Abstract
Breast cancer is a type of cancer that is distinguished by the uncontrolled and abnormal growth of breast cells. Globally, it remained the most frequently diagnosed neoplastic disease in women and the leading cause of cancer-related death. Despite the increasing incidence of breast cancer in Ethiopia, there has been a limited study that determines the risk factors for breast cancer. This study employed a hospital-based matched case-control design to analyze breast cancer risk factors for women seeking care at the Hawassa University Comprehensive Specialized Hospital in Hawassa, Ethiopia. A hospital-based, unmatched case-control study design was employed from March 1 to April 30, 2022, among 131 cases and 257 control women attending Hawassa University Comprehensive Specialized Hospital. Data were collected using a standardized, pre-tested questionnaire. SPSS version 20 was used for the statistical analysis of the data. Descriptive statistics were used to summarize the socio-demographic, reproductive, and other characteristics of respondents. The bivariable and multivariable logistic regression analyses were used to assess variables associated with breast cancer and were presented with a 95% confidence interval. The final result was displayed using text figures and tables. In this study, age [AOR=5.79, 95%CI (2.11, 12.75)], family history of cancer (AOR=6.05, 95% CI (1.92 19.03), not consuming fruits (AOR=3.34, 955; CI 1.32, 8.48), eating sea foods (fish) (AOR=.24, 95% CI 0.1, 0.60), using packed food or drink (AOR= 4.10 95% CI, 1.23, 13.67), hormonal contraceptive use (AOR= 3.86 95%, CI 1.62, 9.24), having history of breast injury (AOR= 3.29 95% CI 1.20 9.01), history of abortion (AOR=3.16, 95% CI 1.11 9.00), exposure of radiation (AOR= 2.64 95% CI, 1.14 6.15) were risk factors associated with breast cancer. Having a family history of cancer, not eating fruits, not eating sea foods (fish), using packed foods or drinks, using hormonal contraception, having a history of breast injury, a history of abortion, and previous radiation exposure were all risk factors for breast cancer. Health professionals should deliver health education on the importance of a fruit and fish diet and its association with lower breast cancer risk.
|
Published in
|
Cancer Research Journal (Volume 13, Issue 2)
|
|
DOI
|
10.11648/j.crj.20251302.14
|
|
Page(s)
|
56-70 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Risk Factors, Breast Cancer, Hawassa
1. Introduction
1.1. Background
Cancer is a disease in which certain cells of the body grow uncontrollably and spread to other parts of the body. It has the potential to begin almost anywhere in the human body
| [1] | C. Zeng, W. Wen, A. K. Morgans, W. Pao, X. O. Shu, and W. Zheng, “Disparities by Race, Age, and Sex in the Improvement of Survival for Major Cancers: Results From the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) Program in the United States, 1990 to 2010,” JAMA Oncol., vol. 1, no. 1, pp. 88–96, Apr. 2015, https://doi.org/10.1001/JAMAONCOL.2014.161 |
[1]
. In 2020, an estimated 19.3 million new cancer cases (18.1 million excluding non-melanoma skin cancer) and nearly 10.0 million cancer deaths (9.9 million excluding non-melanoma skin cancers) occurred worldwide
| [2] | J. Ferlay et al., “Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012,” Int. J. Cancer, vol. 136, no. 5, pp. E359–E386, Mar. 2015, https://doi.org/10.1002/IJC.29210 |
[2]
.
Breast cancer is a type of cancer that is distinguished by the uncontrolled and abnormal growth of breast cells. Breast cancer almost always occurs in the glands or ducts that produce milk and transport it to the nipple. Breast cancer is a metastatic cancer and can commonly disseminate to distant organs and systems such as the lymph nodes, bone, liver, lung, and brain, which mainly accounts for its incurability. Staging describes the extent of the breast cancer, including the size of the tumor, whether it has distributed to lymph nodes, if it has spread to distant parts of the body, and what genetic markers are present
| [3] | A. Fazel et al., “Marked increase in breast cancer incidence in young women: A 10-year study from Northern Iran, 2004–2013,” Cancer Epidemiol., vol. 62, p. 101573, Oct. 2019, https://doi.org/10.1016/J.CANEP.2019.101573 |
[3]
.
The American Joint Committee on Cancer staged breast cancer by using tumor node metastasis (TNM); stages 0–4 are included, with subcategories for each step. Sub-stages can provide information about a tumor's features, such as its human epidermal growth factor receptor 2 (HER2) status. HER2 is a protein that controls the growth, division, and repair of breast cells. When it doesn’t work properly, many abnormal breast cells will be formed
| [4] | R. M. Tamimi et al., “Population Attributable Risk of Modifiable and Nonmodifiable Breast Cancer Risk Factors in Postmenopausal Breast Cancer,” Am. J. Epidemiol., vol. 184, no. 12, pp. 884–893, Dec. 2016, https://doi.org/10.1093/AJE/KWW145 |
[4]
.
The clinical manifestation of breast cancer varies from person to person. Some people show no signs or symptoms at all. Some breast cancer symptoms include: a new lump in the breast or underarm (armpit); thickening or swelling of a portion of the breast; irritation or dimpling of breast skin; redness or flaky skin in the nipple area or the breast; pulling in of the nipple or pain in the nipple area; nipple discharge other than breast milk, including blood; and changes in the size or shape of the breast
| [5] | K. Unger-Saldaña, “Challenges to the early diagnosis and treatment of breast cancer in developing countries,” World J. Clin. Oncol., vol. 5, no. 3, p. 465, Aug. 2014, https://doi.org/10.5306/WJCO.V5.I3.465 |
[5]
.
Globally, breast cancer remained the most frequently diagnosed neoplastic disease in women and the leading cause of cancer-related death
| [6] | F. W. Dos Santos Figueiredo, T. C. Do Carmo Almeida, J. H. M. Schoueri, C. Luisi, and F. Adami, “Association between primary care coverage and breast cancer mortality in Brazil,” PLoS One, vol. 13, no. 8, p. e0200125, Aug. 2018, https://doi.org/10.1371/JOURNAL.PONE.0200125 |
[6]
. Breast cancer affects one out of every four women and accounts for one out of every six cancer deaths, ranking first in incidence in the vast majority of countries
| [7] | H. Sung et al., “Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA. Cancer J. Clin., vol. 71, no. 3, pp. 209–249, May 2021, https://doi.org/10.3322/CAAC.21660 |
[7]
. According to WHO reports, in 2020, a total of 2.3 million women were diagnosed with breast cancer, and 685, 000 deaths were attributed to breast cancer worldwide
.
In Africa, breast cancer is responsible for 28% of all cancers and 20% of all cancer deaths in women; according to evidence from GLOBOCAN, 74 072 women lost their lives due to breast cancer, and 168 690 cases were estimated to have occurred in 2018
. The International Agency for Cancer Research (IARC) estimated that the incidence of breast cancer varied from 26.8 per 100,000 women in Middle Africa to 38.9 per 100,000 women in southern Africa in 2012
| [10] | S. T. Memirie et al., “Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data,” J. Glob. Oncol., vol. 2018, no. 4, pp. 1–11, Mar. 2018, https://doi.org/10.1200/JGO.17.00175 |
[10]
. In Ethiopia, the incidence of breast cancer accounted for 22.6% of all cases of cancer and 17% of cancer mortality annually
| [12] | H. M. Asif, S. Sultana, N. Akhtar, J. U. Rehman, and R. U. Rehman, “Prevalence, risk factors and disease knowledge of breast cancer in Pakistan,” Asian Pacific J. Cancer Prev., vol. 15, no. 11, pp. 4411–4416, 2014, https://doi.org/10.7314/APJCP.2014.15.11.4411 |
[12]
. However, little is known about breast cancer risk factors in low- and middle-income countries due to poor registration and reporting systems.
Breast cancer risk, like all cancer risks, is determined by a variety of factors and differs from person to person. Reproductive factors, including early menarche, late menopause, null parity, and the absence of a history of breastfeeding, increase the risk of breast cancer
| [11] | M. Harvie, A. Howell, and D. G. Evans, “Can Diet and Lifestyle Prevent Breast Cancer: What Is the Evidence?,” Am. Soc. Clin. Oncol. Educ. B., no. 35, pp. e66–e73, May 2015, https://doi.org/10.14694/edbook_am.2015.35.e66 |
| [13] | A. Balekouzou et al., “Reproductive risk factors associated with breast cancer in women in Bangui: A case-control study,” BMC Womens. Health, vol. 17, no. 1, pp. 1–9, Mar. 2017, https://doi.org/10.1186/S12905-017-0368-0/TABLES/3 |
[11, 13]
.
Avoiding modifiable risks will help reduce morbidity related to cancer. According to reports from experts, successful lifestyle changes could prevent 25% to 30% of breast cancer cases
. These reductions will only be realized if targeted prevention programs for high-risk women, as well as women participating in population-based breast screening programs, can be implemented during childhood, adolescence, and early adulthood
.
