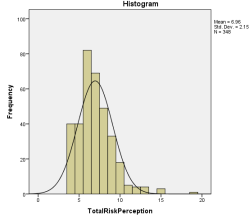
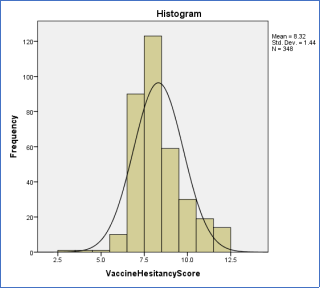
Background: The impact of COVID-19 on people living with HIV (PLWH) is particularly concerning due to their existing health vulnerabilities. The low uptake of the COVID-19 vaccine and the failure to achieve herd immunity highlight the need to address vaccine hesitancy, especially in developing countries battling multiple infectious diseases. Objective: This study aimed to determine the relationship between COVID-19 vaccine risk perception and vaccine hesitancy among PLWH. Materials and Methods: An analytical cross-sectional design was used, involving 348 participants from Parirenyatwa Centre of Excellence, recruited via systematic random sampling. Data collection, following ethical approval, was conducted using a self-administered questionnaire. The data were categorized into structure, process, and outcome, and analyzed with SPSS version 22. Results: The study found that 79.9% of PLWH perceived a risk in taking the COVID-19 vaccine. About 55% had moderate knowledge of COVID-19, and 48.4% of those vaccinated had completed the vaccine course, with 43.2% receiving two doses and 7.2% only one dose. Motivations for vaccination included accessing services, travel compliance, work allowances, and entry permissions. Vaccine hesitancy was evident in 56% of participants, who were also unlikely to recommend vaccination to others. A positive correlation (r=0.159, p<0.03) was observed between vaccine risk perception and hesitancy. Barriers included fear of long waits, vaccine safety concerns, and insufficient information. Conclusions: The study demonstrated a significant positive correlation between vaccine risk perception and hesitancy among PLWH. It underscores the necessity of tailored vaccination messages addressing the specific concerns of PLWH and the need for increased governmental investment in awareness campaigns to achieve 75% herd immunity.
| Published in | American Journal of Nursing Science (Volume 13, Issue 4) |
| DOI | 10.11648/j.ajns.20241304.11 |
| Page(s) | 64-76 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
COVID-19, COVID-19 Vaccine, Risk Perception, Vaccine Hesitancy, PLWH
Characteristics | Frequency (N=348) | Percentage % |
|---|---|---|
Age | ||
18-30 years | 136 | 39.1 |
31-64 years | 180 | 51.7 |
65 and above | 32 | 9.2 |
Sex | ||
Male | 157 | 45.1 |
Female | 191 | 54.9 |
Marital status | ||
Not married | 107 | 30.7 |
Separated | 79 | 22.7 |
Widowed | 39 | 11.2 |
Married | 123 | 35.3 |
Level of education | ||
I never went to school | 10 | 2.9 |
Primary | 7 | 2.0 |
'O' level | 191 | 54.9 |
'A' level | 71 | 20.4 |
Tertiary Level | 69 | 19.8 |
Employment status | ||
Unemployed | 12 | 3.4 |
Formally employed | 100 | 28.7 |
Informally employed | 135 | 38.8 |
Self-employed | 101 | 29.0 |
Monthly income | ||
Less than $100 | 185 | 53.2 |
$100-$200 | 112 | 32.2 |
