Background: According to the National Asthma Prevalence Study (NAPS), around seven million people in Bangladesh suffer from asthma. While inhaled medications are key to asthma treatment, incorrect inhaler techniques remain a global issue. This study aimed to assess healthcare providers' knowledge of metered-dose inhaler techniques in a tertiary hospital. Aim of the study: The aim of the study was to evaluate the knowledge and proficiency of healthcare providers in performing nine-steps of the metered-dose inhaler technique in a tertiary-level hospital. Methods: This cross-sectional observational study in the Department of Internal Medicine at Bangabandhu Sheikh Mujib Medical University (BSMMU) Hospital, Dhaka, from July to December 2015, involved 108 healthcare providers. Ethical approval and informed consent were obtained. Data were collected via interviews and observations, and analyzed using SPSS version 17.0 with Chi-square tests, considering p < 0.05 as significant. Results: In a study of 108 healthcare providers, 42.2% were in their fourth decade of life, with a mean age of 30.8 years. Of the respondents, 74.1% were doctors, while 25.9% were nurses. All respondents counseled on inhaler use, and 72.2% recommended inhaler medications. Over 70% removed the cap and shook the inhaler vigorously, with 96.3% breathing out slowly and completely. Doctors outperformed nurses in most steps, with significant differences except for breathing out slowly and completely (p = 0.228). Conclusion: Healthcare providers, particularly nurses, lack proficiency in the final steps of the metered-dose inhaler technique, with doctors generally outperforming nurses in all steps.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Asthma is a major cause of chronic morbidity and mortality worldwide, and its prevalence is increasing, especially among children.
[1]
Scheffer AL. Global strategy for asthma management and prevention. Bethesda. 2002; 3659: 20-9.
[1]
Despite recent advances in the understanding of asthma, its pathophysiology, and the availability of effective treatments, the disease continues to be a major cause of morbidity, leading to a significant economic burden on individuals and societies.
[2]
Ellis ME, Friend JA. How well do asthma clinic patients understand their asthma?. British journal of diseases of the chest. 1985 Jan 1; 79: 43-8.
[2]
Poor asthma control has been linked to several common and important issues, including underdiagnosis and inadequate treatment, poor patient understanding of the disease and its treatment,
[2]
Ellis ME, Friend JA. How well do asthma clinic patients understand their asthma?. British journal of diseases of the chest. 1985 Jan 1; 79: 43-8.
[3]
Bousquet J. A physician’s view of health economics in asthma.
[2, 3]
non-compliance,
[4]
Lim SH, Goh DY, Tan AY, Lee BW. Parents' perceptions towards their child's use of inhaled medications for asthma therapy. Journal of paediatrics and child health. 1996 Aug; 32(4): 306-9.
[5]
Nadi E, Zeraati F, BEYG MA. Evaluation the Rate of Correct Use of a Metered Dose Inhaler in Patients with Obstructive Lung Diseases in Ekbatan Hospital of Hamadan.
[6]
Self TH, Rumbak MJ, Kelso TM. Correct use of metered-dose inhalers and spacer devices. Postgraduate medicine. 1992 Sep 1; 92(3): 95-106.
[4-6]
and incorrect use of inhaler devices.
[5]
Nadi E, Zeraati F, BEYG MA. Evaluation the Rate of Correct Use of a Metered Dose Inhaler in Patients with Obstructive Lung Diseases in Ekbatan Hospital of Hamadan.
[6]
Self TH, Rumbak MJ, Kelso TM. Correct use of metered-dose inhalers and spacer devices. Postgraduate medicine. 1992 Sep 1; 92(3): 95-106.
[5, 6]
Inhaled medications are the cornerstone of asthma treatment.
[7]
Cockcroft DW. Practical issues in asthma management: correct use of inhalation devices. Annals of allergy. 1993 Aug; 71(2): 83-4.
[7]
However, poor patient inhaler technique has been identified as a common and persistent problem worldwide.
[8]
De Blaquiere P, Christensen DB, Carter WB, Martin TR. Use and misuse of metered-dose inhalers by patients with chronic lung disease. Am Rev Respir Dis. 1989; 140(4): 910-6.
[9]
Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. British Journal of General Practice. 1990 Dec 1; 40(341): 505-6.
[10]
Thompson CJ, Irvine MT, Grathwohl CK, Roth MB. Misuse of metered-dose inhalers in hospitalized patients. Chest. 1994 Mar 1; 105(3): 715-7.
[11]
Horsley MG, Bailie GR. Risk factors for inadequate use of pressurized aerosol inhalers. Journal of clinical pharmacy and therapeutics. 1988 Apr; 13(2): 139-43.
[12]
Crompton GK. Problems patients have using pressurized aerosol inhalers. European journal of respiratory diseases. Supplement. 1982 Jan 1; 119: 101-4.
