Background: Connective Tissue Disease (CTD) in children may involve the laryngeal muscles and structures, leading to voice disorders that can significantly affect communication and quality of life. Objectives: This study aimed to assess voice disorders in children with CTD using the Pediatric Voice Handicap Index (pVHI) score and Fiber Optic Laryngoscopy (FOL), and to analyze the association between these two parameters. Methods: This study included children aged 1–18 years diagnosed with CTD. The pVHI was used as a subjective tool for voice assessment (scores ≥10.5 indicated pathology), while FOL was used as an objective tool to evaluate the anatomy and physiology of the vocal folds and surrounding cartilages. The association between pVHI and FOL findings was assessed using the chi-square test with kappa agreement analysis. Results: There were 33 patients with SLE and 5 patients with other CTDs. Eight out of 38 children demonstrated high pVHI scores, while 30 out of 38 demonstrated low pVHI scores. Arytenoid hyperemia was the most frequent inflammatory finding (n = 7), followed by hyperemia of the vocal folds (n = 5). Edema was observed in the arytenoids (n = 2), as well as in the vocal folds and ventricular folds (n = 1 each). Hyperemia of the epiglottis and ventricular folds was each noted in one patient. A pVHI score ≥10.5 showed a significant association with abnormal FOL findings (OR = 8.250; 95% CI: 1.373–49.574; p = 0.012). The agreement between pVHI scores ≥10.5 and abnormal FOL findings was moderate (Kappa = 0.379, p = 0.012). Conclusions: The prevalence of voice disorders was identified in a substantial proportion (36.8%) of children with CTD. pVHI scores ≥10.5 were significantly associated with abnormal findings on fiber optic laryngoscopy. However, the pVHI alone cannot be used to diagnose voice disorders because its agreement with FOL findings was only moderate.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Connective Tissue Disease, Voice Disorder, Voice Handicap Index
1. Introduction
Connective Tissue Disease (CTD) in children, such as systemic lupus erythematosus (SLE), dermatomyositis, systemic sclerosis, and mixed connective tissue disease (MCTD), is a chronic multisystem autoimmune disorder characterized by the production of autoantibodies and immune complex deposition, leading to widespread inflammation and organ damage. While CTD has been predominantly studied for its renal, neurological, and dermatological manifestations, voice impairment has also been documented in adults with CTD. However, there is still a paucity of research focusing on the pediatric population
[1]
Ormazabal A, Cañete JD, Espinosa G, et al. Connective tissue diseases in childhood: epidemiology, clinical features, diagnostic procedures and treatment. J Clin Pediatr. 2005; 39(2): 80–90.
[1]
.
The incidence of SLE in children in the Asia-Pacific region is approximately 0.9–3.1 per 100,000 population per year, with a prevalence of 4.3–45.3 per 100,000 population. The impact of CTD on voice disorders in children has also been observed clinically, with two severe cases of voice disorder, including aphonia, documented at Prof. I. G. N. G. Ngoerah General Hospital. These findings suggest that CTD may affect laryngeal structures, leading to voice disorders
[2]
Pusat Data dan Informasi Kementerian Kesehatan Republik Indonesia. Situasi Lupus di Indonesia. Jakarta: PUSDATIN; 2017.
[2]
.
Laryngeal involvement in CTD, although under-reported, may manifest as mucosal inflammation, vocal fold edema, cricoarytenoid arthritis, and even vocal fold paralysis. These pathological changes can significantly affect voice quality and may impair a child’s communication, social interactions, emotional well-being, and overall quality of life. Despite these potential impairments, voice assessment is not routinely integrated into the clinical evaluation of pediatric CTD patients, which may result in the underdiagnosis of voice disorders in this population
[3]
acobson BH, Johnson A, Grywalski C, et al. The Voice Handicap Index (VHI): Development and Validation. Am J Speech Lang Pathol. 1997; 6(3): 66-70.
[4]
Zur KB, Cotton S, Kelchner L, et al. Pediatric Voice Handicap Index (pVHI): A New Tool for Evaluating Pediatric Dysphonia. Int J Pediatr Otorhinolaryngol. 2007; 71(1): 77-82.
[3, 4]
.
The Pediatric Voice Handicap Index (pVHI) is a validated caregiver-reported instrument used to assess the functional, emotional, and physical impact of voice disorders in children. The pVHI provides a subjective assessment of voice-related quality of life and may help identify children requiring further otolaryngological evaluation
[3]
acobson BH, Johnson A, Grywalski C, et al. The Voice Handicap Index (VHI): Development and Validation. Am J Speech Lang Pathol. 1997; 6(3): 66-70.
