Abstract
The objectives of this study were to determine the main indications for CT-guided lumbar infiltrations, to list the clinical picture post-CT-guided lumbar infiltration and to describe the intensity of pain post-CT-guided lumbar infiltration in the radiology department. This was a descriptive study to be collected prospectively over a period of seven months from June 2023 to December 2023 relating to CT-guided lumbar infiltration in the radiology and medical imaging department of the Mother Hospital. Child “Luxembourg”. It focused on patients aged 20 to 80 years and over, admitted and having performed a CT-guided infiltration in our department during the period. We glued 50 patients during our study. The 40-59 age group was the most common, at 54%. There is a male predominance with a sex ratio equal to 1.08. The maximum number of patients came from the neurology department (78%). Patients without medical care were the most represented, i.e. 60%. 64% of our patients have not had any infiltration in the last six months. Patients with pain lasting less than 6 months were the most represented, i.e. 40%. The level of pain intensity increasing between 5-7 (severe pain) was the most represented, i.e. 58%. The visual analog scale after three months was estimated between 1-3 and was the most represented, i.e. 70%. The visual analog scale (VAS) estimated between 3-5 after one month was the most represented, i.e. 66%. Discopathy represented 47% followed by the combination of herniated disc and disc disease, i.e. 26.4%. The lesions were more localized at the L5-S1 level, i.e. 62%. Epidural infiltration was performed in 66% of our patients. The complication rate was 0% due to the strict hygiene conditions applied for each procedure. Infiltration is very important in the treatment of active disc disease. Our study demonstrates that epidural infiltrations can be an alternative in the overall management of inflammatory disc disease.
Keywords
Pain, Infiltration, Epidural, Lumbar, CT-guided
1. Introduction
An infiltration is a medical technique consisting of injecting a corticosteroid and/or an anesthetic locally, in or as close as possible to a painful site such as the joint, bursa, synovial sheath, epidural, intradiscal and peritendinous canal.
| [1] | Mader R, Lavi I, Luboshitzky R, Evaluation of the pitutary-adrenal axis function following simple intra articular injection of methyl prednisolone. Arthritis Rheun. 2005(52): 924-928. |
[1]
In 2014, more than 5 million infiltrations were carried out in the United States.
| [2] | Manchikanti, Laxmaiah, Vidyasagar Pampati, and Joshua A. Hirsch. Retrospective Cohort Study of Usage Patterns of Epidural Injections for Spinal pain in the US Fee-for-service Medicare Population from 2000 to 2014 6(13 2016); e013042, https://doi.org/10.1002/art.20884 |
[2]
The increase in these therapeutic procedures has highlighted a rare immediate and permanent complication: spinal cord infarction after foraminal infiltration.
| [3] | Diehn, Felix E, Naveen S, Murthy, and Timothy P. Maus. Science to Practice: What Causes Arterial Infarction in Transforaminal Epidural Steroid Injections, and Which Steroid Is Safe? Radiology 279(2016): 657-59. https://doi.org/10.1148/radiol.2016160171 |
[3]
The main indications at the spine level are pain linked to inflammation of the vertebral endplates, disco-radicular conflicts or pain linked to damage to the zygapophyseal joints, as well as foraminal stenoses of disco-osteophytic origin.
Spinal, intra-discal, epidural and foraminal infiltrations under scanner are today a treatment of choice in spinal pain symptoms. Over the past 20 years, we have observed a clear increase in the number of infiltrations carried out throughout the world which is difficult to quantify, however in the United States, a large retrospective study carried out by Manchikanti et al described that epidural injections had increased by 99%. and 69% for foraminal injections per 100,000 health insurance beneficiaries between 2000 and 2014.
In 1930, the injection of an epidural anesthetic agent was described in the treatment of sciatic nerve pathology symptoms.
Epidural steroid injection was first performed in the 1950s and became a cornerstone of treatment for low back and lower back pain in the 1970s.
| [5] | Meulen, Bastiaan C. ter, Esther T. Maas, Amrita Vyas, Marinus van der vegt, Koo de Priester, Michiel R. de Boer, et al. Treatment of Acute Sciatica with Transforaminal Epidural Corticosteroids and Local Anesthetic: Design of a Randomized Controlled Trial. BMC Musculosketal Disorders 18(2017): 215. https://doi.org/10.1186/s12891-017-1571-8 |
[5]
The management of chronic low back pain patients would require specifying the nature of the anatomical damage and, in the case of disc disease, it would then be necessary to offer an effective and well-tolerated treatment. The first-line methods remain analgesic treatment, physiotherapy, and lumbar infiltrations are only indicated in the event of failure of drug treatments.
However, sometimes these treatments are insufficient, and intradisc injections of corticosteroids have been proposed for the management of this low back pain that is resistant to first-line treatment.
| [6] | Nguyen C, Bénichou M, Revel M, Poiraudeau S, Rannou F. Association of accelerated switch from vertebral end-plate Modic I to Modic 0 signal changes with clinical benefit of intradiscal corticosteroid injection for chronic low back pain. American College of Rheumatology 2011; Volume 3, pages: 2828-2831. https://doi.org/10.1002/art.30443 |
[6]
Magnetic resonance imaging (MRI) has revealed signal abnormalities in the vertebral bodies adjacent to a degenerative intervertebral disc in some patients with low back pain. Three stages make up the Modic classification
| [7] | Mayo Clinic Staff. Herniated Disk -Symptoms and Causes. Mayo Clinic. 2019. Pages 15-67. |
[7].
