Abstract
This case report and clinical overview examines rare but persistent post-vaccination cardiac complications associated with mRNA COVID-19 vaccine platforms, which exhibit a higher incidence rate ratio of post-vaccination arrhythmia compared to traditional or vector-based designs. Currently, there is a distinct clinical gap regarding the management of long-term, vaccine-associated arrhythmias that remain refractory over multiple years. We present the case of a 77-year-old male with no prior cardiac history who developed persistent ventricular bigeminy and frequent premature ventricular contractions (PVCs) following a primary mRNA vaccination series (Moderna). The arrhythmia continuously recurred through subsequent mRNA booster doses (Moderna and Pfizer) over a three-year period. Extensive clinical evaluations, including echocardiography and myocardial perfusion stress testing, ruled out structural heart disease, ischemia, or metabolic abnormalities. Because the overall arrhythmia burden was measured at a low 6%, below the standard 15% clinical treatment threshold, no antiarrhythmic medications or invasive interventions were initiated. However, following a self-initiated platform switch to a single dose of the protein-based recombinant adjuvanted vaccine (Novavax), the patient’s multi-year arrhythmia resolved completely within days, and normal sinus rhythm has been continuously documented for over a year. Putative mechanisms for mRNA-induced myocardial electrical instability include prolonged intracellular processing of encoded spike proteins within host cardiomyocytes, lipid nanoparticle-mediated systemic inflammation, and autoimmune molecular mimicry—cascades that are entirely avoided by recombinant protein vaccines. Ultimately, this case highlights a profound temporal association between long-term ventricular arrhythmia and mRNA vaccines, followed by rapid, sustained resolution upon switching platforms. Clinicians should consider enhanced, long-term arrhythmia monitoring for select patients presenting with post-mRNA palpitations, and therapeutic platform-switching to non-mRNA configurations warrants immediate further investigation as a safe, highly viable mitigation strategy for persistent vaccine-associated cardiac symptoms.
Keywords
COVID-19 Vaccine, mRNA, Arrhythmia, Novavax®, Case Report, Cardiac Rhythm, Vaccine Safety, Bigeminy
1. Introduction
1.1. Background
Messenger Ribonucleic Acid (RNA) COVID-19 vaccines have demonstrated significant efficacy in reducing severe COVID-19 outcomes, but rare cardiovascular complications - including myocarditis and atrial/ventricular arrhythmias - have been reported globally.
| [1] | Lee S, Kim J, Lee S, et al. Atrial Fibrillation After mRNA-1273 SARS-CoV-2 Vaccination: Case Report and Literature Review. Risk Manag Healthcare Policy. 2023; 16: 363-368.
https://doi.org/10.2147/RMHP.S403789 |
[1]
Large-scale studies, such as Kim and Lee’s 2023 analysis of 3.3 million individuals, indicate a 48% increased risk of acute arrhythmia following mRNA vaccination, highlighting the need for mechanistic and therapeutic investigations.
| [1] | Lee S, Kim J, Lee S, et al. Atrial Fibrillation After mRNA-1273 SARS-CoV-2 Vaccination: Case Report and Literature Review. Risk Manag Healthcare Policy. 2023; 16: 363-368.
https://doi.org/10.2147/RMHP.S403789 |
[1]
1.2. Case History
A 77-year-old male retired podiatrist with no prior cardiac history presented to his family physician 4/27/21 for routine physical exam. He had history of well controlled hypertension, hyperlipidemia and impaired glucose tolerance. His medications included Olmesartan 5mg, Rosuvastatin 5mg and Metformin 500 mg. He was a non-smoker and consumed minimal alcohol. At his 4/27/21 office visit, he was feeling well without any chest pain or shortness of breath. He complained of occasional rare palpitations. It was noted by auscultation that he was in Bigeminy. He had recently completed his initial two COVID-19 Moderna® vaccinations on 2/3/21 and 3/4/21.