1.2. Statement of Problem
Breast cancer is an emerging public health problem with a growing incidence in all countries since 1960. It was the leading cause of cancer deaths among all women worldwide
. The global incidence of breast cancer grew by 3.1% each year, from 641,000 cases in 1980 to 1,643,000 cases in 2010 and 2.3 million in 2020
| [8] | M. Evelina Arzanova and P. Harvey N. Mayrovitz, “The Epidemiology of Breast Cancer,” Exon Publ., vol. 23, pp. 1–19, Aug. 2022, https://doi.org/10.36255/EXON-PUBLICATIONS-BREAST-CANCER-EPIDEMIOLOGY |
| [15] | M. H. Forouzanfar et al., “Breast and cervical cancer in 187 countries between 1980 and 2010: A systematic analysis,” Lancet, vol. 378, no. 9801, pp. 1461–1484, Oct. 2011, https://doi.org/10.1016/S0140-6736(11)61351-2 |
[8, 15]
. Overall, the global burden of cancer incidence and death is quickly increasing, reflecting population aging and expansion as well as changes in the prevalence and distribution of the key cancer risk factors
| [7] | H. Sung et al., “Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA. Cancer J. Clin., vol. 71, no. 3, pp. 209–249, May 2021, https://doi.org/10.3322/CAAC.21660 |
[7]
.
Breast cancer rates are rapidly increasing in developing nations as well as in high-income Asian countries, where rates have traditionally been low. Breast cancer is the most common cancer among women in Africa as a whole. In Africa, the estimated number of new cases in 2008 was 92,600, rising to 133,900 in 2012
| [2] | J. Ferlay et al., “Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012,” Int. J. Cancer, vol. 136, no. 5, pp. E359–E386, Mar. 2015, https://doi.org/10.1002/IJC.29210 |
[2]
.
In Ethiopia, breast cancer is rapidly becoming the most frequent malignancy, with significant rates of morbidity and death. For instance, of the 4139 newly diagnosed cases of cancer registered between 2012 and 2013, 67% were female, with breast cancer accounting for 31.5%
. The age-standardized incidence rate of breast cancer was 43.3 per 100,000 females
| [10] | S. T. Memirie et al., “Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data,” J. Glob. Oncol., vol. 2018, no. 4, pp. 1–11, Mar. 2018, https://doi.org/10.1200/JGO.17.00175 |
[10]
. Incidence increased rapidly between 1997 and 2012, with a total of 3460 new cases of breast cancer, averaging 216 incident cases per year
.
The World Health Organization's Global Breast Cancer Initiative (GBCI) aimed to reduce global breast cancer mortality by 2.5 percent per year, averting 2.5 million breast cancer deaths between 2020 and 2040. Reduced global breast cancer mortality by 2.5 percent per year would prevent 25% of breast cancer deaths by 2030 and 40% by 2040 in women under the age of 70. Health promotion for early detection, timely diagnosis, and comprehensive breast cancer management are the three pillars for achieving these goals
.
Despite the fact that early diagnosis and treatment are the mainstays for the prevention of cancer-related mortality, a number of facility-based studies from developing countries show many women present with late-stage For example, women with stage III and IV disease accounted for 71.2% of breast cancer patients at the oncology units of the University of Gondar and Felege Hiwot specialized hospitals in northern Ethiopia
| [18] | F. J. Alsolami et al., “Determinants of breast cancer in Saudi women from Makkah region: A case-control study (breast cancer risk factors among Saudi women),” BMC Public Health, vol. 19, no. 1, pp. 1–8, Nov. 2019, https://doi.org/10.1186/S12889-019-7942-3/TABLES/4 |
[18]
, 77 percent of patients with breast cancer at Mulago Hospital in Uganda, and 78% of breast cancer patients at the Angolan Institute of Cancer Control center
| [18] | F. J. Alsolami et al., “Determinants of breast cancer in Saudi women from Makkah region: A case-control study (breast cancer risk factors among Saudi women),” BMC Public Health, vol. 19, no. 1, pp. 1–8, Nov. 2019, https://doi.org/10.1186/S12889-019-7942-3/TABLES/4 |
| [19] | E. Jedy-Agba, V. McCormack, C. Adebamowo, and I. dos-Santos-Silva, “Stage at diagnosis of breast cancer in sub-Saharan Africa: a systematic review and meta-analysis,” Lancet Glob. Heal., vol. 4, no. 12, pp. e923–e935, Dec. 2016, https://doi.org/10.1016/S2214-109X(16)30259-5 |
[18, 19]
.
There is no single known cause for breast cancer; however, evidence from different studies has shown that reproductive factors increase the risk of breast cancer
| [13] | A. Balekouzou et al., “Reproductive risk factors associated with breast cancer in women in Bangui: A case-control study,” BMC Womens. Health, vol. 17, no. 1, pp. 1–9, Mar. 2017, https://doi.org/10.1186/S12905-017-0368-0/TABLES/3 |
| [18] | F. J. Alsolami et al., “Determinants of breast cancer in Saudi women from Makkah region: A case-control study (breast cancer risk factors among Saudi women),” BMC Public Health, vol. 19, no. 1, pp. 1–8, Nov. 2019, https://doi.org/10.1186/S12889-019-7942-3/TABLES/4 |
[13, 18]
. Several lifestyle-related factors have also been significantly associated with breast cancer development
| [12] | H. M. Asif, S. Sultana, N. Akhtar, J. U. Rehman, and R. U. Rehman, “Prevalence, risk factors and disease knowledge of breast cancer in Pakistan,” Asian Pacific J. Cancer Prev., vol. 15, no. 11, pp. 4411–4416, 2014, https://doi.org/10.7314/APJCP.2014.15.11.4411 |
| [13] | A. Balekouzou et al., “Reproductive risk factors associated with breast cancer in women in Bangui: A case-control study,” BMC Womens. Health, vol. 17, no. 1, pp. 1–9, Mar. 2017, https://doi.org/10.1186/S12905-017-0368-0/TABLES/3 |
| [20] | Z. J. Andersen, J. T. Jørgensen, R. Grøn, E. V. Brauner, and E. Lynge, “Active smoking and risk of breast cancer in a Danish nurse cohort study,” BMC Cancer, vol. 17, no. 1, pp. 1–11, Aug. 2017, https://doi.org/10.1186/S12885-017-3546-4/TABLES/5 |
[12, 13, 20]
. In addition, studies of families with high breast cancer incidence have shown that about 5%–7% of breast carcinomas are hereditary
| [21] | H. R. Brewer, M. E. Jones, M. J. Schoemaker, A. Ashworth, and A. J. Swerdlow, “Family history and risk of breast cancer: an analysis accounting for family structure,” Breast Cancer Res. Treat., vol. 165, no. 1, pp. 193–200, Aug. 2017, https://doi.org/10.1007/S10549-017-4325-2/TABLES/4 |
[21]
.
However, in Ethiopia, limited data were found regarding risk factors associated with breast cancer. Nationally, there was no established risk factor for breast cancer in Ethiopia. The Federal Ministry of Health of Ethiopia sets a strategic objective for the prevention and control of non-communicable disease (NCD), including breast cancer, through minimizing risk factors and promoting a healthy lifestyle
| [22] | D. Ali et al., “Integrating private health facilities in government-led health systems: a case study of the public–private mix approach in Ethiopia,” BMC Health Serv. Res., vol. 22, no. 1, Dec. 2022, https://doi.org/10.1186/S12913-022-08769-7 |
[22]
.
Ethiopia's population, on the other hand, is diversified, with a vast range of lifestyles, cultures, socio-economic levels, and reproductive and breastfeeding habits. These factors can affect general health, including the risk of breast cancer
| [23] | L. Tolessa, E. G. Sendo, N. G. Dinegde, and A. Desalew, “Risk factors associated with breast cancer among women in addis ababa, ethiopia: Unmatched case–control study,” Int. J. Womens. Health, vol. 13, pp. 101–110, 2021, https://doi.org/10.2147/IJWH.S292588 |
[23]
.
In Hawassa University's comprehensive specialized hospital oncology center, breast cancer is one of the top diseases among diagnosed malignancies
. Breast cancer was found to be the most common cancer, accounting for 18.62% of all cancers registered at Hawassa University Comprehensive Specialized Hospitals (HUCSH)
| [25] | C. Marant-Micallef et al., “The risk of cancer attributable to diagnostic medical radiation: Estimation for France in 2015,” Int. J. Cancer, vol. 144, no. 12, pp. 2954–2963, Jun. 2019, https://doi.org/10.1002/IJC.32048 |
[25]
.
Despite the increasing incidence of breast cancer in Ethiopia, there has been a limited study that determines the risk factors for breast cancer. Furthermore, there was an insistence on finding different studies. Additionally, those studies that were done in Ethiopia previously in Addis Ababa recommend further research on the same area. Therefore, this study is aimed at assessing predictors of breast cancer among women attending Hawassa University's comprehensive specialized hospital.
1.3. Objectives of Study
General Objective
To examined a hospital-based matched case control study of the breast cancer risk factors for women who visit the Hawassa university comprehensive specialized hospital in Hawassa, Ethiopia, 2022.
1.4. Significance of Study
Despite the fact that early diagnosis and treatment are the mainstays for preventing cancer-related mortality, many women from developing countries, including Ethiopia, present with late-stage breast cancer. Therefore, the findings of this study will help health-care providers identify risky groups early and prioritize effective diagnostic services and appropriate treatment modalities.
Furthermore, the findings of this study can aid health policymakers in developing locally effective prevention and health promotion strategies for identified risk factors. Identifying risk factors for breast cancer can enhance early detection of breast cancer among high-risk groups through effective diagnostic technology; this will further help to achieve the health sector transformation plan (HSTP) of the Ministry of Health.
The findings of the study can add knowledge to existing body of evidence and can be used as base-line information for further study.