[8-12]
Up to 90% of adult patients have been reported to have inadequate inhaler technique, with higher rates of errors in children and older patients.
[7]
Cockcroft DW. Practical issues in asthma management: correct use of inhalation devices. Annals of allergy. 1993 Aug; 71(2): 83-4.
[8]
De Blaquiere P, Christensen DB, Carter WB, Martin TR. Use and misuse of metered-dose inhalers by patients with chronic lung disease. Am Rev Respir Dis. 1989; 140(4): 910-6.
[9]
Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. British Journal of General Practice. 1990 Dec 1; 40(341): 505-6.
[10]
Thompson CJ, Irvine MT, Grathwohl CK, Roth MB. Misuse of metered-dose inhalers in hospitalized patients. Chest. 1994 Mar 1; 105(3): 715-7.
[7-10]
Poor inhaler technique reduces drug delivery to the airways, decreasing the efficiency of the inhaled medication.
[6]
Self TH, Rumbak MJ, Kelso TM. Correct use of metered-dose inhalers and spacer devices. Postgraduate medicine. 1992 Sep 1; 92(3): 95-106.
[6]
The high prevalence of incorrect inhaler technique among patients has been attributed to several factors.
[11]
Horsley MG, Bailie GR. Risk factors for inadequate use of pressurized aerosol inhalers. Journal of clinical pharmacy and therapeutics. 1988 Apr; 13(2): 139-43.
[12]
Crompton GK. Problems patients have using pressurized aerosol inhalers. European journal of respiratory diseases. Supplement. 1982 Jan 1; 119: 101-4.
[11, 12]
Most healthcare providers do not spend sufficient time educating patients on the correct use of inhalers.
[13]
Mickle TR, Self TH, Farr GE, Bess DT, Tsiu SJ, Caldwell FL. Evaluation of pharmacists' practice in patient education when dispensing a metered-dose inhaler.
[14]
Jones JS, Holstege CP, Riekse R, White L, Bergquist T. Metered-dose inhalers: do emergency health care providers know what to teach?. Annals of emergency medicine. 1995 Sep 1; 26(3): 308-11.
[15]
Kelling JS, Strohl KP, Smith RL, Altose MD. Physician knowledge in the use of canister nebulizers. Chest. 1983 Apr 1; 83(4): 612-4.
[16]
O'Bey KA, Jim LK, Gee JP, Cowen ME, Quigley AE. An education program that improves the psychomotor skills needed for metaproterenol inhaler use. Drug Intelligence & Clinical Pharmacy. 1982 Dec; 16(12): 945-8.
[17]
Khan AA, Hassan MR, Hossain MA, Mahmud AM, Bennoor KS, Ahmad MM, Habib GM. Trends of asthma in Bangladesh: findings of the National asthma prevalence study 1999 and 2010. Respirology. 2020; 15: 33.
[18]
Barman RC, Islam MM, Saha R, Alam T, Ali SY, Ali MY. Improper inhalation technique-a barrier to good asthma control. Faridpur Medical College Journal. 2011; 6(2): 104-6.
[13-18]
Another issue is the absence of routine evaluations of patients' inhaler technique, which are necessary to ensure proper use.
[12]
Crompton GK. Problems patients have using pressurized aerosol inhalers. European journal of respiratory diseases. Supplement. 1982 Jan 1; 119: 101-4.
[13]
Mickle TR, Self TH, Farr GE, Bess DT, Tsiu SJ, Caldwell FL. Evaluation of pharmacists' practice in patient education when dispensing a metered-dose inhaler.
[12, 13]
More importantly, studies show that many providers themselves have poor inhaler technique,
[14]
Jones JS, Holstege CP, Riekse R, White L, Bergquist T. Metered-dose inhalers: do emergency health care providers know what to teach?. Annals of emergency medicine. 1995 Sep 1; 26(3): 308-11.
[15]
Kelling JS, Strohl KP, Smith RL, Altose MD. Physician knowledge in the use of canister nebulizers. Chest. 1983 Apr 1; 83(4): 612-4.
[14, 15]
which can lead them to give incorrect instructions to patients.
[14]
Jones JS, Holstege CP, Riekse R, White L, Bergquist T. Metered-dose inhalers: do emergency health care providers know what to teach?. Annals of emergency medicine. 1995 Sep 1; 26(3): 308-11.
[14]
The correct use of inhalers has been shown to be influenced by patients' characteristics, such as their age and their understanding of asthma and its treatment.
[16]
O'Bey KA, Jim LK, Gee JP, Cowen ME, Quigley AE. An education program that improves the psychomotor skills needed for metaproterenol inhaler use. Drug Intelligence & Clinical Pharmacy. 1982 Dec; 16(12): 945-8.
[16]
As a result, the severity of the problem may vary among different populations.
