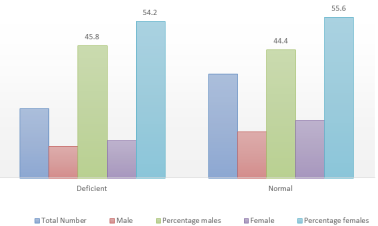
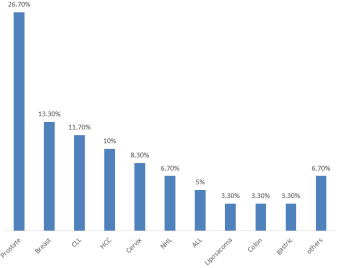
Glucose-6-phosphate dehydrogenase (G6PD) is a sensitive cytosolic antioxidant enzyme that could be associated with carcinogenesis. Hence, its plasma levels are a good indicator to monitor cancer-induced cellular stress. This study aimed to determine the correlation between Glucose-6-phosphate dehydrogenase and oxidative stress markers among cancer patients in Jos, Nigeria. This case-control study involved 100 subjects (60 cancer patients and 40 healthy control subjects). Their blood samples were collected to measure the levels of G6PD and oxidative stress markers (malondialdehyde, total plasma peroxide, total antioxidant potential, and oxidative stress indices). Twenty-four (40.0%) of the cancer patients were G6PD deficient. Of this, 13 (54.2%) were females G6PD. Of the G6PD deficient cancer patients, 11(45.8%) were male, conversely, 16 (44.4%) of the cancer subjects who had normal G6PD were males. Of the cancer patients, 26.7%; 13.3%, 11.7 % and 10% had prostate, breast cancer, chronic lymphocytic leukemia (CLL), and hepatocellular carcinoma (HCC), respectively were the most frequent. There was no significant association between G6PD deficiency and cancer (X2=0.025, p=0.804). Among G6PD deficiency cancer patients, the oxidative stress markers were significantly (p<0.05) higher compared to the control group. These findings showed that relatively more of the cancer patients had normal G6PD status even in increased cellular oxidative stress which could be due to host genetic factors. This suggests the need for further experiments on molecular characterization of mechanisms responsible for the findings.
| Published in | Cancer Research Journal (Volume 12, Issue 3) |
| DOI | 10.11648/j.crj.20241203.11 |
| Page(s) | 36-43 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Glucose-6-Phosphate Dehydrogenase, Oxidative Stress, Malondialdehyde, Plasma Peroxide, Cellular Oxidation
Parameters | Control | Cancer | P-value |
|---|---|---|---|
MDA (nmol/ml) | 0.93 ± 0.03 | 0.98 ± 0.03 | 0.267 |
TPP (µmol/L) | 83.58 ±3.64 | 95.36 ± 4.87 | 0.051 |
TAP (µmol/L) | 239.44 ± 14.04 | 189.97 ± 10.65 | 0.006* |
OSI | 41.72 ± 2.81 | 58.47 ± 7.10 | 0.015* |
GROUP | N | MDA (nmol/ml) | TPP (µmol/L) | TAP (µmol /L) | OSI |
|---|---|---|---|---|---|
A | 24 | 0.977±0.0379 | 99.664±7.659 | 190.861±18.456 | 69.508±17.707 |
B | 36 | 0.972±0.4797 | 92.779±6.351 | 189.438±13.255 | 51.843±4.057 |
C | 15 | 0.938±0.0398 | 88.938±4.985 | 232.463±22.660 | 44.407±4.526 |
D | 25 | 0.911±0.043 | 80.202±5.044 | 244.086±18.097 | 39.923±3.599 |
p value | p>0.05 | p>0.05 | p>0.05 | p>0.05 |
POST HOC | ||||
|---|---|---|---|---|
A vs B | p>0.05 | p>0.05 | p>0.05 | p>0.05 |
A vs C | p>0.05 | p>0.05 | p>0.05 | p>0.05 |
A vs D | p>0.05 | p>0.05 | p>0.05 | p>0.05 |
B vs C | p>0.05 | p<0.05* | p>0.05 | p<0.05* |
B vs D | P>0.05 | P>0.05 | P<0.05* | P<0.05* |
Parameter | Male (n=27) | Female (n=33) | P-value |
|---|---|---|---|
MDA (nmol/ml) | 0.984±0.0233 | 0.881±0.048 | p>0.05 |
TPP (µmol/L) | 86.643±4.736 | 81.067±5.382 | p>0.05 |
TAP (µmol/L) | 241.227±21.4397 | 7.972±18.850 | p>0.05 |
OSI | 43.556±4.689 | 40.212±3.415 | p>0.05 |
ANOVA | Analysis of Variance |
CLL | Chronic Lymphocytic Leukemia |
DNA | Deoxyribonucleic Acid |
EDTA | Ethylene Diamine Tetraacetic Acid |
FOX2 | Ferrous Oxidation Xylenol Orange |
G6PD | Glucose-6-phosphate Dehydrogenase |
GSH | Glutathione |
GSHPx | Glutathione Peroxidase |
Hb | Haemoglobin |
HCC | Hepatocellular Carcinoma |
H2O2 | Hydrogen Peroxide |
IDH | Isocitrate Dehydrogenase |
JUTH | Jos University Teaching Hospital |
ME | Malic Enzyme |
MDA-TBA2 | Malondialdehyde with Thiobarbituric Acid |
Hi | Methaemoglobin |
NADPH | Nicotinamide Adenine Dinucleotide Phosphate |
OSI | Oxidative Stress Index |