Above $200 | 51 | 14.7 |
Characteristic | Frequency (N=348) | Percentage (%) |
|---|---|---|
Below 5 years | 102 | 29.3 |
5-10 years | 75 | 21.6 |
Above 10 years | 171 | 49.1 |
Characteristic | Frequency (n=348) | Percentage (%) |
|---|---|---|
Have you heard about the COVID-19 vaccine? | ||
No | 5 | 1.4 |
Yes | 343 | 98.6 |
How safe do you think the COVID-19 vaccine will be for you? | ||
Not safe | 203 | 58.3 |
Not sure | 117 | 33.6 |
Safe | 28 | 8.0 |
Strongly Agree | Agree | Not Sure | Disagree | Strongly Disagree | |
|---|---|---|---|---|---|
HIV-infected people are at risk of contracting COVID-19? | 72.1% (n=251) | 21.0% (n=73) | 5.5% (n=19) | 0.6% (n=2) | 0.9% (n=3) |
If HIV-infected people receive the COVID-19 vaccine they will be at risk of re-infections | 21.6% (n=75) | 24.7% (n=86) | 45.4% (n=158) | 6.3% (n=22) | 2.0% (n=7) |
I believe an unvaccinated person near me will not give me COVID-19? | 58.9% (n=205) | 29.0% (n=101) | 8.3% (n=29) | 1.7% (n=6) | 2.0% (n=7) |
I am worried COVID-19 is severe in HIV-infected people? | 63.5% (n=221) | 21.8% (n=76) | 8.9% (n=31 | 4.9% (n=17) | 0.9% (n=3) |
Last dose | Frequency (n=192 | Percentage % |
|---|---|---|
First dose | 14 | 7.2 |
Second Dose | 83 | 43.2 |
Third Dose | 93 | 48.4 |
Missing | 3 | 1.2 |
Reason | Frequency (N=348) | Percentage (%) |
|---|---|---|
Difficulty travelling to receive the vaccine | 20 | 5.7 |
Cost of travel to receive the vaccine | 15 | 4.3 |
I would feel unsafe going to receive the vaccine due to the risk of catching the coronavirus (COVID-19) | 61 | 17.5 |
Worries about accessibility at the vaccination centre | 37 | 10.6 |
Difficulty finding help for caring responsibilities while I am getting vaccinated | 55 | 15.8 |
Possible long wait at the vaccination centre | 63 | 18.1 |
Difficult to take time off work | 58 | 16.7 |
I am not expecting any difficulties | 37 | 10.6 |
Missing | 2 | .6 |
Total Risk Perception | Vaccine Hesitancy Score | ||
|---|---|---|---|
Total Risk Perception | Pearson Correlation | 1 | .159** |
Sig. (2-tailed) | .003 | ||
N | 348 | 348 | |
Vaccine Hesitancy Score | Pearson Correlation | .159** | 1 |
Sig. (2-tailed) | .003 | ||
N | 348 | 348 | |
Model | R | R Square | Adjusted R Square | Std. Error of the Estimate |
|---|---|---|---|---|
1 | .159a | .025 | .023 | 1.423 |
Model | Unstandardized Coefficients | Standardized Coefficients | T | Sig. | 95.0% Confidence Interval for B | |||
|---|---|---|---|---|---|---|---|---|
B | Std. Error | Beta | Lower Bound | Upper Bound | ||||
1 | (Constant) | 7.574 | .259 | 29.252 | .000 | 7.064 | 8.083 | |
Total Risk Perception | .107 | .036 | .159 | 3.001 | .003 | .037 | .177 | |
Value | df | Asymp. Sig. (2-sided) | |
|---|---|---|---|
Pearson Chi-Square | 1.286a | 2 | .526 |
Likelihood Ratio | 2.184 | 2 | .336 |
Linear-by-Linear Association | .001 | 1 | .979 |
N of Valid Cases | 348 |
Value | Df | Asymp. Sig. (2-sided) | |