Modic 1, which corresponds to edematous changes in T1 hypo-signal and T2 hyper-signal (active disc disease);
Modic 2, combining a T1 hyper signal and a T2 hyper signal, which is considered the natural evolution of Modic 1 (fatty involution).
Modic 3, combining hypo T1 signal and hypo T2 signal, rare, which correspond to osteocondensation.
Modic 1-2: Patients with a mixture of type I and II changes.
To date, cortivazol (Altim), a corticosteroid known to be effective and associated with a low complication rate, is no longer available since February 2017. In this context of absence, prednisolone (Hydrocortancyl), the only corticosteroid approved to ensure the continuity of patient care, has seen its use restricted: in fact in a press release dated February 17, 2017, the laboratory informs that the foraminal route “should not be practiced” with Hydrocortancyl
| [8] | Changes to the conditions of use of hydrocortancyl 2.5%, suspension for injection (prednisolone acetate), Available at http://www.sanofi.fr |
[8]
. Therefore, we find ourselves in a situation of reduction in therapeutic offer
| [9] | Cotten, A, J-L Drapé, N Sans, A Feydy, J-M Bartoli, and J-F Meder. Recommendations from SIMS, SFR and FRI-SFR Concerning Corticosteroids Injected Epidurally and Foraminal, 2017. https://doi.org/10.1016/j.diii.2018.01.012 |
[9]
: cortivazol is no longer available and prednisolone is restricted in its use.
In France, the Musculo-Skeletal Imaging Society (SIMS) has published a press release regarding the action to be taken regarding the prolonged unavailability of Altim: foraminal infiltrations at the cervical and lumbar level are no longer recommended
| [10] | Thomas, E, C. Cyteval, L. Abiad, M. C. Picot, P. Taourel, and F. Blotman. Efficacy of Transforaminal versus Interspinous Corticosteroid Injectionin Discal Radiculalgia? A Prospective, Randomized, Double-Blind Study 22(1, 2003): 299-304. https://doi.org/10.1007/s10067-003-0736-z |
| [11] | Rhee, John M, Tim Yoon, and K. Daniel Riew. Cervical Radiculopathy. The Journal of the American Academy of Orthopedic Surgeons 15 (2007): 486-94, https://doi.org/10.5435/00124635-200708000-00005 |
[10, 11]
. Therefore, the substitution of the foraminal route by the epidural route at the lumbar level has been commented on. However, several studies have proven the superiority of the foraminal approach compared to the epidural approach because it allows getting as close as possible to the affected root
| [10] | Thomas, E, C. Cyteval, L. Abiad, M. C. Picot, P. Taourel, and F. Blotman. Efficacy of Transforaminal versus Interspinous Corticosteroid Injectionin Discal Radiculalgia? A Prospective, Randomized, Double-Blind Study 22(1, 2003): 299-304. https://doi.org/10.1007/s10067-003-0736-z |
| [11] | Rhee, John M, Tim Yoon, and K. Daniel Riew. Cervical Radiculopathy. The Journal of the American Academy of Orthopedic Surgeons 15 (2007): 486-94, https://doi.org/10.5435/00124635-200708000-00005 |
[10, 11]
.
Despite the effectiveness of epidural infiltration in the management of spinal pathology, little data exists in sub-Saharan Africa and in Mali in particular.
The aim of this study was to:
1) Determine the main indications for CT-guided lumbar infiltrations in the radiology department.
2) List the clinical picture after CT-guided lumbar infiltration.
3) Describe the intensity of pain after CT-guided lumbar infiltration.
2. Methodology
2.1. Type of Study and Period of Study
This is a descriptive study with prospective collection over a seven-month period from June 2023 to December 2023.
2.2. Location and Study Setting
Our study took place in the radiology department of the “Le Luxembourg” mother-child hospital center.
2.3. Study Variable
The clinical parameters were recorded when the patient was received and after the procedures.
1) Sociodemographic parameters: age, sex and profession.
2) Clinical parameters: duration of symptoms, previous surgery, medical history (ATCD), history of infiltration in the last six months, pain scale (VAS = Visual Analog Scale), improvement in pain at one month and at 3 months after the action.
3) Data: CT/MRI on scan changes.
2.4. Study Population
Our study involved all patients aged 20 to 80 years and over, of both sexes requiring CT-guided lumbar infiltration during the study period.
1) Inclusion criteria:
Were included in this study, Patients aged 20 to 80 years and over, admitted and having performed a CT-guided infiltration in our department during the period.
2) Non-inclusion criteria:
Were not included in the study: subjects aged under 20 and those who did not give their consent to participate in the study on the one hand and on the other hand patients with problems of systemic inflammation, metabolic disorder, metabolic bone disease and local infection.