2. Materials and Method
2.1. Study Design and Period
A hospital based un-matched case control study design was employed from March 1 –April 30, 2022.
2.2. Study Setting
Hawassa University is one of the leading teaching institutions in Ethiopia, located in the Sidama region, 275km south of Addis Ababa. Hawassa University comprehensive specialized hospital, which was established under Hawassa University, provides health services for more than 5 million people. The hospital was established in 1991 E.C. and accommodates about 400 beds for inpatient service, of which 250 are functional
. The hospital consists of different units that provide services for the community. Oncology Center is one of the units established in 2007 E.C. under Hawassa University Comprehensive Specialized Hospital. Since its establishment, the center has provided both curative and rehabilitative services for different types of malignancies. According to the oral report of the oncology unit director, in the oncology center, a total of 1023 breast cancer patients were on follow-up in 2021. The frequency of patient visits varies by the type of treatment they are taking. Each month, on average, 79 patients with breast cancer visit the oncology center for treatment. Patients who are on hormonal treatment visit every third month, while those who are on chemotherapy therapy visit every 21 days.
2.3. Populations
2.3.1. Source Population
All women visiting the Hawassa university comprehensive specialized hospital.
2.3.2. Study Population
The cases were all women who had histologically confirmed breast cancer and visited Hawassa University's comprehensive specialized hospital during the data collection period (March 1–April 30, 2022).
Controls were all women free of breast cancer who visited Hawassa University's comprehensive specialized hospital during the study period (March 1–April 30).
Ascertainments of the cases and control
Cases of breast cancer were ascertained by reviewing documents, clinical diagnoses, and histologically confirmed evidence for breast cancer.
To ascertain control of diseases, clinical breast examinations (CBE) were performed by senior physicians before recruiting participants to study. A clinical breast examination is a very low-cost test that could improve the detection of breast cancer. Clinical breast examination, which contributes independently to mammography in the detection of breast cancer, has a sensitivity of 54% and a specificity of 94% in the detection of breast cancer. A CBE was considered abnormal in the presence of a palpable mass, nipple discharge, skin or nipple retraction, edema, erythema, or skin ulcers
| [26] | R. D. Nindrea, T. Aryandono, L. Lazuardi, and I. Dwiprahasto, “Protective Effect of Omega-3 Fatty Acids in Fish Consumption Against Breast Cancer in Asian Patients: A Meta-Analysis,” Asian Pac. J. Cancer Prev., vol. 20, no. 2, p. 327, Feb. 2019, https://doi.org/10.31557/APJCP.2019.20.2.327 |
[26]
.
2.4. Eligibility Criteria
2.4.1. Inclusion Criteria
All women aged >15 years and diagnosed with clinically and histologically confirmed breast cancer were included as cases, and controls were all women aged >15 years who came for other conditions unrelated to cancer at the Hawassa University Comprehensive Specialized Hospital during the study period.
2.4.2. Exclusion Criteria
Breast cancer cases and controls women who were critically ill and unable to provide information and control who had abnormal clinical breast examination results were excluded from the study. Cases that revisited Hawassa University during the data collection period were excluded.
2.5. Sample Size Determination
The sample was estimated based on a double population formula using Epi-Info based on the following assumptions: a confidence level of 95%, 80% power, and 1:2 ratios of cases to controls. To determine the required sample size for this study, various factors that were significantly associated with the outcome variables were considered, and the maximum sample size was taken.
Table 1. Sample size calculation based on different factor.
S.no | Confidence level (alpha) | Power of study | C-C ratio | Odd ratio | Proportion of exposure in control % | Exposure variable | Calculated sample size (Total) |
1 | 95% | 80% | 1:2 | 2.11 | 14.5 | Family history of BCA | 380 |
2 | 95% | 80% | 1:2 | 2.38 | 25% | Overweight and Obesity | 207 |
3 | 95% | 80% | 1:2 | 2.41 | 30.17 | Smoked dried meat consumption | 191 |
4 | 95% | 80% | 1:2 | 0.294 | 88.07 | Breast feeding | 140 |
5 | 95% | 80% | 1:2 | 5 | 56.36 | Physical inactivity | 69 |
Based on above table largest sample sizes determined by using Epi Info 7 Stat Calc software for unmatched case-control were 380. By adding 10% non-response rate the final sample size was 408 (136 cases and 272 controls).
2.6. Sampling Technique and Procedure
Cases were selected from confirmed breast cancer women attending Hawassa University comprehensive specialized hospital during the data collection period until the final sample size was attained. All histologically confirmed new and old cases of breast cancer who visited an oncology unit during data collection were enrolled as cases.
For each case, two controls were chosen from women over the age of 15 who were visiting the same health facility for a condition unrelated to breast cancer. A systematic random sampling technique was used to recruit controls. K was calculated using the following assumptions: The proportion of women who visited Hawassa University compressive specialized hospital during the study period was approximately identical to the previous similar period. To calculate k, the previous year's two-month population of women attending Hawassa University's comprehensive specialized hospital was divided into total numbers of controls. The total number of women who visited the hospital during the last year was 1,245 women. Dividing the total number of women by the total number of controls produces 4.46, indicating that the value of K was 4. The number 2 was chosen randomly from a list of numbers ranging from 1 to 4.
2.7. Variables
2.7.1. Dependent Variable
Presence of breast cancer.
2.7.2. Independent Variables
Socio-demographic variables such as age, educational level, occupation, household income, place of residence, and family history of breast cancer.
Behavioral and/or nutritional variables: alcohol consumption, smoking, fatty diet consumption, smoke-dried meat consumption, body mass index.
Reproductive variables like age at first birth, age at menarche, parity, breast feeding practice, use of hormonal contraceptives, and history of exposure to chemical pesticides.
Environmental and health-related variables: pesticide exposure, radiation exposure, breast trauma, history of breast infection.
2.8. Operational Definition
Menopausal status Women who met any of the following criteria were classified as post-menopausal: 1) absence of menstruation for at least 1 year (any age); 2) bilateral oophorectomy or estrogen deprivation therapy.
Active smoking was defined as smoking for more than 6 months (including former smokers). Passive smoking is defined as non-smokers who were exposed to tobacco smoking for more than 15 minutes at least once per week.
Alcohol drinking is drinking 12 ounces of ordinary beer, 5 ounces of wine, or 1.5 ounces of 80-proof distilled liquor every day.
2.9. Data Collection Tools and Procedures
A questionnaire was constructed after reviewing various pieces of literature. To collect data, a structured questionnaire was adapted from a prior study done in a similar context, and an interviewer-administered technique was employed. Breast cancer cases were identified by checking patient records. The participant's weight and height were measured using a standard scale. The questionnaire was prepared in English, translated into Amharic, and then back into English to ensure uniformity. Four professional nurses collected data, and one senior physician specializing in oncology did a clinical breast examination to ensure control of disease. One master’s health profession supervisor oversaw the entire data collection process.
2.10. Quality Control Method
The data was collected using a structured interviewer-administered questionnaire and electronic data collection techniques known as Kobo Collect. Before collecting actual data in Hawassa University Comprehensive Specialized Hospital, a pre-test was conducted on 5% (20) of the sample in Adare General Hospital. The completeness, accuracy, and consistency of the collected data were checked. The identified errors, ambiguities, and incompleteness were immediately addressed. Data collectors received one-day training to share their knowledge of the data collection instrument and how to approach study participants. Throughout the data collection period, a supervisor was assigned to monitor the data collection process.
2.10.1. Data Management, Analysis and Interpretation
The data was checked for completeness and consistency before being exported to SPSS window version 20 for statistical analysis. Descriptive statistics are used to describe a respondent's socio-demographic and other features.
To identify the factor associated with breast cancer, bivariable and multivariable logistic regression models were used. To adjust for potential confounding effects on the association, variables with p-values of 0.25 in bivariate logistic regression are fitted to the final multivariable model. The Hosmer-Lomeshow-Lomeshow of fit test was used to measure model fitness, while the variance inflating factor (VIF) was used to assess multi-collinearity. Crude Odds Ratios (COR) and Adjusted Odds Ratios (AOR) are presented with 95% confidence intervals. In the final multivariable logistic regression model, the association with breast cancer is declared significant at a p value of 0.05. Text figures and tables are used to show the results.
2.10.2. Ethical clearance
Ethical approval was received from Hawassa University's institutional review board (IRB), and a supporting official letter in the study area was obtained from Hawassa University's comprehensive specialized hospital. Respondents were asked to provide informed permission after being informed about the goal of the study, the potential risks and advantages of participation, and the right to withdraw from the study at any moment during their interview.
The confidentiality of study participants was guaranteed and safeguarded; their responses were not shared with anyone other than the study. Participants were told that if they came across a question they didn't want to answer; they could stop or move on to the next one. Participants were questioned alone with the interviewer in an area where they felt at ease. To ensure participants' trustworthiness in secrecy, codes were utilized for identification instead of study participant names. Control Participants who had abnormal clinical breast examination results during the study were advised to get additional tests for their condition.
3. Result and Discussion
3.1. Socio-demographic Characteristics of Participants
For this study, a total of 388 participants (131 cases and 257 controls) participated, with a response rate of 95% (96% in cases and 94.4% in controls). The mean age of participants is 31.7 (SD±8.03) for controls and 40.8 (SD 10.4) for cases. From the total participants, 142 (55.3%) controls and 75 (57.3%) cases are from urban residences. Regarding the occupation of participants, 64 (35.6%) of control participants and 47 (20.9%) of cases were housewives.