[4]
Zur KB, Cotton S, Kelchner L, et al. Pediatric Voice Handicap Index (pVHI): A New Tool for Evaluating Pediatric Dysphonia. Int J Pediatr Otorhinolaryngol. 2007; 71(1): 77-82.
[5]
Cialente F, Torsello M, Meucci D, et al. Pediatric Voice Handicap Index (pVHI): A Tool for Evaluating the Reliability and Validity of Voice Therapy in Children With Benign Vocal Fold Nodules. J Voice. 2024 Nov; 38(6): 1527. e21-1527. e26.
Given the limited evidence regarding voice disorders in pediatric CTD populations, further investigation is needed to better understand the prevalence and clinical significance of laryngeal involvement in these patients.
[6]
Kılıç MA, Okur E, Yildirim I, et al. Reliability and Validity of the Turkish Version of the Pediatric Voice Handicap Index. J Voice. 2012; 26(5): 687. e19-687. e23.
[7]
Maio VD, Mozzanica F, Cardella A, et al. Normative Values for the Children's Voice Handicap Index-10 (CVHI-10) and for the Children Voice Handicap Index-10 for Parents (CVHI-10-P). J Voice. 2024 Aug 13: S0892-1997(24)00222-4.
Therefore, this study aimed to assess voice disorders in pediatric CTD patients using the pVHI and fiberoptic laryngoscopy, and to analyze the association between these two parameters.
2. Materials and Methods
This was a cross-sectional study conducted at pediatric Allergy, Immunology, and Rheumatology Division and the otolaryngology outpatient clinic of Prof. I. G. N. G. Ngoerah General Hospital from March to June 2025.
The research population was children diagnosed with CTD at Prof. Dr. I. G. N. G. Ngoerah General Hospital, and the target population consisted of those who attended the hospital from March to June 2025. The inclusion criteria were children aged 1–18 years, having a current or previous history of voice problems, children or parents who were able to read and write, and accessible and complete electronic medical record data. The exclusion criteria were patients who refused to participate in completing the questionnaire, refused to undergo the laryngoscopy procedure, had a history of congenital voice disorders, neurological diseases affecting phonation, recent or active upper respiratory tract infections, intubation, head and neck trauma, or decreased consciousness.
Samples were collected using consecutive sampling. All patients who met the inclusion criteria were included in the study. The minimum sample size calculation for an analytical comparative study with unpaired categorical data resulted in a required sample size of 32 participants.
The data collected in this study included age, gender, initial diagnosis, duration of CTD treatment, and voice disorder. The operational definitions of the variables were as follows: Age was the chronological age at the time of sampling. Age was calculated based on the date, month and year of birth, and is expressed in full years. The variable was presented as continuous data. Gender was determined based on phenotypic appearance. The variable was presented as categorical data, with the categories (1) male and (2) female. Connective Tissue Disease was defined as a chronic multisystem autoimmune condition in children treated at the Pediatric Allergy, Immunology, and Rheumatology Division.
Voice disorder was assessed using the Pediatric Voice Handicap Index (pVHI) and flexible laryngoscopy. Either the child or their parents can complete the pVHI, which assesses functional, physical, and emotional aspects of voice disorders in children. A cut-off point of 10.5 with 95.9% sensitivity and 92.5% specificity was determined for the overall score of the pVHI. Patients with a pVHI score ≥10.5 were considered abnormal
[13]
Guimarães, I., Almeida, L., Quintal, A., Batista, A. P., Teixeira, A., Romeiro, C., Ferreira, D. B., Fernandes, I. S., Saraiva, M., Bom, R., Almeida, S., & Freitas, S. V. (2023). Pediatric Voice Handicap Index (pVHI): Validation in European Portuguese Children. Journal of voice: official journal of the Voice Foundation, 37(5), 804. e11–804. e19.
Objective Voice Analysis was performed using flexible laryngoscope to identify structural laryngeal abnormalities. Flexible laryngoscopy examinations were performed by a single Ear-Nose-Throat specialist in the outpatient clinic according to standard operational procedures
[9]
De Macedo MSFC, Costa KM, da Silva Filho M. Voice disorder in systemic lupus erythematosus. PLoS One. 2017; 12(4): e0175893. Published 2017 Apr 17.
The research instruments consisted of electronic medical record data from Prof. I. G. N. G. Ngoerah General Hospital, the pVHI questionnaire, and flexible laryngoscopy findings evaluated by an ENT consultant.