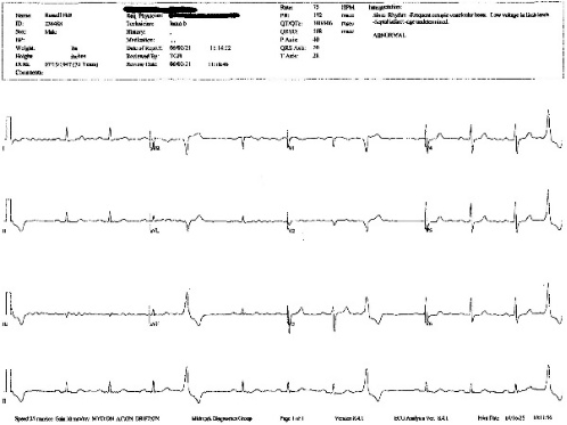
At his initial Cardiology referral visit on 6/02/21, the electrocardiogram (ECG) recorded multiple premature ventricular beats (PVCs).
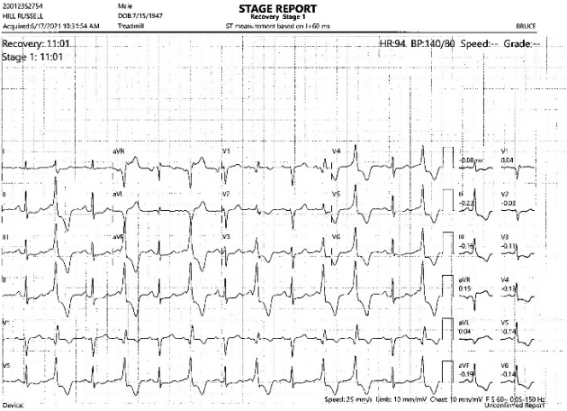
A stress treadmill from 6/17/21 revealed a return to bigeminy.
After April 2021, the patient experienced continuous alternation between sinus rhythm, irregular premature ventricular beat patterns, bigeminy, and trigeminy for over 3 years, well documented by hundreds of single-lead ECGs. Throughout the entire period of documented arrhythmias, the patient remained mostly asymptomatic except occasional palpitations. Interestingly, he noted that activities elevating his basal heart rate often temporarily alleviated the arrhythmias, but they invariably returned.
1.3. Diagnostic Workup and Clinical Course
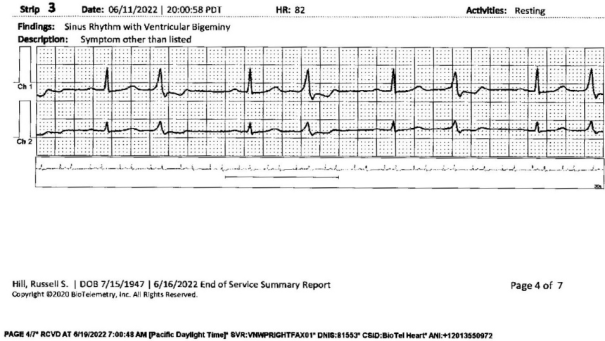
The patient underwent comprehensive cardiac evaluation including myocardial perfusion stress test, which was negative for ischemia. Holter monitoring revealed ventricular bigeminy and 6% PVC burden.
Figure 3. Holter Monitor.
Cardiac Echocardiogram revealed normal Ejection Fraction of 55%, mild-moderate Left Ventricular Hypertrophy and decreased LV compliance. Multiple visits back to the specialist did not result in any prescribed interventions. At the final cardiology visit (November 4, 2024) prior to the Novavax® vaccination, the patient was told that because his arrhythmia measured at only 6% PVC burden (normal: 2%, treatment threshold: 15%), he was below the treatment threshold. Remarkably, after receiving a single dose of the Novavax® (Nuvaxovid) COVID-19 vaccine on November 8, 2024, the arrhythmias resolved within a few days and have not recurred for over a year.
2. Timeline and Clinical Interventions
2.1. Vaccination Timeline and Onset of Arrhythmia
February 3, 2021: Received initial 100 μg dose of Moderna® COVID-19 vaccine.
March 4, 2021: Received second Moderna® dose (100 μg).
