Abstract
Health security remains a critical concern in global public health, particularly in low- and middle-income countries facing recurrent infectious disease outbreaks. National health security plans provide the policy architecture for translating international commitments into domestic preparedness capacities, yet their operational effectiveness depends on stakeholder awareness, financing, coordination and subnational implementation. This study examines the role of health policy in enhancing health security in Nigeria, using the National Action Plan for Health Security (NAPHS) as a case study. Specifically, it assesses stakeholders’ awareness of NAPHS, perceived relevance of the policy framework, implementation effectiveness, perceived improvements in health security domains, barriers to implementation and recommendations for strengthening Nigeria’s preparedness system. A quantitative cross-sectional survey design supported by documentary policy analysis was adopted. Data were collected from 380 purposively selected stakeholders using a structured questionnaire covering institutional profile, familiarity with NAPHS, perceived relevance, implementation effectiveness, preparedness improvements, funding adequacy, inter-agency coordination, One Health awareness, training exposure, barriers and recommendations. Descriptive statistics, cross-tabulations, chi-square tests of independence and Cramér’s V were used for analysis. NAPHS was widely recognised as relevant (90.3%) and strategically aligned with national and international frameworks (81.1% and 80.8%, respectively). However, only 9.2% rated implementation as very effective, while 60.3% rated it moderately effective. Familiarity was strongly concentrated at the federal level (92.4%) compared with state (44.2%) and community/facility levels (15.8%). The strongest improvements were observed in disease surveillance (69.2%) and laboratory capacity (67.1%), whereas funding mobilisation (15.0%), workforce training (26.0%) and inter-agency coordination (26.8%) were the weakest domains. Inadequate funding (84.7%) and weak coordination (76.1%) were the most frequently reported barriers. While NAPHS provides a strong policy foundation for health security in Nigeria, its operational impact depends on sustainable domestic financing, decentralised implementation, strengthened coordination, workforce development and improved subnational awareness. The study contributes evidence-based recommendations for strengthening national preparedness planning in resource-constrained settings.
|
Published in
|
World Journal of Public Health (Volume 11, Issue 3)
|
|
DOI
|
10.11648/j.wjph.20261103.12
|
|
Page(s)
|
234-248 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Health Security, Health Policy, National Action Plan for Health Security, Health Regulations, Stakeholder Perception
1. Introduction
Health security has become a major concern in global public health because infectious disease outbreaks, zoonotic spillovers, antimicrobial resistance, climate-related emergencies and other public health threats can rapidly disrupt health systems, economies and social stability
. The experiences of Ebola virus disease in West Africa, COVID-19 and recurrent epidemic-prone diseases across sub-Saharan Africa have shown that public health emergencies are not only biomedical events but also governance, policy and security challenges
| [5] | Frieden TR, Damon I, Bell BP, Kenyon T, Nichol S. Ebola 2014: new challenges, new global response and responsibility. N Engl J Med. 2014; 371(13): 1177-1180.
https://doi.org/10.1056/NEJMra1411025 |
| [6] | Moon S, Sridhar D, Pate MA, Jha AK, Clinton C, Delaunay S, et al. Will Ebola change the game? Ten essential reforms before the next pandemic. Lancet. 2015; 386(10009): 2204-2221.
https://doi.org/10.1016/S0140-6736(15)00946-0 |
| [7] | World Bank. People, pathogens and our planet: the economics of One Health. Washington, DC: World Bank; 2012. |
[5-7]
. Therefore, strengthening national preparedness requires coherent health policy, sustainable financing, functional institutions, trained human resources, multisectoral coordination, effective surveillance and strong laboratory systems
| [8] | Kruk ME, Myers M, Varpilah ST, Dahn BT. What is a resilient health system? Lessons from Ebola. Lancet. 2015; 385(9980): 1910-1912. https://doi.org/10.1016/S0140-6736(15)60755-3 |
| [9] | Hanefeld J, Mayhew S, Legido-Quigley H, Martineau F, Karanikolos M, Blanchet K, et al. Towards an understanding of resilience: responding to health systems shocks. BMJ Glob Health. 2018; 3(1): e000688.
https://doi.org/10.1136/bmjgh-2017-000688 |
| [10] | Lal A, Erondu NA, Heymann DL, Gitahi G, Yates R. Fragmented health systems in COVID-19: rectifying the misalignment between global health security and universal health coverage. Lancet. 2021; 397(10268): 61-67.
https://doi.org/10.1016/S0140-6736(20)32207-3 |
[8-10]
. The International Health Regulations (IHR 2005) provide the main global legal framework for strengthening countries’ capacities to prevent, detect, assess, notify and respond to public health risks of international concern
| [11] | World Health Organization. International Health Regulations. Geneva: WHO; 2005. |
[11]
. Under the IHR framework, countries are expected to build core capacities in surveillance, laboratory confirmation, emergency preparedness, risk communication, response coordination and points of entry
| [11] | World Health Organization. International Health Regulations. Geneva: WHO; 2005. |
| [12] | World Health Organization. Joint External Evaluation tool: International Health Regulations. Geneva: WHO; 2016. |
[11, 12]
. However, the effectiveness of IHR implementation depends largely on domestic policy ownership, institutional capacity, political commitment and the ability to translate assessment findings into funded and measurable actions
| [13] | Kandel N, Chungong S, Omaar A, Xing J. Health security capacities in the context of COVID-19 outbreak: an analysis of International Health Regulations annual report data from 182 countries. Lancet. 2020; 395(10229): 1047-1053.
https://doi.org/10.1016/S0140-6736(20)30551-7 |
| [14] | Oppenheim B, Gallivan M, Madhav NK, Brown N, Serhiyenko V, Wolfe ND, et al. Assessing global preparedness for the next pandemic: development and application of an Epidemic Preparedness Index. BMJ Glob Health. 2019; 4(1): e001157.
https://doi.org/10.1136/bmjgh-2018-001157 |
| [15] | Katz R, Dowell SF. Revising the International Health Regulations: call for a 2017 review conference. Lancet Glob Health. 2015; 3(7): e352-e353.