Formal training and demonstration of the correct use of inhalers have been shown to improve the inhaler skills of both patients and healthcare providers
[16]
O'Bey KA, Jim LK, Gee JP, Cowen ME, Quigley AE. An education program that improves the psychomotor skills needed for metaproterenol inhaler use. Drug Intelligence & Clinical Pharmacy. 1982 Dec; 16(12): 945-8.
[5]
Nadi E, Zeraati F, BEYG MA. Evaluation the Rate of Correct Use of a Metered Dose Inhaler in Patients with Obstructive Lung Diseases in Ekbatan Hospital of Hamadan.
[16, 5]
. Local baseline information is, therefore, essential for each country to develop its own asthma care services and educational programs tailored to their specific problems and needs
[1]
Scheffer AL. Global strategy for asthma management and prevention. Bethesda. 2002; 3659: 20-9.
[1]
. The present study aims to collect information on the metered-dose inhaler technique suggested by service providers to asthma patients in our country.
2. Objective
The aim of the study was to evaluate the knowledge and proficiency of healthcare providers in performing the metered-dose inhaler technique in a tertiary-level hospital.
Methodology & Materials
This cross-sectional observational study was conducted in the Department of Internal Medicine, Bangabandhu Sheikh Mujib Medical University (BSMMU) Hospital, Dhaka, from July 2015 to December 2015. A total of 108 healthcare providers (doctors and nurses) who met the inclusion and exclusion criteria were purposively selected for the study.
Inclusion Criteria:
1) Doctors and nurses of any age and either sex working at BSMMU Hospital.
2) Healthcare providers involved in prescribing or demonstrating metered-dose inhaler (MDI) techniques to asthma patients.
Exclusion Criteria:
Healthcare providers unwilling to participate.
Informed consent was obtained from all participants, ensuring voluntary participation, confidentiality, and the right to withdraw at any time. Ethical approval was obtained from the Ethical Review Committee of Bangabandhu Sheikh Mujib Medical University, Dhaka, following the Helsinki Declaration. Data were collected through structured interviews and observations, assessing participants’ skills in performing the nine-step metered-dose inhaler technique using a checklist. Demographic information and performance data were recorded for analysis. Data were cleaned, coded, and analyzed using SPSS version 17.0, with descriptive statistics summarizing the data and the Chi-square (χ²) test employed to compare variables. A p-value < 0.05 was considered statistically significant.
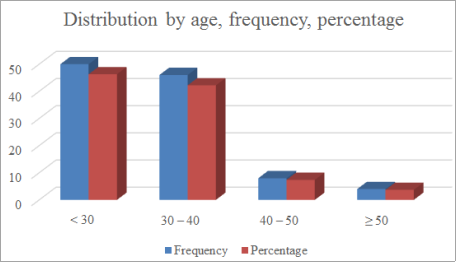
Figure 1. Distribution of Healthcare Providers by Age (n = 108).
Figure 1 shows the age distribution of the 108 healthcare providers involved in the study. Of the respondents, 46 (42.2%) were in their 4th decade of life, followed by 31.5% in their 3rd decade, 14% in their 2nd decade, and 7.4% in their 5th decade. The mean age of the respondents was 30.8 ± 6.3 years, with the youngest being 22 years and the oldest being 51 years. All respondents were urban residents.
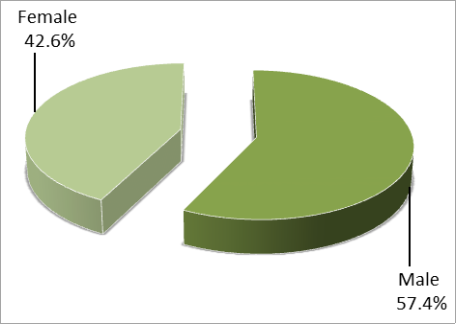
Figure 2. Distribution of respondents by sex (n=108).
Table 1. Distribution of Healthcare Providers by Professional Identity (n = 108).
Professional identity
Frequency
Percentage
Doctor
80
74.1
Nurses
28
25.9
Table 1 presents the distribution of healthcare providers by their professional identity. Of the total respondents, 80 (74.1%) were doctors, while the remaining 28 (25.9%) were nurses.
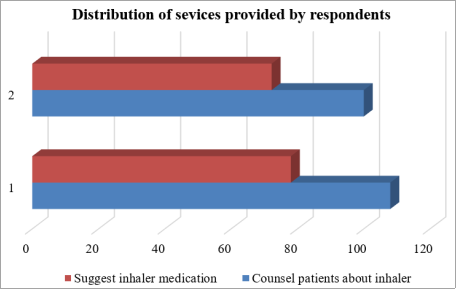
Figure 3 illustrates the types of services provided by the respondents. All respondents reported counseling asthma patients on inhaler use and demonstrating proper inhaler techniques. Additionally, 72.2% of the respondents recommended inhaler medications to asthma patients.