April 27, 2021: Routine physical auscultation revealed bigeminal cardiac rhythm, confirmed by Cardiologist on ECG of 6/02/21:
Subsequent Vaccinations: Switched to Pfizer® (50 μg) with doses on December 1, 2021; September 7, 2022; and April 25, 2023.
2.2. Intervention and Outcome
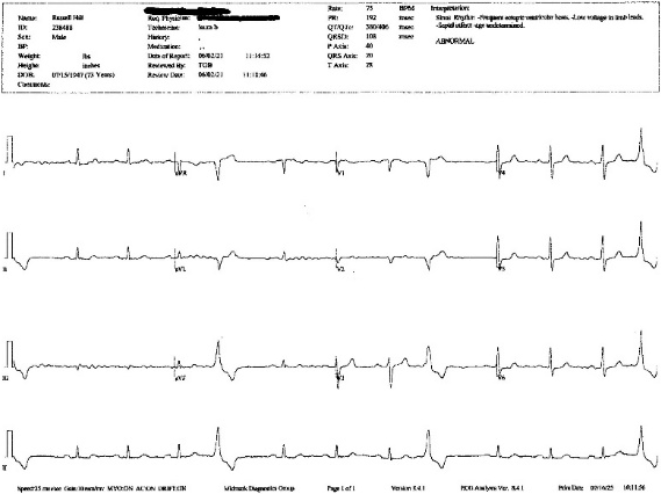
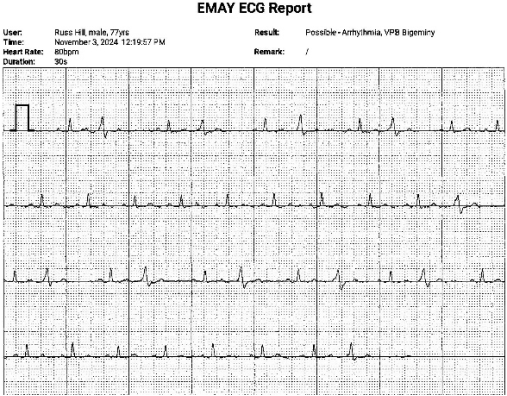
November 3, 2024: ECG five days prior to receiving Novavax® vaccine.
November 8, 2024: Patient received a single 0.5cc (50 μg) dose of Novavax®.
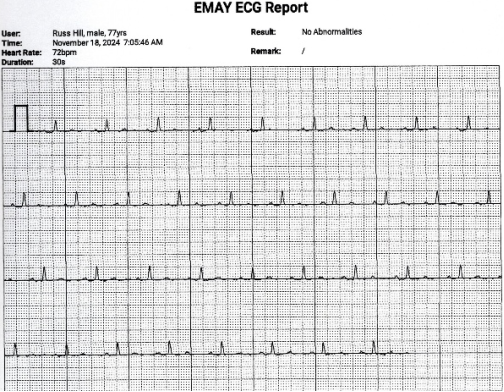
November 18, 2024: Rhythm strip confirmed return to sinus rhythm.
Follow-Up: No arrhythmias have been detected in the eight months since Novavax® administration. Sinus rhythm has been confirmed in over one hundred rhythm strips and confirmed by two independent physicians, most recently on April 23, 2025.
3. Clinical Summary
3.1. Diagnostic Assessment
All investigations ruled out ischemic, structural, and metabolic etiologies. Arrhythmia burden remained below treatment threshold (15%).
3.2. Therapeutic Intervention
No antiarrhythmic medications prescribed. Self-initiated switch to Novavax® vaccine.