Of the total participants, 61 (23.7%) controls and 37 (28.2%) cases were from the Oromo ethnic group, and 64 (24.9%) controls and 17.6% of cases were from the Sidama ethnic group. Of total respondents, 194 (75.5%) of controls and 89 (67.9%) of cases were married, and 37 (14.37%) of controls and 22 (16.8%) of cases were never married. About 48 (36.6%) of cases and 18 (7%) of controls had a family history of cancer.
Table 2. Socio-demographic characteristics of participants in Hawassa university comprehensive specialized hospital, Hawassa, Ethiopia, 2022.
Variables | Controls | Breast cancer Cases | |
Residence | Rural | 115 (44.7%) | 56 (42.7%) |
Urban | 142 (55.3%) | 75 (57.3%) |
Ethnicity | Sidama | 64 (24.9%) | 23 (17.6%) |
Oromo | 61 (23.7%) | 37 (28.2%) |
Wolayta | 49 (19.1%) | 15 (11.5%) |
Hadiya | 32 (12.5%) | 6 (4.6%) |
Amhara | 10 (3.9%) | 9 (6.9%) |
Others* | 41 (15.9%) | 41 (31.3%) |
Education | No formal education | 17 (6.6%) | 34 (26.0%) |
Primary education | 95 (37.0%) | 35 (26.7%) |
Secondary education | 83 (32.3%) | 32 (24.4%) |
College and above | 62 (24.1%) | 30 (22.9%) |
Marital status | Married | 194 (75.5%) | 89 (67.9%) |
widowed | 14 (5.4%) | 16 (12.2%) |
Divorced | 12 (4.7%) | 4 (3.1%) |
Never married | 37 (14.39%) | 22 (16.8%) |
Occupation | Housewife | 64 (24.9%) | 47 (35.9%) |
Private Employee | 44 (17.1%) | 8 (6.1%) |
Farmers | 22 (8.6%) | 12 (9.2%) |
Gov’t Employers | 48 (18.7%) | 27 (20.6%) |
Daily laborer | 14 (5.4%) | 4 (3.1%) |
Merchants | 39 (15.2%) | 25 (19.1%) |
Others* | 26 (10.1%) | 8 (6.2%) |
Family History of cancer | Yes | 18 (7.0%) | 48 (36.6%) |
No | 239 (93.0%) | 83 (63.4%) |
3.2. Behavioral Characteristics of Participants
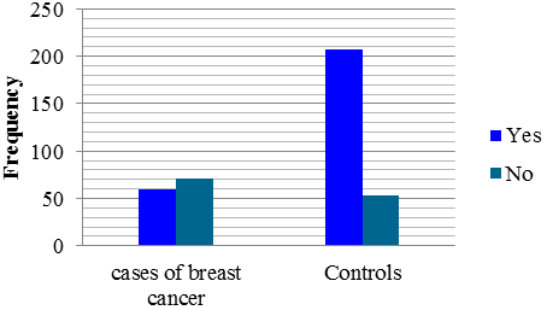
Figure 1. Fruit consumption of women in Hawassa university comprehensive specialized hospitals.
Of the total number of participants, about 166 (64.6%) of controls and 45 (34.4%) of cases engaged in physical exercise, while 193 (75.1%) of controls and 88 (67.2%) of cases engaged in home activities. The respondents mean body mass index (BMI) is 24.8 kg/m2 for cases and 25.0 kg/m2 for controls. About 7% of controls and 14% of cases used packed food or drink.
Of total participants, about 54 (21.0%) controls and 42 (32.1%) of cases consumed smoke-dried meat, while 44 (17.1%) controls and 38 (29.0%) of cases had drunk alcohol. About 71 (27.6%) of controls and 29 (22.1%) of cases have practiced their own breast self-examination. Regarding high-fat diet consumption, 230 (89.5%) controls and 121 (92.4%) cases ever consumed high-fat food. Regarding smoking, more than 99% of cases and controls were non-smokers, while 32 (12.5%) of controls and 23 (15%) of cases were exposed to secondary smoking (passive smoking), of which 25 (78.1%) of controls and 13 (56.5%) of cases were frequently exposed to secondary smoking (passive smoking).
Table 3. Behavioral and dietary related characteristics of participants in Hawassa university comprehensive specialized hospital, Hawassa, Ethiopia 2022.
Variable | Controls (257) | Cases (131) | |
Using packed food or drink | Yes | 18 (7.0%) | 19 (14.5%) |
No | 239 (93.0%) | 112 (85.5%) |
Using fatty food | Yes | 230 (89.5%) | 121 (92.4%) |
No | 27 (10.5%) | 10 (7.6%) |
Consuming smoke dried meat | Yes | 54 (21.0%) | 42 (32.1%) |
No | 203 (79.0%) | 89 (67.9%) |
Eating vegetables | Yes | 208 (80.9%) | 94 (71.8%) |
No | 49 (19.1%) | 37 (28.2%) |
Drink alcohol | Yes | 44 (17.1%) | 38 (29.0%) |
No | 213 (82.9%) | 93 (71.0%) |
Exposed to secondary smoking | Yes | 32 (12.5%) | 23 (17.6%) |
No | 225 (87.5%) | 108 (82.4%) |
Eats fruits | Yes | 204 (79.4%) | 60 (45.8%) |
No | 53 (20.6%) | 71 (54.2%) |
Ever done physical activity | Yes | 166 (64.6%) | 45 (34.4%) |
No | 91 (35.4%) | 86 (65.6%) |
Conduct household activity | Yes | 193 (75.1%) | 88 (67.2%) |
No | 64 (24.9%) | 43 (32.8%) |
Ever examined own breast | Yes | 71 (27.6%) | 29 (22.1%) |
No | 186 (72.4%) | 102 (77.9%) |
Eating sea foods (fish) | Yes | 164 (63.8%) | 33 (25.2%) |
No | 93 (36.2%) | 98 (74.8%) |
3.3. Reproductive Characteristics of Respondent
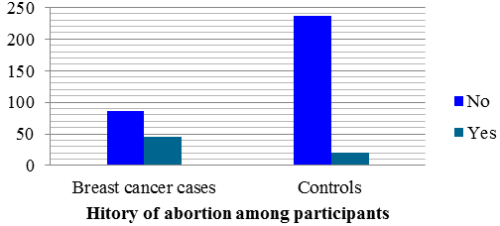
Figure 2. History of abortion among participants in Hawassa university comprehensive specialized hospitals, Ethiopia, 2022.
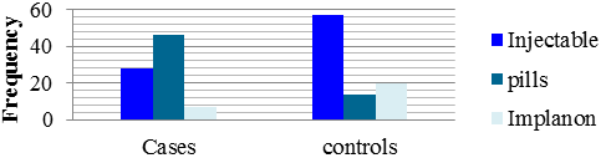
Regarding menstrual history 20 (7.8%) of controls and 29 (23.3%) of cases begin menstruation before 13 years of age. About 206 (80.2%) controls and 77 (58.8%) cases had regular menstrual cycles, 18 (7.0%) of controls, and 40 (30.5%) of cases experienced menopause. In total, 91 (35.4%) and 81 (61.8%) of controls and cases had ever used contraceptives, respectively, of which 15% of controls and 56% of cases used pills. The median duration of using hormonal contraceptives was 36 months for controls and 56 months for cases.
From total participants, 193 (75.1%) of controls and 101 (77.1%) of cases had previous history of pregnancy, and about 21 (8.2%) controls and 45 (34.4%) of cases had experienced abortions.
Among those who had a previous history of giving birth, 156 (81.2%) of the control and 68 (68.0%) of the cases had at least three children. Of the total, 178 (69.3%) of the controls and 81 (61.8%) of the cases had a history of breast-feeding their children.
Figure 3. Types of contraceptive methods used by participants in Hawassa university comprehensive specialized hospitals.
Table 4. Reproductive characteristics of participants in Hawassa University comprehensive specialized hospitals, Hawassa, Ethiopia 2022.
Variables | Controls | Cases | |
Age at menarche | ≤ 12 years | 20 (7.8%) | 29 (23.4%) |
≥ 13 years | 237 (92.2%) | 95 (76.6%) |
Ever been pregnant | Yes | 193 (75.1%) | 101 (77.1%) |
No | 64 (24.9%) | 30 (22.9%) |
Menstrual period regular | Yes | 206 (80.2%) | 77 (58.8%) |
No | 51 (19.8%) | 54 (41.2%) |
Had history of abortion | Yes | 21 (10.88%) | 45 (44.55%) |
No | 172 (89.12%) | 56 (54.45%) |
Have history of breastfeeding | Yes | 178 (92.7%) | 81 (81%) |
No | 14 (7.3%) | 19 (19%) |
Number of children participant have | ≤ 3 children | 156 (81.2%) | 68 (68.0%) |
≥ children | 36 (18.8%) | 32 (32.0%) |
Menopausal status | Premenopausal | 239 (93.0%) | 91 (69.5%) |
Menopause | 18 (7.0%) | 40 (30.5%) |
History of family planning using | Yes | 91 (35.4%) | 81 (61.8%) |
No | 166 (64.6%) | 50 (38.2%) |
Types of contraceptives | Injectable | 57 (62.6%) | 28 (34.6%) |
Pills | 14 (15.38%) | 46 (56.8%) |
Implanon | 20 (21.97%) | 7 (8.6%) |
Duration of breastfeeding per child | <12 month | 113 (63.5%) | 48 (59.3%) |
12-24 month | 53 (29.8%) | 29 (35.8%) |
>24 month | 12 (6.7%) | 4 (4.9%) |
3.4. Environmental and Health Related Characteristics of Respondents
Of the total, 49 (19.1%) controls and 52 (39.7%) had a previous history of breast infection. About 34 (13.2%) of controls and above one-fourth of 38 (29%) of cases had a history of breast injury. From the total number of participants, 56 (21.8%) of controls and 53 (40.5%) of cases had a history of previous diagnostic radiation exposure, and 50 (19.5%) of controls and 44 (33.6%) of cases had a history of pesticide exposure.
