2. Observation 1
23 year old patient, mechanic, admitted with abdominal pain, vomiting, cessation of fluid and gas, abdominal distension, fever. Progression: 72 hours.
History: epigastralgia. Traditherapy (use of decoctions).
On examination: patient agitated, dry lips, hypocoloured integuments and mucous membranes. Blood pressure (BP) = 80/60 mm Hg, temperature = 38.1°C, pulse = 122. Painful abdomen, maximum in the epigastrium. Generalized parietal defensiveness. Decreased tenderness of flanks. Inaudible peristalsis. Rectal examination: Douglas bulging and painful.
Emergency workup: white blood cells 13 giga/litre, haemoglobin 11 g/dl, blood glucose 0.97 g/l.
Preoperative diagnosis: Acute generalised peritonitis due to probable perforation of peptic ulcer + shock.
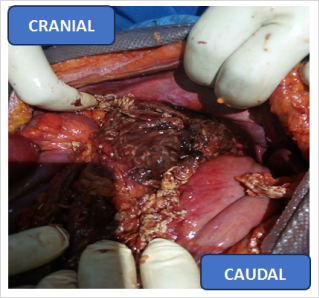
After midline laparotomy. Aspiration of 4.5 litres of odourless blackish fluid. Examination showed thickened, infiltrated large omentum and transverse colon. There were no perforations in the stomach or duodenum. Access to the omental bursa by opening the gastrocolic ligament: necrotic-haemorrhagic lesions of the pancreatic lodge infiltrating the supramesocolic stage (
Figure 1). We performed:
(1). omental biopsy for histopathological examination, sampling of peritoneal fluid for bacteriological examination. (2). Necrosectomy, cleansing and drainage of the pancreatic and subhepatic cavities.
Postoperative diagnosis: Acute necrotic-haemorrhagic pancreatitis.
Postoperative care: ceftriaxone 2 g/24H, Tramadol 100 mg/8H, perfusable Metronidazole 500 mg/8H, Omeprazole 40 mg injectable /24H. Rehydration (0.9% saline, 5% glycosylated serum, Ringer lactate, Hemacel).
Post-operative biological check-up: haemoglobin 9 g/dl, lipasemia: 180 U/L, blood glucose: 1.2 g/l, blood calcium: 3 mmol/l.
Post-operative follow-up: oedema of lower limbs, fever to 39°C, parietal then deep suppuration, evisceration. At 30 days post-op acute generalised peritonitis + evisceration of necrotic-haemorrhagic pancreatitis. Intraoperatively we noted total necrosis of the pancreas and deposits of false membranes in places. We performed a necrosectomy and peritoneal lavage. During these procedures, the patient died on the operating table from probable septic shock, with multiple organ failure.
Figure 1. Operating view Pancreatic necrosis.
3. Observation 2
60 year old patient, sailor, admitted for sudden epigastric pain after a meal, radiating to the bar and back, nausea, cessation of bowel movements and gas, fever. Progression 22 hours. Chronic alcoholic-smoker.
On examination: BP =110/70 mmHg, pulse = 86, temperature = 38.5°C, respiratory rate =24 cycles/minute. General condition satisfactory, normal-coloured integument and mucous membranes, active posture. Abdomen only slightly involved in breathing, painful overall with a maximum in the umbilical region, epigastrium, right hypochondrium and right flank with parietal defence. Prehepatic dullness preserved. No sloping flank fat. Free hernial orifices. Elsewhere no particularities.
ASP: diffuse aerocolia with pneumatisation of the distal portion of the digestive tract without hydroaeric images.
Abdominal ultrasound: moderate peritoneal fluid effusion in the perivesicular, intervesical and Douglas areas, suggesting probable peritonitis due to gastric perforation. Homogeneous hepatomegaly with no abnormalities of the bile ducts or portal trunk. Absence of pancreatic and spleno-renal morphological lesions.
Biology: hyperleukocytosis of 12.8 giga/litre, positive retroviral serology, haemoglobin level: 14 g/litre, blood glucose: 1.31 g/litre, blood group B+.
Preoperative diagnosis: acute generalised peritonitis due to perforation of a gastroduodenal ulcer, probably? in a human immunodeficiency virus (HIV) infection.
After median supra and sub umbilical laparotomy. Aspiration of 200 ml of haematic fluid. Investigation showed local ‘candle spot’ lesions and necrotic and haemorrhagic areas in the pancreatic cavity (
Figure 1). Peritoneal lavage with 4 litres of 0.9% SS. Placement of a drain in the omental bursa through the omental foramen, brought out by a counter incision under the right rib. Parietal closure.