Data analysis was conducted with descriptive statistics (mean ± SD, frequencies) for pVHI scores and clinical variables. The association between pVHI scores and flexible laryngoscopy findings was assessed using the chi-square test and kappa agreement analysis in SPSS version 25.
Ethical clearance was obtained from the Institutional Ethical Committee of the Faculty of Medicine, Universitas Udayana Ngoerah Hospital with approval number DP.04.03/D.XVII.2.2.2/35903/2025. Research permission was secured before accessing medical records from Ngoerah Hospital with number 1108/UN14.2.2.VII.14/LT/2025.
3. Results
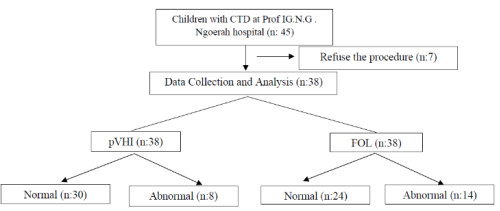
There were 45 children diagnosed with CTD during the study period. Seven children refused to undergo the procedure, and 38 children were included in this study as shown in the study flowchart (Figure 1). The characteristics of the study subjects are shown in Table 1.
*Percentages for CTD treatment were calculated based on the total number of treatment regimens because some patients received combination therapy
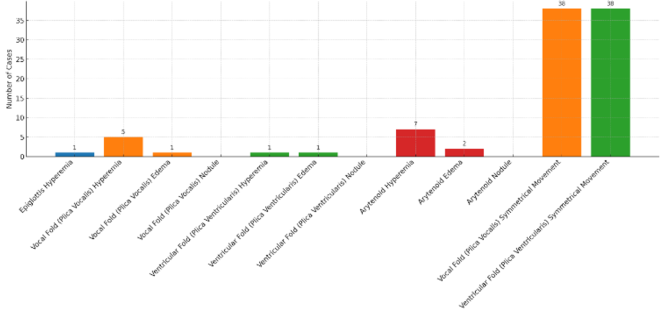
A total of 38 patients underwent flexible fiber optic laryngoscopy to evaluate laryngeal structures (Figure 2). The most common finding was symmetrical movement of the vocal folds, observed in all 38 cases. Arytenoid hyperemia was the most frequent inflammatory finding (n = 7), followed by hyperemia of the vocal folds (n = 5). Arytenoid edema was observed in 2 patients, while edema of the vocal folds and ventricular folds was observed in 1 patient each. Hyperemia of the epiglottis and ventricular folds was each noted in one patient. No nodules were identified in any laryngeal subsite.
The Pediatric Voice Handicap Index (pVHI) score showed a statistically significant association with abnormal findings on fiber optic laryngoscopy (FOL). The odds of having laryngeal structural abnormalities were significantly greater in children with pVHI scores ≥10.5 (OR = 8.250; 95% CI: 1.373–49.574; p = 0.012). The agreement between pVHI score classification and FOL findings was moderate (Kappa = 0.379, p = 0.012) (Table 2).
Figure 2. Distribution of Fiber Optic Laryngoscopy.
Table 2. Association Between pVHI scores and Fiber Optic Laryngoscopy.
Variable
FOL Abnormal
FOL Normal
OR
95% CI
P value*
Kappa
Kappa p value
pVHI scores
≥10.5
6 (75.0%)
2 (25.0%)
8.250
1.373–49.574
0.012
0.379
0.012
<10.5
8 (26.7%)
22 (73.3%)
4. Discussion
Our study results demonstrated that voice disorders were identified in 14 patients (36.8%) based on FOL findings and in 8 patients (21.1%) based on pVHI scores, highlighting that voice disorders are common in pediatric CTD populations. This finding is important, as voice disorders may be under-recognized in children with chronic systemic conditions, yet they can significantly affect communication, emotional well-being, and quality of life.
In a cross-sectional analysis by Sanz et al. (2010) involving 140 participants, the prevalence of voice disorders was significantly higher in patients with SLE, rheumatoid arthritis (RA), and Sjögren’s syndrome (SS) (32–38%) compared to healthy controls (5–8%). Among the three conditions, SLE had the highest risk for voice disorders (OR = 3.07), consistent with our study in which SLE patients also showed a high prevalence of voice disorders and structural abnormalities on laryngoscopy. Interestingly, Sanz et al. found no significant correlation between voice disorder and biochemical markers such as complement levels or anti-dsDNA during disease flares, suggesting that voice disorders may not always align with traditional measures of disease activity
[8]
Sanz L, Cuende E, Rivera T. Prevalence of dysphonia in immunomediated diseases. Otolaryngol Head Neck Surg. 2010; 143(2_suppl): P217.
