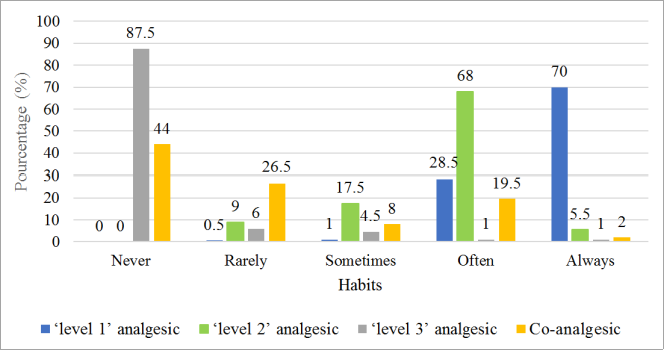
Background: Headaches can be detrimental to patients if they are inadequately managed. Objective: Our aim was to study the diagnostic and therapeutic knowledge of General Practitioners (GPs) in relation to headache. Methods: We conducted a cross-sectional, descriptive, questionnaire-based study of general practitioners from 1 January to 28 February 2022 in Abidjan. The questionnaire focused on the type of headache patients present to the clinic and GPs' diagnostic and therapeutic pattern with regard to headache. Results: 200 GPs were surveyed. In terms of diagnostic habits, GPs had poor habits regarding the characteristics of headaches, apart from the site, type and duration, which were ‘always’ sought in 79.5%, 74.5% and 70% of cases respectively. They were also not very familiar with the patient's history, apart from high blood pressure, which was ‘always’ sought in 78.5% of cases. Regarding headache disability, the habit was poor, as it was assessed ‘always’ and ‘often’ in 2.5% and 48% of cases respectively. GPs were also unaccustomed to physical examination for neurological signs, with motor deficit and meningeal syndrome ‘always’ sought by 10.5% and 11% of GPs respectively. Indications for prescribing brain imaging were followed by GPs in 38.1% of cases. As for treatment habits, WHO level 1 analgesics were ‘always’ prescribed in 70% of cases, and level II analgesics ‘often’ prescribed in 68% of cases. Level 3 analgesics and Co analgesics were ‘never’ prescribed in 44% and 87.5% of cases respectively. Headache patients were mainly referred to neurologists (96%). Conclusion: This study highlighted a lack of diagnostic and therapeutic knowledge. This suggests that GPs should be given more training to improve headache management.
| Published in | American Journal of Psychiatry and Neuroscience (Volume 13, Issue 1) |
| DOI | 10.11648/j.ajpn.20251301.12 |
| Page(s) | 7-15 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Diagnostic Knowledge, General Practitioner, Headache, Management
Number of GPs | Percentage | |
|---|---|---|
Socio-demographic characteristics of GPs | ||
Age ranges | ||
< 30 | 33 | 16.5 |
30-50 | 165 | 82.5 |
> 50 | 2 | 1 |
Gender | ||
Female | 67 | 33.5 |
Male | 133 | 66.5 |
Number of years practicing medicine | ||
[1, 11] | 117 | 58.5 |
[11, 21] | 46 | 23.0 |
[21, > ] | 37 | 18.5 |
Profile of headache cases seen by GPs | ||
Average number of cases per consultation | ||
1 | 10 | 5 |
2 | 22 | 11 |
3 | 7 | 3.5 |
4 | 18 | 9 |
5 | 143 | 71.5 |
Age ranges | ||
< 25 years old | 20 | 10 |
25 - 44 years old | 146 | 73 |
> 44 | 34 | 17 |
Gender | ||
Male | 54 | 27 |
Female | 146 | 73 |
Chronicity | ||
< 3 months | 191 | 95.5 |
> 3 months | 9 | 4.5 |
Severity | ||
Benign | 194 | 97 |
Severe | 6 | 3 |
Components of questioning | Habit (%) | ||||
|---|---|---|---|---|---|
Never | Rarely | Sometimes | Often | Always | |
Characteristics of headaches | |||||
Age | 0 | 0 | 1 | 29 | 70 |
Whether usual or not | 0.5 | 6 | 9 | 53.5 | 31 |
Mode on onset | 0 | 1.5 | 3.5 | 40 | 55 |
Subsequent course | 0 | 8.5 | 10.3 | 50 | 31.5 |
Location | 0.5 | 0 | 1.5 | 18.5 | 79.5 |
Irradiation | 0 | 11.5 | 5.5 | 56.5 | 26.5 |
Type | 0 | 3.5 | 3 | 19 | 74.5 |
Triggering factors/sedation | 0 | 4 | 6.5 | 54.5 | 35 |
Severity | 1 | 9 | 12 | 63 | 15 |
Associated signs | |||||