https://doi.org/10.1016/S2214-109X(15)00009-7 |
[13-15]
. The National Action Plan for Health Security (NAPHS) was developed as a country-owned, multi-year, multisectoral and all-hazards planning framework for accelerating the implementation of IHR core capacities
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
[16]
. The NAPHS approach is based on whole-of-government, whole-of-society and One Health principles, recognising that health threats often emerge at the intersection of human, animal and environmental systems
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [17] | Zinsstag J, Schelling E, Waltner-Toews D, Tanner M. From “one medicine” to “one health” and systemic approaches to health and well-being. Prev Vet Med. 2011; 101(3-4): 148-156. https://doi.org/10.1016/j.prevetmed.2011.05.008 |
| [18] | Mackenzie JS, Jeggo M. The One Health approach: why is it so important? Trop Med Infect Dis. 2019; 4(2): 88.
https://doi.org/10.3390/tropicalmed4020088 |
[16-18]
. As a policy instrument, NAPHS helps countries identify health security gaps, prioritise interventions, cost activities, assign implementation responsibilities, mobilise resources and monitor progress
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [19] | Bell JA, Nuzzo JB. Global Health Security Index: advancing collective action and accountability amid global crisis. Washington, DC: Nuclear Threat Initiative; 2021. |
[16, 19]
. Nigeria provides an important case for examining the role of health policy in enhancing health security. As Africa’s most populous country, Nigeria faces a complex risk environment shaped by high population mobility, recurrent infectious disease outbreaks, urbanisation, climate-sensitive disease patterns, porous borders and a federal governance structure that requires coordination across federal, state and local government levels
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
| [21] | Nigeria Centre for Disease Control and Prevention. Nigeria commences its second Joint External Evaluation for the International Health Regulations core capacities. Abuja: NCDC; 2023. |
| [22] | Nkengasong JN, Maiyegun O, Moeti M. Establishing the Africa Centres for Disease Control and Prevention: responding to Africa’s health threats. Lancet Glob Health. 2017; 5(3): e246-e247. https://doi.org/10.1016/S2214-109X(17)30025-6 |
[20-22]
. The country has experienced repeated outbreaks of Lassa fever, cholera, meningitis, yellow fever, mpox and other epidemic-prone diseases, making preparedness and response capacity a continuing national priority
| [21] | Nigeria Centre for Disease Control and Prevention. Nigeria commences its second Joint External Evaluation for the International Health Regulations core capacities. Abuja: NCDC; 2023. |
| [23] | World Health Organization. Joint external evaluation of the International Health Regulations core capacities of Nigeria: mission report, 14-18 August 2023. Geneva: WHO; 2024. |
[21, 23]
. Nigeria’s National Action Plan for Health Security 2018-2022 was developed to address gaps identified through the Joint External Evaluation and related assessments
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
| [24] | World Health Organization Regional Office for Africa. NCDC/WHO map resources for NAPHS in 36 states and Federal Capital Territory. Brazzaville: WHO AFRO; 2019. |
[20, 24]
. The plan integrated existing national workplans and strategic priorities, including disease surveillance, emergency preparedness, antimicrobial resistance, immunisation, risk communication and laboratory strengthening
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
[20]
. The establishment of the Nigeria Centre for Disease Control and Prevention through the NCDC Establishment Act 2018 further strengthened the legal and institutional basis for disease surveillance, outbreak response and public health emergency coordination in Nigeria
| [25] | Federal Republic of Nigeria. Nigeria Centre for Disease Control and Prevention Establishment Act, 2018. Abuja: Federal Republic of Nigeria Official Gazette; 2018. |
[25]
. Despite these policy developments, implementation gaps remain. Nigeria’s health security system continues to face challenges related to inadequate domestic financing, weak inter-agency coordination, uneven state-level implementation, limited workforce capacity, weak data systems and dependence on donor-supported programmes
| [24] | World Health Organization Regional Office for Africa. NCDC/WHO map resources for NAPHS in 36 states and Federal Capital Territory. Brazzaville: WHO AFRO; 2019. |
| [26] | Balajee SA, Pasi OG, Etoundi AGM, Rzeszotarski P, Do TT, Hennessee I, et al. Sustainable model for public health emergency operations centers for global settings. Emerg Infect Dis. 2017; 23(13): S190-S195.
https://doi.org/10.3201/eid2313.170682 |
| [27] | Nkengasong JN, Tessema SK. Africa needs a new public health order to tackle infectious disease threats. Cell. 2020; 183(2): 296-300. https://doi.org/10.1016/j.cell.2020.09.004 |
[24, 26, 27]
. These challenges are important because the existence of a national plan does not automatically guarantee operational preparedness unless the plan is adequately financed, decentralised, implemented and monitored
| [13] | Kandel N, Chungong S, Omaar A, Xing J. Health security capacities in the context of COVID-19 outbreak: an analysis of International Health Regulations annual report data from 182 countries. Lancet. 2020; 395(10229): 1047-1053.
https://doi.org/10.1016/S0140-6736(20)30551-7 |
| [15] | Katz R, Dowell SF. Revising the International Health Regulations: call for a 2017 review conference. Lancet Glob Health. 2015; 3(7): e352-e353.
https://doi.org/10.1016/S2214-109X(15)00009-7 |
| [28] | Resolve to Save Lives. Developing the 2024 National Action Plan for Health Security annual operational plan, Lagos, Nigeria. New York: Resolve to Save Lives; 2024. |
[13, 15, 28]
. Although previous policy documents and technical reports have described the design and objectives of Nigeria’s NAPHS, limited empirical attention has been given to stakeholders’ perceptions of its implementation and contribution to health security preparedness. Understanding stakeholder perceptions is important because policy implementation depends on awareness, institutional ownership, coordination, resource mobilisation and frontline engagement
| [14] | Oppenheim B, Gallivan M, Madhav NK, Brown N, Serhiyenko V, Wolfe ND, et al. Assessing global preparedness for the next pandemic: development and application of an Epidemic Preparedness Index. BMJ Glob Health. 2019; 4(1): e001157.
https://doi.org/10.1136/bmjgh-2018-001157 |
| [29] | Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015; 10: 53.
https://doi.org/10.1186/s13012-015-0242-0 |
[14, 29]
. Stakeholder views can therefore reveal whether NAPHS is functioning as a practical implementation framework or merely as a strategic policy document.