Our findings are consistent with prior studies suggesting that autoimmune conditions may affect vocal function. Notably, Macedo et al. (2017) demonstrated that patients with SLE exhibit significant alterations in both objective vocal parameters (such as decreased vocal intensity, increased jitter, and shimmer) and subjective vocal quality, as assessed by the GRBAS scale. Moreover, a large proportion of SLE patients in that study reported symptoms such as vocal fatigue and hoarseness, which were significantly correlated with tissue damage scores, suggesting a direct relationship between disease burden and voice dysfunction
[9]
De Macedo MSFC, Costa KM, da Silva Filho M. Voice disorder in systemic lupus erythematosus. PLoS One. 2017; 12(4): e0175893. Published 2017 Apr 17.
In a systematic review by De La Chapa et al. (2025), Autoimmune Associated Vocal Fold Lesions (AaVFLs) were documented across 83 patients. These lesions were often bilateral (83.8%) and frequently occurred in individuals with pre-established autoimmune diagnoses such as rheumatoid arthritis, systemic lupus erythematosus, and mixed connective tissue disease (75.9%). Notably, 25% of patients first presented to otolaryngologists before being diagnosed with an underlying autoimmune condition, suggesting that vocal fold changes may be an early or sentinel manifestation of systemic disease
[10]
Chapa J, Jonas RH, Weidman AA, et al. Autoimmune Associated Vocal Fold Lesions: A Systematic Review. J Voice. 2025; 39(3): 744-751.
A large-scale US-based study by Fujiki and Thibeault (2024) reported a point prevalence of voice problems of 6.7% and a lifetime prevalence of 12% among school-aged children.
[14]
Fujiki RB, Thibeault SL. Voice Disorder Prevalence and Vocal Health Characteristics in Children. JAMA Otolaryngol Head Neck Surg. 2024; 150(8): 677-687.
The higher prevalence observed in our study may be related to the distinct characteristics of pediatric CTD patients, in whom chronic inflammation and systemic involvement may affect laryngeal function. Swain et al. (2022) reported that vocal fold lesions are common in children, with vocal fold nodules and hoarseness being the most frequent findings. Voice abuse was identified as a major etiological factor in their study
[11]
Swain SK, Dubey D. Vocal fold lesions in the pediatric age group: our experiences at a tertiary care teaching hospital of India. Int J Contemp Pediatr. 2022; 9(10): 946-951.
In that case, voice loss occurred in the context of systemic manifestations including hematologic abnormalities, proteinuria, brain atrophy, and serologic evidence of high disease activity. Fiber optic laryngoscopy confirmed bilateral vocal cord paralysis, and treatment with high-dose methylprednisolone, cyclophosphamide, and speech therapy led to gradual improvement. This case illustrates that while rare, direct laryngeal involvement can occur in SLE and should be considered in patients with sudden voice changes, particularly in the context of active systemic disease
All children with MCTD and psoriasis in this study exhibited voice disorder, suggesting a possible increased risk in these subtypes, although the small sample sizes precluded statistical significance. These results are consistent with previous literatures that suggests autoimmune processes may involve the larynx, either through mucosal inflammation, muscle involvement, neuropathic mechanisms, systemic fatigue, or medication effects
[8]
Sanz L, Cuende E, Rivera T. Prevalence of dysphonia in immunomediated diseases. Otolaryngol Head Neck Surg. 2010; 143(2_suppl): P217.
Connective tissue diseases can impair voice quality through inflammatory, neurological, and systemic mechanisms. Chronic inflammation may affect the laryngeal mucosa and vocal folds, leading to edema, fibrosis, or atrophy that disrupt normal phonation and cause hoarseness or reduced vocal quality. Autoimmune involvement of the cranial or recurrent laryngeal nerves may also result in vocal cord paresis or paralysis. In addition, systemic fatigue and musculoskeletal involvement in CTD can reduce respiratory and phonatory muscle endurance, contributing to vocal fatigue and increased effort during speech, particularly during disease flares
[8]
Sanz L, Cuende E, Rivera T. Prevalence of dysphonia in immunomediated diseases. Otolaryngol Head Neck Surg. 2010; 143(2_suppl): P217.