Table 5. Environmental and Health related characteristics of respondents in Hawassa University comprehensive specialized Hospitals Hawassa, Ethiopia 2022.
Variables | Controls (N= 257) | Cases of breast cancer (N=131) |
History of breast infection | Yes | 49 (19.1%) | 52 (39.7%) |
No | 208 (80.9%) | 79 (60.3%) |
Previous history of breast injury | Yes | 34 (13.2%) | 38 (29.0%) |
No | 223 (86.8%) | 93 (71.0%) |
History of radiation exposure | Yes | 56 (21.8%) | 53 (40.5%) |
No | 201 (78.2%) | 78 (59.5%) |
History of Exposure to pesticide chemical | Yes | 50 (19.5%) | 44 (33.6%) |
No | 207 (80.5%) | 87 (66.4%) |
3.5. Factor Associated with Breast Cancer Among Women Attending Hawassa University Comprehensive Specialized Hospitals
During multivariable logistic regression, after adjusting for potential confounders, age, having a family history of cancer, consuming fruits, eating sea foods (fish), using packed food or drink, using hormonal contraceptives, history of abortion, history of breast injury, and exposure to radiation from an x-ray or CT scan are significantly associated with breast cancer.
In this study, family history of having cancer has a significant association with the outcome variable. The odds of breast cancer are six times [AOR 6.05, 95% CI 1.92–19.03] higher among those who have a family history of cancer as compared to their counterparts. The odds of breast cancer are 3.34 [AOR 3.34, 955CI (1.32, 8.48)] times higher among those who don’t consume fruits as compared to those who do. Similarly, the risk of breast cancer is 76% [AOR.24, 95% CI (0.1, 0.60)] higher among those who didn’t eat sea foods (fish) as compared to those who eat sea food (fish).
Using packed food or drink is four [AOR = 4.10, 95% CI, 1.23, 13.67] times related to a higher risk of breast cancer as compared to their counterparts. Using hormonal contraceptives is approximately four [AOR, 3.86, 95% CI, 1.62, 9.24] times related to a higher risk of breast cancer as compared to their counterparts. Having a breast injury and a history of abortion were 3.29 (AOR, 3.29, 95% CI 1.20–9.01) and 3.16 (AOR, 3.16, 95% CI 1.11–9.00) times more related to higher odds of breast cancer as compared to their counterparts, respectively. The odds of breast cancer were 2.64 [AOR 2.64 95% CI, (1.14 6.15)] times higher among those who have exposure to X-ray or CT-scan radiation compared to those who are not exposed to radiation.
Table 6. Factors associated with breast cancer among women attending Hawassa university comprehensive specialized hospital, Hawassa, Ethiopia 2022.
Variables | Breast cancer | COR, 95%CI | AOR (95% CI) | | |
Yes | No |
N=131 | N =257 |
Age | <36 | 47 | 211 | 8.11 [5.079, 13.23] | 5.7 (2.11, 12.75)* |
≥36 | 84 | 46 | 1.0 | 1.0 |
Occupation | Housewife | 47 | 64 | 1.0 | 1.0 |
Private empl | 12 | 45 | .248 (.107,.575) | .51 (.12, 2.20) |
Farmers | 12 | 22 | .743 (.334, 1.649) | .56 (.13, 2.44) |
Gov’t empl | 27 | 48 | .766 (.419, 1.400) | 1.37 (.45, 4.16) |
Merchants | 25 | 39 | .873 (.466, 1.635) | .62 (.16, 2.48) |
Others | 8 | 39 | .389 (.120, 1.258) | .42 (.36, 1.5) |
Family history of cancer | Yes | 48 | 18 | 7.68 (4.23, 13.94) | 6.05 (1.92, 19.03)* |
No | 83 | 239 | 1.0 | |
physical activity | Yes | 45 | 166 | 1.0 | 1.0 |
No | 86 | 91 | 3.48 (2.24, 5.42) | 1.38 (.59, 3.23) |
Eating fruits | Yes | 60 | 204 | 1.0 | |
No | 71 | 53 | 4.55 (2.88, 7.20) | 3.34 (1.32, 8.48)* |
Smoke dried meat use | Yes | 42 | 54 | 1.77 (1.104, 2.85) | 1.85 (.70, 4.86) |
No | 89 | 203 | 1.0 | |
Eating vegetables | Yes | 94 | 208 | .598 (.366,.978) | .91 (.30, 2.74) |
No | 37 | 49 | 1 | |
consuming sea foods (fish) | Yes | 33 | 164 | .191 (.119,.305) | .24 (0.1, 0.60)* |
No | 98 | 93 | 1 | |
Using packed food or drink | Yes | 19 | 18 | 2.25 (1.14, 4.46) | 4.10 (1.23, 13.67)* |
No | 112 | 239 | 1 | |
Ever drunk Alcohol | Yes | 38 | 44 | 1.98 (1.20, 3.25) | 1.060 (.31, 3.62) |
No | 93 | 213 | 1 | |
Regular menstruation | Yes | 77 | 206 | .353 (.222,.561) | .481 (.20, 1.14) |
No | 54 | 51 | 1 | |
contraceptive use | Yes | 81 | 91 | 2.96 (1.91, 4.57) | 3.86 (1.62, 9.24)* |
No | 50 | 166 | 1.0 | |
Menstruation status | Premenopausal Menopause | 91 | 239 | .171 (.09,.31) | .708 (0.19, 2.67) |
40 | 18 | 1.0 | |
History of breastfeeding | Yes | 81 | 178 | .34 (.16,.70) | .54 (.13, 2.30 ) |
No | 19 | 14 | 1 | |
History of abortion | Yes | 45 | 21 | 6.58 (3.61, 11.98) | 3.29 (1.20, 9.01)* |
No | 56 | 172 | 1.0 | |
Age at menarche | <13 years | 29 | 20 | 3.62 (1.95, 6.70) | 1.38 (.33, 5.71) |
≥ 13 years | 95 | 237 | 1.0 | |
History of Breast injury | Yes | 38 | 34 | 2.68 (1.59, 4.52) | 3.16 (1.11, 9.00)* |
No | 93 | 223 | 1.0 | |
History of breast infection | Yes | 52 | 49 | 2.79 (1.75, 4.46) | 2.44 (.95, 6.26) |
No | 79 | 208 | 1.0 | |
Radiation exposure | Yes | 53 | 56 | 2.44 (1.54, 3.85) | 2.64 (1.14, 6.15)* |
No | 78 | 201 | 1.0 | |
Pesticide exposure | Yes | 44 | 50 | 2.09 (1.30, 3.37) | 1.95 (.74, 5.16) |
No | 87 | 207 | 1.0 | 1.0 |
3.6. Discussion
This study investigated the association of socio-economic factors, behavioral and/or dietary-related factors, reproductive factors, and environmental and health-related characteristics with breast cancer among women who visited Hawassa University's comprehensive specialized hospitals.
The study shows significant variation in the age of participants among cases and control groups. The age of participants had a significant association with breast cancer. Since there is a difference in age among cases and control participants, it is not used to compare risk among groups but is included in multivariate analysis for controlling confounding effects.
In this finding, the family history of cancer had a significant association with breast cancer. The odds of breast cancer were six times higher among those who had a family history of cancer. This finding is consistent with a study conducted in Pakistan, the United Kingdom, and Addis Ababa, which shows that the incidence of breast cancer is significantly higher among women who have a family history of breast cancer
| [21] | H. R. Brewer, M. E. Jones, M. J. Schoemaker, A. Ashworth, and A. J. Swerdlow, “Family history and risk of breast cancer: an analysis accounting for family structure,” Breast Cancer Res. Treat., vol. 165, no. 1, pp. 193–200, Aug. 2017, https://doi.org/10.1007/S10549-017-4325-2/TABLES/4 |
| [23] | L. Tolessa, E. G. Sendo, N. G. Dinegde, and A. Desalew, “Risk factors associated with breast cancer among women in addis ababa, ethiopia: Unmatched case–control study,” Int. J. Womens. Health, vol. 13, pp. 101–110, 2021, https://doi.org/10.2147/IJWH.S292588 |
| [27] | C. La Vecchia, M. Anelli, E. Zuccato, R. Fanelli, G. Sermeus, and N. Milazzo, “Perceived risk of cancer in population samples from 5 European countries,” Int. J. Cancer, vol. 86, no. 5, pp. 747–748, 2000, https://doi.org/10.1002/(ISSN)1097-0215 |
[21, 23, 27]
. This might be due to a genetic predisposition, whose function disorder is associated with an increased risk of the occurrence of malignant breast cancer. The most important genes are BRCA1 and BRCA2 (breast cancer susceptibility 1 and 2), which fulfill the function of tumor suppressor genes in a cell
.