Postoperative diagnosis: Acute necrotic-haemorrhagic pancreatitis with HIV (Human immunodeficiency Virus).
The postoperative course was favourable under treatment: rehydration with 1.5 litres of fluids (LR, 0.9% saline, 5% glycosylated serum) / 24 hours, atropine 0.5 mg, perfusable paracetamol 1 g, ceftriaxone 2 g/24H, metronidazole 500 mg perfusable /8H, omeprazole 40 mg injectable /24H, fat-free refeeding. Post-operative follow-up at 11 days post-op revealed genital herpes which was treated, after a dermatological consultation, with aciclovir 200 mg, Betadine scrub and dermal betadine. The patient was seen again at 20 days with good clinical progress. The surgical wound was healing well. A biological check-up: lipasemia, glycaemia, transaminases, was unremarkable.
4. Discussion
Severe acute pancreatitis is one of the most serious digestive disorders. It is a medical and surgical emergency
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
[2]
. Severe forms of acute pancreatitis are defined by the occurrence of visceral failure or necrosis and superinfection of the necrosis, or pseudocysts or abscesses
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
[1]
. In our two (2) cases, the necrotic-haemorrhagic form was discovered in the context of an acute peritoneal syndrome caused by perforation of a gastroduodenal ulcer.
The probable causes of the acute necrotic-haemorrhagic pancreatitis were alcoholic (observation 2) and unknown (observation 1).
Terrain is a prognostic factor. Elements of severity are: age ˃ 50 years, obesity (Body Mass Index BMI ˃30), visceral failure (respiratory, cardiac, renal), hypovolaemic shock (haemodynamic visceral failure)
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
[1, 2]
.
In the first case, our patient was young (under 50 years of age), not obese, and had no particular history suggesting a pancreatic origin. However, he was admitted in a state of shock, reflecting very marked visceral failure. The risk factors are correlated with the aetiologies, the main ones being alcohol and lithiasis
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
[1]
.
The clinical investigation in the first case did not reveal any alcoholic or lithiasis-related aetiology. It was an idiopathic necrotic-hemorrhagic pancreatitis. Only 5-10% of cases of PANH in adults remain unexplained
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
[1]
.
In the second case, the patient was aged 60 (over 50). The main risk factor was alcohol intoxication
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
[1, 2]
for more than 20 years in a specific HIV setting. He had been on antiretroviral therapy (Emtricitabine/Tenofovir Disoproxil) for about 10 years.
The etiologies were dominated by biliary lithiasis (45%) and alcohol intoxication (35%)
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
[1, 2]
.
From a pathophysiological point of view, early organ failure associated with hypovolaemia determines late necrotic superinfection, due to the existence of mesenteric hypoperfusion associated with bacterial translocation
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
[1]
.
However, the clinical features (diffuse pain with a maximum in the epigastrium, vomiting, cessation of bowel movements and gas) led to the diagnosis of acute generalised peritonitis due to perforation of a gastroduodenal ulcer in both cases.
Biological tests showed a hyperleukocytosis with neutrophilic polymorphonuclear cells.
In both cases, the unprepared abdomen X-ray was non-contributory. Abdominal computed tomography was not performed because it was not available urgently in our context. The standard techniques (unprepared abdominal X-ray and chest X-ray) are still of definite value in diagnosing complications (peritonitis, pleurisy, etc.): rule out pneumoperitoneum due to perforation or intestinal ischaemia
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [3] | Pupelis G, Fokin V, Zeiza K, Kazaka I, Pereca J, Skuja V, et al. Ultrasound assisted focused open necrosectomy in the treatment of necrotizing pancreatitis. JOP. 2015; 20; 16(2): 15 158. |
[1, 3]
. PSA may show evidence of PANH (calcium-toned image in the vesicular or pancreatic area).
Abdominopelvic CT scans can identify changes in the pancreas (homogeneous enlargement of the pancreas, areas of necrosis, peripancreatic flows)
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
| [3] | Pupelis G, Fokin V, Zeiza K, Kazaka I, Pereca J, Skuja V, et al. Ultrasound assisted focused open necrosectomy in the treatment of necrotizing pancreatitis. JOP. 2015; 20; 16(2): 15 158. |
[2, 3]
.