|---|---|---|---|
Pearson Chi-Square | 21.018a | 4 | .000 |
Likelihood Ratio | 16.779 | 4 | .002 |
Linear-by-Linear Association | 4.846 | 1 | .028 |
N of Valid Cases | 348 |
| [1] |
World Health Organisation. Coronavirus disease 2019 pandemic. Available at:
https://www.who.int/emergencies/diseases/novel-coronavirus-2019 [accessed on 28 February, 2022]. |
| [2] | Murewanhema G, Musuka G, Denhere K, Chingombe I, Mapingure MP, Dzinamarira T. The Landscape of COVID-19 Vaccination in Zimbabwe: A Narrative Review and Analysis of the Strengths, Weaknesses, Opportunities and Threats of the Programme. Vaccines (Basel). 2022 Feb |
| [3] | Mazingaizo S. Zimbabwe may consider Mandatory COVID-19 Vaccinations. Sunday Times. 2021. |
| [4] | Xiao, Y., & Torok, M. E. (2020). Taking the right measures to control COVID-19. The Lancet Infectious Diseases, 20(5), 523-524. |
| [5] | MacDonald, N. E. (2015). Vaccine hesitancy: Definition, scope and determinants. Vaccine, 33(34), 4161-4164. |
| [6] | Bogart, L. M., Ojikutu, B. O., Tyagi, K., Klein, D. J., Mutchler, M. G., Dong, L. & Kellman, S. (2021). COVID-19 related medical mistrust, health impacts, and potential vaccine hesitancy among Black Americans living with HIV. Journal of acquired immune deficiency syndromes (1999), 86(2), 200. |
| [7] | Paek, H. J., & Hove, T. (2017). Risk perceptions and risk characteristics. In Oxford research. |
| [8] | Sigel, K., Swartz, T., Golden, E., Paranjpe, I., Somani, S., Richter, F., ... & Glicksberg, B. S. (2020). Coronavirus 2019 and people living with human immunodeficiency virus: outcomes for hospitalized patients in New York City. Clinical infectious diseases, 71(11), 2933-2938. |
| [9] | Guan, W. J., Ni, Z. Y., Hu, Y., Liang, W. H., Ou, C. Q., He, J. X., ... & Zhong, N. S. (2020). Clinical characteristics of coronavirus disease 2019 in China. New England journal of medicine, 382(18), 1708-1720. |
| [10] | Gerretsen, P., Kim, J., Quilty, L., Wells, S., Brown, E. E., Agic, B, & Graff-Guerrero, A. (2021). Vaccine Hesitancy Is a Barrier to Achieving Equitable Herd Immunity Among Racial Minorities. Frontiers in medicine, 8. |
| [11] | Ogolodom, M. P., Mbaba, A. N., Alazigha, N., Erondu, O. F., Egbe, N. O., Golden, I., ... & Eke, C. M. (2020). Knowledge, attitudes and fears of healthcare workers towards the Coronavirus disease (COVID-19) pandemic in South-South, Nigeria. Health Science Journal, 1-10. |
| [12] | Prabhu, S., Poongulali, S., & Kumarasamy, N. (2020). Impact of COVID-19 on people living with HIV: a review. Journal of virus eradication, 6(4), 100019. |
| [13] | Abu, E. K., Oloruntoba, R., Osuagwu, U. L., Bhattarai, D., Miner, C. A., Goson, P. C., ... & Agho, K. E. (2021). Risk perception of COVID-19 among sub-Sahara Africans: a web-based comparative survey of local and diaspora residents. BMC public health, 21(1), 1-13. |
| [14] |
UNAIDS. COVID-19 vaccines and HIV.