2.5. Material
The equipment consisted of the scanner, sterile fields, sterile gloves, lumbar puncture needles, 10 cc syringes, 40x40 compresses, tape, betadine, xylocaine, iopamicron 300 mg/50 ml and dexamethasone.
2.6. Procedure
Lumbar scanner technique:
We used a helical acquisition on the lumbar spine without injection of contrast product with coronal and sagittal reconstruction. The patient was placed in a supine position with the head inward.
Patient preparation:
Patients were psychologically prepared during the pre-infiltrative consultation. The physical preparation of the patients was done on the day of the infiltration.
Installation of the patient in the scanner during infiltration:
Patient in procubitus position, head in, arms extended forward, lumbar region unclothed, he remains motionless so that the landmarks are not lost. Asepsis is carried out with povidone at least 3 layers followed by the concomitant installation of a sterile table prepared by the manipulators including the equipment to be used. The installation of the patient is ensured by the manipulators under the supervision of the radiologist.
Operators:
A reference cut is then chosen for the infiltration with identification of the site, a skin marking is made then the manipulator cleans the skin.
1) The radiologist carefully disinfects his hand by surgically washing with soap then using hydroalcoholic gel before wearing sterile gloves.
2) A second cleaning of the skin is carried out by the radiologist after covering the area with a sterile field.
3) Local anesthesia with 5 to 10 cc of xylocaine.
4) Placement of the 22G lumbar puncture needle and progression to the site.
5) Injections of 1 cc of contrast product (omnipaque) to opacify the site and check the position of the needle.
6) Injections 2ml of dexamethasone into the center of the disc or into the epidural space.
7) Removing the needle.
8) Cleaning and application of a local dressing. The latter will be kept until washing the next day.
9) Patient mobilization is immediate.
2.7. Informed Consent of Patients
Informed consent from patients constitutes one of the essential steps in all research activities. In our case, it is obtained after explaining to patients the objectives, risks and benefits linked to this study.
2.8. Data Collection
The data was collected from a pre-established survey form including clinical and radiological epidemiological data.
2.9. Data Analysis
The data was collected on a survey form developed for this purpose and then inserted into an Access database. Their analysis will be done by SPSS statistical software.
Fisher's exact test was used for the analysis of quantitative variables, described with mean and standard errors (SE). The Chi2 test was used for the analysis of qualitative variables described with numbers and percentages. A P<0.05 considered statistically significant.
3. Results
During our study, we had a total of 50 patients.
3.1. Sociodemographic Study
A. Age:
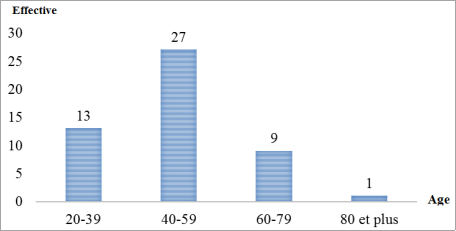
Figure 1. Distribution of patients according to age group.
The most represented age group was between 40 - 59 years old with 54% or 27 cases.
B. Sex:
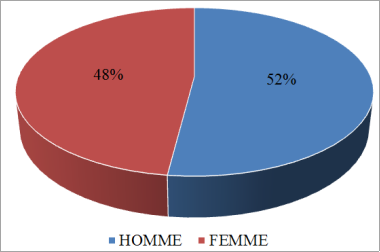
Figure 2. Distribution of patients according to gender.
The male sex represented 52%, i.e. a sex ratio of 1.08.
C. The requesting service:
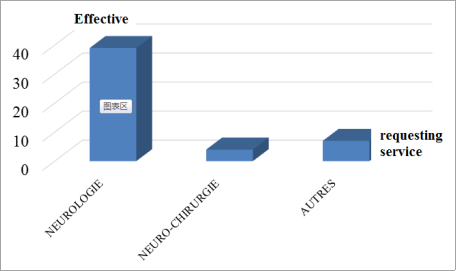
Figure 3. Distribution of patients according to the requesting service.
The maximum number of patients came from the neurology department (78%).
3.2. Clinical Data
A. Medical history:
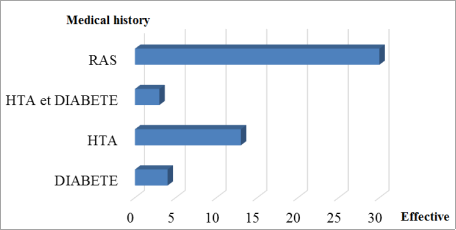
Figure 4. Distribution of patients based on medical history.
Patients with no medical history were the most represented with 60% followed by hypertensive patients.
B. History of infiltration:
Table 1. Distribution of patients according to infiltration ATCD (the last six months).
Infiltration in the last six months | Effective | Frequency |
Yes | 18 | 36,0 |
NO | 32 | 64,0 |
Total | 50 | 100,0 |
There was no infiltration in the last six months in 32 patients or 64%.
C. The beginning of the onset of pain:
Table 2. Distribution of patients according to duration of progression.