Mucosal dryness, as seen in Sjögren’s syndrome, contributes to friction during vocal fold vibration and impairs resonance. Glandular dysfunction leads to dryness of the laryngeal and oropharyngeal mucosa, producing a harsh, strained voice quality. Additionally, joint involvement, such as cricoarytenoid arthritis in RA, may restrict vocal fold mobility, causing further voice disorder and pitch control issues. Medication effects also play a role. Long-term corticosteroid use can lead to vocal fold thinning or steroid-induced myopathy, while immunosuppressive therapies may predispose patients to opportunistic infections, such as laryngeal candidiasis, which can alter voice quality
[8]
Sanz L, Cuende E, Rivera T. Prevalence of dysphonia in immunomediated diseases. Otolaryngol Head Neck Surg. 2010; 143(2_suppl): P217.
One of the key findings in this study is the significant association between pVHI scores ≥10.5 and abnormal findings on FOL. Children with elevated pVHI scores were more likely to present with structural abnormalities such as arytenoid or vocal fold hyperemia and edema. This reinforces the value of the pVHI as a screening instrument for identifying children at risk of laryngeal pathology, with the potential to guide referrals for further otolaryngological evaluation. The moderate agreement between pVHI scores and FOL findings (kappa = 0.379, p = 0.012) supports the integration of both subjective and objective assessments in clinical practice
[9]
De Macedo MSFC, Costa KM, da Silva Filho M. Voice disorder in systemic lupus erythematosus. PLoS One. 2017; 12(4): e0175893. Published 2017 Apr 17.
The pVHI is a validated caregiver-reported adaptation of the adult Voice Handicap Index (VHI) designed to assess the impact of voice disorders in children. It evaluates functional, physical, and emotional aspects of voice-related problems and has demonstrated good reliability and validity in pediatric populations. In the context of CTD, where voice disorders may be subtle or overlooked, the pVHI may serve as a useful screening and follow-up tool for identifying children who require further otolaryngological evaluation or intervention
[4]
Zur KB, Cotton S, Kelchner L, et al. Pediatric Voice Handicap Index (pVHI): A New Tool for Evaluating Pediatric Dysphonia. Int J Pediatr Otorhinolaryngol. 2007; 71(1): 77-82.
[4]
.
The findings of this study have important clinical implications for the screening and management of pediatric CTD patients. Voice disorders may represent an under-recognized manifestation of CTD and can occur even in the absence of severe systemic symptoms. Routine screening using the pVHI may help clinicians identify children at risk of laryngeal involvement at an earlier stage, particularly in patients presenting with hoarseness, vocal fatigue, or communication difficulties. Children with elevated pVHI scores may benefit from further evaluation with fiberoptic laryngoscopy and multidisciplinary management involving pediatric rheumatologists, otolaryngologists, and speech therapists. Early identification and intervention may improve communication abilities, psychosocial well-being, and overall quality of life in children with CTD.
This study has several limitations that may impact the interpretation of the findings. First, the relatively small sample size (n = 38) limits the statistical power, particularly in subgroup analyses, and may reduce the generalizability of the results to broader populations. The small number of participants with less common connective tissue diseases, such as mixed connective tissue disease and psoriasis, further restricts the ability to draw meaningful conclusions within those groups. Second, the cross-sectional design of the study precludes any inference of causality or longitudinal changes in voice function over the course of the disease or treatment. Additionally, as a single-center study, the findings may not be representative of patients in other clinical settings or geographic regions. The reliance on the pVHI introduces the possibility of subjective bias, as the responses are dependent on parental and/or child perception. This study does not assess the factors that influence voice disorder. All FOL examinations were performed by a single ENT specialist, which may have reduced interobserver variability and minimized interpretation bias.
5. Conclusions
The prevalence of voice disorders was substantial (36.8%) among children with CTD. The pVHI scores ≥10.5 were significantly associated with abnormal findings on fiber optic laryngoscopy. However, the pVHI value alone cannot be applied to diagnose voice disorders as the agreement with FOL was moderate. These findings suggest that pVHI may serve as a useful screening tool for early identification of children with CTD who are at risk of laryngeal involvement and may benefit from further otolaryngological evaluation. Further studies with larger sample sizes are warranted to validate the predictive value of pVHI in detecting voice disorders among pediatric CTD patients.
Abbreviations
CI
Confident Interval
CTD
Connective Tissue Disease
ENT
Ear Nose Throat
FOL
Fiber Optic Laryngoscopy
HDMP
High Dose Methylprednisolone
IV
Intravenous
MCTD
Mixed Connective Tissues Disease
OR
Odd Ratio
pVHI
Pediatric Voice Handicap Index
SLE
Systemic Lupus Erythematosus
Author Contributions
Joy Aprianis Haning: Conceptualization, Resources, Writing – original draft
Ketut Dewi Kumara Wati: Data curation, Methodology, Writing – review & editing
The data supporting the outcome of this research work has been reported in this manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Ormazabal A, Cañete JD, Espinosa G, et al. Connective tissue diseases in childhood: epidemiology, clinical features, diagnostic procedures and treatment. J Clin Pediatr. 2005; 39(2): 80–90.
