Background: Malaria remains a leading public health problem in Cameroon, with the northern Sahelian region experiencing intense seasonal transmission. This study aimed to determine the prevalence and identify the determinants of malaria infection and its severity at Regional Hospital of Garoua (RHG). Methods: A hospital-based retrospective analysis was conducted between January 1, 2021, and December 31, 2023. Records of 3,506 patients with suspected malaria were reviewed. Data from 663 patients with confirmed malaria and complete files were collected and analyzed to determine malaria severity. Results: The prevalence of confirmed malaria was 30.6%. Among the analytical sample of confirmed cases, the population was predominantly male (77.4%) and young children (55.4%). Relevant determinants for malaria infection among suspected cases included age 0-6 years (aOR=3.42), rural residence (aOR=2.25), marshy area residence (aOR=2.18), and non-use of Insecticide Treated Nets (aOR=1.92). Among confirmed cases, 24.8% were severe. Determinants of severe malaria included convulsions (aOR=28.45), delayed presentation (>48h) (aOR=3.76), absence of prior consultation at another health facility (aOR=3.25), and lower paternal education level (aOR=2.85 for no formal education). Conclusion: This study confirms the high malaria burden in northern Cameroon, driven by pediatric age, environmental and seasonal exposure, and healthcare access barriers. Progression to severe disease is strongly associated with specific clinical signs, paternal education level, and care-seeking behavior.
| Published in | Central African Journal of Public Health (Volume 12, Issue 3) |
| DOI | 10.11648/j.cajph.20261203.11 |
| Page(s) | 130-140 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Malaria, Determinants, Garoua, Retrospective Study, Prevalence
Characteristic | Category | Frequency (n) | Percentage (%) |
|---|---|---|---|
Sex, | Male | 513 | 77.4 |
Female | 150 | 22.6 | |
Sex Ratio (M: F) | 3.4: 1 | ||
Age Group | 0-5 years | 367 | 55.4 |
6-20 years | 232 | 35.0 | |
21-35 years | 52 | 7.8 | |
36-65 years | 12 | 1.8 | |
Residence Type | Rural | 447 | 67.4 |
Residence Type, | Urban | 216 | 32.6 |
Environmental Exposure | Marshy Area | 384 | 57.9 |
Non-Marshy Area | 279 | 42.1 |
Parameter | Category | Number of Patients | Percentage (%) |
|---|---|---|---|
Therapeutic pathway before RHG admission | Yes | 474 | 71.5 |
No | 189 | 28.5 | |
Consultation in another Health Facility | Yes | 189 | 28.5 |
No | 474 | 71.5 |
Clinical Management Parameter | Category | Number of Patients | Percentage (%) |
|---|---|---|---|
Treatment Compliance | Yes | 656 | 98.9 |
No | 7 | 1.1 | |
Diagnostic Pathway Compliance | Yes | 653 | 98.5 |
No | 10 | 1.5 |
Factor | Category | aOR | 95% CI | p-value |
|---|---|---|---|---|
Age Group | 0-6 years | 3.42 | 2.91 – 4.01 | <0.001 |
6-20 years | 1.28 | 1.09 – 1.51 | 0.003 | |
>20 years | Ref. | |||
Residence Type | Rural | 2.25 | 1.98 – 2.56 | <0.001 |
Urban | Ref. | |||
Environmental Exposure | Marshy Area | 2.18 | 1.89 – 2.52 | <0.001 |
Non-Marshy Area | Ref. | |||
Season | Rainy Season | 1.88 | 1.62 – 2.18 | <0.001 |
Dry Season | Ref. | |||
ITNs Use | No | 1.92 | 1.61 – 2.29 | <0.001 |
Yes | Ref. | |||
Prior Consultation | Yes | 0.62 | 0.51 – 0.75 | <0.001 |
No | Ref. | |||
Father's Education | Higher | 0.58 | 0.45 – 0.75 | <0.001 |
Secondary | 0.72 | 0.57 – 0.91 | 0.006 | |
Primary | 0.85 | 0.68 – 1.06 | 0.148 | |