https://www.Unaids.Org/en/resources/documents/2021/covid19-vaccines-and-hiv |
| [15] | Apuke, O. D., & Asude Tunca, E. (2021). Modelling the Factors That Predict the Intention to Take COVID-19 Vaccine in Nigeria. Journal of Asian and African Studies, 00219096211069642. |
| [16] | Patwary MM, Disha AS, Bardhan M, Haque MZ, Kabir MP, Billah SM, Hossain MR, Alam MA, Browning MHEM, Shuvo FK, Piracha A, Zhao B, Swed S, Shah J, Shoib S. Knowledge, Attitudes, and Practices Toward Coronavirus and Associated Anxiety Symptoms Among University Students: A Cross-Sectional Study During the Early Stages of the COVID-19 Pandemic in Bangladesh. Front Psychiatry. 2022 Apr 1; 13: 856202. |
| [17] | Cabello A, Zamarro B, Nistal S, Victor V, Hernández J, Prieto-Pérez L, Carrillo I, Álvarez B, Fernández-Roblas R, Hernández-Segurado M, Becares J, Benito JM, Rallón N, Téllez R, Castaño ÁL, Herrero A, Górgolas M. COVID-19 in people living with HIV: A multicenter case-series study. Int J Infect Dis. 2021 Jan; 102: 310-315. |
| [18] | Butler, R. (2016). Vaccine Hesitancy: what it means and what we need to know in order to tackle it. J. Vaccine, 34, 1643-1649. |
| [19] | Liang, M., Luo, N., Chen, M., Chen, C., Singh, S., Singh, S., & Tan, S. (2021). Prevalence and mortality due to COVID-19 in HIV co-infected population: a systematic review and meta-analysis. Infectious diseases and therapy, 10(3), 1267-1285. |
| [20] | Drain PK, Garrett N. SARS-CoV-2 pandemic expanding in sub-Saharan Africa: Considerations for COVID-19 in people living with HIV. EClinical Medicine. 2020 Apr 22; 22: 100342. |
| [21] | Siegrist, M., & Árvai, J. (2020). Risk perception: Reflections on 40 years of research. Risk Analysis, 40(S1), 2191-2206. |
| [22] | Ministry of Health and Child Care of Zimbabwe (2021). |
| [23] | Eve Dubé, Caroline Laberge, Maryse Guay, Paul Bramadat, Réal Roy & Julie A. Bettinger (2013) Vaccine hesitancy, Human Vaccines & Immunotherapeutics, 9: 8, 1763-1773, |
| [24] | Chen, H., Li, X., Gao, J., Liu, X., Mao, Y., Wang, R., & Dai, J. (2021). Health Belief Model Perspective on the Control of COVID-19 Vaccine Hesitancy and the Promotion of Vaccination in China: Web-Based Cross-sectional Study. Journal of Medical Internet Research, 23(9), e29329. |
| [25] | Chigevenga, R. (2021). Commentary on the Zimbabwean People’s Response towards the Anticipated COVID-19 Vaccine. Journal ISSN, 2766, 2276. |
| [26] | Ekstrand, M. L., Heylen, E., Gandhi, M., Steward, W. T., Pereira, M., & Srinivasan, K. (2021). COVID-19 Vaccine Hesitancy Among PLWH in South India: Implications for Vaccination Campaigns. Journal of acquired immune deficiency syndromes (1999), 88(5), 421. |
| [27] | Kaida, A., Brotto, L. A., Murray, M., Côté, H. C., Albert, A. Y., Nicholson, V., ... & Ogilvie, G. S. (2022). Intention to receive a COVID-19 vaccine by HIV status among a population-based sample of women and gender-diverse individuals in British Columbia, Canada. AIDS and Behavior, 1-14. |
| [28] | Wu J, Xu D, Li Q, Tarimo CS, Wang M, Gu J, Wei W, Zhang X, Huang Y, Ma M, Zhao L, Shen Z, Miao Y. The association between lifestyle and COVID-19 vaccine hesitancy in China: A large-scale cross-sectional survey. J Affect Disord. 2022 Sep 15; 313: 92-99. |
| [29] | Huang, X., Yu, M., Fu, G., Lan, G., Li, L., Yang, J., ... & Xu, J. (2021). Willingness to receive COVID-19 vaccination among people living with HIV and AIDS in China: a nationwide cross-sectional online survey. JMIR public health and surveillance, 7(10), e31125. |
| [30] | Govere-Hwenje, S., Jarolimova, J., Yan, J., Khumalo, A., Zondi, G., Ngcobo, M., ... & Bassett, I. V. (2022). Willingness to accept COVID-19 vaccination among people living with HIV in a high HIV prevalence community. Research Square, rs-3. |
| [31] | Mundagowa, P. T., Tozivepi, S. N., Chiyaka, E. T., Mukora-Mutseyekwa, F., & Makurumidze, R. (2022). Assessment of COVID-19 vaccine hesitancy among Zimbabweans: A rapid national survey.PloS one, 17(4), e0266724. |