[2]
Pusat Data dan Informasi Kementerian Kesehatan Republik Indonesia. Situasi Lupus di Indonesia. Jakarta: PUSDATIN; 2017.
[3]
acobson BH, Johnson A, Grywalski C, et al. The Voice Handicap Index (VHI): Development and Validation. Am J Speech Lang Pathol. 1997; 6(3): 66-70.
[4]
Zur KB, Cotton S, Kelchner L, et al. Pediatric Voice Handicap Index (pVHI): A New Tool for Evaluating Pediatric Dysphonia. Int J Pediatr Otorhinolaryngol. 2007; 71(1): 77-82.
[5]
Cialente F, Torsello M, Meucci D, et al. Pediatric Voice Handicap Index (pVHI): A Tool for Evaluating the Reliability and Validity of Voice Therapy in Children With Benign Vocal Fold Nodules. J Voice. 2024 Nov; 38(6): 1527. e21-1527. e26.
Kılıç MA, Okur E, Yildirim I, et al. Reliability and Validity of the Turkish Version of the Pediatric Voice Handicap Index. J Voice. 2012; 26(5): 687. e19-687. e23.
[7]
Maio VD, Mozzanica F, Cardella A, et al. Normative Values for the Children's Voice Handicap Index-10 (CVHI-10) and for the Children Voice Handicap Index-10 for Parents (CVHI-10-P). J Voice. 2024 Aug 13: S0892-1997(24)00222-4.
Swain SK, Dubey D. Vocal fold lesions in the pediatric age group: our experiences at a tertiary care teaching hospital of India. Int J Contemp Pediatr. 2022; 9(10): 946-951.
Guimarães, I., Almeida, L., Quintal, A., Batista, A. P., Teixeira, A., Romeiro, C., Ferreira, D. B., Fernandes, I. S., Saraiva, M., Bom, R., Almeida, S., & Freitas, S. V. (2023). Pediatric Voice Handicap Index (pVHI): Validation in European Portuguese Children. Journal of voice: official journal of the Voice Foundation, 37(5), 804. e11–804. e19.
Fujiki RB, Thibeault SL. Voice Disorder Prevalence and Vocal Health Characteristics in Children. JAMA Otolaryngol Head Neck Surg. 2024; 150(8): 677-687.
Haning, J. A., Wati, K. D. K., Putri, P. D. A. (2026). Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy. American Journal of Pediatrics, 12(2), 69-75. https://doi.org/10.11648/j.ajp.20261202.13
Haning, J. A.; Wati, K. D. K.; Putri, P. D. A. Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy. Am. J. Pediatr.2026, 12(2), 69-75. doi: 10.11648/j.ajp.20261202.13
Haning JA, Wati KDK, Putri PDA. Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy. Am J Pediatr. 2026;12(2):69-75. doi: 10.11648/j.ajp.20261202.13
@article{10.11648/j.ajp.20261202.13,
author = {Joy Aprianis Haning and Ketut Dewi Kumara Wati and Putu Dian Ariyanti Putri},
title = {Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy},
journal = {American Journal of Pediatrics},
volume = {12},
number = {2},
pages = {69-75},
doi = {10.11648/j.ajp.20261202.13},
url = {https://doi.org/10.11648/j.ajp.20261202.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20261202.13},
abstract = {Background: Connective Tissue Disease (CTD) in children may involve the laryngeal muscles and structures, leading to voice disorders that can significantly affect communication and quality of life. Objectives: This study aimed to assess voice disorders in children with CTD using the Pediatric Voice Handicap Index (pVHI) score and Fiber Optic Laryngoscopy (FOL), and to analyze the association between these two parameters. Methods: This study included children aged 1–18 years diagnosed with CTD. The pVHI was used as a subjective tool for voice assessment (scores ≥10.5 indicated pathology), while FOL was used as an objective tool to evaluate the anatomy and physiology of the vocal folds and surrounding cartilages. The association between pVHI and FOL findings was assessed using the chi-square test with kappa agreement analysis. Results: There were 33 patients with SLE and 5 patients with other CTDs. Eight out of 38 children demonstrated high pVHI scores, while 30 out of 38 demonstrated low pVHI scores. Arytenoid hyperemia was the most frequent inflammatory finding (n = 7), followed by hyperemia of the vocal folds (n = 5). Edema was observed in the arytenoids (n = 2), as well as in the vocal folds and ventricular folds (n = 1 each). Hyperemia of the epiglottis and ventricular folds was each noted in one patient. A pVHI score ≥10.5 showed a significant association with abnormal FOL findings (OR = 8.250; 95% CI: 1.373–49.574; p = 0.012). The agreement between pVHI scores ≥10.5 and abnormal FOL findings was moderate (Kappa = 0.379, p = 0.012). Conclusions: The prevalence of voice disorders was identified in a substantial proportion (36.8%) of children with CTD. pVHI scores ≥10.5 were significantly associated with abnormal findings on fiber optic laryngoscopy. However, the pVHI alone cannot be used to diagnose voice disorders because its agreement with FOL findings was only moderate.},