Ref. |
Factor | Category | aOR | 95% CI | p-value |
|---|---|---|---|---|
Clinical Symptoms | Convulsions (Present) | 28.45 | 15.80 – 51.20 | <0.001 |
Absent | Ref. | |||
Clinical Course | Delayed Presentation (>48h) | 3.76 | 2.31 – 6.11 | <0.001 |
Presentation ≤48h | Ref. | |||
Healthcare Access | No Prior FOSA Consultation | 3.25 | 1.98 – 5.33 | <0.001 |
Prior Consultation | Ref. | |||
Age Group | 0-6 years | 3.85 | 2.31 – 6.42 | <0.001 |
>20 years | Ref. | |||
Father's Education | No Formal Education | 2.85 | 1.42 – 5.72 | 0.003 |
Higher Education | Ref. | |||
ITNs Use | Non-use of ITNs | 2.18 | 1.31 – 3.61 | 0.003 |
ITNs Use | Ref. | |||
Environmental Exposure | Marshy Area | 2.05 | 1.29 – 3.26 | 0.002 |
Non-Marshy Area | Ref. | |||
Season | Rainy Season | 2.08 | 1.12 – 3.85 | 0.020 |
Dry Season | Ref. | |||
Sex | Male | 1.12 | 0.71 – 1.77 | 0.624 |
Female | Ref. |
DAMA | Discharged Against Medical Advice |
ITNs | Insecticide Treated Nets |
RHG | Regional Hospital of Garoua |
USD | United States’ Dollar |
| [1] | Obasohan PE, Walters SJ, Jacques R, Khatab K. A Scoping Review of the Risk Factors Associated with Anaemia among Children Under Five Years in Sub-Saharan African Countries. International Journal of Environmental Research and Public Health. 2020; 17: 8829. |
| [2] | World malaria report 2025: addressing the threat of antimalarial drug resistance. Geneva: World Health Organization; 2025. Licence: CC BY-NC-SA 3.0 IGO. |
| [3] | Programme National de Lutte contre le Paludisme (PNLP). Synthèse des données de surveillance en 2024. 2025. |
| [4] | Kuetche MTC, Tabue RN, Fokoua-Maxime CD, Evouna AM, Billong S, Kakesa O. Prevalence and risk factors determinants of the non-use of insecticide-treated nets in an endemic area for malaria: analysis of data from Cameroon. Malar J. Springer Science and Business Media LLC; 2023; 22. |
| [5] | Nyasa RB, Ngwa SF, Esemu SN, Titanji VPK. A Comparative Study of the Risk Factors of Malaria within Urban and Rural Settings in the Sahelian Region of Cameroon and the Role of Insecticide Resistance in Mosquitoes. Int J Trop Dis Health. 2023; 44: 43–59. |
| [6] |
National Institute of Statistics. Fifth Cameroon Household Survey: Situation of household living conditions in 2021-2022. 2024.
https://ins-cameroun.cm/wp-content/uploads/2025/07/Brochure-Ecam-5-En-1.pdf Accessed 1 Feb 2026. |
| [7] | Nembot Ndeffo L, Tene MM, Kuelah JRT, Ningaye P. Analysis of monetary and non-monetary determinants of access to education in Cameroon. Rev of economy Dev. 2013; Vol. 21: 91–125. |
| [8] | Saïdou S. Urgences Educatives à l’Extrême-Nord du Cameroun : Réponses aux Crises et Enjeux de la Scolarisation. J Educ Pract. 2025; 9: 36–50. |
| [9] | Achidi EA, Apinjoh TO, Anchang-Kimbi JK, Mugri RN, Ngwai AN, Yafi CN. Severe and uncomplicated falciparum malaria in children from three regions and three ethnic groups in Cameroon: prospective study. Malar J. 2012; 11: 215. |
| [10] | Imboumy-Limoukou RK, Lendongo-Wombo JB, Nguimbyangue-Apangome AF, Biteghe Bi Essone J-C, Mounioko F, Oyegue-Libagui LS, et al. Severe malaria in Gabon: epidemiological, clinical and laboratory features in Amissa Bongo Hospital of Franceville. Malar J. 2023; 22: 88. |
| [11] | Kwenti TE, Kwenti TDB, Njunda LA, Latz A, Tufon KA, Nkuo-Akenji T. Identification of the Plasmodium species in clinical samples from children residing in five epidemiological strata of malaria in Cameroon. Trop Med Health. 2017; 45: 14. |