Fruit consumption has a significant negative association with the risk of breast cancer. The odds of breast cancer were 3.44 times higher among non-consumers of fruits when compared to fruit consumers. This finding is in line with a hospital-based case-control study conducted in Guangdong, China, which shows an inverse association between vegetable and fruit intake and breast cancer risk
| [28] | C. X. Zhang, S. C. Ho, Y. M. Chen, J. H. Fu, S. Z. Cheng, and F. Y. Lin, “Greater vegetable and fruit intake is associated with a lower risk of breast cancer among Chinese women,” Int. J. Cancer, vol. 125, no. 1, pp. 181–188, Jul. 2009, https://doi.org/10.1002/IJC.24358 |
[28]
. However, the finding is inconsistent with the study done in Addis Ababa, which found no significant association between fruit consumption and the risk of breast cancer
| [29] | H. Duche, A. Tesfahun, T. & Koku, S. Tamirat, A. T. Tsegay, and K. S. Tamirat, “Identifying risk factors of breast cancer among women attending selected hospitals of addis ababa city: Hospital-based unmatched case-control study,” Breast Cancer Targets Ther., vol. 13, pp. 189–197, 2021, https://doi.org/10.2147/BCTT.S293867 |
[29]
. A possible reason for this disparity is that various populations consume different amounts and types of fruit. In our study, about 58% of participants had a history of fruit consumption, whereas a study conducted in Addis Ababa showed that around 23% of the total participants consumed fruits
| [29] | H. Duche, A. Tesfahun, T. & Koku, S. Tamirat, A. T. Tsegay, and K. S. Tamirat, “Identifying risk factors of breast cancer among women attending selected hospitals of addis ababa city: Hospital-based unmatched case-control study,” Breast Cancer Targets Ther., vol. 13, pp. 189–197, 2021, https://doi.org/10.2147/BCTT.S293867 |
[29]
.
Fruits are thought to protect against breast cancer through a variety of methods. Antioxidant vitamins, fiber, and folate are thought to be useful elements in fruits. Vitamin C, vitamin E, and carotenoids are antioxidants that protect DNA from oxidative damage. Vitamin C's function may also be connected to its effect on the immune system. In animal studies, vitamin E has been shown to suppress cancer and diminish cell growth. Furthermore, vitamin C, vitamin E, and carotenoids have chemopreventive properties. Dietary fiber may reduce the incidence of breast cancer by lowering the reabsorption of estrogen excreted in the biliary system in the stomach
.
Omega-3 fatty acids found in fish have been shown to reduce the risk of breast cancer in studies
| [26] | R. D. Nindrea, T. Aryandono, L. Lazuardi, and I. Dwiprahasto, “Protective Effect of Omega-3 Fatty Acids in Fish Consumption Against Breast Cancer in Asian Patients: A Meta-Analysis,” Asian Pac. J. Cancer Prev., vol. 20, no. 2, p. 327, Feb. 2019, https://doi.org/10.31557/APJCP.2019.20.2.327 |
[26]
. Similarly, this study shows the odds of breast cancer were 76% higher among those who didn’t consume fish, which is consistent with the above-mentioned study that reports the preventive effect of fish consumption on the risk of breast cancer. However, this finding is in contrast with a study conducted in Korea that reports no significant association between seafood consumption and the risk of breast cancer
| [30] | O. Agodirin et al., “Determinants of Delayed Presentation and Advanced-Stage Diagnosis of Breast Cancer in Africa: A Systematic Review and Meta-Analysis,” Asian Pac. J. Cancer Prev., vol. 22, no. 4, p. 1007, Apr. 2021, https://doi.org/10.31557/APJCP.2021.22.4.1007 |
[30]
. This might be due to variations in dietary habits in the study population.
This study found that using packed food or drink has a statistically significant association with breast cancer risk. The odds of breast cancer risk were four times higher among packed food or drink users as compared to their counterparts. This finding complies with a study conducted in Addis Ababa, which showed that breast cancer risk was approximately three times higher in women who consumed packaged meals or beverages
| [29] | H. Duche, A. Tesfahun, T. & Koku, S. Tamirat, A. T. Tsegay, and K. S. Tamirat, “Identifying risk factors of breast cancer among women attending selected hospitals of addis ababa city: Hospital-based unmatched case-control study,” Breast Cancer Targets Ther., vol. 13, pp. 189–197, 2021, https://doi.org/10.2147/BCTT.S293867 |
[29]
.
The study shows that hormonal contraceptive use increases the risk of breast cancer. The odds of breast cancer were 3.86 times higher among hormonal contraceptive users as compared to non-users. This finding is comparable to a study conducted in northern Algeria, Saudi Arabia, and a female nurse cohort that showed hormonal contraceptive use was linked to an increased risk of getting breast cancer
| [12] | H. M. Asif, S. Sultana, N. Akhtar, J. U. Rehman, and R. U. Rehman, “Prevalence, risk factors and disease knowledge of breast cancer in Pakistan,” Asian Pacific J. Cancer Prev., vol. 15, no. 11, pp. 4411–4416, 2014, https://doi.org/10.7314/APJCP.2014.15.11.4411 |
| [31] | D. J. Hunter et al., “Oral contraceptive use and breast cancer: A prospective study of young women,” Cancer Epidemiol. Biomarkers Prev., vol. 19, no. 10, pp. 2496–2502, Oct. 2010, https://doi.org/10.1158/1055-9965.EPI-10-0747/66522/AM/ORAL-CONTRACEPTIVE-USE-AND-BREAST-CANCER-A |
[12, 31]
. However, this finding contradicts a study conducted in Bangui, which showed that using oral hormonal contraceptives had a protective effect on the risk of breast cancer
. This might be due to the differences in socio-demographic characteristics of the study participants and their cultures. For instance, in this study, above 72% of participant women are married, while only 16.6%
of the total participants were married, since the use of hormonal contraceptives might vary among married and single women.
The study shows that having a history of abortion is significantly associated with breast cancer risk. The risk of breast cancer is 3.16 times higher among those who experienced abortion. The result is consistent with a study conducted in Bangui women that showed the risk of breast cancer was higher in women with a history of abortion
.
In this study, a prior history of breast trauma was significantly associated with a high breast cancer risk. The finding was suggested by a study conducted by Rigby et al., which shows a powerful statistical link between reported breast trauma and the development of invasive breast cancer
| [32] | A. C. G. J E Rigby, J A Morris, J Lavelle, M Stewart, “Can physical trauma cause breast cancer? on JSTOR,” JSTOR. |
[32]
. However, no clear mechanism was indicated regarding how breast injury leads to breast cancer.
X-rays, gamma rays, alpha particles, beta particles, and neutrons are examples of high-energy radiation that can damage DNA and cause cancer
| [25] | C. Marant-Micallef et al., “The risk of cancer attributable to diagnostic medical radiation: Estimation for France in 2015,” Int. J. Cancer, vol. 144, no. 12, pp. 2954–2963, Jun. 2019, https://doi.org/10.1002/IJC.32048 |
[25]
. The findings of this study suggest that the risk of breast cancer is higher among those who have had previous exposure to diagnostic radiation. The odds of having breast cancer were 2.64 times higher among those who had radiation exposure as compared to their counterparts. This finding was comparable to a study conducted in France to analyze the risk of cancer attributed to diagnostic medical radiation, which showed the top malignancies attributable to medical imaging radiation (MIR) were female breast cancer
| [25] | C. Marant-Micallef et al., “The risk of cancer attributable to diagnostic medical radiation: Estimation for France in 2015,” Int. J. Cancer, vol. 144, no. 12, pp. 2954–2963, Jun. 2019, https://doi.org/10.1002/IJC.32048 |
[25]
.
3.7. Strength and Limitation of Study
This study assessed the risk factor of breast cancer among women attending Hawassa University comprehensive specialized hospitals by case-control design. The study used a relatively large sample size and primary data, which might increase precision.
The study assessed past exposure for an outcome that might have recall bias. In this study, variables related to diet were measured based on whether the participant had a previous history of consumption or was using a specific diet or not; these might cause measurement bias. Control was selected based on the absence of clinical signs and symptoms and the absence of a previous history of breast cancer; this could lead to selection bias, but a clinical breast examination was performed by a senior physician to minimize the mixing of asymptomatic cases with control. Furthermore, this study was a facility-based study, and the findings of the study might be difficult to conclude for the general population.
3.8. Conclusion
The study found that having a family history of cancer is a risk factor for breast cancer. The risk of breast cancer was higher among those who did not consume fruits and sea food (fish) compared to their counterparts. Using packed food or drink and hormonal contraceptive use were also associated with a higher risk of breast cancer as compared to non-users. Furthermore, having a breast injury, a history of abortion, and radiation exposure were related to a higher risk of breast cancer when compared to their counterparts.
3.9. Recommendation
This study points out risk factors for breast cancer. Avoiding modifiable factors may help reduce the burden of diseases. The community should abstain from using packaged food or drink to decrease the risk of breast cancer. Health care providers should give health education to the community using different media outlets and encourage them to consume diets that have a decreased risk of breast cancer, such as fruits and fish.
Furthermore, the ministry of health should strengthen regular screening for risky groups, especially those who have a family history of cancer, older people, and those who have had radiation exposure and have used hormonal contraceptives, for early detection and treatment. Health care providers should consider the risk of radiation exposure for breast cancer, and radiation exposure should be minimized as much as possible.