This study examines the role of health policy in enhancing health security in Nigeria, using NAPHS as a case study. Specifically, the study assesses stakeholders’ awareness of NAPHS, perceived relevance of the policy framework, perceived implementation effectiveness, perceived improvements in health security domains, barriers to implementation and recommendations for strengthening Nigeria’s preparedness system. By combining survey evidence with policy analysis, the study contributes to the literature on health security governance, IHR implementation and national preparedness planning in low- and middle-income settings.
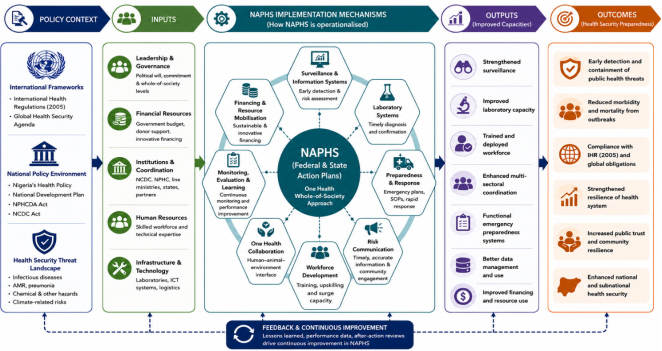
The conceptual logic of the study is that health policy enhances health security when it provides a clear strategic framework, mobilises resources, strengthens implementation mechanisms and produces measurable improvements in preparedness outcomes. In this study, NAPHS is conceptualised as a policy instrument linking global and national health security commitments to practical implementation mechanisms such as financing, surveillance, laboratory capacity, emergency response, workforce training, One Health coordination, risk communication, monitoring and evaluation.
Figure 1. Conceptual framework showing the role of NAPHS in enhancing health security preparedness in Nigeria.
2. Literature Review
2.1. Health Security and Health Policy
Health security refers to the capacity of countries and health systems to prevent, detect, assess, report and respond to public health threats that may endanger populations or spread across borders
| [1] | Gostin LO, Katz R. The International Health Regulations: the governing framework for global health security. Milbank Q. 2016; 94(2): 264-313.
https://doi.org/10.1111/1468-0009.12186 |
| [11] | World Health Organization. International Health Regulations. Geneva: WHO; 2005. |
[1, 11]
. The concept has expanded from a narrow focus on infectious disease control to a broader concern with antimicrobial resistance, zoonotic diseases, climate-related health risks, chemical hazards, emergency preparedness and health-system resilience
. This expansion reflects the growing recognition that public health emergencies can produce social, economic and political consequences beyond the health sector
| [5] | Frieden TR, Damon I, Bell BP, Kenyon T, Nichol S. Ebola 2014: new challenges, new global response and responsibility. N Engl J Med. 2014; 371(13): 1177-1180.
https://doi.org/10.1056/NEJMra1411025 |
| [6] | Moon S, Sridhar D, Pate MA, Jha AK, Clinton C, Delaunay S, et al. Will Ebola change the game? Ten essential reforms before the next pandemic. Lancet. 2015; 386(10009): 2204-2221.
https://doi.org/10.1016/S0140-6736(15)00946-0 |
[5, 6]
. Health policy is central to health security because preparedness requires organised public action. Health policy defines mandates, sets priorities, allocates resources, establishes institutions and creates accountability mechanisms
| [8] | Kruk ME, Myers M, Varpilah ST, Dahn BT. What is a resilient health system? Lessons from Ebola. Lancet. 2015; 385(9980): 1910-1912. https://doi.org/10.1016/S0140-6736(15)60755-3 |
| [13] | Kandel N, Chungong S, Omaar A, Xing J. Health security capacities in the context of COVID-19 outbreak: an analysis of International Health Regulations annual report data from 182 countries. Lancet. 2020; 395(10229): 1047-1053.
https://doi.org/10.1016/S0140-6736(20)30551-7 |
[8, 13]
. Without clear policy direction, health security activities may become fragmented across institutions and sectors. This is particularly important in low- and middle-income countries, where health systems may face limited financing, workforce shortages, infrastructure gaps and weak information systems
| [9] | Hanefeld J, Mayhew S, Legido-Quigley H, Martineau F, Karanikolos M, Blanchet K, et al. Towards an understanding of resilience: responding to health systems shocks. BMJ Glob Health. 2018; 3(1): e000688.
https://doi.org/10.1136/bmjgh-2017-000688 |
| [10] | Lal A, Erondu NA, Heymann DL, Gitahi G, Yates R. Fragmented health systems in COVID-19: rectifying the misalignment between global health security and universal health coverage. Lancet. 2021; 397(10268): 61-67.
https://doi.org/10.1016/S0140-6736(20)32207-3 |
[9, 10]
. Studies on health-system resilience show that countries respond better to health emergencies when routine health systems are strong, adaptive and well coordinated
. Kruk et al. argued that resilient health systems must be able to prepare for, absorb and learn from shocks while maintaining essential services
. Hanefeld et al. similarly emphasised governance, financing, information systems and workforce capacity as important components of resilience
| [9] | Hanefeld J, Mayhew S, Legido-Quigley H, Martineau F, Karanikolos M, Blanchet K, et al. Towards an understanding of resilience: responding to health systems shocks. BMJ Glob Health. 2018; 3(1): e000688.
https://doi.org/10.1136/bmjgh-2017-000688 |
[9]
. These arguments suggest that health security should not be treated as an isolated emergency agenda but as part of broader health-system strengthening.