| [12] | Ashaolu JO, Akanji TS, Ayansola VI, Olawale-Succes OO, Sunday AJ, Some SYM. From risk factors to predictive modelling: applying machine learning to childhood malaria surveillance in resource-limited settings. BMC Infect Dis. 2025; 25: 1693. |
| [13] | Nounouce NPJ, Zakariaou N, Marie-José E, Yollande T, Carele D, Christelle B. Prevalence and socio-economic determinants of malaria among children under five in Cameroon. Int J Community Med Public Health. 2022; 9: 603–11. |
| [14] | Kenny A, Basu G, Ballard M, Griffiths T, Kentoffio K, Niyonzima JB, et al. Remoteness and maternal and child health service utilization in rural Liberia: A population–based survey. J Glob Health. 2015; 5: 020401. |
| [15] | Nishan MDNH, Akter K. Coverage and determinants of Intermittent Preventive Treatment in pregnancy (IPTp) in Cameroon, Guinea, Mali, and Nigeria. PLOS ONE. 2024; 19: e0313087. |
| [16] | McLaren ZM, Ardington C, Leibbrandt M. Distance decay and persistent health care disparities in South Africa. BMC Health Serv Res. 2014; 14: 541. |
| [17] | Chiabi A, Djimafo ANM, Nguefack S, Mah E, Nguefack Dongmo F, Angwafo F. Severe malaria in Cameroon: Pattern of disease in children at the Yaounde Gynaeco-Obstetric and Pediatric hospital. J Infect Public Health. 2020; 13: 1469–72. |
| [18] | Mala W, Wilairatana P, Samerjai C, Masangkay FR, Kotepui KU, Kotepui M. Prevalence of Signs of Severity Identified in the Thai Population with Malaria: A Systematic Review and Meta-Analysis. Int J Environ Res Public Health. 2022; 19: 1196. |
| [19] | Zhou G, Minakawa N, Githeko A, Yan G. Spatial Distribution Patterns of Malaria Vectors and Sample Size Determination in Spatially Heterogeneous Environments: A Case Study in the West Kenyan Highland. J Med Entomol. 2004; 41: 1001–9. |
| [20] | James M, Edward M. Analysis of the Factors Influencing Healthcare Provider Choice in Rural Uganda, a Case of 2009/10 Uganda National Household Survey. Rochester, NY: Social Science Research Network; 2015. |
| [21] | Konde-Lule J, Gitta SN, Lindfors A, Okuonzi S, Onama VO, Forsberg BC. Private and public health care in rural areas of Uganda. BMC Int Health Hum Rights. 2010; 10: 29. |
| [22] | Weltgesundheitsorganisation, editor. Management of severe and complicated malaria: a practical handbook. 3. ed. Geneva: World Health Organization; 2012. |
| [23] | Macarayan E, Papanicolas I, Jha A. The quality of malaria care in 25 low-income and middle-income countries. BMJ Glob Health. 2020; 5: e002023. |
| [24] | Mousa A, Al-Taiar A, Anstey NM, Badaut C, Barber BE, Bassat Q, et al. The impact of delayed treatment of uncomplicated P. falciparum malaria on progression to severe malaria: A systematic review and a pooled multicentre individual-patient meta-analysis. PLOS Med. Public Library of Science; 2020; 17: e1003359. |
| [25] | Anjorin S, Okolie E, Yaya S. Malaria profile and socioeconomic predictors among under-five children: an analysis of 11 sub-Saharan African countries. Malar J. 2023; 22: 55. |
| [26] | Diiro GM, Affognon HD, Muriithi BW, Wanja SK, Mbogo C, Mutero C. The role of gender on malaria preventive behaviour among rural households in Kenya. Malar J. 2016; 15: 14. |
| [27] | Tesfahunegn A, Zenebe D, Addisu A. Determinants of malaria treatment delay in northwestern zone of Tigray region, Northern Ethiopia, 2018. Malar J. 2019; 18: 358. |
