgery Journal. 2018; 5(3): 965-70. |
| [25] | Talley NJ, Zinsmeister AR, Schleck CD, Melton III LJ. Dyspepsia and dyspepsia subgroups: a population-based study. Gastroenterology. 1992; 102(4): 1259-68. |
| [26] | Olokoba A, Bojuwoye B. Indications for oesophagogastroduodenoscopy in Ilorin, Nigeria-a 30 month review. Nigerian journal of clinical practice. 2010; 13(3). |
| [27] | Obayo S, Muzoora C, Ocama P, Cooney MM, Wilson T, Probert CS. Upper gastrointestinal diseases in patients for endoscopy in South-Western Uganda. African health sciences. 2015; 15(3): 959-66. |
| [28] | Zullo A, Manta R, De Francesco V, Fiorini G, Hassan C, Vaira D. Diagnostic yield of upper endoscopy according to appropriateness: A systematic review in Digestive and Liver Disease Italy, 2017. |
| [29] | Yi Liu, Naomi Uemura, Shu-Dong Xiao, Guido N. J. Tytgat, Fiebo J. W. Ten KateAgreement between endoscopic and histological gastric atrophy scores. |
APA Style
Munema, F., Rambau, P., Byabato, S., Binde, A., Mabega, N. (2025). Endoscopic and Clinicopathological Patterns of Upper Gastrointestinal Conditions Among Patients Receiving Endoscopic Examinations at Bugando Medical Centre Mwanza Tanzania. European Journal of Preventive Medicine, 13(2), 34-42. https://doi.org/10.11648/j.ejpm.20251302.11
ACS Style
Munema, F.; Rambau, P.; Byabato, S.; Binde, A.; Mabega, N. Endoscopic and Clinicopathological Patterns of Upper Gastrointestinal Conditions Among Patients Receiving Endoscopic Examinations at Bugando Medical Centre Mwanza Tanzania. Eur. J. Prev. Med. 2025, 13(2), 34-42. doi: 10.11648/j.ejpm.20251302.11
AMA Style
Munema F, Rambau P, Byabato S, Binde A, Mabega N. Endoscopic and Clinicopathological Patterns of Upper Gastrointestinal Conditions Among Patients Receiving Endoscopic Examinations at Bugando Medical Centre Mwanza Tanzania. Eur J Prev Med. 2025;13(2):34-42. doi: 10.11648/j.ejpm.20251302.11
@article{10.11648/j.ejpm.20251302.11,
author = {Furaha Munema and Peter Rambau and Samwel Byabato and Ahmed Binde and Ndakibae Mabega},
title = {Endoscopic and Clinicopathological Patterns of Upper Gastrointestinal Conditions Among Patients Receiving Endoscopic Examinations at Bugando Medical Centre Mwanza Tanzania},
journal = {European Journal of Preventive Medicine},
volume = {13},
number = {2},
pages = {34-42},
doi = {10.11648/j.ejpm.20251302.11},
url = {https://doi.org/10.11648/j.ejpm.20251302.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ejpm.20251302.11},
abstract = {Background: Upper Gastrointestinal endoscopy is a safe procedure, and widely available technique for investigation of upper GI conditions. The demand for the investigation continues resulting in an increase number of endoscopic procedures. This observation little information is available in BMC regarding the profile of patients attending for endoscopic examination. The study aim to determine the endoscopic and clinicopathological patterns of upper GI tract conditions and establish agreement between biopsied endoscopic findings and histopathological findings of upper GI tract conditions among patients attending BMC. Methodology: This was a cross-sectional study involving patients with upper gastrointestinal tract conditions receiving endoscopic examination with or without biopsy at BMC between January and May 2020. Recruitment of patient based on serial technique and endoscopic examination done under short sedation. Biopsy were taken on the same sit in eligible patient and preserved in 10% formalin for further histology evaluation. Results: Total of 150 participants were included in the study,139 (92.7%) were attended from outpatient clinics and 11 (7.3%) from inpatients. The median age was 50[IQR 34-65] years. Dyspepsia was the leading clinical presentation 87 (58.0%). In the study population, 141 (94.0%) had abnormal endoscopic findings. Gastritis was the leading finding in both endoscopic and histopathological finding with 41(29.1%) and 36(32.1%). Among patients with abnormal histopathological findings, 23 were esophageal malignancies, 10 gastric malignancies, and 1 duodenal malignancy. The Kappa value 0.778 considered a substantial agreement between endoscopic findings and histopathological findings where K value interpreted as 0.8 near perfect. Conclusion: Dyspepsia was the commonest clinical presentation among the study participants while gastritis was the leading finding on both endoscopic and histopathological results, followed by esophageal and gastric malignancy. There is substantial agreement between endoscopic and histopathological findings; therefore endoscopy is incomplete without biopsy and histopathology as the gold standard for the diagnosis of upper gastrointestinal conditions.