PPP | Pentose Phosphate Pathway |
ROS | Reactive Oxygen Species |
SD | Standard Deviation |
TBARS | Thiobarbituric Acid Reactive Substances |
TAP | Total Antioxidant Potential |
TPP | Total Plasma Peroxide |
TCA | Tricarboxylic Acid |
| [1] | Filosa, S., Fico, A., Paglialunga, F., Balestrieri, M., Crooke, A., Verde, P et al., Failure to increase glucose consumption through the pentose phosphate pathway results in the death of glucose-6-phosphate dehydrogenase gene-deleted mouse embryonic stem cells subjected to oxidative stress. Biochem J 2003; 370: 935–943. |
| [2] | Graeve, K., von Schaewen, A. and Scheibe, R. Purification, characterization, and cDNA sequence of glucose- 6-phosphate dehydrogenase from potato (Solanum tuberosum L.). Plant J. 2007 5: 353–361. |
| [3] | Hauschild, R. and von Schaewen, A. Differential regulation of glucose-6-phosphate dehydrogenase isoenzyme activities in potato. Plant Physiol. 2003 133: 47–62. |
| [4] | Turner, J. F. and Turner D. H. The regulation of glycolysis and the pentose phosphate pathway. In: Biochemistry of Plants, Stumpf PK, Conn EE (eds). New York: Academic Press; 1980 2: 279–316. |
| [5] | Fico, A., Paglialunga, F., Cigliano, L., Abrescia, P. and Verde, P. Glucose-6-phosphate dehydrogenase plays a crucial role in protection from redox-stress-induced apoptosis. Cell Death Differ. 2004 11: 823-831. |
| [6] | Efferth, T., Fabry, U., Glatte, P. and Osieka, R. Increased induction of apoptosis in mononuclear cells of a glucose-6-phosphate dehydrogenase deficient patient. J Mol. Med. 2005; 73: 47-49. |
| [7] | Kim, S. Y., Lee, S. M., Tak, J. K., Choi, K. S., Kwon, T. K. and Park, J. W. Regulation of singlet oxygen-induced apoptosis by cytosolic NADP+- dependent isocitrate dehydrogenase. Molecular Cell Biochemistry. 2007 302: 27–34. |
| [8] | Salati, L. M. and Amir-Ahmady, B. Dietary regulation of expression of glucose-6- phosphate dehydrogenase. Annu Rev Nutr. 2001 21: 121-140. |
| [9] | Cappellini, M. D. and Fiorelli, G. Glucose-6-phosphate Dehydrogenase Deficiency. Lancet. 2008; 371(9606): 64–74. |
| [10] | Nkhoma, E. T., Poole, C., Vannappagari, V., Hall, S. A. and Beutler, E. The global prevalence of glucose-6-phosphate dehydrogenase deficiency: A systematic review and meta-analysis. Blood Cells Mol Dis. 2009 42: 267-278. |
| [11] | Ruwende, C., Khoo, S. C., Snow, R. W., Yates, S. N., Kwiatkowski, D. (Natural selection of hemi- and heterozygotes for G6PD deficiency in Africa by resistance to severe malaria. Nature. 1995, 376: 246-249. |
| [12] | Ann-Joy, C., Daniel, T. C., Lai-Chu, S., Chun-Ta L., I-How, C., and Joseph T. C. Poor Prognosis in Nasopharyngeal Cancer Patients with Low Glucose-6-phosphate-dehydrogenase Activity. Jpn. J. Cancer Res2001. 92, 576–581. |
| [13] | Haggar, F., A. and Boushey R., P. Colorectal Cancer Epidemiology: incidence, mortality, survival and risk factors (Clin. colon-rectal, surgery) 2009 22(4): 191-197. |
| [14] | Giovanni, M. P., Gabrio, B. and Maria P. D. Colorectal Cancer Mortality about Glucose - 6 - Phosphate Dehydrogenase Deficiency and Consanguinity in Sardinia: A Spatial Correlation Analysis. G6PD and Colorectal Cancer. Asian Pac J Cancer Prev, 2017 18 (9), 2403-2407. |
| [15] | Egesie, O. J, Joseph, D. E., Isuguzoro, I and Egesie, U. G. Glucose 6 Phosphate dehydrogenase (G6PD) activity and deficiency in a population of Nigerian males resident in Jos; Niger J Physiol Sci.; 2008 23(1-2): 9-11. |
| [16] | Amiwero, C. E., & Olatunji, P. O. (2007). Re-evaluation of methaemoglobin reduction as a screening procedure for glucose-6-phosphate dehydrogenase (G6PD). African journal of medicine and medical sciences, 36(2), 177–181. |
| [17] | Niehans W., G and Samuelson B., A., S. Rapid method for estimation of malondialdehyde, European Journal of Bohm: 1968, 6: 126-128. |