| [28] | Argy N, Kendjo E, Augé-Courtoi C, Cojean S, Clain J, Houzé P, et al. Influence of host factors and parasite biomass on the severity of imported Plasmodium falciparum malaria. Plos One. 2017; 12: e0175328. |
| [29] | Atieli HE, Zhou G, Afrane Y, Lee M-C, Mwanzo I, Githeko AK, et al. Insecticide-treated net (ITN) ownership, usage, and malaria transmission in the highlands of western Kenya. Parasit Vectors. 2011; 4: 113. |
| [30] | Koenker H, Taylor C, Burgert-Brucker CR, Thwing J, Fish T, Kilian A. Quantifying Seasonal Variation in Insecticide-Treated Net Use among Those with Access. Am J Trop Med Hyg. 2019; 101: 371–82. |
| [31] | Wehner S, Stieglbauer G, Traoré C, Sie A, Becher H, Müller O. Malaria incidence during early childhood in rural Burkina Faso: Analysis of a birth cohort protected with insecticide-treated mosquito nets. Acta Trop. 2017; 175: 78–83. |
APA Style
Boursou, D., Moise, A., Viviane, D. G., Bouba, G., Hermine, A. A., et al. (2026). Prevalence and Determinants of Malaria at the Regional Hospital of Garoua in the North Region of Cameroon: A Retrospective Study. Central African Journal of Public Health, 12(3), 130-140. https://doi.org/10.11648/j.cajph.20261203.11
ACS Style
Boursou, D.; Moise, A.; Viviane, D. G.; Bouba, G.; Hermine, A. A., et al. Prevalence and Determinants of Malaria at the Regional Hospital of Garoua in the North Region of Cameroon: A Retrospective Study. Cent. Afr. J. Public Health 2026, 12(3), 130-140. doi: 10.11648/j.cajph.20261203.11
@article{10.11648/j.cajph.20261203.11,
author = {Djafsia Boursou and Adamou Moise and Daiferle Godwe Viviane and Gake Bouba and Abessolo Abessolo Hermine and Okomo Marie Claire},
title = {Prevalence and Determinants of Malaria at the Regional Hospital of Garoua in the North Region of Cameroon:
A Retrospective Study},
journal = {Central African Journal of Public Health},
volume = {12},
number = {3},
pages = {130-140},
doi = {10.11648/j.cajph.20261203.11},
url = {https://doi.org/10.11648/j.cajph.20261203.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20261203.11},
abstract = {Background: Malaria remains a leading public health problem in Cameroon, with the northern Sahelian region experiencing intense seasonal transmission. This study aimed to determine the prevalence and identify the determinants of malaria infection and its severity at Regional Hospital of Garoua (RHG). Methods: A hospital-based retrospective analysis was conducted between January 1, 2021, and December 31, 2023. Records of 3,506 patients with suspected malaria were reviewed. Data from 663 patients with confirmed malaria and complete files were collected and analyzed to determine malaria severity. Results: The prevalence of confirmed malaria was 30.6%. Among the analytical sample of confirmed cases, the population was predominantly male (77.4%) and young children (55.4%). Relevant determinants for malaria infection among suspected cases included age 0-6 years (aOR=3.42), rural residence (aOR=2.25), marshy area residence (aOR=2.18), and non-use of Insecticide Treated Nets (aOR=1.92). Among confirmed cases, 24.8% were severe. Determinants of severe malaria included convulsions (aOR=28.45), delayed presentation (>48h) (aOR=3.76), absence of prior consultation at another health facility (aOR=3.25), and lower paternal education level (aOR=2.85 for no formal education). Conclusion: This study confirms the high malaria burden in northern Cameroon, driven by pediatric age, environmental and seasonal exposure, and healthcare access barriers. Progression to severe disease is strongly associated with specific clinical signs, paternal education level, and care-seeking behavior.},