Abbreviations
CBE | Clinical Breast Examination |
CDC | Center for Diseases Control |
ER | Estrogen Receptor |
GBCI | Global Breast Cancer Initiative |
GLOBOCAN | Global Cancer Statistics and Estimates |
HER2 | Human Epidermal growth factor Receptor 2 |
HSTP | Health Sector Transformation Plan |
HUCSH | Hawassa University Comprehensive Specialized Hospitals |
IACR | International Agency for Cancer Research |
IRB | Institutional Review Board |
LMIC | Low and Middle Income Countries |
NCDs | Non-communicable Diseases |
OCP | Oral Contraceptive Pills |
UK | United Kingdom |
USNC | United State National Cancer Institute |
TNM | Tumor Size Lymph Node Involvement and Metastasis |
WHO | World Health Organization |
Acknowledgments
First we would like to thanks Hawassa University college of Medicine and health science school of public health for providing us an opportunity to do this research article and we express our thankfulness to Hawassa University comprehensive specialized hospital and study participants for their cooperation and assistance by giving relevant information.
Author Contributions
Demelash Lemmi Ettisa: Conceptualization, Formal Analysis, Methodology, Project administration, Software, Writing – original draft, Writing – review & editing
Teshale Shalamo: Conceptualization, Writing – review & editing
Abdulhakim Hora: Conceptualization, Writing – review & editing
Beriso Fura: Conceptualization, Writing – review & editing
Ethical Approval
Ethical approval for this research was obtained from the relevant institutional review board.
Funding
This research received no specific grant from any funding agency in the public, commercial, or nonprofit sectors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
C. Zeng, W. Wen, A. K. Morgans, W. Pao, X. O. Shu, and W. Zheng, “Disparities by Race, Age, and Sex in the Improvement of Survival for Major Cancers: Results From the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) Program in the United States, 1990 to 2010,” JAMA Oncol., vol. 1, no. 1, pp. 88–96, Apr. 2015,
https://doi.org/10.1001/JAMAONCOL.2014.161
|
| [2] |
J. Ferlay et al., “Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012,” Int. J. Cancer, vol. 136, no. 5, pp. E359–E386, Mar. 2015,
https://doi.org/10.1002/IJC.29210
|
| [3] |
A. Fazel et al., “Marked increase in breast cancer incidence in young women: A 10-year study from Northern Iran, 2004–2013,” Cancer Epidemiol., vol. 62, p. 101573, Oct. 2019,
https://doi.org/10.1016/J.CANEP.2019.101573
|
| [4] |
R. M. Tamimi et al., “Population Attributable Risk of Modifiable and Nonmodifiable Breast Cancer Risk Factors in Postmenopausal Breast Cancer,” Am. J. Epidemiol., vol. 184, no. 12, pp. 884–893, Dec. 2016,
https://doi.org/10.1093/AJE/KWW145
|
| [5] |
K. Unger-Saldaña, “Challenges to the early diagnosis and treatment of breast cancer in developing countries,” World J. Clin. Oncol., vol. 5, no. 3, p. 465, Aug. 2014,
https://doi.org/10.5306/WJCO.V5.I3.465
|
| [6] |
F. W. Dos Santos Figueiredo, T. C. Do Carmo Almeida, J. H. M. Schoueri, C. Luisi, and F. Adami, “Association between primary care coverage and breast cancer mortality in Brazil,” PLoS One, vol. 13, no. 8, p. e0200125, Aug. 2018,
https://doi.org/10.1371/JOURNAL.PONE.0200125
|
| [7] |
H. Sung et al., “Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries,” CA. Cancer J. Clin., vol. 71, no. 3, pp. 209–249, May 2021,
https://doi.org/10.3322/CAAC.21660
|
| [8] |
M. Evelina Arzanova and P. Harvey N. Mayrovitz, “The Epidemiology of Breast Cancer,” Exon Publ., vol. 23, pp. 1–19, Aug. 2022,
https://doi.org/10.36255/EXON-PUBLICATIONS-BREAST-CANCER-EPIDEMIOLOGY
|
| [9] |
R. Sharma, “Breast cancer burden in Africa: evidence from GLOBOCAN 2018,” J. Public Health (Bangkok)., vol. 43, no. 4, pp. 763–771, Dec. 2021,
https://doi.org/10.1093/PUBMED/FDAA099
|
| [10] |
S. T. Memirie et al., “Estimates of cancer incidence in Ethiopia in 2015 using population-based registry data,” J. Glob. Oncol., vol. 2018, no. 4, pp. 1–11, Mar. 2018,
https://doi.org/10.1200/JGO.17.00175
|
| [11] |
M. Harvie, A. Howell, and D. G. Evans, “Can Diet and Lifestyle Prevent Breast Cancer: What Is the Evidence?,” Am. Soc. Clin. Oncol. Educ. B., no. 35, pp. e66–e73, May 2015,
https://doi.org/10.14694/edbook_am.2015.35.e66
|
| [12] |
H. M. Asif, S. Sultana, N. Akhtar, J. U. Rehman, and R. U. Rehman, “Prevalence, risk factors and disease knowledge of breast cancer in Pakistan,” Asian Pacific J. Cancer Prev., vol. 15, no. 11, pp. 4411–4416, 2014,
https://doi.org/10.7314/APJCP.2014.15.11.4411
|
| [13] |
A. Balekouzou et al., “Reproductive risk factors associated with breast cancer in women in Bangui: A case-control study,” BMC Womens. Health, vol. 17, no. 1, pp. 1–9, Mar. 2017,
https://doi.org/10.1186/S12905-017-0368-0/TABLES/3
|
| [14] |
P. Pisani, D. Maxwell, F. Bray, and J. Ferlay, “ESTIMATES OF THE WORLDWIDE MORTALITY FROM 25 CANCERS IN 1990,” J. Cancer, vol. 83, pp. 18–29, 1999,
https://doi.org/10.1002/(SICI)1097-0215(19990924)83:1
|
| [15] |
M. H. Forouzanfar et al., “Breast and cervical cancer in 187 countries between 1980 and 2010: A systematic analysis,” Lancet, vol. 378, no. 9801, pp. 1461–1484, Oct. 2011,
https://doi.org/10.1016/S0140-6736(11)61351-2
|
| [16] |
G. Timotewos et al., “First data from a population based cancer registry in Ethiopia,” Cancer Epidemiol., vol. 53, pp. 93–98, Apr. 2018,
https://doi.org/10.1016/J.CANEP.2018.01.008
|
| [17] |
S. M. Abate and Z. Yilma Bahir, “Trends of Breast Cancer in Ethiopia,” SciForschen, vol. 2, no. 1, 2016,
https://doi.org/10.16966/2381-3318.121
|
| [18] |
F. J. Alsolami et al., “Determinants of breast cancer in Saudi women from Makkah region: A case-control study (breast cancer risk factors among Saudi women),” BMC Public Health, vol. 19, no. 1, pp. 1–8, Nov. 2019,
https://doi.org/10.1186/S12889-019-7942-3/TABLES/4
|
| [19] |
E. Jedy-Agba, V. McCormack, C. Adebamowo, and I. dos-Santos-Silva, “Stage at diagnosis of breast cancer in sub-Saharan Africa: a systematic review and meta-analysis,” Lancet Glob. Heal., vol. 4, no. 12, pp. e923–e935, Dec. 2016,
https://doi.org/10.1016/S2214-109X(16)30259-5
|
| [20] |
Z. J. Andersen, J. T. Jørgensen, R. Grøn, E. V. Brauner, and E. Lynge, “Active smoking and risk of breast cancer in a Danish nurse cohort study,” BMC Cancer, vol. 17, no. 1, pp. 1–11, Aug. 2017,
https://doi.org/10.1186/S12885-017-3546-4/TABLES/5
|
| [21] |
H. R. Brewer, M. E. Jones, M. J. Schoemaker, A. Ashworth, and A. J. Swerdlow, “Family history and risk of breast cancer: an analysis accounting for family structure,” Breast Cancer Res. Treat., vol. 165, no. 1, pp. 193–200, Aug. 2017,
https://doi.org/10.1007/S10549-017-4325-2/TABLES/4
|
| [22] |
D. Ali et al., “Integrating private health facilities in government-led health systems: a case study of the public–private mix approach in Ethiopia,” BMC Health Serv. Res., vol. 22, no. 1, Dec. 2022,
https://doi.org/10.1186/S12913-022-08769-7
|
| [23] |
L. Tolessa, E. G. Sendo, N. G. Dinegde, and A. Desalew, “Risk factors associated with breast cancer among women in addis ababa, ethiopia: Unmatched case–control study,” Int. J. Womens. Health, vol. 13, pp. 101–110, 2021,
https://doi.org/10.2147/IJWH.S292588
|
| [24] |
H. T. Meza et al., “Impact of COVID-19 outbreak on ischemic stroke admissions and in-hospital mortality in North-West Spain,” Int. J. Stroke, vol. 15, no. 7, pp. 755–762, Oct. 2020,
https://doi.org/10.1177/1747493020938301/ASSET/IMAGES/LARGE/10.1177_1747493020938301-FIG2.JPEG
|
| [25] |
C. Marant-Micallef et al., “The risk of cancer attributable to diagnostic medical radiation: Estimation for France in 2015,” Int. J. Cancer, vol. 144, no. 12, pp. 2954–2963, Jun. 2019,
https://doi.org/10.1002/IJC.32048
|
| [26] |
R. D. Nindrea, T. Aryandono, L. Lazuardi, and I. Dwiprahasto, “Protective Effect of Omega-3 Fatty Acids in Fish Consumption Against Breast Cancer in Asian Patients: A Meta-Analysis,” Asian Pac. J. Cancer Prev., vol. 20, no. 2, p. 327, Feb. 2019,
https://doi.org/10.31557/APJCP.2019.20.2.327
|
| [27] |
C. La Vecchia, M. Anelli, E. Zuccato, R. Fanelli, G. Sermeus, and N. Milazzo, “Perceived risk of cancer in population samples from 5 European countries,” Int. J. Cancer, vol. 86, no. 5, pp. 747–748, 2000,
https://doi.org/10.1002/(ISSN)1097-0215
|
| [28] |
C. X. Zhang, S. C. Ho, Y. M. Chen, J. H. Fu, S. Z. Cheng, and F. Y. Lin, “Greater vegetable and fruit intake is associated with a lower risk of breast cancer among Chinese women,” Int. J. Cancer, vol. 125, no. 1, pp. 181–188, Jul. 2009,
https://doi.org/10.1002/IJC.24358
|
| [29] |
H. Duche, A. Tesfahun, T. & Koku, S. Tamirat, A. T. Tsegay, and K. S. Tamirat, “Identifying risk factors of breast cancer among women attending selected hospitals of addis ababa city: Hospital-based unmatched case-control study,” Breast Cancer Targets Ther., vol. 13, pp. 189–197, 2021,
https://doi.org/10.2147/BCTT.S293867
|
| [30] |
O. Agodirin et al., “Determinants of Delayed Presentation and Advanced-Stage Diagnosis of Breast Cancer in Africa: A Systematic Review and Meta-Analysis,” Asian Pac. J. Cancer Prev., vol. 22, no. 4, p. 1007, Apr. 2021,
https://doi.org/10.31557/APJCP.2021.22.4.1007
|
| [31] |
D. J. Hunter et al., “Oral contraceptive use and breast cancer: A prospective study of young women,” Cancer Epidemiol. Biomarkers Prev., vol. 19, no. 10, pp. 2496–2502, Oct. 2010,
https://doi.org/10.1158/1055-9965.EPI-10-0747/66522/AM/ORAL-CONTRACEPTIVE-USE-AND-BREAST-CANCER-A