Duration of development (months) | Effective | Frequency |
<6 | 20 | 40,0 |
6-12 | 12 | 24,0 |
>12 | 18 | 36,0 |
Total | 50 | 100,0 |
Patients with pain lasting less than 6 months were the most represented, i.e. 40%.
D. L’ assessment of pain intensity:
Table 3. Distribution of patients according to the evaluation of pain intensity according to the visual scale (VAS) when patients arrive.
EVA | Effective | Frequency |
5-7 | 29 | 58,0 |
7-9 | 18 | 36,0 |
10 | 3 | 6,0 |
Total | 50 | 100,0 |
The level of pain intensity estimated between 5-7 (severe pain) was more represented, i.e. 58%.
E. The lesion topography:
Table 4. Distribution of patients according to lesion topography.
Lesion topography | Effective | Frequency |
L3-L4 | 2 | 4,0 |
L4-L5 | 17 | 34,0 |
L5-S1 | 31 | 62,0 |
Total | 50 | 100,0 |
The lesions were more localized at the L5-S1 level, i.e. 62%.
F. The type of infiltration:
Table 5. Distribution of patients according to the type of infiltration.
Types of infiltration | Effective | Frequency |
Epidural | 33 | 66,0 |
Foraminal | 14 | 28,0 |
Intra-discal | 3 | 6,0 |
Total | 50 | 100,0 |
Epidural infiltration was performed in 66% of our patients.
G. Abnormalities on CT/MRI:
Table 6. Distribution of patients according to abnormalities on CT/MRI.
ACT/MRI abnormality | Effective | Frequency |
Herniated disc | 10 | 14,7 |
Discopathy | 32 | 47,0 |
Disc protrusion | 2 | 3,0 |
Lower protrusion | 6 | 8,9 |
Herniated disc and disc disease | 18 | 26,4 |
Total | 68 | 100,0 |
Disc disease represented 47% or 32 patients followed by the combination of disc herniation and disc disease 26.4%.
3.3. Clinical Evolution
A. The intensity of the pain after one month:
Table 7. Distribution of patients according to pain intensity after one month.
after a month | Effective | Frequency |
1-3 | 9 | 18,0 |
3-5 | 33 | 66,0 |
5-7 | 8 | 16,0 |
Total | 50 | 100,0 |
VAS estimated between 3-5 after one month was the most represented, i.e. 66%.
B. The intensity of the pain after three (03 months):
Table 8. Distribution of patients according to pain intensity after three months.
EVA after three months | Effective | Frequency |
1-3 | 35 | 70,0 |
3-5 | 4 | 8,0 |
5-7 | 1 | 2,0 |
Not evaluate | 10 | 20,0 |
Total | 50 | 100,0 |
VAS after three months estimated between 1-3 was the most represented, i.e. 70%.
3.4. Complication
During our study, we did not note any complications.
4. Discussions
4.1. Limitations and Difficulties
Some difficulties were encountered during this work:
1) This work was only carried out in one center. There was therefore a selection bias.
2) In addition, a certain number of patients could not be found 3 months after the procedure.
4.2. Frequency
We collected 50 patients during the 6 months of the investigation, our figure is higher than that of Mr. Kouyaté
| [12] | KOUYATE M. scan-guided spinal infiltrations of active discopathies at the lumbar level in the radiology department of the chu of gouadeloupe. Thesis in medicine. FMOS; 2023: 121. |
[12]
who found 19 patients over a period of 06 months at the CHU of point G and lower than those of I. Braithwaite
| [13] | Braithwaite, J. White, A. Saifuddin, P. Renton, B. A. Taylor Vertebral end-plate (Modic) changes on lumbar spine MRI: correlation with pain reproduction at lumbar discography Eur Spine J (1998) 7: 363–368. https://doi.org/10.1007/s005860050091 |
[13]
who found 62 patients with Modic-type disc changes over a 30-month period. Guillaume Dervin
| [14] | Guillaume Dervin. Active disc disease, an infectious etiology Medicine thesis year 2016 Paris Descartes University - Faculty of Medicine of France. |
[14]
found 32 discs with modic change out of a total of 77, i.e. a frequency of 41%.
Our low frequency could be explained by the duration of the study unlike the others which lasted longer. 3. Sociodemographic aspects.
The male sex dominated our sample, i.e. 52%, with a sex ratio of 1.08. This result is similar to that of I. Braithwaite
| [13] | Braithwaite, J. White, A. Saifuddin, P. Renton, B. A. Taylor Vertebral end-plate (Modic) changes on lumbar spine MRI: correlation with pain reproduction at lumbar discography Eur Spine J (1998) 7: 363–368. https://doi.org/10.1007/s005860050091 |
[13]
who reported a male predominance with a sex ratio of 1.14 but different from that of M. Kouyaté
| [12] | KOUYATE M. scan-guided spinal infiltrations of active discopathies at the lumbar level in the radiology department of the chu of gouadeloupe. Thesis in medicine. FMOS; 2023: 121. |
[12]
, C. Nguyen et al
| [15] | Nguyen C, Boutron I, Baron G et al. Intradiscal glucocorticoid injection for patients with chronic low back pain associated with active discopathy: a randomized. https://doi.org/10.7326/M16-1700 |
[15]
and F. Fayad et al
| [16] | Fayad F, Lefevre-Colau MM, Rannou F et al. Relation of inflammatory Modic changes to intradiscal steroid injection outcome in chronic low back pain. Eur Spine J 2007; 16(7): 925-31. https://doi.org/10.1007/s00586-006-0301-y |
[16]
who found respectively (0.9); (0.5) and (0.7) sex ratio.