3.3. Follow-up and Outcomes
Sustained sinus rhythm confirmed at 2 days after Novavax® vaccine and has not recurred at the time of this writing one-year post-Novavax® as evidenced by:
1) KardiaMobileTM 6L ECG
2) Physician auscultation
3) Pulse waveform analysis
4) Daily ECG rhythm strips run on EMayTM Portable ECG Monitor
4. Discussion
4.1. Discussion Mechanistic Insights
Proposed pathways include molecular mimicry between SARS-CoV-2 spike proteins and cardiac self-antigens, systemic inflammatory responses driven by Interleukin-18 (IL-18) mediated natural killer T-cell (NK/T-cell) activation, and endothelial dysfunction secondary to spike protein interactions.
| [2] | Mevorach D, Anis E, Cedar N, et al. Shedding light on mechanisms of myocarditis with COVID-19 mRNA vaccines. N Engl J Med. 2022; 386(9): 854-857.
https://doi.org/10.1056/NEJMe2116493 |
[2]
Myocardial fibrosis, detectable via late gadolinium enhancement on cardiac magnetic resonance imaging (MRI), further underscores the potential for chronic injury.
| [3] | Farah Y, Najeeb H, Naeem U, et al. Adverse events following COVID-19 mRNA vaccines: A systematic review of cardiovascular complication, thrombosis, and thrombocytopenia. Immunity, Inflammation and Disease. 2023; 11(3): e807.
https://doi.org/10.1002/iid3.807 |
[3]
To understand these mechanisms deeper, Bozkurt outlines how systemic immune-mediated responses—specifically hyper-reactivity of T-cells and molecular mimicry—drive myocardial inflammation following mRNA delivery.
At the cellular level, Schreckenberg et al. demonstrated that the intracellular processing of the spike protein within human AC16 cardiomyocytes can directly alter myocyte function and protein expression profile, providing a direct cardiotoxic pathway distinct from generalized systemic inflammation.
| [13] | Schreckenberg R, Woitasky N, Schlüter KD. Intracellular processing of the spike protein expressed by mRNA-based COVID-19 vaccines in AC16 cardiomyocytes. Front Cardiovasc Med. 2024; 11: 1339345.
https://doi.org/10.3389/fcvm.2024.1339345 |
[13]
While adenovirus-vector and mRNA vaccines both correlate with arrhythmias, mRNA-specific lipid nanoparticles and nucleoside modifications may uniquely prolong spike protein expression, exacerbating immune reactivity.
| [4] | Abutaleb MH, Kamel AM, Abdelnabi M, et al. Arrhythmias after COVID-19 vaccination: have we left all stones unturned? J Cardiovasc Dev Dis. 2023; 10(6): 240.
https://doi.org/10.3390/jcdd10060240 |
| [5] | Abutaleb MH, Makeen HA, Meraya AM, et al. Risks of cardiac arrhythmia associated with COVID-19 vaccination: a systematic review and meta-analysis. Vaccines. 2023; 11(1): 112. https://doi.org/10.3390/vaccines11010112 |
[4, 5]
Marin attributes ECG changes and conduction abnormalities to inflammatory damage in myocardial tissue.
| [6] | Martin SS, Aday AW, Almarzooq ZI, et al; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Committee. 2024 Heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024; 149(8): e347-e913.
https://doi.org/10.1161/CIR.0000000000001209 |
[6]
The clinical presentations of these phenomena vary but are well-documented. In a comprehensive European Society of Cardiology (ESC) clinical consensus document, Heidecker et al. detailed the broad spectrum of post-vaccination myocarditis and rhythm disturbances, establishing that while presentation is often acute and benign, subclinical chronic inflammation can persist.
| [9] | Heidecker B, Dagan N, Balicer R, et al. Myocarditis following COVID‐19 vaccine: incidence, presentation, diagnosis, pathophysiology, therapy, and outcomes put into perspective. A clinical consensus document supported by the Heart Failure Association of the European Society of Cardiology (ESC) and the ESC Working Group on Myocardial and Pericardial Diseases. Eur J Heart Fail. 2022; 24(11): 2000–2018.
https://doi.org/10.1002/ejhf.2669 |
[9]
Though rare, severe outcomes have occurred; for instance, Minato et al. reported a fatal autopsy-confirmed case of a young male presenting with sudden lethal arrhythmia post-mRNA vaccination, highlighting that vaccine-induced electrical instability can be profound.