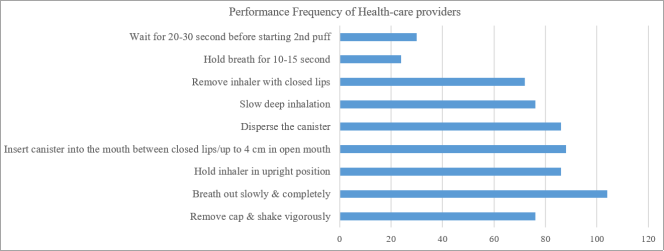
Figure 4. Adherence to the 9-Step Metered-Dose Inhaler Technique.
Respondents were asked to demonstrate their performance skills in using the nine-step metered-dose inhaler technique, which was observed by the investigator. Over 70% of the respondents removed the cap and shook the container vigorously before use. The majority (96.3%) breathed out slowly and completely, and nearly 80% held the inhaler in an upright position. More than 80% inserted the canister into the mouth between closed lips or up to 4 cm away from an open mouth. About 80% dispersed the canister, but only 70% inhaled the medication with slow, deep inhalation. However, adherence to the 8th and 9th steps—holding the breath for 10-15 seconds and waiting 20-30 seconds before starting a second puff—was disappointingly low.
Table 2. Comparison of Performance Skills Between Doctors and Nurses (n = 108).
Performance skills
Group
P-value
Doctors (n = 80)
Nurses (n = 28)
Remove cap & shake vigorously
62(77.5)
14(50.0)
0.006
Breath out slowly & completely
76(95.0)
28(100.0)
0.228
Hold inhaler in upright position
76(95.0)
10(35.7)
<0.001
Insert canister into the mouth between closed lips/up to 4 cm in open mouth
74(92.5)
14(50.0)
<0.001
Disperse the canister
76(95.0)
10(35.7)
<0.001
Slow deep inhalation
68(85.0)
8(28.6)
<0.001
Remove inhaler with closed lips
62(77.5)
10(35.7)
<0.001
Hold breath for 10-15 second
22(27.5)
2(7.1)
0.026
Wait for 20-30 second before starting 2nd puff
26(32.5)
4(14.3)
0.046
Figures in the parentheses indicate corresponding %;
*Chi-squared Test (χ²) was done to analyzed the data
Table 2 presents the comparison of performance skills in the nine-step metered-dose inhaler technique between doctors and nurses. Doctors outperformed nurses in all steps with statistically significant differences (p < 0.05), except for the 2nd step—breathing out slowly and completely—where performance was comparable between the groups (p = 0.228). Notably, 77.5% of doctors and 50% of nurses removed the cap and shook the inhaler vigorously. While 95% of doctors held the inhaler upright, only 35.7% of nurses did the same. Similarly, 92.5% of doctors inserted the inhaler correctly compared to 50% of nurses. Adherence to steps such as slow deep inhalation (85% vs. 28.6%), holding the breath for 10-15 seconds (27.5% vs. 7.1%), and waiting 20-30 seconds before starting a second puff (32.5% vs. 14.3%) was notably higher among doctors than nurses.
4. Discussion
The present study revealed that over two-thirds of the doctors and nurses were skilled in performing the first seven steps of the nine-step metered-dose inhaler technique. However, the skills for the 8th and 9th steps, such as holding the breath for 10-15 seconds and waiting for 20-30 seconds before starting the second puff, were disappointingly low. More than 70% of the respondents removed the cap and shook the container vigorously before use. They then breathed out slowly and completely and held the inhaler in an upright position. The majority inserted the canister into their mouth between closed lips or up to 4 cm in an open mouth and dispersed the canister. However, inhaling the drug with slow, deep inhalation was somewhat low. When comparing the skills of doctors and nurses in inhaler technique, it was evident that, in every step, doctors performed significantly better than nurses (p < 0.05), except in the 2nd step (breathing out slowly and completely), where there was no significant difference between the two groups (p = 0.228).
Inhaled medications form the cornerstone of asthma treatment. However, incorrect inhaler technique has been identified as a common and persistent problem in many studies worldwide.
[19]
Baddar SA, Al-Rawas OA, Al-Riyami KA, Worthing EA, Hanssens YI, Taqi AM, Al-Riyami BM. Metered-dose inhaler technique among healthcare providers practising in Oman. SQU Journal for Scientific Research-Medical Sciences. 2001 Apr; 3(1): 39.
[19]
Up to 90% of adult patients have been reported to have inadequate inhaler technique, with higher rates of errors in children and elderly patients.
[20]
Allen SC, Prior A. What determines whether an elderly patient can use a metered dose inhaler correctly?. British journal of diseases of the chest. 1986 Jan 1; 80: 45-9.