2.2. International Health Regulations and Global Health Security Governance
The International Health Regulations provide the legal foundation for global health security by requiring countries to develop capacities for surveillance, notification, preparedness, response and risk communication
| [11] | World Health Organization. International Health Regulations. Geneva: WHO; 2005. |
[11]
. The IHR framework recognises that public health threats can spread rapidly through travel, trade, migration and ecological change; therefore, national preparedness contributes to regional and global security
| [11] | World Health Organization. International Health Regulations. Geneva: WHO; 2005. |
| [12] | World Health Organization. Joint External Evaluation tool: International Health Regulations. Geneva: WHO; 2016. |
[11, 12]
. However, the implementation of IHR core capacities has remained uneven across countries. Kandel et al. found wide variation in health security capacities across 182 countries, showing that many countries still had gaps in preparedness and response capacity
| [13] | Kandel N, Chungong S, Omaar A, Xing J. Health security capacities in the context of COVID-19 outbreak: an analysis of International Health Regulations annual report data from 182 countries. Lancet. 2020; 395(10229): 1047-1053.
https://doi.org/10.1016/S0140-6736(20)30551-7 |
[13]
. Oppenheim et al. also noted that preparedness indices may identify broad capacity gaps but may not fully capture whether health systems can function effectively during real emergencies
| [14] | Oppenheim B, Gallivan M, Madhav NK, Brown N, Serhiyenko V, Wolfe ND, et al. Assessing global preparedness for the next pandemic: development and application of an Epidemic Preparedness Index. BMJ Glob Health. 2019; 4(1): e001157.
https://doi.org/10.1136/bmjgh-2018-001157 |
[14]
. These findings show that preparedness requires more than formal compliance; it requires functional systems, financing and operational readiness. The Joint External Evaluation was developed as part of the IHR Monitoring and Evaluation Framework to assess country capacities across technical areas such as surveillance, laboratories, emergency preparedness, risk communication, antimicrobial resistance, zoonotic diseases and points of entry
| [12] | World Health Organization. Joint External Evaluation tool: International Health Regulations. Geneva: WHO; 2016. |
| [24] | World Health Organization Regional Office for Africa. NCDC/WHO map resources for NAPHS in 36 states and Federal Capital Territory. Brazzaville: WHO AFRO; 2019. |
[12, 24]
. However, assessment alone is not sufficient. Countries require implementation plans that translate JEE findings into clear activities, budgets and accountability structures. This is the purpose of the NAPHS framework
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
[16]
.
2.3. National Action Plan for Health Security
NAPHS is a policy and planning instrument designed to help countries strengthen IHR core capacities through a multisectoral and all-hazards approach
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
[16]
. It is intended to convert assessment findings into costed and prioritised actions that can guide implementation, resource mobilisation and monitoring
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [19] | Bell JA, Nuzzo JB. Global Health Security Index: advancing collective action and accountability amid global crisis. Washington, DC: Nuclear Threat Initiative; 2021. |
[16, 19]
. Unlike general health-sector plans, NAPHS focuses specifically on capacities required to prevent, detect and respond to health security threats. The literature identifies NAPHS as important for three main reasons. First, it provides a strategic roadmap for addressing health security gaps identified through JEE, after-action reviews and simulation exercises
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [24] | World Health Organization Regional Office for Africa. NCDC/WHO map resources for NAPHS in 36 states and Federal Capital Territory. Brazzaville: WHO AFRO; 2019. |
[16, 24]
. Second, it supports multisectoral coordination by bringing together human health, animal health, environmental health, finance, transport, security, agriculture and other sectors
. Third, it supports accountability by identifying priorities, responsible institutions, timelines and funding needs
| [19] | Bell JA, Nuzzo JB. Global Health Security Index: advancing collective action and accountability amid global crisis. Washington, DC: Nuclear Threat Initiative; 2021. |
| [28] | Resolve to Save Lives. Developing the 2024 National Action Plan for Health Security annual operational plan, Lagos, Nigeria. New York: Resolve to Save Lives; 2024. |
[19, 28]
. Nevertheless, the effectiveness of NAPHS depends on implementation. A plan may be well designed but remain weak if it is not linked to domestic budgets, legal mandates, trained personnel and subnational implementation structures
| [13] | Kandel N, Chungong S, Omaar A, Xing J. Health security capacities in the context of COVID-19 outbreak: an analysis of International Health Regulations annual report data from 182 countries. Lancet. 2020; 395(10229): 1047-1053.
https://doi.org/10.1016/S0140-6736(20)30551-7 |
| [15] | Katz R, Dowell SF. Revising the International Health Regulations: call for a 2017 review conference. Lancet Glob Health. 2015; 3(7): e352-e353.
https://doi.org/10.1016/S2214-109X(15)00009-7 |
| [28] | Resolve to Save Lives. Developing the 2024 National Action Plan for Health Security annual operational plan, Lagos, Nigeria. New York: Resolve to Save Lives; 2024. |
[13, 15, 28]
. This makes the Nigerian case important because it shows how a national health security plan operates within a federal governance system where health responsibilities are shared across federal, state and local levels.