This difference could be explained by the fact that the studies took place in different locations and with different populations.
The highest age range was between 40-59 with an average age of 49.5. This result is higher than those of:
1) C. Nguyen et al
| [15] | Nguyen C, Boutron I, Baron G et al. Intradiscal glucocorticoid injection for patients with chronic low back pain associated with active discopathy: a randomized. https://doi.org/10.7326/M16-1700 |
[15]
who found an average age of 46 years.
2) F. Fayad et al
| [16] | Fayad F, Lefevre-Colau MM, Rannou F et al. Relation of inflammatory Modic changes to intradiscal steroid injection outcome in chronic low back pain. Eur Spine J 2007; 16(7): 925-31. https://doi.org/10.1007/s00586-006-0301-y |
[16]
who found an age range between 32–70 years with an average age of 47.9 years.
3) I Braithwaite
| [13] | Braithwaite, J. White, A. Saifuddin, P. Renton, B. A. Taylor Vertebral end-plate (Modic) changes on lumbar spine MRI: correlation with pain reproduction at lumbar discography Eur Spine J (1998) 7: 363–368. https://doi.org/10.1007/s005860050091 |
[13]
who found an average age of 42 years with extremes of 21–63 years.
This result is lower than that of M. Kouyaté
| [12] | KOUYATE M. scan-guided spinal infiltrations of active discopathies at the lumbar level in the radiology department of the chu of gouadeloupe. Thesis in medicine. FMOS; 2023: 121. |
[12]
who found an age range of 60-79 years with an average age of 59.5 years.
The average age of our patients is a little higher than these last three studies, which could be explained by the fact that patients most often consult the specialist late.
4.3. The Lesion Topography (Table 4) The lesions were more localized at the L5-S1 level, i.e. 31 patients (62%) followed by the L4-L5 level (17 patients).
This result is comparable to those:
1) -Mr. Kouyaté
| [12] | KOUYATE M. scan-guided spinal infiltrations of active discopathies at the lumbar level in the radiology department of the chu of gouadeloupe. Thesis in medicine. FMOS; 2023: 121. |
[12]
who found 10 patients with low back pain on the L5-S1 level and 6 patients on the L4-L5 level.
2) From I. Braithwaite
| [13] | Braithwaite, J. White, A. Saifuddin, P. Renton, B. A. Taylor Vertebral end-plate (Modic) changes on lumbar spine MRI: correlation with pain reproduction at lumbar discography Eur Spine J (1998) 7: 363–368. https://doi.org/10.1007/s005860050091 |
[13]
out of a total of 31 patients with modic type modification, 16 patients had low back pain at the L5-S1 level followed by 10 patients at the L4-L5 level.
3) From F. Fayad et al
| [16] | Fayad F, Lefevre-Colau MM, Rannou F et al. Relation of inflammatory Modic changes to intradiscal steroid injection outcome in chronic low back pain. Eur Spine J 2007; 16(7): 925-31. https://doi.org/10.1007/s00586-006-0301-y |
[16]
found 33 patients with low back pain at the L5-S1 level and 30 patients at the L4-L5 level.
This could be explained by the fact that the preferential location of active disc disease was L5-S1 or L4-L5.
4.4. Infiltration Routes (Table 5, Figures 1, 2, 3 and 4) The majority of patients had epidural infiltration alone (64%) followed by foraminal infiltration alone (28%).
More than half of the patients had a major regression in pain intensity one month after infiltration compared to the pain intensity before infiltration.
This result was close to those:
Kouyaté M.
| [12] | KOUYATE M. scan-guided spinal infiltrations of active discopathies at the lumbar level in the radiology department of the chu of gouadeloupe. Thesis in medicine. FMOS; 2023: 121. |
[12]
who had epidural infiltration alone in 63.2% followed by intradisc infiltration alone in 21.1%.
From J. Beaudreuil et al.
| [17] | Beaudreuil J, Dieude P, Poiraudeau S, Revel M. Disabling chronic low back pain with Modic type 1 MRI signal: acute reduction in pain with intradiscal corticotherapy. Ann PhysRehabil Med 2012; 55(3): 139-47. https://doi.org/10.1016/j.rehab.2012.01.004 |
[17]
and De F. Fayad et al
| [16] | Fayad F, Lefevre-Colau MM, Rannou F et al. Relation of inflammatory Modic changes to intradiscal steroid injection outcome in chronic low back pain. Eur Spine J 2007; 16(7): 925-31. https://doi.org/10.1007/s00586-006-0301-y |
[16]
who only performed intradisc infiltration.
