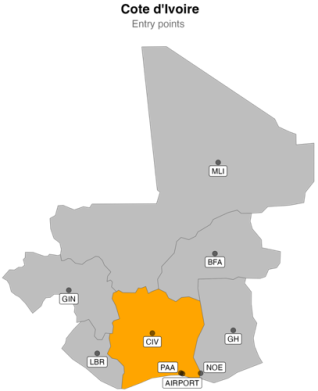
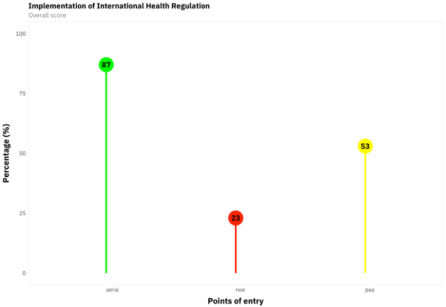
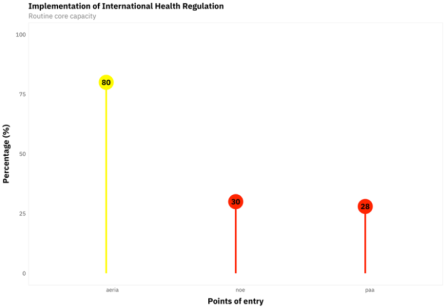
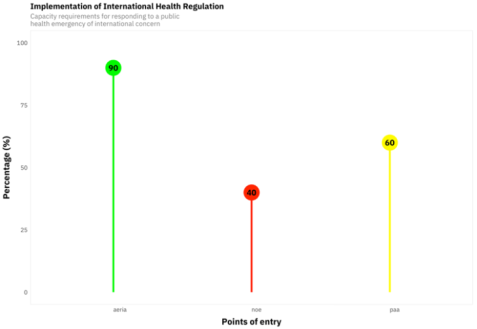
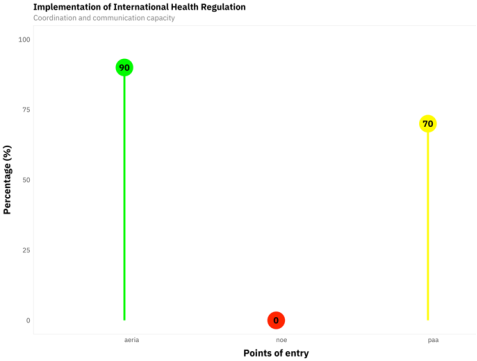
Background: rapid population growth, urbanization, and global interconnectedness have accelerated infectious disease spread, prompting WHO member states, including Côte d'Ivoire, to adopt the International Health Regulations (IHR) to strengthen surveillance, preparedness, and response at points of entry (PoE) and enhance global health security. Objective: to assess Cote d’Ivoire’s capacity to detect and respond to public health emergencies at designated points of entry (PoE), and indicate the strengths and weaknesses identified. Methods: a normative evaluation was carried out from August 1st to 30th, 2021, using the WHO tool for core capacity requirements at designated airports, ports, and ground crossings. Three PoE were selected as a purposive sample based on criteria including the type, highest volume of passengers, and international traffic. This tool collected information on three specific technical capabilities The tool generated scores for each core competency, always including routine (capacities), responding to events that might constitute a public health emergency of international concern (PHEIC), and coordination and communication. Data analysis was color-coded based on assigned scores. Results: Overall, the evaluation demonstrated that all POEs garnered a score surpassing 50%, except for the Noe crossing border (23%). AERIA obtained the highest score of 87%, following (53%). For routine capacity, PAA and Noe ground crossing border scored 28% and 30%, respectively, while AERIA scored 80%. Regarding PHEICs, the Noe ground crossing had the lowest proportion (40%). AERIA demonstrated superior strengths by virtue of the existence of comprehensive procedures and legally mandated administrative provisions for conducting inspections, the availability of sufficient medical services, and designated space to facilitate interviews with potentially infected or suspected travelers. One the opposite Noe has the most weaknesses include lack of an international communication network with competent authorities of the destination POEs, lack of simulation exercises to test the developed plans, unavailability of capacity for isolation or quarantine of sick travelers. Conclusion: Designated points of entry were not fully complied with international health regulations. Further efforts are still needed to bring designated points of entry up to RSI requirements.