year = {2026}
}
TY - JOUR T1 - Prevalence and Determinants of Malaria at the Regional Hospital of Garoua in the North Region of Cameroon: A Retrospective Study AU - Djafsia Boursou AU - Adamou Moise AU - Daiferle Godwe Viviane AU - Gake Bouba AU - Abessolo Abessolo Hermine AU - Okomo Marie Claire Y1 - 2026/05/12 PY - 2026 N1 - https://doi.org/10.11648/j.cajph.20261203.11 DO - 10.11648/j.cajph.20261203.11 T2 - Central African Journal of Public Health JF - Central African Journal of Public Health JO - Central African Journal of Public Health SP - 130 EP - 140 PB - Science Publishing Group SN - 2575-5781 UR - https://doi.org/10.11648/j.cajph.20261203.11 AB - Background: Malaria remains a leading public health problem in Cameroon, with the northern Sahelian region experiencing intense seasonal transmission. This study aimed to determine the prevalence and identify the determinants of malaria infection and its severity at Regional Hospital of Garoua (RHG). Methods: A hospital-based retrospective analysis was conducted between January 1, 2021, and December 31, 2023. Records of 3,506 patients with suspected malaria were reviewed. Data from 663 patients with confirmed malaria and complete files were collected and analyzed to determine malaria severity. Results: The prevalence of confirmed malaria was 30.6%. Among the analytical sample of confirmed cases, the population was predominantly male (77.4%) and young children (55.4%). Relevant determinants for malaria infection among suspected cases included age 0-6 years (aOR=3.42), rural residence (aOR=2.25), marshy area residence (aOR=2.18), and non-use of Insecticide Treated Nets (aOR=1.92). Among confirmed cases, 24.8% were severe. Determinants of severe malaria included convulsions (aOR=28.45), delayed presentation (>48h) (aOR=3.76), absence of prior consultation at another health facility (aOR=3.25), and lower paternal education level (aOR=2.85 for no formal education). Conclusion: This study confirms the high malaria burden in northern Cameroon, driven by pediatric age, environmental and seasonal exposure, and healthcare access barriers. Progression to severe disease is strongly associated with specific clinical signs, paternal education level, and care-seeking behavior. VL - 12 IS - 3 ER -
Department of Microbiology, University of Garoua, Garoua, Cameroon
Department of Biological Sciences, University of Ngaoundere, Ngaoundere, Cameroon
Department of Microbiology, University of Garoua, Garoua, Cameroon
Department of Microbiology, University of Garoua, Garoua, Cameroon
Department of Microbiology, University of Garoua, Garoua, Cameroon
Department of Microbiology, University of Yaounde 1, Yaounde, Cameroon
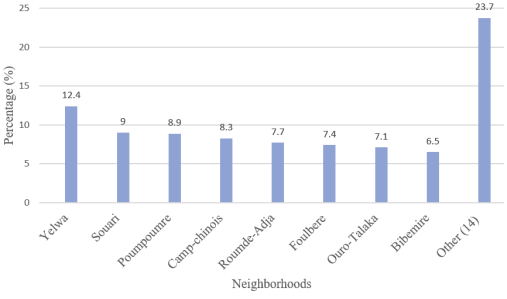
Figure 1. Distribution of attendance frequencies of patients according to the neighborhood (N= 663).
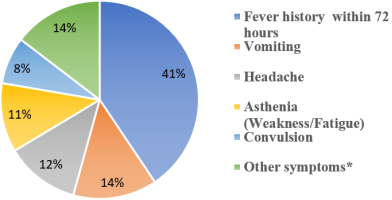
Figure 2. Frequencies of clinical symptoms of patients.
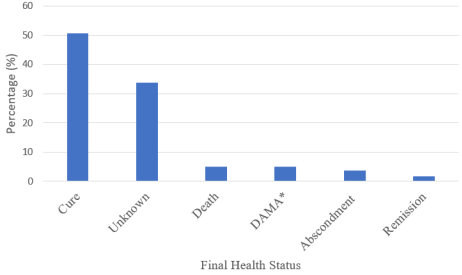
Figure 3. Distribution of patients according to the final health status (N=663).
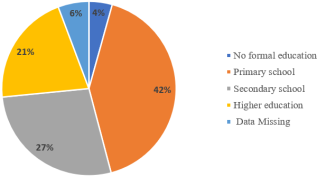
Figure 4. Distribution of patients according to the education level of the fathers (N=583).
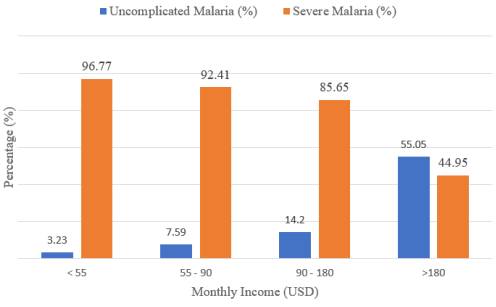
Figure 5. Comparison of severe and uncomplicated malaria with respect to the monthly income of the head of household.
Information