[20]
Poor inhaler technique reduces drug delivery to the airways, decreasing the efficiency of the inhaled drug. Most healthcare providers do not spend sufficient time educating patients on the correct use of inhalers. Another problem is the lack of regular periodic assessment of patients’ inhaler technique, which is essential to ensure proper use.
[20]
Allen SC, Prior A. What determines whether an elderly patient can use a metered dose inhaler correctly?. British journal of diseases of the chest. 1986 Jan 1; 80: 45-9.
[20]
More importantly, studies show that most providers themselves do not have technical knowledge of inhaler techniques, as was evident in 20-30% of cases in our study. If we consider that all nine steps need to be performed correctly to make the inhaler technique effective, the majority of our service providers are not competent enough to educate their patients on how to use inhalers properly. Around 70-80% of doctors and nurses were unable to perform the last two steps (holding the breath for 10-15 seconds and waiting for 20-30 seconds before starting the second puff) as they should have been performed. Thus, they are most likely providing incorrect instructions to their patients.
[21]
Benjaponpitak S, Kraisarin C, Direkwattanachai C, Sasisakunporn C. Incorrect use of metered dose inhaler by pediatric residents. Journal of the Medical Association of Thailand= Chotmaihet thangphaet. 1996 Feb 1; 79(2): 122-6.
[22]
O'Donnell J, Birkinshaw R, Burke V, Driscoll PA. The ability of A&E personnel to demonstrate inhaler technique. Emergency Medicine Journal. 1997 May 1; 14(3): 163-4.
[21, 22]
In addition, the correct use of inhalers has been shown to be influenced by patients' characteristics, such as age, literacy, and their understanding of asthma and its treatment.
[23]
Williams MV, Baker DW, Honig EG, Lee TM, Nowlan A. Inadequate literacy is a barrier to asthma knowledge and self-care. Chest. 1998 Oct 1; 114(4): 1008-15.
[23]
Therefore, the magnitude of the problem may vary in different populations. Hence, poor inhaler technique among asthma patients will not be completely solved by making service providers competent alone. Simultaneous education of the patients is a must. Formal training and demonstration of the correct use of inhalers have been shown to significantly improve inhaler use skills in both patients and healthcare providers. Local baseline information about inhaler technique is, therefore, essential for each country to develop its own asthma care services and educational programs targeted at their specific problems and needs.
Nurses are an important part of the healthcare team and, in many countries, are often the first point of contact and sometimes the closest interaction for people with asthma. They play a vital role in educating patients. Thus, nurses are expected to educate and train patients when inhaler devices are prescribed. However, in our country, doctors' chambers are the first-place asthma patients visit. Therefore, the management knowledge of both doctors and nurses can positively or negatively impact treatment outcomes. Studies in other parts of the world have reported a very low level of knowledge about asthma and inhaler technique among nurses and concluded that there is a need for sufficient knowledge to effectively teach and participate in asthma care.
[24]
Lustosa GM, Britto MC, Bezerra PG. Acute asthma management in children: knowledge of the topic among health professionals at teaching hospitals in the city of Recife, Brazil. Jornal Brasileiro de Pneumologia. 2011; 37: 584-8.
[24]
Poor asthma knowledge and inhaler techniques among patients have been associated with poor asthma control and health outcomes.
[25]
Cabana MD, Slish KK, Evans D, Mellins RB, Brown RW, Lin X, et al. Impact of Physician Asthma Care Education on patient outcomes. Health Educ Behav. 2014; 41(5): 509-17.
[25]
The quality of asthma care depends on the healthcare provider’s knowledge, attitude, experience, and expertise in educating patients on inhaler technique. We hope that the findings derived from this study will have implications for improving the existing asthma care situation in our country.
5. Limitations of the Study
This study had some limitations:
1) Conducted at a single center, limiting diversity and affecting external validity.
2) The sample size was small, may limit generalizability.
3) Relied on self-reporting, introducing potential bias.
6. Conclusion
Based on the findings of the study, it can be concluded that healthcare providers (doctors and nurses) lack sufficient proficiency in performing all nine steps of the metered-dose inhaler technique. Consequently, they may not be adequately equipped to instruct asthma patients on proper inhaler use. While most doctors and nurses demonstrated proficiency in the first seven steps, adherence to the last two steps—holding the breath for 10-15 seconds and waiting for 20-30 seconds before starting a second puff—was notably low. However, doctors outperformed nurses in demonstrating their skills in using the metered-dose inhaler technique.
Abbreviations
BSMMU
Bangabandhu Sheikh Mujib Medical University
MDI
Metered-Dose Inhaler
NAPS
National Asthma Prevalence Study
SPSS
Statistical Package for the Social Sciences
χ²
Chi-square Test
SD
Standard Deviation (if Mentioned Elsewhere in the Results or Figures)
Author Contributions
Mohammad Abdul Motalib is the sole author. The author read and approved the final manuscript.