4.2. Clinical Gap
Despite extensive characterization of post-vaccine cardiac sequelae, no mitigation strategies exist for persistent arrhythmias linked to mRNA platforms. Current management focuses on supportive care, with limited evidence guiding therapeutic intervention. Large-scale real-world safety data and clinical trials demonstrate that while the overall absolute risk of severe adverse events remains low, cardiovascular safety signals are consistently detectable across global populations.
| [8] | Chang Y, Lv G, Liu C, Huang E, Luo B. Cardiovascular safety of COVID-19 vaccines in real-world studies: a systematic review and meta-analysis. Expert Rev Vaccines. 2023; 22(1): 25–34. https://doi.org/10.1080/14760584.2023.2150169 |
| [10] | Kaur RJ, Dutta S, Bhardwaj P, et al. Adverse events reported from COVID-19 vaccine trials: a systematic review. Indian J Clin Biochem. 2021; 36(4): 427–439.
https://doi.org/10.1007/s12291-021-00968-z |
[8, 10]
When serious cardiovascular events occur, managing their long-term chronicity poses a severe therapeutic challenge.
| [12] | Padilla‐Flores T, Sampieri A, Vaca L. Incidence and management of the main serious adverse events reported after COVID‐19 vaccination. Pharmacol Res Perspect. 2024; 12(3): e1224. https://doi.org/10.1002/prp2.1224 |
[12]
This report describes a multi-year mRNA vaccine-associated arrhythmia that resolved spontaneously following administration of Novavax®, a protein-based vaccine lacking mRNA components. Cocco et al. emphasized the necessity of exploring alternate vaccine platforms and conducting thorough evaluations of underlying arrhythmogenic substrates in patients who experience post-vaccination palpitations.
| [14] | Cocco N, Leibundgut G, Pelliccia F, et al. Arrhythmias after COVID-19 vaccination: have we left all stones unturned? Int J Mol Sci. 2023; 24(12): 10405.
https://doi.org/10.3390/ijms241210405 |
[14]
The distinct temporal association observed in this patient suggests that non-mRNA platforms may avoid the specific intracellular pathways and lipid nanoparticle-mediated adjuvanticity driving cardiac autoimmunity, offering a potential therapeutic pathway for refractory cases.
This case presents three novel findings:
1) Chronicity: Unusually prolonged (3+ year) arrhythmia temporally associated with mRNA vaccine administration.
2) Platform Dependence: Differential response to mRNA vs. protein vaccine platforms.
3) Reversibility: Complete resolution post-platform switch to Novavax®.
The temporal association suggests possible mRNA-specific mechanisms:
1)
Molecular Mimicry: Spike protein cross-reactivity with myocardial structural proteins.
2) Adjuvant Effects: Lipid nanoparticle-mediated inflammation and cytokine activation.
3) Autonomic Modulation: Downregulation of Angiotensin-Converting Enzyme 2 (ACE2) receptors, leading to local angiotensin-II excess and subsequent arrhythmogenesis.
Regarding the reversibility of the arrhythmias, Novavax® contains a stabilized prefusion spike protein (a recombinant protein) along with a saponin-based Matrix-M adjuvant, completely avoiding the intracellular mRNA translation phase within host cardiomyocytes.
| [13] | Schreckenberg R, Woitasky N, Schlüter KD. Intracellular processing of the spike protein expressed by mRNA-based COVID-19 vaccines in AC16 cardiomyocytes. Front Cardiovasc Med. 2024; 11: 1339345.
https://doi.org/10.3389/fcvm.2024.1339345 |
[13]
Furthermore, protein vaccines like Novavax® may not provoke as rapid or as intense of an intracellular immune reaction as mRNA vaccines, aiding in cardiac tolerability. While speculative, it is possible that the introduction of a purely protein-based platform acted to modulate the persistent immune/inflammatory loop or successfully competitive-bound chronic antibodies, reducing the inflammatory burden on the heart and restoring autonomic homeostasis.
5. Conclusions
This report highlights the need for:
1) Enhanced arrhythmia monitoring post-mRNA vaccination.
2) Platform-switching as a potential mitigation strategy.
3) Mechanistic studies comparing vaccine-related cardiac effects.
4) Greater transparency in vaccine data to alleviate vaccine hesitancy.