year = {2026}
}
TY - JOUR
T1 - Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy
AU - Joy Aprianis Haning
AU - Ketut Dewi Kumara Wati
AU - Putu Dian Ariyanti Putri
Y1 - 2026/06/02
PY - 2026
N1 - https://doi.org/10.11648/j.ajp.20261202.13
DO - 10.11648/j.ajp.20261202.13
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 69
EP - 75
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20261202.13
AB - Background: Connective Tissue Disease (CTD) in children may involve the laryngeal muscles and structures, leading to voice disorders that can significantly affect communication and quality of life. Objectives: This study aimed to assess voice disorders in children with CTD using the Pediatric Voice Handicap Index (pVHI) score and Fiber Optic Laryngoscopy (FOL), and to analyze the association between these two parameters. Methods: This study included children aged 1–18 years diagnosed with CTD. The pVHI was used as a subjective tool for voice assessment (scores ≥10.5 indicated pathology), while FOL was used as an objective tool to evaluate the anatomy and physiology of the vocal folds and surrounding cartilages. The association between pVHI and FOL findings was assessed using the chi-square test with kappa agreement analysis. Results: There were 33 patients with SLE and 5 patients with other CTDs. Eight out of 38 children demonstrated high pVHI scores, while 30 out of 38 demonstrated low pVHI scores. Arytenoid hyperemia was the most frequent inflammatory finding (n = 7), followed by hyperemia of the vocal folds (n = 5). Edema was observed in the arytenoids (n = 2), as well as in the vocal folds and ventricular folds (n = 1 each). Hyperemia of the epiglottis and ventricular folds was each noted in one patient. A pVHI score ≥10.5 showed a significant association with abnormal FOL findings (OR = 8.250; 95% CI: 1.373–49.574; p = 0.012). The agreement between pVHI scores ≥10.5 and abnormal FOL findings was moderate (Kappa = 0.379, p = 0.012). Conclusions: The prevalence of voice disorders was identified in a substantial proportion (36.8%) of children with CTD. pVHI scores ≥10.5 were significantly associated with abnormal findings on fiber optic laryngoscopy. However, the pVHI alone cannot be used to diagnose voice disorders because its agreement with FOL findings was only moderate.
VL - 12
IS - 2
ER -
Department of Child Health, Faculty of Medicine Udayana University, Denpasar, Indonesia
Biography:
Joy Aprianis Haning is a General Pediatrician at Udayana University. He completed the Pediatric Specialist Program in September 2025 and received the 3rd place award in the national pediatric specialist examination. He is interested in the Allergy and Immunology, Nutrition and Metabolic, and Cardiology divisions. He has participated in several research projects in recent years. Joy Aprianis Haning is currently active in community health outreach and focuses on the management of Allergy and Immunology and nutritional disorders in children
Haning, J. A., Wati, K. D. K., Putri, P. D. A. (2026). Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy. American Journal of Pediatrics, 12(2), 69-75. https://doi.org/10.11648/j.ajp.20261202.13
Haning, J. A.; Wati, K. D. K.; Putri, P. D. A. Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy. Am. J. Pediatr.2026, 12(2), 69-75. doi: 10.11648/j.ajp.20261202.13
Haning JA, Wati KDK, Putri PDA. Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy. Am J Pediatr. 2026;12(2):69-75. doi: 10.11648/j.ajp.20261202.13
@article{10.11648/j.ajp.20261202.13,
author = {Joy Aprianis Haning and Ketut Dewi Kumara Wati and Putu Dian Ariyanti Putri},
title = {Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy},
journal = {American Journal of Pediatrics},
volume = {12},
number = {2},
pages = {69-75},
doi = {10.11648/j.ajp.20261202.13},
url = {https://doi.org/10.11648/j.ajp.20261202.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajp.20261202.13},