Conflicts of Interest
The author declares no conflicts of interest.
References
[1]
Scheffer AL. Global strategy for asthma management and prevention. Bethesda. 2002; 3659: 20-9.
[2]
Ellis ME, Friend JA. How well do asthma clinic patients understand their asthma?. British journal of diseases of the chest. 1985 Jan 1; 79: 43-8.
[3]
Bousquet J. A physician’s view of health economics in asthma.
[4]
Lim SH, Goh DY, Tan AY, Lee BW. Parents' perceptions towards their child's use of inhaled medications for asthma therapy. Journal of paediatrics and child health. 1996 Aug; 32(4): 306-9.
[5]
Nadi E, Zeraati F, BEYG MA. Evaluation the Rate of Correct Use of a Metered Dose Inhaler in Patients with Obstructive Lung Diseases in Ekbatan Hospital of Hamadan.
[6]
Self TH, Rumbak MJ, Kelso TM. Correct use of metered-dose inhalers and spacer devices. Postgraduate medicine. 1992 Sep 1; 92(3): 95-106.
[7]
Cockcroft DW. Practical issues in asthma management: correct use of inhalation devices. Annals of allergy. 1993 Aug; 71(2): 83-4.
[8]
De Blaquiere P, Christensen DB, Carter WB, Martin TR. Use and misuse of metered-dose inhalers by patients with chronic lung disease. Am Rev Respir Dis. 1989; 140(4): 910-6.
[9]
Hilton S. An audit of inhaler technique among asthma patients of 34 general practitioners. British Journal of General Practice. 1990 Dec 1; 40(341): 505-6.
[10]
Thompson CJ, Irvine MT, Grathwohl CK, Roth MB. Misuse of metered-dose inhalers in hospitalized patients. Chest. 1994 Mar 1; 105(3): 715-7.
[11]
Horsley MG, Bailie GR. Risk factors for inadequate use of pressurized aerosol inhalers. Journal of clinical pharmacy and therapeutics. 1988 Apr; 13(2): 139-43.
[12]
Crompton GK. Problems patients have using pressurized aerosol inhalers. European journal of respiratory diseases. Supplement. 1982 Jan 1; 119: 101-4.
[13]
Mickle TR, Self TH, Farr GE, Bess DT, Tsiu SJ, Caldwell FL. Evaluation of pharmacists' practice in patient education when dispensing a metered-dose inhaler.
[14]
Jones JS, Holstege CP, Riekse R, White L, Bergquist T. Metered-dose inhalers: do emergency health care providers know what to teach?. Annals of emergency medicine. 1995 Sep 1; 26(3): 308-11.
[15]
Kelling JS, Strohl KP, Smith RL, Altose MD. Physician knowledge in the use of canister nebulizers. Chest. 1983 Apr 1; 83(4): 612-4.
[16]
O'Bey KA, Jim LK, Gee JP, Cowen ME, Quigley AE. An education program that improves the psychomotor skills needed for metaproterenol inhaler use. Drug Intelligence & Clinical Pharmacy. 1982 Dec; 16(12): 945-8.
[17]
Khan AA, Hassan MR, Hossain MA, Mahmud AM, Bennoor KS, Ahmad MM, Habib GM. Trends of asthma in Bangladesh: findings of the National asthma prevalence study 1999 and 2010. Respirology. 2020; 15: 33.
[18]
Barman RC, Islam MM, Saha R, Alam T, Ali SY, Ali MY. Improper inhalation technique-a barrier to good asthma control. Faridpur Medical College Journal. 2011; 6(2): 104-6.
[19]
Baddar SA, Al-Rawas OA, Al-Riyami KA, Worthing EA, Hanssens YI, Taqi AM, Al-Riyami BM. Metered-dose inhaler technique among healthcare providers practising in Oman. SQU Journal for Scientific Research-Medical Sciences. 2001 Apr; 3(1): 39.
[20]
Allen SC, Prior A. What determines whether an elderly patient can use a metered dose inhaler correctly?. British journal of diseases of the chest. 1986 Jan 1; 80: 45-9.
[21]
Benjaponpitak S, Kraisarin C, Direkwattanachai C, Sasisakunporn C. Incorrect use of metered dose inhaler by pediatric residents. Journal of the Medical Association of Thailand= Chotmaihet thangphaet. 1996 Feb 1; 79(2): 122-6.
[22]
O'Donnell J, Birkinshaw R, Burke V, Driscoll PA. The ability of A&E personnel to demonstrate inhaler technique. Emergency Medicine Journal. 1997 May 1; 14(3): 163-4.
[23]
Williams MV, Baker DW, Honig EG, Lee TM, Nowlan A. Inadequate literacy is a barrier to asthma knowledge and self-care. Chest. 1998 Oct 1; 114(4): 1008-15.