This case study comes at an interesting time in COVID vaccine policy. As recently as May 2025 the Food and Drug Administration (FDA) is asking the two makers of mRNA vaccines to expand warning labels about the possible cardiac side effects. Since vaccination is extremely important for many people, including young patients with underlying immune disorder or lung disease, it will be important to understand that Novavax® could be a safer alternative as it pertains to cardiac side effects and potential mitigation for mRNA vaccine related arrhythmias.
While mRNA vaccines offer impactful opportunities for rapid implementation in emergency situations to prevent the most severe outcomes, we must recognize that no vaccine or medication has a perfect treatment or side effects profile. Recognizing and implementing potential mitigation strategies can reduce vaccine hesitancy and improve overall treatment outcomes.
AI Use Disclosure
During the preparation of this work the authors used Perplexity in order to find suitable mRNA arrhythmia reference articles. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the publication.
Abbreviations
ACE2 | Angiotensin-Converting Enzyme 2 |
COVID-19 | Coronavirus Disease 2019 |
ECG | Electrocardiogram |
FDA | Food and Drug Administration |
IL-18 | Interleukin-18 |
LV | Left Ventricular / Left Ventricle |
LVH | Left Ventricular Hypertrophy |
mRNA | Messenger Ribonucleic Acid |
MRI | Magnetic Resonance Imaging |
NK/T-cell | Natural Killer / T-cell |
PVC | Premature Ventricular Contraction (beat) |
SARS-CoV-2 | Severe Acute Respiratory Syndrome Coronavirus 2 |
Author Contributions
Russell Hill: Conceptualization, Methodology, Data curation, Resources, Project administration, Writing – original draft
Jill Panitch: Data curation, Methodology, Resources, Formal Analysis, Investigation, Writing – review & editing
Conflicts of Interest
One of the authors is the patient described. No external funding was received. There are no conflicts of interest with any party.
References
| [1] |
Lee S, Kim J, Lee S, et al. Atrial Fibrillation After mRNA-1273 SARS-CoV-2 Vaccination: Case Report and Literature Review. Risk Manag Healthcare Policy. 2023; 16: 363-368.
https://doi.org/10.2147/RMHP.S403789
|
| [2] |
Mevorach D, Anis E, Cedar N, et al. Shedding light on mechanisms of myocarditis with COVID-19 mRNA vaccines. N Engl J Med. 2022; 386(9): 854-857.
https://doi.org/10.1056/NEJMe2116493
|
| [3] |
Farah Y, Najeeb H, Naeem U, et al. Adverse events following COVID-19 mRNA vaccines: A systematic review of cardiovascular complication, thrombosis, and thrombocytopenia. Immunity, Inflammation and Disease. 2023; 11(3): e807.
https://doi.org/10.1002/iid3.807
|
| [4] |
Abutaleb MH, Kamel AM, Abdelnabi M, et al. Arrhythmias after COVID-19 vaccination: have we left all stones unturned? J Cardiovasc Dev Dis. 2023; 10(6): 240.
https://doi.org/10.3390/jcdd10060240
|
| [5] |
Abutaleb MH, Makeen HA, Meraya AM, et al. Risks of cardiac arrhythmia associated with COVID-19 vaccination: a systematic review and meta-analysis. Vaccines. 2023; 11(1): 112.
https://doi.org/10.3390/vaccines11010112
|
| [6] |
Martin SS, Aday AW, Almarzooq ZI, et al; American Heart Association Council on Epidemiology and Prevention Statistics Committee and Stroke Statistics Committee. 2024 Heart disease and stroke statistics: a report of US and global data from the American Heart Association. Circulation. 2024; 149(8): e347-e913.
https://doi.org/10.1161/CIR.0000000000001209
|
| [7] |
Bozkurt B. Shedding light on mechanisms of myocarditis with COVID-19 mRNA vaccines. Circulation. 2023; 147(11): 877–880.
https://doi.org/10.1161/CIRCULATIONAHA.123.063396
|
| [8] |
Chang Y, Lv G, Liu C, Huang E, Luo B. Cardiovascular safety of COVID-19 vaccines in real-world studies: a systematic review and meta-analysis. Expert Rev Vaccines. 2023; 22(1): 25–34.