This could be explained by the fact that we used intradisc, epidural routes and a combination of epidural and foraminal routes in order to provide complete treatment of foraminal inflammatory pathologies on the one hand, and on the other hand to demonstrate that epidural infiltrations are as effective as intradisc infiltrations in active low back pain.
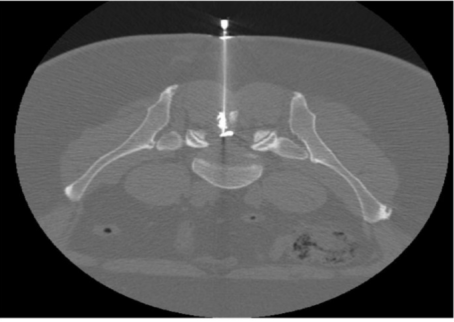
Figure 5. 57-year-old woman admitted to the department for severe lower back pain.
Opacification of the epidural space after positioning the needle in the epidural space at the right L4-L5 level.
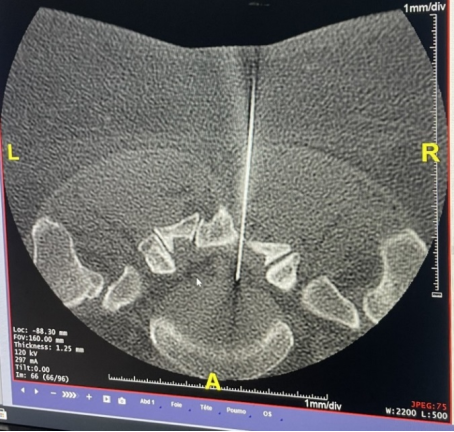
Figure 6. 50-year-old man admitted for lower back pain.
Opacification of the right L5-S1 foraminal space with passage of the contrast product into the epidural space.
Figure 7. 43-year-old men admitted for infiltration at the L5-S1 level.
Figure 8. 59-year-old woman admitted for CT-guided infiltration.
4.5. Impact of the Infiltration on the Intensity of Pain After One Month (Tables 7 and 8) We observed a clear reduction in pain in patients one month after corticosteroid infiltration with pain intensity estimated between 3-5 (VAS) in 33 patients out of 50 patients.
Our results were in agreement with other studies which also showed a significant improvement one month after the injection of corticosteroids: for which we found in:
M. KOUYATE
| [12] | KOUYATE M. scan-guided spinal infiltrations of active discopathies at the lumbar level in the radiology department of the chu of gouadeloupe. Thesis in medicine. FMOS; 2023: 121. |
[12]
who reported a reduction in pain intensity of less than or equal to 5 VAS, i.e. 14 patients out of 19 patients.
F. Fayad et al
| [16] | Fayad F, Lefevre-Colau MM, Rannou F et al. Relation of inflammatory Modic changes to intradiscal steroid injection outcome in chronic low back pain. Eur Spine J 2007; 16(7): 925-31. https://doi.org/10.1007/s00586-006-0301-y |
[16]
reported a reduction in the VAS (Visual Analogue Scale) score 1 month after a corticosteroid injection in 74 patients suffering from low back pain due to disc damage: the reduction was 30.2% in the group Modic 1, 29.4% in the predominant Modic 1 group, versus 5.3% in the Modic 2 group (p = 0.009 and p = 0.017, respectively). Efficacy at 3 and 6 months seemed to be better in the Modic 1 and Modic 1 predominant groups, without being statistically significant
.
These results were explained by the fact that infiltrations have a positive effect on active disc disease and provide relief to patients.
4.6. Complications Linked to the Procedure
Indeed, in our study, no complications were noted. Our study made it possible to understand that if the procedure is carried out in an expert center, by a specialist who takes all precautions, the conditions are met to limit complications.
5. Conclusion
Certainly, lumbar infiltration plays an important role in the treatment of active disc disease. Our study demonstrates that epidural infiltrations can be an alternative in the overall management of inflammatory disc disease.
Abbreviations
MRI | Magnetic Resonance Imaging |
ATCD | Medical History |
VAS | Visual Analogg Scale |
CT | Scanner |
SE | Standard Errors |
SIMS | Musculo-skeletal Imaging Sociey |
CHU | University Hospital Center |
Author Contributions
Mariko Mahamane: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Camara Mamoudou: Conceptualization, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing
Maiga Abdoul Salam: Conceptualization, Writing – original draft, Writing – review & editing
Abdoul Nasser Kimba Bana: Conceptualization, Formal Analysis, Investigation, Software, Writing – original draft, Writing – review & editing
Dena Emmanuel: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Mader R, Lavi I, Luboshitzky R, Evaluation of the pitutary-adrenal axis function following simple intra articular injection of methyl prednisolone. Arthritis Rheun. 2005(52): 924-928.
|
| [2] |
Manchikanti, Laxmaiah, Vidyasagar Pampati, and Joshua A. Hirsch. Retrospective Cohort Study of Usage Patterns of Epidural Injections for Spinal pain in the US Fee-for-service Medicare Population from 2000 to 2014 6(13 2016); e013042,
https://doi.org/10.1002/art.20884
|
| [3] |
Diehn, Felix E, Naveen S, Murthy, and Timothy P. Maus. Science to Practice: What Causes Arterial Infarction in Transforaminal Epidural Steroid Injections, and Which Steroid Is Safe? Radiology 279(2016): 657-59.