2.4. Nigeria’s Health Security Context
Nigeria faces a complex health security environment due to its large population, high mobility, recurrent disease outbreaks, ecological diversity and federal governance structure
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
| [21] | Nigeria Centre for Disease Control and Prevention. Nigeria commences its second Joint External Evaluation for the International Health Regulations core capacities. Abuja: NCDC; 2023. |
| [22] | Nkengasong JN, Maiyegun O, Moeti M. Establishing the Africa Centres for Disease Control and Prevention: responding to Africa’s health threats. Lancet Glob Health. 2017; 5(3): e246-e247. https://doi.org/10.1016/S2214-109X(17)30025-6 |
| [23] | World Health Organization. Joint external evaluation of the International Health Regulations core capacities of Nigeria: mission report, 14-18 August 2023. Geneva: WHO; 2024. |
[20-23]
. Repeated outbreaks of Lassa fever, cholera, meningitis, yellow fever and mpox have demonstrated the need for strong surveillance, laboratory capacity, risk communication and emergency preparedness systems
| [21] | Nigeria Centre for Disease Control and Prevention. Nigeria commences its second Joint External Evaluation for the International Health Regulations core capacities. Abuja: NCDC; 2023. |
| [23] | World Health Organization. Joint external evaluation of the International Health Regulations core capacities of Nigeria: mission report, 14-18 August 2023. Geneva: WHO; 2024. |
[21, 23]
. Nigeria’s position in West Africa also makes its preparedness important for regional health security. Nigeria’s NAPHS 2018-2022 was developed to address health security gaps identified through national assessments, including the Joint External Evaluation
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
| [24] | World Health Organization Regional Office for Africa. NCDC/WHO map resources for NAPHS in 36 states and Federal Capital Territory. Brazzaville: WHO AFRO; 2019. |
[20, 24]
. The plan consolidated several existing strategies and workplans, including disease surveillance, antimicrobial resistance, immunisation, emergency preparedness and laboratory strengthening
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
[20]
. This integration was important because fragmented planning can create duplication, weak accountability and inefficient resource use. The Nigeria Centre for Disease Control and Prevention plays a central role in the country’s health security system. The NCDC Establishment Act 2018 provides the legal basis for disease surveillance, outbreak detection, investigation, prevention and control of public health threats in Nigeria
| [25] | Federal Republic of Nigeria. Nigeria Centre for Disease Control and Prevention Establishment Act, 2018. Abuja: Federal Republic of Nigeria Official Gazette; 2018. |
[25]
. National public health institutes are widely recognised as important institutional anchors for health security because they coordinate surveillance, laboratory systems, emergency operations and technical response
| [26] | Balajee SA, Pasi OG, Etoundi AGM, Rzeszotarski P, Do TT, Hennessee I, et al. Sustainable model for public health emergency operations centers for global settings. Emerg Infect Dis. 2017; 23(13): S190-S195.
https://doi.org/10.3201/eid2313.170682 |
| [27] | Nkengasong JN, Tessema SK. Africa needs a new public health order to tackle infectious disease threats. Cell. 2020; 183(2): 296-300. https://doi.org/10.1016/j.cell.2020.09.004 |
[26, 27]
.
2.5. One Health and Multisectoral Coordination
One Health is a major principle in health security because many public health threats emerge from interactions among humans, animals and the environment
. Zinsstag et al. described One Health as an integrated approach to human, animal and ecosystem health
. Mackenzie and Jeggo argued that One Health is essential for managing zoonotic diseases, antimicrobial resistance and other complex health threats that cannot be addressed by the health sector alone
. Nigeria’s health security context makes One Health especially relevant. Zoonotic diseases, antimicrobial resistance, food safety risks and environmental health threats require collaboration among public health authorities, veterinary services, agriculture, environment, laboratories and community systems
| [17] | Zinsstag J, Schelling E, Waltner-Toews D, Tanner M. From “one medicine” to “one health” and systemic approaches to health and well-being. Prev Vet Med. 2011; 101(3-4): 148-156. https://doi.org/10.1016/j.prevetmed.2011.05.008 |
| [18] | Mackenzie JS, Jeggo M. The One Health approach: why is it so important? Trop Med Infect Dis. 2019; 4(2): 88.
https://doi.org/10.3390/tropicalmed4020088 |
| [30] | Destoumieux-Garzón D, Mavingui P, Boëtsch G, Boissier J, Darriet F, Duboz P, et al. The One Health concept: 10 years old and a long road ahead. Front Vet Sci. 2018; 5: 14.
https://doi.org/10.3389/fvets.2018.00014 |
[17, 18, 30]
. However, effective One Health implementation requires more than policy statements. It requires joint planning, shared surveillance, interoperable data systems, coordinated response mechanisms and sustainable financing
. Weak inter-agency coordination remains a common challenge in health security governance. Different ministries and agencies often operate with separate mandates, budgets and reporting systems
| [15] | Katz R, Dowell SF. Revising the International Health Regulations: call for a 2017 review conference. Lancet Glob Health. 2015; 3(7): e352-e353.
https://doi.org/10.1016/S2214-109X(15)00009-7 |
| [28] | Resolve to Save Lives. Developing the 2024 National Action Plan for Health Security annual operational plan, Lagos, Nigeria. New York: Resolve to Save Lives; 2024. |
[15, 28]
. In Nigeria, these coordination challenges are further complicated by the need to align federal, state and local government structures. Therefore, effective NAPHS implementation requires strong horizontal coordination across sectors and vertical coordination across levels of government.
2.6. Surveillance, Laboratory Systems and Workforce Capacity
Surveillance is a core pillar of health security because early detection determines how quickly threats can be investigated and contained
| [31] | Nsubuga P, White ME, Thacker SB, Anderson MA, Blount SB, Broome CV, et al. Public health surveillance: a tool for targeting and monitoring interventions. In: Jamison DT, Breman JG, Measham AR, et al., editors. Disease control priorities in developing countries. 2nd ed. Washington, DC: World Bank; 2006. |
[31]
. Effective surveillance requires timely reporting, data analysis, feedback, community participation and trained personnel. Weak surveillance systems can delay outbreak detection and increase the risk of wider transmission
| [31] | Nsubuga P, White ME, Thacker SB, Anderson MA, Blount SB, Broome CV, et al. Public health surveillance: a tool for targeting and monitoring interventions. In: Jamison DT, Breman JG, Measham AR, et al., editors. Disease control priorities in developing countries. 2nd ed. Washington, DC: World Bank; 2006. |
| [32] | Woolhouse MEJ, Gowtage-Sequeria S. Host range and emerging and reemerging pathogens. Emerg Infect Dis. 2005; 11(12): 1842-1847. https://doi.org/10.3201/eid1112.050997 |
[31, 32]
. Laboratory systems are also central to preparedness because suspected public health events require rapid and accurate confirmation
. The West African Ebola epidemic showed that delays in laboratory confirmation and weak diagnostic systems can worsen outbreak spread
| [5] | Frieden TR, Damon I, Bell BP, Kenyon T, Nichol S. Ebola 2014: new challenges, new global response and responsibility. N Engl J Med. 2014; 371(13): 1177-1180.