abstract = {Background: Connective Tissue Disease (CTD) in children may involve the laryngeal muscles and structures, leading to voice disorders that can significantly affect communication and quality of life. Objectives: This study aimed to assess voice disorders in children with CTD using the Pediatric Voice Handicap Index (pVHI) score and Fiber Optic Laryngoscopy (FOL), and to analyze the association between these two parameters. Methods: This study included children aged 1–18 years diagnosed with CTD. The pVHI was used as a subjective tool for voice assessment (scores ≥10.5 indicated pathology), while FOL was used as an objective tool to evaluate the anatomy and physiology of the vocal folds and surrounding cartilages. The association between pVHI and FOL findings was assessed using the chi-square test with kappa agreement analysis. Results: There were 33 patients with SLE and 5 patients with other CTDs. Eight out of 38 children demonstrated high pVHI scores, while 30 out of 38 demonstrated low pVHI scores. Arytenoid hyperemia was the most frequent inflammatory finding (n = 7), followed by hyperemia of the vocal folds (n = 5). Edema was observed in the arytenoids (n = 2), as well as in the vocal folds and ventricular folds (n = 1 each). Hyperemia of the epiglottis and ventricular folds was each noted in one patient. A pVHI score ≥10.5 showed a significant association with abnormal FOL findings (OR = 8.250; 95% CI: 1.373–49.574; p = 0.012). The agreement between pVHI scores ≥10.5 and abnormal FOL findings was moderate (Kappa = 0.379, p = 0.012). Conclusions: The prevalence of voice disorders was identified in a substantial proportion (36.8%) of children with CTD. pVHI scores ≥10.5 were significantly associated with abnormal findings on fiber optic laryngoscopy. However, the pVHI alone cannot be used to diagnose voice disorders because its agreement with FOL findings was only moderate.},
year = {2026}
}
TY - JOUR
T1 - Voice Disorder Analysis in Children with Connective Tissue Disease Using Pediatric Voice Handicap Index and Fiber Optic Laryngoscopy
AU - Joy Aprianis Haning
AU - Ketut Dewi Kumara Wati
AU - Putu Dian Ariyanti Putri
Y1 - 2026/06/02
PY - 2026
N1 - https://doi.org/10.11648/j.ajp.20261202.13
DO - 10.11648/j.ajp.20261202.13
T2 - American Journal of Pediatrics
JF - American Journal of Pediatrics
JO - American Journal of Pediatrics
SP - 69
EP - 75
PB - Science Publishing Group
SN - 2472-0909
UR - https://doi.org/10.11648/j.ajp.20261202.13
AB - Background: Connective Tissue Disease (CTD) in children may involve the laryngeal muscles and structures, leading to voice disorders that can significantly affect communication and quality of life. Objectives: This study aimed to assess voice disorders in children with CTD using the Pediatric Voice Handicap Index (pVHI) score and Fiber Optic Laryngoscopy (FOL), and to analyze the association between these two parameters. Methods: This study included children aged 1–18 years diagnosed with CTD. The pVHI was used as a subjective tool for voice assessment (scores ≥10.5 indicated pathology), while FOL was used as an objective tool to evaluate the anatomy and physiology of the vocal folds and surrounding cartilages. The association between pVHI and FOL findings was assessed using the chi-square test with kappa agreement analysis. Results: There were 33 patients with SLE and 5 patients with other CTDs. Eight out of 38 children demonstrated high pVHI scores, while 30 out of 38 demonstrated low pVHI scores. Arytenoid hyperemia was the most frequent inflammatory finding (n = 7), followed by hyperemia of the vocal folds (n = 5). Edema was observed in the arytenoids (n = 2), as well as in the vocal folds and ventricular folds (n = 1 each). Hyperemia of the epiglottis and ventricular folds was each noted in one patient. A pVHI score ≥10.5 showed a significant association with abnormal FOL findings (OR = 8.250; 95% CI: 1.373–49.574; p = 0.012). The agreement between pVHI scores ≥10.5 and abnormal FOL findings was moderate (Kappa = 0.379, p = 0.012). Conclusions: The prevalence of voice disorders was identified in a substantial proportion (36.8%) of children with CTD. pVHI scores ≥10.5 were significantly associated with abnormal findings on fiber optic laryngoscopy. However, the pVHI alone cannot be used to diagnose voice disorders because its agreement with FOL findings was only moderate.
VL - 12
IS - 2
ER -