https://doi.org/10.1148/radiol.2016160171
|
| [4] |
Evans, william. Intrasacral Epidural Injection in the treatment of Sciatica. The Lancet 216(1930): 1225-29.
https://doi.org/10.1016/S0140-6736(00)86498-3
|
| [5] |
Meulen, Bastiaan C. ter, Esther T. Maas, Amrita Vyas, Marinus van der vegt, Koo de Priester, Michiel R. de Boer, et al. Treatment of Acute Sciatica with Transforaminal Epidural Corticosteroids and Local Anesthetic: Design of a Randomized Controlled Trial. BMC Musculosketal Disorders 18(2017): 215.
https://doi.org/10.1186/s12891-017-1571-8
|
| [6] |
Nguyen C, Bénichou M, Revel M, Poiraudeau S, Rannou F. Association of accelerated switch from vertebral end-plate Modic I to Modic 0 signal changes with clinical benefit of intradiscal corticosteroid injection for chronic low back pain. American College of Rheumatology 2011; Volume 3, pages: 2828-2831.
https://doi.org/10.1002/art.30443
|
| [7] |
Mayo Clinic Staff. Herniated Disk -Symptoms and Causes. Mayo Clinic. 2019. Pages 15-67.
|
| [8] |
Changes to the conditions of use of hydrocortancyl 2.5%, suspension for injection (prednisolone acetate), Available at
http://www.sanofi.fr
|
| [9] |
Cotten, A, J-L Drapé, N Sans, A Feydy, J-M Bartoli, and J-F Meder. Recommendations from SIMS, SFR and FRI-SFR Concerning Corticosteroids Injected Epidurally and Foraminal, 2017.
https://doi.org/10.1016/j.diii.2018.01.012
|
| [10] |
Thomas, E, C. Cyteval, L. Abiad, M. C. Picot, P. Taourel, and F. Blotman. Efficacy of Transforaminal versus Interspinous Corticosteroid Injectionin Discal Radiculalgia? A Prospective, Randomized, Double-Blind Study 22(1, 2003): 299-304.
https://doi.org/10.1007/s10067-003-0736-z
|
| [11] |
Rhee, John M, Tim Yoon, and K. Daniel Riew. Cervical Radiculopathy. The Journal of the American Academy of Orthopedic Surgeons 15 (2007): 486-94,
https://doi.org/10.5435/00124635-200708000-00005
|
| [12] |
KOUYATE M. scan-guided spinal infiltrations of active discopathies at the lumbar level in the radiology department of the chu of gouadeloupe. Thesis in medicine. FMOS; 2023: 121.
|
| [13] |
Braithwaite, J. White, A. Saifuddin, P. Renton, B. A. Taylor Vertebral end-plate (Modic) changes on lumbar spine MRI: correlation with pain reproduction at lumbar discography Eur Spine J (1998) 7: 363–368.
https://doi.org/10.1007/s005860050091
|
| [14] |
Guillaume Dervin. Active disc disease, an infectious etiology Medicine thesis year 2016 Paris Descartes University - Faculty of Medicine of France.
|
| [15] |
Nguyen C, Boutron I, Baron G et al. Intradiscal glucocorticoid injection for patients with chronic low back pain associated with active discopathy: a randomized.
https://doi.org/10.7326/M16-1700
|
| [16] |
Fayad F, Lefevre-Colau MM, Rannou F et al. Relation of inflammatory Modic changes to intradiscal steroid injection outcome in chronic low back pain. Eur Spine J 2007; 16(7): 925-31.
https://doi.org/10.1007/s00586-006-0301-y
|
| [17] |
Beaudreuil J, Dieude P, Poiraudeau S, Revel M. Disabling chronic low back pain with Modic type 1 MRI signal: acute reduction in pain with intradiscal corticotherapy. Ann PhysRehabil Med 2012; 55(3): 139-47.