https://doi.org/10.1056/NEJMra1411025 |
| [6] | Moon S, Sridhar D, Pate MA, Jha AK, Clinton C, Delaunay S, et al. Will Ebola change the game? Ten essential reforms before the next pandemic. Lancet. 2015; 386(10009): 2204-2221.
https://doi.org/10.1016/S0140-6736(15)00946-0 |
[5, 6]
. For Nigeria, laboratory strengthening and specimen referral systems are therefore essential for improving outbreak detection and response. Workforce capacity is another important determinant of health security. Preparedness depends on trained epidemiologists, laboratory scientists, clinicians, veterinarians, risk communication officers, emergency managers and community health workers
| [26] | Balajee SA, Pasi OG, Etoundi AGM, Rzeszotarski P, Do TT, Hennessee I, et al. Sustainable model for public health emergency operations centers for global settings. Emerg Infect Dis. 2017; 23(13): S190-S195.
https://doi.org/10.3201/eid2313.170682 |
| [31] | Nsubuga P, White ME, Thacker SB, Anderson MA, Blount SB, Broome CV, et al. Public health surveillance: a tool for targeting and monitoring interventions. In: Jamison DT, Breman JG, Measham AR, et al., editors. Disease control priorities in developing countries. 2nd ed. Washington, DC: World Bank; 2006. |
[26, 31]
. Field epidemiology and public health emergency operations require skilled personnel who can be rapidly deployed during outbreaks. In federal systems, workforce capacity must also be distributed across subnational levels rather than concentrated only at the national level.
2.7. Financing and Implementation Barriers
Sustainable financing is one of the most important requirements for health security. Preparedness investments often follow a cycle of “panic and neglect,” where funding increases during crises but declines when outbreaks subside
| [7] | World Bank. People, pathogens and our planet: the economics of One Health. Washington, DC: World Bank; 2012. |
| [19] | Bell JA, Nuzzo JB. Global Health Security Index: advancing collective action and accountability amid global crisis. Washington, DC: Nuclear Threat Initiative; 2021. |
[7, 19]
. This pattern weakens long-term preparedness because surveillance, laboratories, emergency operations centres and workforce development require continuous investment. In many low- and middle-income countries, health security activities depend heavily on donor support
| [19] | Bell JA, Nuzzo JB. Global Health Security Index: advancing collective action and accountability amid global crisis. Washington, DC: Nuclear Threat Initiative; 2021. |
| [28] | Resolve to Save Lives. Developing the 2024 National Action Plan for Health Security annual operational plan, Lagos, Nigeria. New York: Resolve to Save Lives; 2024. |
[19, 28]
. While external support can strengthen capacity, overdependence on donors may reduce sustainability if domestic financing is weak. Bell and Nuzzo argued that preparedness measurement should be linked to financing and accountability if countries are to improve real-world capacity
| [19] | Bell JA, Nuzzo JB. Global Health Security Index: advancing collective action and accountability amid global crisis. Washington, DC: Nuclear Threat Initiative; 2021. |
[19]
. This is relevant to Nigeria because NAPHS implementation requires predictable funding at both federal and state levels. Implementation barriers also include weak political commitment, poor data systems, limited infrastructure, workforce shortages and weak monitoring and evaluation
| [13] | Kandel N, Chungong S, Omaar A, Xing J. Health security capacities in the context of COVID-19 outbreak: an analysis of International Health Regulations annual report data from 182 countries. Lancet. 2020; 395(10229): 1047-1053.
https://doi.org/10.1016/S0140-6736(20)30551-7 |
| [14] | Oppenheim B, Gallivan M, Madhav NK, Brown N, Serhiyenko V, Wolfe ND, et al. Assessing global preparedness for the next pandemic: development and application of an Epidemic Preparedness Index. BMJ Glob Health. 2019; 4(1): e001157.
https://doi.org/10.1136/bmjgh-2018-001157 |
| [15] | Katz R, Dowell SF. Revising the International Health Regulations: call for a 2017 review conference. Lancet Glob Health. 2015; 3(7): e352-e353.
https://doi.org/10.1016/S2214-109X(15)00009-7 |
| [28] | Resolve to Save Lives. Developing the 2024 National Action Plan for Health Security annual operational plan, Lagos, Nigeria. New York: Resolve to Save Lives; 2024. |
[13-15, 28]
. These barriers can prevent national plans from producing measurable preparedness outcomes. Therefore, NAPHS implementation must be supported by domestic financing, strong coordination, state-level operational plans and regular monitoring.
2.8. Health Security, Universal Health Coverage and System Resilience
Recent literature argues that health security and universal health coverage should be linked rather than treated as separate agendas
| [10] | Lal A, Erondu NA, Heymann DL, Gitahi G, Yates R. Fragmented health systems in COVID-19: rectifying the misalignment between global health security and universal health coverage. Lancet. 2021; 397(10268): 61-67.
https://doi.org/10.1016/S0140-6736(20)32207-3 |
| [33] | Wenham C, Katz R, Birungi C, Boden L, Eccleston-Turner M, Gostin L, et al. Global health security and universal health coverage: from a marriage of convenience to a strategic, effective partnership. BMJ Glob Health. 2019; 4(1): e001145.
https://doi.org/10.1136/bmjgh-2018-001145 |
[10, 33]
. Lal et al. argued that COVID-19 exposed the risks of fragmented health systems and showed the need to align health security with universal health coverage
| [10] | Lal A, Erondu NA, Heymann DL, Gitahi G, Yates R. Fragmented health systems in COVID-19: rectifying the misalignment between global health security and universal health coverage. Lancet. 2021; 397(10268): 61-67.
https://doi.org/10.1016/S0140-6736(20)32207-3 |
[10]
. Wenham et al. also argued that global health security and universal health coverage should function as a strategic partnership
| [33] | Wenham C, Katz R, Birungi C, Boden L, Eccleston-Turner M, Gostin L, et al. Global health security and universal health coverage: from a marriage of convenience to a strategic, effective partnership. BMJ Glob Health. 2019; 4(1): e001145.
https://doi.org/10.1136/bmjgh-2018-001145 |
[33]
. This argument is relevant to Nigeria because emergency preparedness depends on the strength of routine health services. Public health threats are often first detected at community or primary health care level. If local health facilities lack trained staff, diagnostic capacity, communication systems and public trust, national preparedness will remain weak. Therefore, NAPHS should be integrated with primary health care strengthening, workforce development, health information systems and universal health coverage.