| Published in | Central African Journal of Public Health (Volume 11, Issue 1) |
| DOI | 10.11648/j.cajph.20251101.12 |
| Page(s) | 16-26 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
International Sanitary Regulation, Core Capacity Requirements, Points of Entry, Cote d’Ivoire
AERIA | Aéroport International d’Abidjan |
ECOWAS | Economic Community of West Africa States |
IHR | International Health Regulations |
MDG 3 | Millenium Development Goal 3 |
NHDP | National Health Development Plan |
PAA | Port Autonome d’Abidjan |
PHEIC | Public Health Emergency of International Concern |
PoE | Points of Entry |
WHO | World Health Organization |
Core capacity | AERIA | PAA | NOE |
|---|---|---|---|
Coordination and communication | Good communication link with conveyance operators, travelers for health-related information, service providers Existence of procedures and legal and administrative provisions to conduct inspections good communication link between the airport health post and the national IHR focal point via an internal communication network for the transmission of information and recommendations from WHO | Existence legal procedures for inspections of conveyances Fair communication link with travelers for health-related information and service providers | |
Routine | Availability of a medical service Availability of equipment and personnel to enable the transport of sick/suspect passengers to an appropriate medical facility Availability of trained personnel for inspection Availability of special capacities | Availability of a medical service Availability of equipment and personnel to enable the transport of sick/suspect passengers to an appropriate medical facility Availability of trained personnel for inspection Availability of program for vectors and reservoir control and trained personnel to undertake the vector disease surveillance | Availability of trained personnel for inspection |
PHEIC | Availability of public health emergency contingency plan Availability of capacity for assessing care for affected travelers/ animals Availability of space for interview suspect/ suspect travellers Availability of capacity for isolation or quarantine of sick travellers Trained personnel on PPE use | Availability of capacity for assessing care for affected travelers/ animals Availability of space for interview suspect/ suspect travellers Trained personnel on PPE use | Availability of capacity for assessing care for affected travelers/ animals Availability of capacity for isolation or quarantine of sick travellers Trained personnel on PPE use |
Core capacity | AERIA | PAA | NOE |
|---|---|---|---|
Coordination and communication | Communication deficiency between airport authorities and local/intermediate-level health authorities. | Fair an international communication network with competent authorities of the destination POEs Fair communication link with conveyance operators Fair communication between airport authorities and local/intermediate-level health authorities Fair communication link between the seaport health post and the national IHR focal point via an internal communication network for the transmission of information and recommendations from WHO | Lack of an international communication network with competent authorities of the destination POEs Lack of communication between airport authorities and local/intermediate-level health authorities Lack of communication link between the seaport health post and the national IHR focal point via an internal communication network for the transmission of information and recommendations from WHO Lack of procedures and legal and administrative provisions to conduct inspections |
Routine | Lack of a program for vectors and reservoir control and trained personnel to undertake the vector disease surveillance | Fair hygiene of services used by travelers at the entry point Fair specialized capabilities tailored to the specific type of entry point. | Lack of a program for vectors and reservoir control and trained personnel to undertake the vector disease surveillance Lack of hygiene of services used by travelers at the entry point Lack of specialized capabilities tailored to the specific type of entry point |