https://doi.org/10.1080/14760584.2023.2150169
|
| [9] |
Heidecker B, Dagan N, Balicer R, et al. Myocarditis following COVID‐19 vaccine: incidence, presentation, diagnosis, pathophysiology, therapy, and outcomes put into perspective. A clinical consensus document supported by the Heart Failure Association of the European Society of Cardiology (ESC) and the ESC Working Group on Myocardial and Pericardial Diseases. Eur J Heart Fail. 2022; 24(11): 2000–2018.
https://doi.org/10.1002/ejhf.2669
|
| [10] |
Kaur RJ, Dutta S, Bhardwaj P, et al. Adverse events reported from COVID-19 vaccine trials: a systematic review. Indian J Clin Biochem. 2021; 36(4): 427–439.
https://doi.org/10.1007/s12291-021-00968-z
|
| [11] |
Minato H, Yoshikawa A, Tsuyama S, et al. Fatal arrythmia in a young man after COVID-19 vaccination: an autopsy report. Medicine (Baltimore). 2024; 103(6): e37196.
https://doi.org/10.1097/MD.0000000000037196
|
| [12] |
Padilla‐Flores T, Sampieri A, Vaca L. Incidence and management of the main serious adverse events reported after COVID‐19 vaccination. Pharmacol Res Perspect. 2024; 12(3): e1224.
https://doi.org/10.1002/prp2.1224
|
| [13] |
Schreckenberg R, Woitasky N, Schlüter KD. Intracellular processing of the spike protein expressed by mRNA-based COVID-19 vaccines in AC16 cardiomyocytes. Front Cardiovasc Med. 2024; 11: 1339345.
https://doi.org/10.3389/fcvm.2024.1339345
|
| [14] |
Cocco N, Leibundgut G, Pelliccia F, et al. Arrhythmias after COVID-19 vaccination: have we left all stones unturned? Int J Mol Sci. 2023; 24(12): 10405.
https://doi.org/10.3390/ijms241210405
|
Cite This Article
-
APA Style
Hill, R., Panitch, J. (2026). Anecdotal Report: Resolution of Purported mRNA
Vaccine-Induced Arrhythmia Following Novavax Administration. American Journal of Biomedical and Life Sciences, 14(4), 53-60. https://doi.org/10.11648/j.ajbls.20261404.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Hill, R.; Panitch, J. Anecdotal Report: Resolution of Purported mRNA
Vaccine-Induced Arrhythmia Following Novavax Administration. Am. J. Biomed. Life Sci. 2026, 14(4), 53-60. doi: 10.11648/j.ajbls.20261404.11
Copy
|
Download
AMA Style
Hill R, Panitch J. Anecdotal Report: Resolution of Purported mRNA
Vaccine-Induced Arrhythmia Following Novavax Administration. Am J Biomed Life Sci. 2026;14(4):53-60. doi: 10.11648/j.ajbls.20261404.11
Copy
|
Download
-
@article{10.11648/j.ajbls.20261404.11,
author = {Russell Hill and Jill Panitch},
title = {Anecdotal Report: Resolution of Purported mRNA
Vaccine-Induced Arrhythmia Following Novavax Administration},
journal = {American Journal of Biomedical and Life Sciences},
volume = {14},
number = {4},
pages = {53-60},
doi = {10.11648/j.ajbls.20261404.11},
url = {https://doi.org/10.11648/j.ajbls.20261404.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajbls.20261404.11},
abstract = {This case report and clinical overview examines rare but persistent post-vaccination cardiac complications associated with mRNA COVID-19 vaccine platforms, which exhibit a higher incidence rate ratio of post-vaccination arrhythmia compared to traditional or vector-based designs. Currently, there is a distinct clinical gap regarding the management of long-term, vaccine-associated arrhythmias that remain refractory over multiple years. We present the case of a 77-year-old male with no prior cardiac history who developed persistent ventricular bigeminy and frequent premature ventricular contractions (PVCs) following a primary mRNA vaccination series (Moderna). The arrhythmia continuously recurred through subsequent mRNA booster doses (Moderna and Pfizer) over a three-year period. Extensive clinical evaluations, including echocardiography and myocardial perfusion stress testing, ruled out structural heart disease, ischemia, or metabolic abnormalities. Because the overall arrhythmia burden was measured at a low 6%, below the standard 15% clinical treatment threshold, no antiarrhythmic medications or invasive interventions were