2.9. Empirical Gap
Existing literature and policy documents provide important evidence on the design, objectives and technical requirements of NAPHS
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
| [24] | World Health Organization Regional Office for Africa. NCDC/WHO map resources for NAPHS in 36 states and Federal Capital Territory. Brazzaville: WHO AFRO; 2019. |
[16, 20, 24]
. However, there is limited empirical evidence on how stakeholders perceive NAPHS implementation in Nigeria. This gap is important because policy implementation depends on awareness, ownership, coordination and participation among relevant actors
| [14] | Oppenheim B, Gallivan M, Madhav NK, Brown N, Serhiyenko V, Wolfe ND, et al. Assessing global preparedness for the next pandemic: development and application of an Epidemic Preparedness Index. BMJ Glob Health. 2019; 4(1): e001157.
https://doi.org/10.1136/bmjgh-2018-001157 |
| [29] | Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015; 10: 53.
https://doi.org/10.1186/s13012-015-0242-0 |
[14, 29]
. This study addresses the gap by examining stakeholder awareness of NAPHS, perceived implementation effectiveness, perceived improvements in health security domains, barriers to implementation and recommendations for strengthening the policy. The study contributes to health security literature by linking national health policy planning with empirical evidence on implementation challenges in Nigeria.
3. Materials and Methods
3.1. Study Design
This study adopted a quantitative cross-sectional survey design supported by documentary policy analysis. The cross-sectional design was appropriate because the study examined stakeholders’ awareness, perceptions and assessment of Nigeria’s National Action Plan for Health Security (NAPHS) at a specific point in time. The documentary component was used to provide policy context by reviewing relevant health security documents, including the International Health Regulations, WHO NAPHS guidance, Nigeria’s NAPHS 2018-2022, the NCDC Establishment Act and Nigeria’s Joint External Evaluation materials
| [11] | World Health Organization. International Health Regulations. Geneva: WHO; 2005. |
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
| [23] | World Health Organization. Joint external evaluation of the International Health Regulations core capacities of Nigeria: mission report, 14-18 August 2023. Geneva: WHO; 2024. |
| [25] | Federal Republic of Nigeria. Nigeria Centre for Disease Control and Prevention Establishment Act, 2018. Abuja: Federal Republic of Nigeria Official Gazette; 2018. |
[11, 16, 20, 23, 25]
.
3.2. Study Setting
The study was conducted within the context of Nigeria’s health security system. Nigeria was selected because of its recurrent exposure to epidemic-prone diseases and public health emergencies, including Lassa fever, cholera, meningitis, yellow fever, mpox and other infectious disease threats
| [21] | Nigeria Centre for Disease Control and Prevention. Nigeria commences its second Joint External Evaluation for the International Health Regulations core capacities. Abuja: NCDC; 2023. |
| [23] | World Health Organization. Joint external evaluation of the International Health Regulations core capacities of Nigeria: mission report, 14-18 August 2023. Geneva: WHO; 2024. |
[21, 23]
. The study focused on institutions and stakeholders involved in health security policy, disease surveillance, emergency preparedness, laboratory systems, risk communication, One Health coordination, monitoring and evaluation, and public health programme implementation.
3.3. Study Population
The study population comprised stakeholders involved in Nigeria’s health security planning and implementation. These included respondents from federal ministries and agencies, state ministries of health, international partner organisations, non-governmental organisations, primary health care structures and community-level implementation settings. These categories were considered relevant because NAPHS implementation requires coordination across national, subnational, partner and frontline health system levels.
3.4. Sample Size and Sampling Technique
Data were collected from 380 respondents. A purposive sampling technique was used to select respondents with relevant knowledge of NAPHS, health security policy, disease surveillance, outbreak preparedness or public health emergency response. This sampling approach was considered appropriate because NAPHS is a specialised policy framework, and the study required responses from individuals with direct or indirect knowledge of health security planning and implementation in Nigeria.
3.5. Data Collection Instrument
Data were collected using a structured questionnaire developed in line with the objectives of the study and the major domains of health security policy. The questionnaire contained categorical, binary and Likert-scale items. It covered respondents’ institutional profile, familiarity with NAPHS, perceived relevance of NAPHS, policy alignment, implementation effectiveness, perceived improvement in health security domains, funding adequacy, inter-agency coordination, One Health awareness, NAPHS-related training, implementation barriers and policy recommendations. The Likert-scale items were measured on a five-point scale, where 1 represented the lowest level of agreement or assessment and 5 represented the highest level. Binary response items were used to identify barriers and recommendations, while categorical items were used to capture organisation type, work level, years of experience and direct involvement in NAPHS-related activities.
3.6. Variables and Measurement
The main outcome variable was perceived improvement in health security preparedness under NAPHS. This was measured through respondents’ assessment of improvements in disease surveillance, laboratory capacity, emergency response, risk communication, community engagement, digital/data systems, monitoring and evaluation, inter-agency coordination, workforce training, and funding/resource mobilisation. The explanatory variables included respondents’ familiarity with NAPHS, direct involvement in NAPHS-related activities, institutional affiliation, work level, years of experience, perceived relevance of NAPHS, policy alignment, funding adequacy, coordination effectiveness, One Health awareness and exposure to NAPHS-related training. Implementation barriers were measured using binary responses. The barriers assessed included inadequate funding, weak inter-agency coordination, inadequate workforce capacity, overdependence on donor funding, limited political commitment, weak state/local implementation, poor infrastructure and poor data management. Policy recommendations were also measured using binary response options.