| [18] | Benzie, I. E. and Strain J. J. The ferric reducing ability of plasma (FRAP) as a measure of antioxidant power (the FRAP assay). Annal of Biochemistry1996; 239, 70-76. |
| [19] | Oduola T, Jelani I., Bolarin D., M, Ndakotsu M., A, Dallatu M., K. Prevalence of G6PD deficiency in Sokoto: liver function and oxidative stress markers in deficient individuals: BJMMR2016 13 (11): 1-6. |
| [20] | Kanno, H. and Ogurah H. Glucose-6-phosphate dehydrogenase deficiency in Japan. Rinsho Akatsuki; 2015 56(7): 771-7. |
| [21] | Errigo, A., Bitti, A., Galistu, F., Salis, R., Pes, G. M., & Dore, M. P. (2023). Relationship between Glucose-6-Phosphate Dehydrogenase Deficiency, X-Chromosome Inactivation and Inflammatory Markers. Antioxidants (Basel, Switzerland), 12(2), 334. |
| [22] | Au, W. Y., Lam, V., Pang, A., Lee, W. M., Chan, J. L., Song, Y. Q., Ma, E. S., & Kwong, Y. L. (2006). Glucose-6-phosphate dehydrogenase deficiency in female octogenarians, nanogenarians, and centenarians. The journals of gerontology. Series A, Biological sciences and medical sciences, 61(10), 1086–1089. |
| [23] | Akiibinu M. O., Ogundahunsi A. O., Kareem O. I., Adesiyan A. A., Idonije B. O., and Adeniyi F. A. A.. Trace metals and oxidative metabolic changes in malignant prostate cancer patients. African Journal of Biochemistry Research 2011Vol. 5(3), pp. 102-105. |
| [24] | Valko, M., Leibfritz, D., Moncol, J., Cronin, M. T. D., Mazur, M. and Telser, J. Free radicals and antioxidants in normal physiological functions and human disease. Int. J. Biochem. Cell Biol; 2007 39: 44–84. |
| [25] | Pham-Huy, L. A., He, H. and Pham-Huy, C. Free radicals, antioxidants in disease and health. Int. J. Biomed. Sci. 2008 4: 89–96. |
| [26] | Sen, S., Chakraborty, R., Sridhar, C., Reddy, Y. S. R. and De, B. Free radicals, antioxidants, diseases and phytomedicines: Current status and prospect. Int. J. Pharma. Sci. Rev. Res. 2010, 3: 91–100. |
APA Style
Samuel, B. E., Dangana, A., Oduola, T., Onwuchekwa, C., Oyeniyi, Y., et al. (2024). Glucose-6-Phosphate Dehydrogenase Levels and Oxidative Stress Markers Among Cancer Patients in Jos, Nigeria. Cancer Research Journal, 12(3), 36-43. https://doi.org/10.11648/j.crj.20241203.11
ACS Style
Samuel, B. E.; Dangana, A.; Oduola, T.; Onwuchekwa, C.; Oyeniyi, Y., et al. Glucose-6-Phosphate Dehydrogenase Levels and Oxidative Stress Markers Among Cancer Patients in Jos, Nigeria. Cancer Res. J. 2024, 12(3), 36-43. doi: 10.11648/j.crj.20241203.11
AMA Style
Samuel BE, Dangana A, Oduola T, Onwuchekwa C, Oyeniyi Y, et al. Glucose-6-Phosphate Dehydrogenase Levels and Oxidative Stress Markers Among Cancer Patients in Jos, Nigeria. Cancer Res J. 2024;12(3):36-43. doi: 10.11648/j.crj.20241203.11
@article{10.11648/j.crj.20241203.11,
author = {Bwede Eugene Samuel and Amos Dangana and Taofeeq Oduola and Chinedu Onwuchekwa and Yinka Oyeniyi and Mangpin Leviticus Dansura and Villeng Felix Gagari and Mercy Ekene Mobi and Ezeama Juliet Chika and Adesuyi Ayodeji Omoare and Muhammad Sani Usman and Agwu Enoch Ojenya and Nyiri Miriam Gyang and Chinwe Ndidi Ugwu and Idris Nasir Abdullahi},
title = {Glucose-6-Phosphate Dehydrogenase Levels and Oxidative Stress Markers Among Cancer Patients in Jos, Nigeria
},
journal = {Cancer Research Journal},
volume = {12},
number = {3},
pages = {36-43},
doi = {10.11648/j.crj.20241203.11},
url = {https://doi.org/10.11648/j.crj.20241203.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.crj.20241203.11},