PHEIC | Lack of simulation exercises to test the developed plans Lack of pre- and post-action reviews | Lack of simulation exercises to test the developed plans Lack of in- and after-action reviews Lack of capacity for isolation or quarantine of sick travellers Lack of entry and exit screenings for travelers upon arrival and departure Public health emergency contingency plan not yet approved | Lack of simulation exercises to test the developed plans Lack of pre- and post-action reviews Lack of entry and exit screenings for travelers upon arrival and departure Availability of space for interview suspect/ suspect travellers No regional center for the management of public health emergencies |
| [1] | World Health Organization. Rapport sur la santé dans le monde 2007 : un avenir plus sûr : la sécurité sanitaire mondiale au XXIè siècle. The world health report 2007: a safer future: global public health security in the 21st century [Internet]. 2007 [cited 2022 Feb 10]; Available from: |
| [2] | Youssouf T. The International Health Regulations (2005): State of Implementation in Côte D' Ivoire in 2011. SJPH. 2018; 6(3): 66. |
| [3] | Plotkin BJ, Hardiman MC. The international health regulations (2005), tuberculosis and air travel. Travel Medicine and Infectious Disease. 2010 Mar; 8(2): 90–5. |
| [4] | OMS. Règlement sanitaire international (2005). Troisième Edition. 2016 p. 89. |
| [5] | Gostin L, Katz R. The International Health Regulations: The Governing Framework for Global Health Security. Milbank Q. 2016 Jun; 94(2): 264–313. |
| [6] | Singh SK, Kumar S. International Health Regulations: a major paradigm shift from 1969 to 2005. J Commun Dis. 2009 Jun; 41(2): 113–6. |
| [7] | Rodier G, Hardiman M, Plotkin B, Ganter B. Implementing the International Health Regulations (2005) in Europe. Euro Surveill. 2006; 11(12): 208–11. |
| [8] | Sá Machado R, Abreu Santos C, Martins M, Antunes D. International Health Regulations: core capacities assessment at Points of Entry in Portugal. European Journal of Public Health. 2018 Nov 1; 28(suppl_4): cky214.271. |
| [9] |
WHO. Assessment tool for core capacity requirements at designated airports, ports and ground crossings [Internet]. 2009 [cited 2021 Dec 3]. Available from:
https://www.who.int/ihr/ports_airports/PoE_Core_capacity_assessment_tool.pdf |
| [10] | Ministère de la santé et de l’hygiène publique. Rapport Annuel sur la situation Sanitaire (RASS) 2019. 2019; 471. |
| [11] | Government Secretariat. Annex to Decree No. 2020-498 of June 10, 2020 on the control of persons at land, sea, river-lagoon, rail and air-port entry points. 2020-498 Jun 10, 2020. |
| [12] | Johns MC, Blazes DL. International Health Regulations (2005) and the U.S. Department of Defense: building core capacities on a foundation of partnership and trust. BMC Public Health. 2010 Dec 3; 10(1): S4. |
| [13] | Shehu M, Olalubi O, Sawyerr H. Assessment of Human Resources Core Capacity under International Health Regulations 2005 (Ihr 2005) At Ports of Entry (PoE) in Lagos. 2018 Sep 1; 1–08. |
| [14] | Ndoungué VF, Ngapagna AN, Kouadio SA, Djinguebey R, Gnigninanjouena O, Eyangoh S, et al. Assessing core capacities for addressing public health emergencies of international concern at designated points of entry in cameroon during the COVID-19 Pandemic. BMC Public Health. 2022 Nov 28; 22(1): 2197. |
| [15] | Singh R, Sumit K, Hossain SS. Core Capacities for Public Health Emergencies of International Concern at Ground Crossings: A Case Study from North India. Disaster med public health prep. 2020 Apr; 14(2): 214–21. |
| [16] | Taylor L. Ivory Coast rolls out Ebola vaccine after first confirmed case since 1994. BMJ. 2021 Aug 18; 374: n2047. |
| [17] | Lokossou VK, Usman AB, Sombie I, Paraiso MN, Balogun MS, Umeokonkwo CD, et al. COVID-19 pandemic in Economic Community of West African States (ECOWAS) region: implication for capacity strengthening at Point of Entry. Pan African Medical Journal [Internet]. 2021 May 25 [cited 2024 Apr 22]; 39(1). Available from: |
| [18] | Merrill RD, Rogers K, Ward S, Ojo O, Kakaī CG, Agbeko TT, et al. Responding to Communicable Diseases in Internationally Mobile Populations at Points of Entry and along Porous Borders, Nigeria, Benin, and Togo. Emerg Infect Dis. 2017 Dec; 23(Suppl 1): S114–20. |
| [19] | Ellwanger JH, Veiga ABG da, Kaminski V de L, Valverde-Villegas JM, Freitas AWQ de, Chies JAB. Control and prevention of infectious diseases from a One Health perspective. Genetics and Molecular Biology. 2021; 44: e20200256. |
| [20] | Roy A, Parida SP, Bhatia V. Role of disinfection and hand hygiene: a COVID-19 perspective. Int J Community Med Public Health. 2020; 7: 2845. |
| [21] | Gray SLA, Nyenswah TG, Sr JSMG, Amo-Addae M, Sesay HW, Babalola OJ, et al. Evaluation of the International Health Regulations core capacities at designated points of entry in Liberia, December 2019. Journal of Interventional Epidemiology and Public Health [Internet]. 2024 Feb 27 [cited 2024 Apr 23]; 7(8). Available from: |