| [32] | Schmid P, Rauber D, Betsch C, Lidolt G, Denker M-L. Barriers of Influenza Vaccination Intention and Behavior – A Systematic Review of Influenza Vaccine Hesitancy, 2005–2016. PLoS One. 2017; 12(1): e0170550. |
| [33] | Shmueli, L. (2021). Predicting intention to receive COVID-19 vaccine among the general population using the health belief model and the theory of planned behaviour model. BMC Public Health, 21(1), 1-13. |
| [34] | Hossain, M. B., Alam, M., Islam, M., Sultan, S., Faysal, M., Rima, S., ... & Mamun, A. A. (2021). Health belief model, theory of planned behaviour, or psychological antecedents: what predicts COVID-19 vaccine hesitancy better among the Bangladeshi adults?. Frontiers in Public Health, 1172. |
| [35] | Vallée, A., Fourn, E., Majerholc, C., Touche, P., & Zucman, D. (2021). COVID-19 vaccine hesitancy among French people living with HIV. Vaccines, 9(4), 302. |
| [36] | Lin Y, Hu Z, Zhao Q, Alias H, Danaee M, Wong LP (2020) Understanding COVID-19 vaccine demand and hesitancy: A nationwide online survey in China. PLoS Negl Trop Dis 14(12): e0008961. |
| [37] | Chimbetete, C., Shamu, T., Roelens, M., Bote, S., Mudzviti, T., & Keiser, O. (2020). Mortality trends and causes of death among HIV positive patients at Newlands Clinic in Harare, Zimbabwe. PloS one, 15(8), e0237904. |
| [38] | Qi, L., Yang, L., Ge, J., Yu, L., & Li, X. (2021). COVID-19 Vaccination Behavior of People Living with HIV: The Mediating Role of Perceived Risk and Vaccination Intention. Vaccines, 9(11), 1288. |
| [39] | Mufunda, E., Albin, B., & Hjelm, K. (2012). Differences in health and illness beliefs in Zimbabwean men and women with diabetes. The open nursing journal, 6, 117. |
| [40] | Hole G, (2017), Research Skills One, Correlation interpretation, accesed at |
| [41] | Perehudoff, K., Demchenko, I., Alexandrov, N. V., Brutsaert, D., Ackon, A., Durán, C. E., ... & Babar, Z. U. D. (2020). Essential medicines in universal health coverage: a scoping review of public health law interventions and how they are measured in five middle-income countries. International journal of environmental research and public health, 17(24), 9524. |
APA Style
Fungirayi, M., Rukweza, J., Mhlanga, M. (2024). COVID-19 Vaccine Risk Perception and Associated Vaccine Hesitancy Among HIV-Infected People at Parirenyatwa Centre of Excellence. American Journal of Nursing Science, 13(4), 64-76. https://doi.org/10.11648/j.ajns.20241304.11
ACS Style
Fungirayi, M.; Rukweza, J.; Mhlanga, M. COVID-19 Vaccine Risk Perception and Associated Vaccine Hesitancy Among HIV-Infected People at Parirenyatwa Centre of Excellence. Am. J. Nurs. Sci. 2024, 13(4), 64-76. doi: 10.11648/j.ajns.20241304.11
AMA Style
Fungirayi M, Rukweza J, Mhlanga M. COVID-19 Vaccine Risk Perception and Associated Vaccine Hesitancy Among HIV-Infected People at Parirenyatwa Centre of Excellence. Am J Nurs Sci. 2024;13(4):64-76. doi: 10.11648/j.ajns.20241304.11
@article{10.11648/j.ajns.20241304.11,
author = {Moreblessing Fungirayi and Judith Rukweza and Maxwell Mhlanga},
title = {COVID-19 Vaccine Risk Perception and Associated Vaccine Hesitancy Among HIV-Infected People at Parirenyatwa Centre of Excellence
},
journal = {American Journal of Nursing Science},
volume = {13},
number = {4},
pages = {64-76},
doi = {10.11648/j.ajns.20241304.11},
url = {https://doi.org/10.11648/j.ajns.20241304.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajns.20241304.11},