Nausea ± vomiting | 0 | 3.5 | 3.5 | 73 | 20 |
Visual disturbances | 0 | 43.5 | 12.5 | 32.5 | 11.5 |
Fever | 0 | 1.5 | 1.5 | 14.5 | 82.5 |
Disability assessment | 8.5 | 16 | 25 | 48 | 2.5 |
History | |||||
Hypertension | 0 | 3 | 2.5 | 16 | 78.5 |
Diabetes | 2.5 | 44.5 | 13 | 29.5 | 10.5 |
Familial headaches | 7 | 37.5 | 18.5 | 33 | 4 |
Signs of immunosuppression | 6 | 12 | 7.5 | 71 | 3.5 |
Trauma | 4 | 35.5 | 22.5 | 30.5 | 7.5 |
Components of the physical examination | Habit (%) | ||||
|---|---|---|---|---|---|
Never | Rarely | Sometimes | Often | Always | |
Vitals | |||||
Blood pressure | 0 | 2 | 0.5 | 11 | 82.5 |
Pulse | 0 | 1 | 2 | 17.5 | 75.5 |
Temperature | 0 | 0.5 | 2 | 3.5 | 90 |
Neurological signs | |||||
Motor deficit | 0 | 35 | 12.5 | 33.5 | 10.5 |
Meningeal syndrome | 0 | 32.5 | 17.5 | 35.5 | 11 |
Reasons | Expected answers | Number (n= 187) | Percentage |
|---|---|---|---|
All patients with headaches | False | 1 | 0.5 |
Inaugural headache after the age of 50 | True | 137 | 73.3 |
Recent or recently worsening (< 7 days) and unusual headaches | True | 9 | 4.8 |
Unusual headache in a known headache sufferer | True | 10 | 5.3 |
Headache + meningeal syndrome | True | 90 | 48.1 |
Habitual chronic Headache | False | 51 | 27.3 |
Headache + neurological sign | True | 132 | 70.6 |
Headache + change in general condition | True | 7 | 3.7 |
Post-partum headache | True | 5 | 2.7 |
Headache in HIV immunocompromised patients | True | 153 | 81.8 |
Average proportion of expected responses = 31,8% | |||
GPs | General Practitioners |
| [1] | Stovner LJ, Hagen K, Linde M et al. The global prevalence of headache: an update, with analysis of the infuences of methodological factors on prevalence estimates. The Journal of Headache and Pain (2022) 23: 34. |
| [2] | Do TP, Remmers A, Schytz HW et al. Red and orange flags for secondary headaches in clinical practice SNNOOP10 list. Neurology 2019; 92 (3): 134-44. |
| [3] | Silva MM, Schultze ACB, Cavalheiro BP et al. Profile and generalist physician knowledge about neurology in emergency department: headache management. Arq Neuropsiquiatr 2020; 78(1): 44-49. |
| [4] | Domitrz I, Lipa A, Rożniecki J. Migraine diagnosis and treatment in Poland: survey of primary care practitioners. Polish Journal of Neurology and Neurosurgery 2021, Volume 55, no. 4 pages: 380–386. |
| [5] | Fathy M, Sadek AE, Farag S et al. Dilemma of migraine diagnosis and management among non-neurologists. Egypt J Neurol Psychiatry Neurosurg (2021) 57: 118. |
| [6] | García-Azorín D, Molina-Sánchez M, Gómez-Iglesias P et al. Headache education and management in Cameroon: a healthcare provider study. Acta Neurol Belg 2022 Feb; 122(1): 75-81. |
| [7] | Dabilgou AA, Dravé A, Kyelem JMA. et al. Knowledge, Attitudes, and Management of General Practitioners of the Hospital Districts of Ouagadougou about Migraine (Burkina Faso. Pain Research and Management Volume 2021. |
| [8] | Kennis K, Kernick D, O'Flynn N. Diagnosis and management of headaches in young people and adults: NICE guideline. Br J Gen Pract. Août 2013; 63(613): 443-445. |
| [9] | Schytz HW, Amin FM, Jensen RH et al. Reference programme: diagnosis and treatment of headache disorders and facial pain. Danish Headache Society, 3rd edition, 2020. The Journal of Headache and Pain (2021) 22: 22. |