| [22] | IOM. Assessment of core capacities at points of entry, Sri Lanka to implement international health regulations (2005) [Internet]. Sri Lanka; 2013 [cited 2024 Apr 23] p. 38. Available from: |
| [23] | Organization WH, others. WHO simulation exercise manual: a practical guide and tool for planning, conducting and evaluating simulation exercises for outbreaks and public health emergency preparedness and response. World Health Organization; 2017. |
APA Style
Akani, B. C., Traoré, Y., Douba, A., Samassi-Sokodogo, A. M., Aristide, D., et al. (2025). Assessment of Core Capacities at the Designated Points of Entry According to the International Health Regulations 2005: Cote D’Ivoire. Central African Journal of Public Health, 11(1), 16-26. https://doi.org/10.11648/j.cajph.20251101.12
ACS Style
Akani, B. C.; Traoré, Y.; Douba, A.; Samassi-Sokodogo, A. M.; Aristide, D., et al. Assessment of Core Capacities at the Designated Points of Entry According to the International Health Regulations 2005: Cote D’Ivoire. Cent. Afr. J. Public Health 2025, 11(1), 16-26. doi: 10.11648/j.cajph.20251101.12
AMA Style
Akani BC, Traoré Y, Douba A, Samassi-Sokodogo AM, Aristide D, et al. Assessment of Core Capacities at the Designated Points of Entry According to the International Health Regulations 2005: Cote D’Ivoire. Cent Afr J Public Health. 2025;11(1):16-26. doi: 10.11648/j.cajph.20251101.12
@article{10.11648/j.cajph.20251101.12,
author = {Bangaman Christian Akani and Youssouf Traoré and Alfred Douba and Awa Madaho Samassi-Sokodogo and Dionkounda Aristide and Marie Noelle Ano and Nicaise Bernadin Lépri Aka},
title = {Assessment of Core Capacities at the Designated Points of Entry According to the International Health Regulations 2005: Cote D’Ivoire
},
journal = {Central African Journal of Public Health},
volume = {11},
number = {1},
pages = {16-26},
doi = {10.11648/j.cajph.20251101.12},
url = {https://doi.org/10.11648/j.cajph.20251101.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.cajph.20251101.12},
abstract = {Background: rapid population growth, urbanization, and global interconnectedness have accelerated infectious disease spread, prompting WHO member states, including Côte d'Ivoire, to adopt the International Health Regulations (IHR) to strengthen surveillance, preparedness, and response at points of entry (PoE) and enhance global health security. Objective: to assess Cote d’Ivoire’s capacity to detect and respond to public health emergencies at designated points of entry (PoE), and indicate the strengths and weaknesses identified. Methods: a normative evaluation was carried out from August 1st to 30th, 2021, using the WHO tool for core capacity requirements at designated airports, ports, and ground crossings. Three PoE were selected as a purposive sample based on criteria including the type, highest volume of passengers, and international traffic. This tool collected information on three specific technical capabilities The tool generated scores for each core competency, always including routine (capacities), responding to events that might constitute a public health emergency of international concern (PHEIC), and coordination and communication. Data analysis was color-coded based on assigned scores. Results: Overall, the evaluation demonstrated that all POEs garnered a score surpassing 50%, except for the Noe crossing border (23%). AERIA obtained the highest score of 87%, following (53%). For routine capacity, PAA and Noe ground crossing border scored 28% and 30%, respectively, while AERIA scored 80%. Regarding PHEICs, the Noe ground crossing had the lowest proportion (40%). AERIA demonstrated superior strengths by virtue of the existence of comprehensive procedures and legally mandated administrative provisions for conducting inspections, the availability of sufficient medical services, and designated space to facilitate interviews with potentially infected or suspected travelers. One the opposite Noe has the most weaknesses include lack of an international communication network with competent authorities of the destination POEs, lack of simulation exercises to test the developed plans, unavailability of capacity for isolation or quarantine of sick travelers. Conclusion: Designated points of entry were not fully complied with international health regulations. Further efforts are still needed to bring designated points of entry up to RSI requirements.