initiated. However, following a self-initiated platform switch to a single dose of the protein-based recombinant adjuvanted vaccine (Novavax), the patient’s multi-year arrhythmia resolved completely within days, and normal sinus rhythm has been continuously documented for over a year. Putative mechanisms for mRNA-induced myocardial electrical instability include prolonged intracellular processing of encoded spike proteins within host cardiomyocytes, lipid nanoparticle-mediated systemic inflammation, and autoimmune molecular mimicry—cascades that are entirely avoided by recombinant protein vaccines. Ultimately, this case highlights a profound temporal association between long-term ventricular arrhythmia and mRNA vaccines, followed by rapid, sustained resolution upon switching platforms. Clinicians should consider enhanced, long-term arrhythmia monitoring for select patients presenting with post-mRNA palpitations, and therapeutic platform-switching to non-mRNA configurations warrants immediate further investigation as a safe, highly viable mitigation strategy for persistent vaccine-associated cardiac symptoms.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Anecdotal Report: Resolution of Purported mRNA
Vaccine-Induced Arrhythmia Following Novavax Administration
AU - Russell Hill
AU - Jill Panitch
Y1 - 2026/07/11
PY - 2026
N1 - https://doi.org/10.11648/j.ajbls.20261404.11
DO - 10.11648/j.ajbls.20261404.11
T2 - American Journal of Biomedical and Life Sciences
JF - American Journal of Biomedical and Life Sciences
JO - American Journal of Biomedical and Life Sciences
SP - 53
EP - 60
PB - Science Publishing Group
SN - 2330-880X
UR - https://doi.org/10.11648/j.ajbls.20261404.11
AB - This case report and clinical overview examines rare but persistent post-vaccination cardiac complications associated with mRNA COVID-19 vaccine platforms, which exhibit a higher incidence rate ratio of post-vaccination arrhythmia compared to traditional or vector-based designs. Currently, there is a distinct clinical gap regarding the management of long-term, vaccine-associated arrhythmias that remain refractory over multiple years. We present the case of a 77-year-old male with no prior cardiac history who developed persistent ventricular bigeminy and frequent premature ventricular contractions (PVCs) following a primary mRNA vaccination series (Moderna). The arrhythmia continuously recurred through subsequent mRNA booster doses (Moderna and Pfizer) over a three-year period. Extensive clinical evaluations, including echocardiography and myocardial perfusion stress testing, ruled out structural heart disease, ischemia, or metabolic abnormalities. Because the overall arrhythmia burden was measured at a low 6%, below the standard 15% clinical treatment threshold, no antiarrhythmic medications or invasive interventions were initiated. However, following a self-initiated platform switch to a single dose of the protein-based recombinant adjuvanted vaccine (Novavax), the patient’s multi-year arrhythmia resolved completely within days, and normal sinus rhythm has been continuously documented for over a year. Putative mechanisms for mRNA-induced myocardial electrical instability include prolonged intracellular processing of encoded spike proteins within host cardiomyocytes, lipid nanoparticle-mediated systemic inflammation, and autoimmune molecular mimicry—cascades that are entirely avoided by recombinant protein vaccines. Ultimately, this case highlights a profound temporal association between long-term ventricular arrhythmia and mRNA vaccines, followed by rapid, sustained resolution upon switching platforms. Clinicians should consider enhanced, long-term arrhythmia monitoring for select patients presenting with post-mRNA palpitations, and therapeutic platform-switching to non-mRNA configurations warrants immediate further investigation as a safe, highly viable mitigation strategy for persistent vaccine-associated cardiac symptoms.
VL - 14
IS - 4
ER -
Copy
|
Download