[24]
Lustosa GM, Britto MC, Bezerra PG. Acute asthma management in children: knowledge of the topic among health professionals at teaching hospitals in the city of Recife, Brazil. Jornal Brasileiro de Pneumologia. 2011; 37: 584-8.
[25]
Cabana MD, Slish KK, Evans D, Mellins RB, Brown RW, Lin X, et al. Impact of Physician Asthma Care Education on patient outcomes. Health Educ Behav. 2014; 41(5): 509-17.
Motalib, M. A. (2025). A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital. American Journal of Clinical and Experimental Medicine, 13(1), 8-13. https://doi.org/10.11648/j.ajcem.20251301.12
Motalib, M. A. A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital. Am. J. Clin. Exp. Med.2025, 13(1), 8-13. doi: 10.11648/j.ajcem.20251301.12
Motalib MA. A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital. Am J Clin Exp Med. 2025;13(1):8-13. doi: 10.11648/j.ajcem.20251301.12
@article{10.11648/j.ajcem.20251301.12,
author = {Mohammad Abdul Motalib},
title = {A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital},
journal = {American Journal of Clinical and Experimental Medicine},
volume = {13},
number = {1},
pages = {8-13},
doi = {10.11648/j.ajcem.20251301.12},
url = {https://doi.org/10.11648/j.ajcem.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajcem.20251301.12},
abstract = {Background: According to the National Asthma Prevalence Study (NAPS), around seven million people in Bangladesh suffer from asthma. While inhaled medications are key to asthma treatment, incorrect inhaler techniques remain a global issue. This study aimed to assess healthcare providers' knowledge of metered-dose inhaler techniques in a tertiary hospital. Aim of the study: The aim of the study was to evaluate the knowledge and proficiency of healthcare providers in performing nine-steps of the metered-dose inhaler technique in a tertiary-level hospital. Methods: This cross-sectional observational study in the Department of Internal Medicine at Bangabandhu Sheikh Mujib Medical University (BSMMU) Hospital, Dhaka, from July to December 2015, involved 108 healthcare providers. Ethical approval and informed consent were obtained. Data were collected via interviews and observations, and analyzed using SPSS version 17.0 with Chi-square tests, considering p Results: In a study of 108 healthcare providers, 42.2% were in their fourth decade of life, with a mean age of 30.8 years. Of the respondents, 74.1% were doctors, while 25.9% were nurses. All respondents counseled on inhaler use, and 72.2% recommended inhaler medications. Over 70% removed the cap and shook the inhaler vigorously, with 96.3% breathing out slowly and completely. Doctors outperformed nurses in most steps, with significant differences except for breathing out slowly and completely (p = 0.228). Conclusion: Healthcare providers, particularly nurses, lack proficiency in the final steps of the metered-dose inhaler technique, with doctors generally outperforming nurses in all steps.},
year = {2025}
}
TY - JOUR
T1 - A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital
AU - Mohammad Abdul Motalib
Y1 - 2025/02/11
PY - 2025
N1 - https://doi.org/10.11648/j.ajcem.20251301.12
DO - 10.11648/j.ajcem.20251301.12
T2 - American Journal of Clinical and Experimental Medicine
JF - American Journal of Clinical and Experimental Medicine
JO - American Journal of Clinical and Experimental Medicine
SP - 8
EP - 13
PB - Science Publishing Group
SN - 2330-8133
UR - https://doi.org/10.11648/j.ajcem.20251301.12
AB - Background: According to the National Asthma Prevalence Study (NAPS), around seven million people in Bangladesh suffer from asthma. While inhaled medications are key to asthma treatment, incorrect inhaler techniques remain a global issue. This study aimed to assess healthcare providers' knowledge of metered-dose inhaler techniques in a tertiary hospital. Aim of the study: The aim of the study was to evaluate the knowledge and proficiency of healthcare providers in performing nine-steps of the metered-dose inhaler technique in a tertiary-level hospital. Methods: This cross-sectional observational study in the Department of Internal Medicine at Bangabandhu Sheikh Mujib Medical University (BSMMU) Hospital, Dhaka, from July to December 2015, involved 108 healthcare providers. Ethical approval and informed consent were obtained. Data were collected via interviews and observations, and analyzed using SPSS version 17.0 with Chi-square tests, considering p Results: In a study of 108 healthcare providers, 42.2% were in their fourth decade of life, with a mean age of 30.8 years. Of the respondents, 74.1% were doctors, while 25.9% were nurses. All respondents counseled on inhaler use, and 72.2% recommended inhaler medications. Over 70% removed the cap and shook the inhaler vigorously, with 96.3% breathing out slowly and completely. Doctors outperformed nurses in most steps, with significant differences except for breathing out slowly and completely (p = 0.228). Conclusion: Healthcare providers, particularly nurses, lack proficiency in the final steps of the metered-dose inhaler technique, with doctors generally outperforming nurses in all steps.