|
| [32] |
A. C. G. J E Rigby, J A Morris, J Lavelle, M Stewart, “Can physical trauma cause breast cancer? on JSTOR,” JSTOR.
|
Cite This Article
-
APA Style
Ettisa, D. L., Shalamo, T., Hora, A., Furo, B. (2025). A Hospital-Based Matched Case Control Study Examined the Breast Cancer Risk Factors for Women Who Visit the Hawassa University Comprehensive Specialized Hospital in Hawassa, Ethiopia. Cancer Research Journal, 13(2), 56-70. https://doi.org/10.11648/j.crj.20251302.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Ettisa, D. L.; Shalamo, T.; Hora, A.; Furo, B. A Hospital-Based Matched Case Control Study Examined the Breast Cancer Risk Factors for Women Who Visit the Hawassa University Comprehensive Specialized Hospital in Hawassa, Ethiopia. Cancer Res. J. 2025, 13(2), 56-70. doi: 10.11648/j.crj.20251302.14
Copy
|
Download
AMA Style
Ettisa DL, Shalamo T, Hora A, Furo B. A Hospital-Based Matched Case Control Study Examined the Breast Cancer Risk Factors for Women Who Visit the Hawassa University Comprehensive Specialized Hospital in Hawassa, Ethiopia. Cancer Res J. 2025;13(2):56-70. doi: 10.11648/j.crj.20251302.14
Copy
|
Download
-
@article{10.11648/j.crj.20251302.14,
author = {Demelash Lemmi Ettisa and Teshale Shalamo and Abdulhakim Hora and Berisa Furo},
title = {A Hospital-Based Matched Case Control Study Examined the Breast Cancer Risk Factors for Women Who Visit the Hawassa University Comprehensive Specialized Hospital in Hawassa, Ethiopia
},
journal = {Cancer Research Journal},
volume = {13},
number = {2},
pages = {56-70},
doi = {10.11648/j.crj.20251302.14},
url = {https://doi.org/10.11648/j.crj.20251302.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.crj.20251302.14},
abstract = {Breast cancer is a type of cancer that is distinguished by the uncontrolled and abnormal growth of breast cells. Globally, it remained the most frequently diagnosed neoplastic disease in women and the leading cause of cancer-related death. Despite the increasing incidence of breast cancer in Ethiopia, there has been a limited study that determines the risk factors for breast cancer. This study employed a hospital-based matched case-control design to analyze breast cancer risk factors for women seeking care at the Hawassa University Comprehensive Specialized Hospital in Hawassa, Ethiopia. A hospital-based, unmatched case-control study design was employed from March 1 to April 30, 2022, among 131 cases and 257 control women attending Hawassa University Comprehensive Specialized Hospital. Data were collected using a standardized, pre-tested questionnaire. SPSS version 20 was used for the statistical analysis of the data. Descriptive statistics were used to summarize the socio-demographic, reproductive, and other characteristics of respondents. The bivariable and multivariable logistic regression analyses were used to assess variables associated with breast cancer and were presented with a 95% confidence interval. The final result was displayed using text figures and tables. In this study, age [AOR=5.79, 95%CI (2.11, 12.75)], family history of cancer (AOR=6.05, 95% CI (1.92 19.03), not consuming fruits (AOR=3.34, 955; CI 1.32, 8.48), eating sea foods (fish) (AOR=.24, 95% CI 0.1, 0.60), using packed food or drink (AOR= 4.10 95% CI, 1.23, 13.67), hormonal contraceptive use (AOR= 3.86 95%, CI 1.62, 9.24), having history of breast injury (AOR= 3.29 95% CI 1.20 9.01), history of abortion (AOR=3.16, 95% CI 1.11 9.00), exposure of radiation (AOR= 2.64 95% CI, 1.14 6.15) were risk factors associated with breast cancer. Having a family history of cancer, not eating fruits, not eating sea foods (fish), using packed foods or drinks, using hormonal contraception, having a history of breast injury, a history of abortion, and previous radiation exposure were all risk factors for breast cancer. Health professionals should deliver health education on the importance of a fruit and fish diet and its association with lower breast cancer risk.
},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - A Hospital-Based Matched Case Control Study Examined the Breast Cancer Risk Factors for Women Who Visit the Hawassa University Comprehensive Specialized Hospital in Hawassa, Ethiopia
AU - Demelash Lemmi Ettisa
AU - Teshale Shalamo
AU - Abdulhakim Hora
AU - Berisa Furo
Y1 - 2025/06/18
PY - 2025
N1 - https://doi.org/10.11648/j.crj.20251302.14
DO - 10.11648/j.crj.20251302.14
T2 - Cancer Research Journal
JF - Cancer Research Journal
JO - Cancer Research Journal
SP - 56
EP - 70
PB - Science Publishing Group
SN - 2330-8214
UR - https://doi.org/10.11648/j.crj.20251302.14
AB - Breast cancer is a type of cancer that is distinguished by the uncontrolled and abnormal growth of breast cells. Globally, it remained the most frequently diagnosed neoplastic disease in women and the leading cause of cancer-related death. Despite the increasing incidence of breast cancer in Ethiopia, there has been a limited study that determines the risk factors for breast cancer. This study employed a hospital-based matched case-control design to analyze breast cancer risk factors for women seeking care at the Hawassa University Comprehensive Specialized Hospital in Hawassa, Ethiopia. A hospital-based, unmatched case-control study design was employed from March 1 to April 30, 2022, among 131 cases and 257 control women attending Hawassa University Comprehensive Specialized Hospital. Data were collected using a standardized, pre-tested questionnaire. SPSS version 20 was used for the statistical analysis of the data. Descriptive statistics were used to summarize the socio-demographic, reproductive, and other characteristics of respondents. The bivariable and multivariable logistic regression analyses were used to assess variables associated with breast cancer and were presented with a 95% confidence interval. The final result was displayed using text figures and tables. In this study, age [AOR=5.79, 95%CI (2.11, 12.75)], family history of cancer (AOR=6.05, 95% CI (1.92 19.03), not consuming fruits (AOR=3.34, 955; CI 1.32, 8.48), eating sea foods (fish) (AOR=.24, 95% CI 0.1, 0.60), using packed food or drink (AOR= 4.10 95% CI, 1.23, 13.67), hormonal contraceptive use (AOR= 3.86 95%, CI 1.62, 9.24), having history of breast injury (AOR= 3.29 95% CI 1.20 9.01), history of abortion (AOR=3.16, 95% CI 1.11 9.00), exposure of radiation (AOR= 2.64 95% CI, 1.14 6.15) were risk factors associated with breast cancer. Having a family history of cancer, not eating fruits, not eating sea foods (fish), using packed foods or drinks, using hormonal contraception, having a history of breast injury, a history of abortion, and previous radiation exposure were all risk factors for breast cancer. Health professionals should deliver health education on the importance of a fruit and fish diet and its association with lower breast cancer risk.
VL - 13
IS - 2
ER -
Copy
|
Download