},
year = {2025}
}
TY - JOUR T1 - Endoscopic and Clinicopathological Patterns of Upper Gastrointestinal Conditions Among Patients Receiving Endoscopic Examinations at Bugando Medical Centre Mwanza Tanzania AU - Furaha Munema AU - Peter Rambau AU - Samwel Byabato AU - Ahmed Binde AU - Ndakibae Mabega Y1 - 2025/03/18 PY - 2025 N1 - https://doi.org/10.11648/j.ejpm.20251302.11 DO - 10.11648/j.ejpm.20251302.11 T2 - European Journal of Preventive Medicine JF - European Journal of Preventive Medicine JO - European Journal of Preventive Medicine SP - 34 EP - 42 PB - Science Publishing Group SN - 2330-8230 UR - https://doi.org/10.11648/j.ejpm.20251302.11 AB - Background: Upper Gastrointestinal endoscopy is a safe procedure, and widely available technique for investigation of upper GI conditions. The demand for the investigation continues resulting in an increase number of endoscopic procedures. This observation little information is available in BMC regarding the profile of patients attending for endoscopic examination. The study aim to determine the endoscopic and clinicopathological patterns of upper GI tract conditions and establish agreement between biopsied endoscopic findings and histopathological findings of upper GI tract conditions among patients attending BMC. Methodology: This was a cross-sectional study involving patients with upper gastrointestinal tract conditions receiving endoscopic examination with or without biopsy at BMC between January and May 2020. Recruitment of patient based on serial technique and endoscopic examination done under short sedation. Biopsy were taken on the same sit in eligible patient and preserved in 10% formalin for further histology evaluation. Results: Total of 150 participants were included in the study,139 (92.7%) were attended from outpatient clinics and 11 (7.3%) from inpatients. The median age was 50[IQR 34-65] years. Dyspepsia was the leading clinical presentation 87 (58.0%). In the study population, 141 (94.0%) had abnormal endoscopic findings. Gastritis was the leading finding in both endoscopic and histopathological finding with 41(29.1%) and 36(32.1%). Among patients with abnormal histopathological findings, 23 were esophageal malignancies, 10 gastric malignancies, and 1 duodenal malignancy. The Kappa value 0.778 considered a substantial agreement between endoscopic findings and histopathological findings where K value interpreted as 0.8 near perfect. Conclusion: Dyspepsia was the commonest clinical presentation among the study participants while gastritis was the leading finding on both endoscopic and histopathological results, followed by esophageal and gastric malignancy. There is substantial agreement between endoscopic and histopathological findings; therefore endoscopy is incomplete without biopsy and histopathology as the gold standard for the diagnosis of upper gastrointestinal conditions. VL - 13 IS - 2 ER -
Department of Surgery, Sekou Toure Regional Referral Hospital, Mwanza, United Republic of Tanzania
Department of Pathology, Catholic University of Healthy and Allied Sciences, Mwanza, United Republic of Tanzania
Department of Surgery, Catholic University of Health and Allied Sciences, Mwanza, United Republic of Tanzania
Department of Surgery, Catholic University of Health and Allied Sciences, Mwanza, United Republic of Tanzania
Department of Clinical Research, National Institute for Medical Research, Mwanza Research Centre, Mwanza, United Republic of Tanzania
Information