VL - 13
IS - 1
ER -
Motalib, M. A. (2025). A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital. American Journal of Clinical and Experimental Medicine, 13(1), 8-13. https://doi.org/10.11648/j.ajcem.20251301.12
Motalib, M. A. A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital. Am. J. Clin. Exp. Med.2025, 13(1), 8-13. doi: 10.11648/j.ajcem.20251301.12
Motalib MA. A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital. Am J Clin Exp Med. 2025;13(1):8-13. doi: 10.11648/j.ajcem.20251301.12
@article{10.11648/j.ajcem.20251301.12,
author = {Mohammad Abdul Motalib},
title = {A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital},
journal = {American Journal of Clinical and Experimental Medicine},
volume = {13},
number = {1},
pages = {8-13},
doi = {10.11648/j.ajcem.20251301.12},
url = {https://doi.org/10.11648/j.ajcem.20251301.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajcem.20251301.12},
abstract = {Background: According to the National Asthma Prevalence Study (NAPS), around seven million people in Bangladesh suffer from asthma. While inhaled medications are key to asthma treatment, incorrect inhaler techniques remain a global issue. This study aimed to assess healthcare providers' knowledge of metered-dose inhaler techniques in a tertiary hospital. Aim of the study: The aim of the study was to evaluate the knowledge and proficiency of healthcare providers in performing nine-steps of the metered-dose inhaler technique in a tertiary-level hospital. Methods: This cross-sectional observational study in the Department of Internal Medicine at Bangabandhu Sheikh Mujib Medical University (BSMMU) Hospital, Dhaka, from July to December 2015, involved 108 healthcare providers. Ethical approval and informed consent were obtained. Data were collected via interviews and observations, and analyzed using SPSS version 17.0 with Chi-square tests, considering p Results: In a study of 108 healthcare providers, 42.2% were in their fourth decade of life, with a mean age of 30.8 years. Of the respondents, 74.1% were doctors, while 25.9% were nurses. All respondents counseled on inhaler use, and 72.2% recommended inhaler medications. Over 70% removed the cap and shook the inhaler vigorously, with 96.3% breathing out slowly and completely. Doctors outperformed nurses in most steps, with significant differences except for breathing out slowly and completely (p = 0.228). Conclusion: Healthcare providers, particularly nurses, lack proficiency in the final steps of the metered-dose inhaler technique, with doctors generally outperforming nurses in all steps.},
year = {2025}
}
TY - JOUR
T1 - A Study of Knowledge About Metered-Dose Inhaler Technique Among Health Care Providers in a Tertiary-Level Hospital
AU - Mohammad Abdul Motalib
Y1 - 2025/02/11
PY - 2025
N1 - https://doi.org/10.11648/j.ajcem.20251301.12
DO - 10.11648/j.ajcem.20251301.12
T2 - American Journal of Clinical and Experimental Medicine
JF - American Journal of Clinical and Experimental Medicine
JO - American Journal of Clinical and Experimental Medicine
SP - 8
EP - 13
PB - Science Publishing Group
SN - 2330-8133
UR - https://doi.org/10.11648/j.ajcem.20251301.12
AB - Background: According to the National Asthma Prevalence Study (NAPS), around seven million people in Bangladesh suffer from asthma. While inhaled medications are key to asthma treatment, incorrect inhaler techniques remain a global issue. This study aimed to assess healthcare providers' knowledge of metered-dose inhaler techniques in a tertiary hospital. Aim of the study: The aim of the study was to evaluate the knowledge and proficiency of healthcare providers in performing nine-steps of the metered-dose inhaler technique in a tertiary-level hospital. Methods: This cross-sectional observational study in the Department of Internal Medicine at Bangabandhu Sheikh Mujib Medical University (BSMMU) Hospital, Dhaka, from July to December 2015, involved 108 healthcare providers. Ethical approval and informed consent were obtained. Data were collected via interviews and observations, and analyzed using SPSS version 17.0 with Chi-square tests, considering p Results: In a study of 108 healthcare providers, 42.2% were in their fourth decade of life, with a mean age of 30.8 years. Of the respondents, 74.1% were doctors, while 25.9% were nurses. All respondents counseled on inhaler use, and 72.2% recommended inhaler medications. Over 70% removed the cap and shook the inhaler vigorously, with 96.3% breathing out slowly and completely. Doctors outperformed nurses in most steps, with significant differences except for breathing out slowly and completely (p = 0.228). Conclusion: Healthcare providers, particularly nurses, lack proficiency in the final steps of the metered-dose inhaler technique, with doctors generally outperforming nurses in all steps.
VL - 13
IS - 1
ER -