Infection of the necrosis occurs after the first week or two. It is the cause of multiple visceral failures and, in the absence of effective eradication, the majority of deaths
| [4] | Hackert T, Büchler MW. Decision making in necrotizing pancreatitis. Dig Dis. 2016; 34(5): 51 24. |
[4]
. The presence of air bubbles within the necrosis on CT scan is a good sign, supporting the diagnosis of infection of the necrosis when it reaches 30% of the gland
| [3] | Pupelis G, Fokin V, Zeiza K, Kazaka I, Pereca J, Skuja V, et al. Ultrasound assisted focused open necrosectomy in the treatment of necrotizing pancreatitis. JOP. 2015; 20; 16(2): 15 158. |
[3]
. This necrosis is an important prognostic factor
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [4] | Hackert T, Büchler MW. Decision making in necrotizing pancreatitis. Dig Dis. 2016; 34(5): 51 24. |
[1, 4]
.
Computed tomography (CT) is the reference examination that provides the most information about the severity of pancreatitis and predicts the occurrence of complications and mortality
| [3] | Pupelis G, Fokin V, Zeiza K, Kazaka I, Pereca J, Skuja V, et al. Ultrasound assisted focused open necrosectomy in the treatment of necrotizing pancreatitis. JOP. 2015; 20; 16(2): 15 158. |
| [4] | Hackert T, Büchler MW. Decision making in necrotizing pancreatitis. Dig Dis. 2016; 34(5): 51 24. |
[3, 4]
.
The diagnostic approach has 3 objectives: - to make a positive diagnosis on the basis of the characteristics of the epigastric pain, the lipasemia assay (essentially), and radiological investigations;
1) Assess the initial severity (bioclinical and radiological scores);
2) look for local, loco-regional and systemic complications
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [4] | Hackert T, Büchler MW. Decision making in necrotizing pancreatitis. Dig Dis. 2016; 34(5): 51 24. |
| [6] | Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014 Feb; 109(2): 302]. Am J Gastroenterol. 2013; 108(9): 140 16. |
[1, 4, 6]
.
In both cases, the diagnosis of necrotic-haemorrhagic pancreatitis was made intraoperatively by the discovery of:
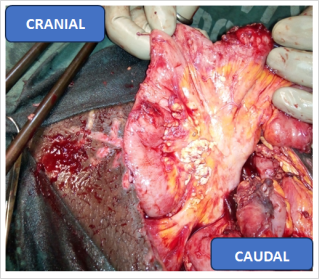
1) candle stains on the omental apron, (
Figure 2).
2) necrotic-haemorrhagic lesions of the pancreatic cavity in a context of acute generalised peritonitis (
Figure 1).
3) Peritoneal fluid effusion reflects visceral failure, which is responsible for systemic haemodynamic, respiratory, renal, haematological and metabolic complications (shock)
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
| [6] | Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014 Feb; 109(2): 302]. Am J Gastroenterol. 2013; 108(9): 140 16. |
[5, 6]
, as in our observations.
Figure 2. Operating view Candle stains.
Local complications include pancreatic necrosis. Superinfection of pancreatic necrosis has a decisive influence on the local course and prognosis
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [4] | Hackert T, Büchler MW. Decision making in necrotizing pancreatitis. Dig Dis. 2016; 34(5): 51 24. |
| [6] | Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014 Feb; 109(2): 302]. Am J Gastroenterol. 2013; 108(9): 140 16. |
[1, 4, 6]
. Diagnosis of the severity of PANH depends on the aetiology, the patient's condition, associated pathologies and pancreatic lesions, particularly necrosis and superinfection
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
| [4] | Hackert T, Büchler MW. Decision making in necrotizing pancreatitis. Dig Dis. 2016; 34(5): 51 24. |
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
| [6] | Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014 Feb; 109(2): 302]. Am J Gastroenterol. 2013; 108(9): 140 16. |
[2, 4-6]
.
The surgical indications for PANH are: superinfection of necrosis (a serious factor), pseudocysts, haemorrhage, perforation, and treatment of the aetiology
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
| [7] | Logue JA, Carter CR. Minimally invasive necrosectomy techniques in severe acute pancreatitis: role of percutaneous necrosectomy and video-assisted retroperitoneal debridement. Gastroenterol Res Pract. 2015; 2015: 693040 (ESGE) evidence-based multidisciplinary guidelines. Endoscopy. 2018; 50(5): 52 46. |
[1, 2, 5, 7]
.