| [10] | Moisset X, Mawet J, Guegan-Massardierd E et al. French guidelines for the emergency management of headaches. Douleurs: Évaluation - Diagnostic - Traitement 2018; 19, 14 - 6. |
| [11] | Viera AJ, Antono B. Acute Headache in Adults: A Diagnostic Approach. Am Fam Physician. 2022; 106(3): 260-268. |
| [12] | Collège des Enseignants de Neurologie. Céphalée inhabituelle aiguë et chronique chez l'adulte et l'enfant. |
| [13] | Frese T, Druckrey H, Sandholzer H. Headache in General Practice: Frequency, Management, and Results of Encounter. International Scholarly Research Notices Volume 2014. |
| [14] | Bautista C, Grossman S. Somatosensory function, pain, and headache. In: Grossman SC, Porth CM. Porth’s Pathophysiology: Concepts of Altered Health States. 9th ed. Philadelphia, PA: Wolters Kluwer; 2014: 422-451. |
| [15] |
Bajwa ZH, Wootton RJ. Evaluation of headache in adults. Up To Date. December 10, 2014.
http://www.uptodate.com/contents/evaluation-of-headache-in-adults |
| [16] | Hale N, Paauw DS. Diagnosis and treatment of headache in the ambulatory setting: a review of classic presentations and new considerations in diagnosis and management. Med Clin North Am. 2014; 98(3): 505-527. |
| [17] | Hainer BL, Matheson EM. Approach to acute head - ache in adults. Am Fam Physician. 2013; 87(10): 682-687. |
| [18] | Rizzoli P, Mullally WJ. Headache. The American Journal of Medicine (2018) 131, 17–24. |
| [19] | Lee VME, Ang LL, Soon DTL et al. The adult patient with headache. Singapore Med J 2018; 59(8): 399-406. |
| [20] | Winland-Brown JE, Keller MB. Neurological problems. In: Dunphy LM, Winland-Brown JE, Porter BO, Thomas DJ. Primary Care: Art and Science of Advanced Practice Nursing. 4th ed. Philadelphia, PA: F. A. Davis; 2015: 77-148. |
| [21] | Silberstein SD. Approach to the patient with head - ache. Merck Manual. April 2014. |
| [22] | Kristoffersen ES, Faiz KW, Hansen JM. The management and clinical knowledge of headache disorders among general practitioners in Norway: a questionnaire survey. The Journal of Headache and Pain 2021; 22: 136. |
| [23] | Holle D, Obermann M. The role of neuroimaging in the diagnosis of headache disorders. Ther Adv Neurol Disord. 2013; 6(6): 369-374. |
| [24] | Eigenbrodt AK, Ashina H, Khan S et al. Diagnosis and management of migraine in ten steps. Rév. Nat. Neurol 2021; 17(8): 501-514. |
| [25] | Anekar AA, Hendrix JM, Cascella M. WHO Analgesic Ladder. [Updated 2023 Apr 23]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. |
| [26] | Carlsen LN, Stefansen S, Ahnfeldt-Mollerup P et al. Diagnostics and management of headache in general practice. Family Practice, 2024, 41, 470–476 |
| [27] | Libert F, Adam F, Eschalier A et al. Les medicaments adjuvants (ou co-analgésiques). Douleur et Analgésie 2006; 19(4): 91-97. |
| [28] | Fejes E, Feher G, Gurdan Z et al. Characteristics of Patients Referred To A Specialized Headache Clinic. Scientific Reports | (2020) 10: 1146. |
| [29] | Doretti A, Shestaritc I, Ungaro D, et al. Headaches in the emergency department – a survey of patients’ characteristics, facts and needs. The Journal of Headache and Pain (2019) 20: 100. |
| [30] | Mehrotra CN, Kanodia N, Shankar P et al. Knowledge, attitude and practice of general physicians related to migraine. World J Pharm Sci 2015; 3(12): 2470-2471. |
APA Style