https://doi.org/10.1016/j.rehab.2012.01.004
|
Cite This Article
-
APA Style
Mahamane, M., Mamoudou, C., Salam, M. A., Alassane, D. S., Bana, A. N. K., et al. (2025). Evaluation of the Practice of CT-guided Lumbar Infiltration at the Mother Hospital Center Child “The Luxemburg”. American Journal of Psychiatry and Neuroscience, 13(1), 16-23. https://doi.org/10.11648/j.ajpn.20251301.13
 Copy
|
Copy
|
 Download
Download
ACS Style
Mahamane, M.; Mamoudou, C.; Salam, M. A.; Alassane, D. S.; Bana, A. N. K., et al. Evaluation of the Practice of CT-guided Lumbar Infiltration at the Mother Hospital Center Child “The Luxemburg”. Am. J. Psychiatry Neurosci. 2025, 13(1), 16-23. doi: 10.11648/j.ajpn.20251301.13
Copy
|
Download
AMA Style
Mahamane M, Mamoudou C, Salam MA, Alassane DS, Bana ANK, et al. Evaluation of the Practice of CT-guided Lumbar Infiltration at the Mother Hospital Center Child “The Luxemburg”. Am J Psychiatry Neurosci. 2025;13(1):16-23. doi: 10.11648/j.ajpn.20251301.13
Copy
|
Download
-
@article{10.11648/j.ajpn.20251301.13,
author = {Mariko Mahamane and Camara Mamoudou and Maiga Abdoul Salam and Diallo Seydou Alassane and Abdoul Nasser Kimba Bana and Keita Adama Diaman and Dena Emmanuel},
title = {Evaluation of the Practice of CT-guided Lumbar Infiltration at the Mother Hospital Center Child “The Luxemburg”},
journal = {American Journal of Psychiatry and Neuroscience},
volume = {13},
number = {1},
pages = {16-23},
doi = {10.11648/j.ajpn.20251301.13},
url = {https://doi.org/10.11648/j.ajpn.20251301.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajpn.20251301.13},
abstract = {The objectives of this study were to determine the main indications for CT-guided lumbar infiltrations, to list the clinical picture post-CT-guided lumbar infiltration and to describe the intensity of pain post-CT-guided lumbar infiltration in the radiology department. This was a descriptive study to be collected prospectively over a period of seven months from June 2023 to December 2023 relating to CT-guided lumbar infiltration in the radiology and medical imaging department of the Mother Hospital. Child “Luxembourg”. It focused on patients aged 20 to 80 years and over, admitted and having performed a CT-guided infiltration in our department during the period. We glued 50 patients during our study. The 40-59 age group was the most common, at 54%. There is a male predominance with a sex ratio equal to 1.08. The maximum number of patients came from the neurology department (78%). Patients without medical care were the most represented, i.e. 60%. 64% of our patients have not had any infiltration in the last six months. Patients with pain lasting less than 6 months were the most represented, i.e. 40%. The level of pain intensity increasing between 5-7 (severe pain) was the most represented, i.e. 58%. The visual analog scale after three months was estimated between 1-3 and was the most represented, i.e. 70%. The visual analog scale (VAS) estimated between 3-5 after one month was the most represented, i.e. 66%. Discopathy represented 47% followed by the combination of herniated disc and disc disease, i.e. 26.4%. The lesions were more localized at the L5-S1 level, i.e. 62%. Epidural infiltration was performed in 66% of our patients. The complication rate was 0% due to the strict hygiene conditions applied for each procedure. Infiltration is very important in the treatment of active disc disease. Our study demonstrates that epidural infiltrations can be an alternative in the overall management of inflammatory disc disease.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Evaluation of the Practice of CT-guided Lumbar Infiltration at the Mother Hospital Center Child “The Luxemburg”
AU - Mariko Mahamane
AU - Camara Mamoudou
AU - Maiga Abdoul Salam
AU - Diallo Seydou Alassane
AU - Abdoul Nasser Kimba Bana
AU - Keita Adama Diaman
AU - Dena Emmanuel
Y1 - 2025/02/17
PY - 2025
N1 - https://doi.org/10.11648/j.ajpn.20251301.13
DO - 10.11648/j.ajpn.20251301.13
T2 - American Journal of Psychiatry and Neuroscience
JF - American Journal of Psychiatry and Neuroscience
JO - American Journal of Psychiatry and Neuroscience
SP - 16
EP - 23
PB - Science Publishing Group
SN - 2330-426X
UR - https://doi.org/10.11648/j.ajpn.20251301.13
AB - The objectives of this study were to determine the main indications for CT-guided lumbar infiltrations, to list the clinical picture post-CT-guided lumbar infiltration and to describe the intensity of pain post-CT-guided lumbar infiltration in the radiology department. This was a descriptive study to be collected prospectively over a period of seven months from June 2023 to December 2023 relating to CT-guided lumbar infiltration in the radiology and medical imaging department of the Mother Hospital. Child “Luxembourg”. It focused on patients aged 20 to 80 years and over, admitted and having performed a CT-guided infiltration in our department during the period. We glued 50 patients during our study. The 40-59 age group was the most common, at 54%. There is a male predominance with a sex ratio equal to 1.08. The maximum number of patients came from the neurology department (78%). Patients without medical care were the most represented, i.e. 60%. 64% of our patients have not had any infiltration in the last six months. Patients with pain lasting less than 6 months were the most represented, i.e. 40%. The level of pain intensity increasing between 5-7 (severe pain) was the most represented, i.e. 58%. The visual analog scale after three months was estimated between 1-3 and was the most represented, i.e. 70%. The visual analog scale (VAS) estimated between 3-5 after one month was the most represented, i.e. 66%. Discopathy represented 47% followed by the combination of herniated disc and disc disease, i.e. 26.4%. The lesions were more localized at the L5-S1 level, i.e. 62%. Epidural infiltration was performed in 66% of our patients. The complication rate was 0% due to the strict hygiene conditions applied for each procedure. Infiltration is very important in the treatment of active disc disease. Our study demonstrates that epidural infiltrations can be an alternative in the overall management of inflammatory disc disease.
VL - 13
IS - 1
ER -
Copy
|
Download