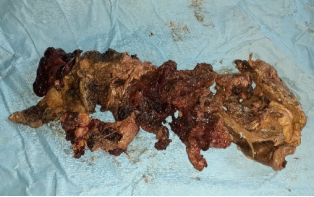
In our context, the indication was, a fortiori, pancreatic necrosis in both cases (
Figure 3).
Figure 3. Surgical specimen of pancreatic necrosis.
Management was multidisciplinary (anaesthesia-intensive care, surgery, radiology and microbiology): surgery for sterile necrosis, indication for biliary surgery and endoscopic retrograde cholangiopancreatography (ERCP)
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
| [7] | Logue JA, Carter CR. Minimally invasive necrosectomy techniques in severe acute pancreatitis: role of percutaneous necrosectomy and video-assisted retroperitoneal debridement. Gastroenterol Res Pract. 2015; 2015: 693040 (ESGE) evidence-based multidisciplinary guidelines. Endoscopy. 2018; 50(5): 52 46. |
[5, 7]
.
Treatment was surgical. Treatment consisted of drainage, omental biopsy (necrosis) and bacteriological sampling of the peritoneal fluid. Bacteriological analysis isolated ceftriaxone-sensitive Staphylococcus aureus.
Treatment of infection of the necrosis is based on transparietal radiological drainage
| [7] | Logue JA, Carter CR. Minimally invasive necrosectomy techniques in severe acute pancreatitis: role of percutaneous necrosectomy and video-assisted retroperitoneal debridement. Gastroenterol Res Pract. 2015; 2015: 693040 (ESGE) evidence-based multidisciplinary guidelines. Endoscopy. 2018; 50(5): 52 46. |
[7]
, surgical necrosectomy
| [8] | Lucia Ilaria Sgaramella, Angela Gurrado, Alessandro Pasculli, Francesco Paolo Prete, Fausto Catena et Mario Testin. La nécrosectomie ouverte est réalisable en dernier recours dans des cas sélectionnés de nécrose pancréatique infectée: une série de cas et une revue systématique de la littérature. World Journal of Emergency Surgery (2020) 15: 44 https://doi.org/10.1186/s1301020032z |
| [9] | Wroński M, Cebulski W, Witkowski B, Jankowski M, Kluciński A, Krasnodębski IW, et al. Comparaison entre le traitement chirurgical mini-invasif et ouvert dans la pancréatite nécrosante. J Surg Res. 2017; 210: 2 31. |
[8, 9]
(
Figure 3) or endoscopic necrosectomy
| [10] | Arvanitakis M, Dumonceau JM, Albert J, Badaoui A, Bali MA, Barthet M, et al. Endoscopic management of acute necrotizing pancreatitis: Société européenne d'endoscopie gastro-intestinale. |
| [11] | Haney CM, Kowalewski KF, Schmidt MW, Koschny R, Felinska EA, Kalkum E, et al. Endoscopic versus surgical treatment for infected necrotizing pancreatitis: a systematic review and meta-analysis of randomized controlled trials. Surg Endosc. 2020; 34(6): 242 44. |
[10, 11]
. Appropriate antibiotic therapy, in terms of bacteriology and pharmacokinetics, may be justified early on in severe cases
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [4] | Hackert T, Büchler MW. Decision making in necrotizing pancreatitis. Dig Dis. 2016; 34(5): 51 24. |
| [12] | Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013; 62(1): 10 11. |
[1, 4, 12]
. In both cases, drainage was surgical, combined with antibiotic therapy (ceftriaxone 2 g/24hrs, metronidazole 500 mg 1.5 g/24hrs) and rehydration (9% saline, Ringer lactate) 2 L/24hrs.
The other therapeutic options (radiological and endoscopic) are not commonly used in emergencies in our context.
In the first observation, the post-operative course was riddled with septic complications on postoperative day 12: purulent fluid flow through the drains, into the pancreatic cavity and the subhepatic cavity, through the median wound responsible for evisceration, fever, progressive weight loss. Superinfection of the necrosis may occur early (1-2 weeks) in 25-30% of cases, but the maximum risk is observed during the 3rd week
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
| [6] | Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014 Feb; 109(2): 302]. Am J Gastroenterol. 2013; 108(9): 140 16. |
[1, 5, 6]
. This risk increased during the 2nd week in our first observation
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
[1, 2]
. Superinfection of the necrosis is a serious complication from the 2nd week onwards, revealed by a septic syndrome that can be confirmed by radioguided puncture + bacteriological examination
| [13] | Mäkelä J. T., Eila H., Kiviniemi H., Laurila J., Laitinen S. Computed tomography severity index and C-reactive protein values predicting mortality in emergency and intensive care units for patients with severe acute pancreatitis. Am J Surg, 2007; 194: 3 4. |
[13]
.