Kouassi, K. L., Konan, K. C., Broh, Y., Abbé, S., Essoin, A. N., et al. (2025). General Practitioners' Knowledge in the Management of Headaches on First Contact Health Centres in Abidjan, Ivory Coast. American Journal of Psychiatry and Neuroscience, 13(1), 7-15. https://doi.org/10.11648/j.ajpn.20251301.12
ACS Style
Kouassi, K. L.; Konan, K. C.; Broh, Y.; Abbé, S.; Essoin, A. N., et al. General Practitioners' Knowledge in the Management of Headaches on First Contact Health Centres in Abidjan, Ivory Coast. Am. J. Psychiatry Neurosci. 2025, 13(1), 7-15. doi: 10.11648/j.ajpn.20251301.12
AMA Style
Kouassi KL, Konan KC, Broh Y, Abbé S, Essoin AN, et al. General Practitioners' Knowledge in the Management of Headaches on First Contact Health Centres in Abidjan, Ivory Coast. Am J Psychiatry Neurosci. 2025;13(1):7-15. doi: 10.11648/j.ajpn.20251301.12
@article{10.11648/j.ajpn.20251301.12,
author = {Kouamé Léonard Kouassi and Kouassi Cyrille Konan and Yves Broh and Stéphane Abbé and Ahya Nancy Essoin and Roxane Beuseize and Nawa Samuel Yeo and Mariam Ouattara-Doumbia},
title = {General Practitioners' Knowledge in the Management of Headaches on First Contact Health Centres in Abidjan, Ivory Coast},
journal = {American Journal of Psychiatry and Neuroscience},
volume = {13},
number = {1},
pages = {7-15},
doi = {10.11648/j.ajpn.20251301.12},
url = {https://doi.org/10.11648/j.ajpn.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpn.20251301.12},
abstract = {Background: Headaches can be detrimental to patients if they are inadequately managed. Objective: Our aim was to study the diagnostic and therapeutic knowledge of General Practitioners (GPs) in relation to headache. Methods: We conducted a cross-sectional, descriptive, questionnaire-based study of general practitioners from 1 January to 28 February 2022 in Abidjan. The questionnaire focused on the type of headache patients present to the clinic and GPs' diagnostic and therapeutic pattern with regard to headache. Results: 200 GPs were surveyed. In terms of diagnostic habits, GPs had poor habits regarding the characteristics of headaches, apart from the site, type and duration, which were ‘always’ sought in 79.5%, 74.5% and 70% of cases respectively. They were also not very familiar with the patient's history, apart from high blood pressure, which was ‘always’ sought in 78.5% of cases. Regarding headache disability, the habit was poor, as it was assessed ‘always’ and ‘often’ in 2.5% and 48% of cases respectively. GPs were also unaccustomed to physical examination for neurological signs, with motor deficit and meningeal syndrome ‘always’ sought by 10.5% and 11% of GPs respectively. Indications for prescribing brain imaging were followed by GPs in 38.1% of cases. As for treatment habits, WHO level 1 analgesics were ‘always’ prescribed in 70% of cases, and level II analgesics ‘often’ prescribed in 68% of cases. Level 3 analgesics and Co analgesics were ‘never’ prescribed in 44% and 87.5% of cases respectively. Headache patients were mainly referred to neurologists (96%). Conclusion: This study highlighted a lack of diagnostic and therapeutic knowledge. This suggests that GPs should be given more training to improve headache management.},
year = {2025}
}