},
year = {2025}
}
TY - JOUR T1 - Assessment of Core Capacities at the Designated Points of Entry According to the International Health Regulations 2005: Cote D’Ivoire AU - Bangaman Christian Akani AU - Youssouf Traoré AU - Alfred Douba AU - Awa Madaho Samassi-Sokodogo AU - Dionkounda Aristide AU - Marie Noelle Ano AU - Nicaise Bernadin Lépri Aka Y1 - 2025/01/16 PY - 2025 N1 - https://doi.org/10.11648/j.cajph.20251101.12 DO - 10.11648/j.cajph.20251101.12 T2 - Central African Journal of Public Health JF - Central African Journal of Public Health JO - Central African Journal of Public Health SP - 16 EP - 26 PB - Science Publishing Group SN - 2575-5781 UR - https://doi.org/10.11648/j.cajph.20251101.12 AB - Background: rapid population growth, urbanization, and global interconnectedness have accelerated infectious disease spread, prompting WHO member states, including Côte d'Ivoire, to adopt the International Health Regulations (IHR) to strengthen surveillance, preparedness, and response at points of entry (PoE) and enhance global health security. Objective: to assess Cote d’Ivoire’s capacity to detect and respond to public health emergencies at designated points of entry (PoE), and indicate the strengths and weaknesses identified. Methods: a normative evaluation was carried out from August 1st to 30th, 2021, using the WHO tool for core capacity requirements at designated airports, ports, and ground crossings. Three PoE were selected as a purposive sample based on criteria including the type, highest volume of passengers, and international traffic. This tool collected information on three specific technical capabilities The tool generated scores for each core competency, always including routine (capacities), responding to events that might constitute a public health emergency of international concern (PHEIC), and coordination and communication. Data analysis was color-coded based on assigned scores. Results: Overall, the evaluation demonstrated that all POEs garnered a score surpassing 50%, except for the Noe crossing border (23%). AERIA obtained the highest score of 87%, following (53%). For routine capacity, PAA and Noe ground crossing border scored 28% and 30%, respectively, while AERIA scored 80%. Regarding PHEICs, the Noe ground crossing had the lowest proportion (40%). AERIA demonstrated superior strengths by virtue of the existence of comprehensive procedures and legally mandated administrative provisions for conducting inspections, the availability of sufficient medical services, and designated space to facilitate interviews with potentially infected or suspected travelers. One the opposite Noe has the most weaknesses include lack of an international communication network with competent authorities of the destination POEs, lack of simulation exercises to test the developed plans, unavailability of capacity for isolation or quarantine of sick travelers. Conclusion: Designated points of entry were not fully complied with international health regulations. Further efforts are still needed to bring designated points of entry up to RSI requirements. VL - 11 IS - 1 ER -
Public Health Department, Felix Houphouet-Boigny University, Abidjan, Côte d’Ivoire
Public Health Department, Felix Houphouet-Boigny University, Abidjan, Côte d’Ivoire
Public Health Department, Felix Houphouet-Boigny University, Abidjan, Côte d’Ivoire
Public Health Department, Felix Houphouet-Boigny University, Abidjan, Côte d’Ivoire
Tackling Deadly Diseases in Africa, Abidjan, Côte d’Ivoire
Public Health Department, Felix Houphouet-Boigny University, Abidjan, Côte d’Ivoire
Public Health Department, Felix Houphouet-Boigny University, Abidjan, Côte d’Ivoire
Information