abstract = {Background: The impact of COVID-19 on people living with HIV (PLWH) is particularly concerning due to their existing health vulnerabilities. The low uptake of the COVID-19 vaccine and the failure to achieve herd immunity highlight the need to address vaccine hesitancy, especially in developing countries battling multiple infectious diseases. Objective: This study aimed to determine the relationship between COVID-19 vaccine risk perception and vaccine hesitancy among PLWH. Materials and Methods: An analytical cross-sectional design was used, involving 348 participants from Parirenyatwa Centre of Excellence, recruited via systematic random sampling. Data collection, following ethical approval, was conducted using a self-administered questionnaire. The data were categorized into structure, process, and outcome, and analyzed with SPSS version 22. Results: The study found that 79.9% of PLWH perceived a risk in taking the COVID-19 vaccine. About 55% had moderate knowledge of COVID-19, and 48.4% of those vaccinated had completed the vaccine course, with 43.2% receiving two doses and 7.2% only one dose. Motivations for vaccination included accessing services, travel compliance, work allowances, and entry permissions. Vaccine hesitancy was evident in 56% of participants, who were also unlikely to recommend vaccination to others. A positive correlation (r=0.159, pConclusions: The study demonstrated a significant positive correlation between vaccine risk perception and hesitancy among PLWH. It underscores the necessity of tailored vaccination messages addressing the specific concerns of PLWH and the need for increased governmental investment in awareness campaigns to achieve 75% herd immunity.
},
year = {2024}
}
TY - JOUR T1 - COVID-19 Vaccine Risk Perception and Associated Vaccine Hesitancy Among HIV-Infected People at Parirenyatwa Centre of Excellence AU - Moreblessing Fungirayi AU - Judith Rukweza AU - Maxwell Mhlanga Y1 - 2024/07/23 PY - 2024 N1 - https://doi.org/10.11648/j.ajns.20241304.11 DO - 10.11648/j.ajns.20241304.11 T2 - American Journal of Nursing Science JF - American Journal of Nursing Science JO - American Journal of Nursing Science SP - 64 EP - 76 PB - Science Publishing Group SN - 2328-5753 UR - https://doi.org/10.11648/j.ajns.20241304.11 AB - Background: The impact of COVID-19 on people living with HIV (PLWH) is particularly concerning due to their existing health vulnerabilities. The low uptake of the COVID-19 vaccine and the failure to achieve herd immunity highlight the need to address vaccine hesitancy, especially in developing countries battling multiple infectious diseases. Objective: This study aimed to determine the relationship between COVID-19 vaccine risk perception and vaccine hesitancy among PLWH. Materials and Methods: An analytical cross-sectional design was used, involving 348 participants from Parirenyatwa Centre of Excellence, recruited via systematic random sampling. Data collection, following ethical approval, was conducted using a self-administered questionnaire. The data were categorized into structure, process, and outcome, and analyzed with SPSS version 22. Results: The study found that 79.9% of PLWH perceived a risk in taking the COVID-19 vaccine. About 55% had moderate knowledge of COVID-19, and 48.4% of those vaccinated had completed the vaccine course, with 43.2% receiving two doses and 7.2% only one dose. Motivations for vaccination included accessing services, travel compliance, work allowances, and entry permissions. Vaccine hesitancy was evident in 56% of participants, who were also unlikely to recommend vaccination to others. A positive correlation (r=0.159, pConclusions: The study demonstrated a significant positive correlation between vaccine risk perception and hesitancy among PLWH. It underscores the necessity of tailored vaccination messages addressing the specific concerns of PLWH and the need for increased governmental investment in awareness campaigns to achieve 75% herd immunity. VL - 13 IS - 4 ER -
Department of Nursing Science, University of Zimbabwe, Harare, Zimbabwe
Department of Nursing Science, University of Zimbabwe, Harare, Zimbabwe
Centre of Gender Equity, University of Global Health Equity, Kigali, Rwanda
Information