Post-operative biological monitoring revealed: lipasemia ˃ 3N, anaemia at 8 g/L (a blood transfusion was carried out). Iterative clinical controls led to an indication for repeat surgery for post-operative generalised acute peritonitis plus Evisceration. The total necrosis of the pancreas found in the first observation may reflect the severity of the superinfection, a consequence of the delay in management
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
| [6] | Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014 Feb; 109(2): 302]. Am J Gastroenterol. 2013; 108(9): 140 16. |
| [12] | Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013; 62(1): 10 11. |
[5, 6, 12]
.
Secondary complications such as diabetes and exocrine pancreatic insufficiency are correlated with the extent of necrosis
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [13] | Mäkelä J. T., Eila H., Kiviniemi H., Laurila J., Laitinen S. Computed tomography severity index and C-reactive protein values predicting mortality in emergency and intensive care units for patients with severe acute pancreatitis. Am J Surg, 2007; 194: 3 4. |
[1, 13]
. This makes the prognosis more guarded
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
[1, 5]
.
Lipasemia is produced and secreted exclusively by the pancreas. It is the best, most specific and most sensitive biological test for diagnosing acute pancreatitis
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
[1, 2, 5]
.
Surgical treatment of complications (superinfection of necrosis, haemorrhage) remains cumbersome, with a high morbidity and mortality rate
| [14] | E Allah-kouadio, M Diakité, S koné. Pancréatite aigue nécrotico-hémorragique révélée par une hémorragie digestive haute par rupture de varices œsophagienne. Rev Int Sc Méd 2013; 15, 2: 10 103. |
[14]
. In the first observation, death occurred intraoperatively. It was caused by septic shock, probably due to superinfection of the total necrosis of the pancreas (poly-visceral failure). The main cause of death is (infection of the necrotic tissue, which is associated with a poor prognosis
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
| [12] | Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013; 62(1): 10 11. |
[5, 12]
. In our case, the duration of the pancreatitis (72 hours) and the use of traditional decoctions would have been factors in the poor prognosis. Mortality varies from 11 to 39%
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
[1]
. Mortality due to PANH remains high (25 to 35%) compared with oedematous forms
| [6] | Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014 Feb; 109(2): 302]. Am J Gastroenterol. 2013; 108(9): 140 16. |
[6]
. From the point of view of evolution, the two main causes of death associated with acute pancreatitis, which are of equivalent importance, are organ failure in the first few days and infection of the pancreatic necrosis between the 2nd and 4th week of the evolution of AP
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
| [2] | Leppäniemi A, Tolonen M, Tarasconi A, Segovia-Lohse H, Gamberini E, Kirkpatrick AW, et al. 2019 WSES guidelines for the management of severe acute pancreatitis. World J Emerg Surg. 2019; 14: 27. |
| [5] | Boland B, Colquhoun S, Menon V, Kim A, Lo S, Nissen NN. Current surgical management of infected pancreatic necrosis. Am Surg. 2010; 76(10): 109 9. |
| [12] | Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis--2012: revision of the Atlanta classification and definitions by international consensus. Gut. 2013; 62(1): 10 11. |
[1, 2, 5, 12]
, as was the case in our first observation.
In the 2nd observation, in contrast to the first case, the post-operative course was favourable, with healing in the first instance notwithstanding the HIV infection. Morbidity was 40%
| [1] | K Aziz, D Bonnet, B Foppa. Hepato-gastro-enterology, Digestive surgery. Pancréatite aigüe. Elsevier Masson SAS 2012, 2nd edition, Camille Desmoulins. ISBN: 97 29 0964 9. |
[1]
. It is manifested by fistulas, endocrine sequelae and ventrations
| [4] | Hackert T, Büchler MW. Decision making in necrotizing pancreatitis. Dig Dis. 2016; 34(5): 51 24. |
| [6] | Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology guideline: management of acute pancreatitis [published correction appears in Am J Gastroenterol. 2014 Feb; 109(2): 302]. Am J Gastroenterol. 2013; 108(9): 140 16. |
| [14] | E Allah-kouadio, M Diakité, S koné. Pancréatite aigue nécrotico-hémorragique révélée par une hémorragie digestive haute par rupture de varices œsophagienne. Rev Int Sc Méd 2013; 15, 2: 10 103. |
[4, 6, 14]
.