abstract = {Glucose-6-phosphate dehydrogenase (G6PD) is a sensitive cytosolic antioxidant enzyme that could be associated with carcinogenesis. Hence, its plasma levels are a good indicator to monitor cancer-induced cellular stress. This study aimed to determine the correlation between Glucose-6-phosphate dehydrogenase and oxidative stress markers among cancer patients in Jos, Nigeria. This case-control study involved 100 subjects (60 cancer patients and 40 healthy control subjects). Their blood samples were collected to measure the levels of G6PD and oxidative stress markers (malondialdehyde, total plasma peroxide, total antioxidant potential, and oxidative stress indices). Twenty-four (40.0%) of the cancer patients were G6PD deficient. Of this, 13 (54.2%) were females G6PD. Of the G6PD deficient cancer patients, 11(45.8%) were male, conversely, 16 (44.4%) of the cancer subjects who had normal G6PD were males. Of the cancer patients, 26.7%; 13.3%, 11.7 % and 10% had prostate, breast cancer, chronic lymphocytic leukemia (CLL), and hepatocellular carcinoma (HCC), respectively were the most frequent. There was no significant association between G6PD deficiency and cancer (X2=0.025, p=0.804). Among G6PD deficiency cancer patients, the oxidative stress markers were significantly (p0.05) higher compared to the control group. These findings showed that relatively more of the cancer patients had normal G6PD status even in increased cellular oxidative stress which could be due to host genetic factors. This suggests the need for further experiments on molecular characterization of mechanisms responsible for the findings.
},
year = {2024}
}
TY - JOUR T1 - Glucose-6-Phosphate Dehydrogenase Levels and Oxidative Stress Markers Among Cancer Patients in Jos, Nigeria AU - Bwede Eugene Samuel AU - Amos Dangana AU - Taofeeq Oduola AU - Chinedu Onwuchekwa AU - Yinka Oyeniyi AU - Mangpin Leviticus Dansura AU - Villeng Felix Gagari AU - Mercy Ekene Mobi AU - Ezeama Juliet Chika AU - Adesuyi Ayodeji Omoare AU - Muhammad Sani Usman AU - Agwu Enoch Ojenya AU - Nyiri Miriam Gyang AU - Chinwe Ndidi Ugwu AU - Idris Nasir Abdullahi Y1 - 2024/07/04 PY - 2024 N1 - https://doi.org/10.11648/j.crj.20241203.11 DO - 10.11648/j.crj.20241203.11 T2 - Cancer Research Journal JF - Cancer Research Journal JO - Cancer Research Journal SP - 36 EP - 43 PB - Science Publishing Group SN - 2330-8214 UR - https://doi.org/10.11648/j.crj.20241203.11 AB - Glucose-6-phosphate dehydrogenase (G6PD) is a sensitive cytosolic antioxidant enzyme that could be associated with carcinogenesis. Hence, its plasma levels are a good indicator to monitor cancer-induced cellular stress. This study aimed to determine the correlation between Glucose-6-phosphate dehydrogenase and oxidative stress markers among cancer patients in Jos, Nigeria. This case-control study involved 100 subjects (60 cancer patients and 40 healthy control subjects). Their blood samples were collected to measure the levels of G6PD and oxidative stress markers (malondialdehyde, total plasma peroxide, total antioxidant potential, and oxidative stress indices). Twenty-four (40.0%) of the cancer patients were G6PD deficient. Of this, 13 (54.2%) were females G6PD. Of the G6PD deficient cancer patients, 11(45.8%) were male, conversely, 16 (44.4%) of the cancer subjects who had normal G6PD were males. Of the cancer patients, 26.7%; 13.3%, 11.7 % and 10% had prostate, breast cancer, chronic lymphocytic leukemia (CLL), and hepatocellular carcinoma (HCC), respectively were the most frequent. There was no significant association between G6PD deficiency and cancer (X2=0.025, p=0.804). Among G6PD deficiency cancer patients, the oxidative stress markers were significantly (p0.05) higher compared to the control group. These findings showed that relatively more of the cancer patients had normal G6PD status even in increased cellular oxidative stress which could be due to host genetic factors. This suggests the need for further experiments on molecular characterization of mechanisms responsible for the findings. VL - 12 IS - 3 ER -
Department of Medical Laboratory Science, Ahmadu Bello University, Zaria, Nigeria
Information