TY - JOUR T1 - General Practitioners' Knowledge in the Management of Headaches on First Contact Health Centres in Abidjan, Ivory Coast AU - Kouamé Léonard Kouassi AU - Kouassi Cyrille Konan AU - Yves Broh AU - Stéphane Abbé AU - Ahya Nancy Essoin AU - Roxane Beuseize AU - Nawa Samuel Yeo AU - Mariam Ouattara-Doumbia Y1 - 2025/02/11 PY - 2025 N1 - https://doi.org/10.11648/j.ajpn.20251301.12 DO - 10.11648/j.ajpn.20251301.12 T2 - American Journal of Psychiatry and Neuroscience JF - American Journal of Psychiatry and Neuroscience JO - American Journal of Psychiatry and Neuroscience SP - 7 EP - 15 PB - Science Publishing Group SN - 2330-426X UR - https://doi.org/10.11648/j.ajpn.20251301.12 AB - Background: Headaches can be detrimental to patients if they are inadequately managed. Objective: Our aim was to study the diagnostic and therapeutic knowledge of General Practitioners (GPs) in relation to headache. Methods: We conducted a cross-sectional, descriptive, questionnaire-based study of general practitioners from 1 January to 28 February 2022 in Abidjan. The questionnaire focused on the type of headache patients present to the clinic and GPs' diagnostic and therapeutic pattern with regard to headache. Results: 200 GPs were surveyed. In terms of diagnostic habits, GPs had poor habits regarding the characteristics of headaches, apart from the site, type and duration, which were ‘always’ sought in 79.5%, 74.5% and 70% of cases respectively. They were also not very familiar with the patient's history, apart from high blood pressure, which was ‘always’ sought in 78.5% of cases. Regarding headache disability, the habit was poor, as it was assessed ‘always’ and ‘often’ in 2.5% and 48% of cases respectively. GPs were also unaccustomed to physical examination for neurological signs, with motor deficit and meningeal syndrome ‘always’ sought by 10.5% and 11% of GPs respectively. Indications for prescribing brain imaging were followed by GPs in 38.1% of cases. As for treatment habits, WHO level 1 analgesics were ‘always’ prescribed in 70% of cases, and level II analgesics ‘often’ prescribed in 68% of cases. Level 3 analgesics and Co analgesics were ‘never’ prescribed in 44% and 87.5% of cases respectively. Headache patients were mainly referred to neurologists (96%). Conclusion: This study highlighted a lack of diagnostic and therapeutic knowledge. This suggests that GPs should be given more training to improve headache management. VL - 13 IS - 1 ER -
Faculty of Medical Sciences, Felix Houphouet-Boigny University, Abidjan, Ivory Coast; Department of Neurology, University Hospital of Yopougon, Abidjan, Ivory Coast
Department of Neurology, University Hospital of Yopougon, Abidjan, Ivory Coast
Faculty of Medical Sciences, Felix Houphouet-Boigny University, Abidjan, Ivory Coast; Department of Neurology, University Hospital of Yopougon, Abidjan, Ivory Coast
Faculty of Medical Sciences, Felix Houphouet-Boigny University, Abidjan, Ivory Coast; Department of Neurology, University Hospital of Yopougon, Abidjan, Ivory Coast
Faculty of Medical Sciences, Felix Houphouet-Boigny University, Abidjan, Ivory Coast; Department of Neurology, University Hospital of Yopougon, Abidjan, Ivory Coast
Faculty of Medical Sciences, Felix Houphouet-Boigny University, Abidjan, Ivory Coast; Department of Neurology, University Hospital of Yopougon, Abidjan, Ivory Coast
Faculty of Medical Sciences, Felix Houphouet-Boigny University, Abidjan, Ivory Coast; Department of Neurology, University Hospital of Yopougon, Abidjan, Ivory Coast
Information