3.7. Data Sources
The study used both primary and secondary data. Primary data were collected from 380 respondents using the structured questionnaire. Secondary data were obtained through documentary review of relevant official and scholarly sources, including the International Health Regulations, WHO NAPHS guidance, Nigeria’s NAPHS 2018-2022, the NCDC Establishment Act, Nigeria’s Joint External Evaluation report and related health security literature
| [11] | World Health Organization. International Health Regulations. Geneva: WHO; 2005. |
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
| [23] | World Health Organization. Joint external evaluation of the International Health Regulations core capacities of Nigeria: mission report, 14-18 August 2023. Geneva: WHO; 2024. |
| [25] | Federal Republic of Nigeria. Nigeria Centre for Disease Control and Prevention Establishment Act, 2018. Abuja: Federal Republic of Nigeria Official Gazette; 2018. |
[11, 16, 20, 23, 25]
.
3.8. Validity and Reliability
Content validity was ensured by aligning the questionnaire items with the major domains of NAPHS and health security preparedness. These domains included governance, surveillance, laboratory capacity, emergency preparedness, risk communication, workforce development, financing, One Health coordination, monitoring and evaluation, and subnational implementation
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
| [23] | World Health Organization. Joint external evaluation of the International Health Regulations core capacities of Nigeria: mission report, 14-18 August 2023. Geneva: WHO; 2024. |
[16, 20, 23]
. Reliability was supported through the use of standardised response options, consistent coding and clearly defined variable categories. Where applicable, internal consistency of related Likert-scale items should be assessed using Cronbach’s alpha. A Cronbach’s alpha value of 0.70 or above is generally considered acceptable for health policy and social science research.
3.9. Data Analysis
Data were analysed using descriptive and inferential statistical methods. Descriptive statistics, including frequencies and percentages, were used to summarise respondents’ background characteristics, NAPHS awareness, perceived relevance, policy alignment, implementation effectiveness, perceived improvement in health security domains, implementation barriers and policy recommendations. Cross-tabulations were used to examine differences in responses across work level, institutional category, NAPHS familiarity and direct involvement in NAPHS-related activities. Chi-square tests of independence were used to test associations between categorical variables. Cramér’s V was used to determine the strength of statistically significant associations. Statistical significance was assessed at the 5% level.
Results were presented using Tables and Figures. Figures were used to provide visual summaries of key findings, including familiarity with NAPHS, perceived improvement in health security domains, work-level differences in NAPHS familiarity, implementation barriers and stakeholder recommendations.
3.10. Ethical Considerations
Ethical approval for the study was obtained from the Health Research and Ethics Review Committee, Bingham University Teaching Hospital, Jos, Plateau State. The approval number was not stated in the available thesis document. Respondents were informed about the purpose of the study, and participation was entirely voluntary. Informed consent was obtained from all participants before data collection, and respondents were informed of their right to decline participation or withdraw from the study at any stage without penalty. To ensure privacy and confidentiality, all responses were anonymised and coded before analysis. No personal identifiers, names, job titles or institutional details that could reveal respondents’ identities were included in the analysis or final report. The collected data were handled confidentially, stored securely and used strictly for research purposes. Findings were reported in aggregate form to ensure that no individual respondent or institution could be identified.
4. Results
4.1. Respondents’ Background Characteristics
A total of 380 respondents were analysed. Federal ministries/agencies constituted the largest institutional group, representing 45.0% of the sample. State ministries of health accounted for 25.0%, while international partners/NGOs and PHC/community-level stakeholders each accounted for 15.0%. Most respondents had substantial professional experience, with 38.4% reporting 6-10 years of experience and 32.9% reporting more than 10 years. Overall, 71.1% of respondents reported direct involvement in NAPHS-related activities.
Table 1. Respondents’ background characteristics.
Variable | Category | Frequency | Percentage |
Organisation type | Federal ministry/agency | 171 | 45.0 |
| State ministry of health | 95 | 25.0 |
| International partner/NGO | 57 | 15.0 |
| PHC/community-level stakeholder | 57 | 15.0 |
Work level | Federal | 171 | 45.0 |
| State | 95 | 25.0 |
| International/partner | 57 | 15.0 |
| Community/facility | 57 | 15.0 |
Years of experience | Less than 2 years | 23 | 6.1 |
| 2-5 years | 86 | 22.6 |
| 6-10 years | 146 | 38.4 |
| More than 10 years | 125 | 32.9 |
Direct NAPHS involvement | Yes | 270 | 71.1 |
| No | 110 | 28.9 |
4.2. Awareness, Relevance and Policy Alignment
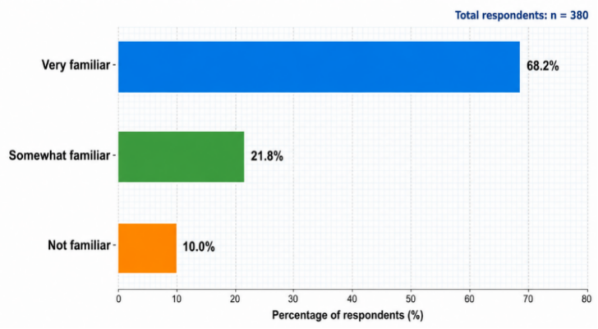
Awareness of NAPHS was high among respondents. A total of 68.2% were very familiar with NAPHS, 21.8% were somewhat familiar, and 10.0% were not familiar. The estimated proportion of respondents who were very familiar with NAPHS was 68.2% with a 95% confidence interval of 63.5%-72.8%.
Figure 2. Respondents’ level of familiarity with Nigeria’s National Action Plan for Health Security.
Most respondents considered NAPHS relevant to Nigeria’s health security needs. Overall, 90.3% reported that NAPHS was relevant, with a 95% confidence interval of 87.3%-93.2%. In addition, 81.1% perceived NAPHS as moderately or highly aligned with Nigeria’s national policy priorities, while 80.8% perceived it as moderately or highly aligned with international health security frameworks.
Table 2. Awareness, relevance and alignment indicators.
Indicator | Frequency | Percentage | 95% CI |
Very familiar with NAPHS | 259 | 68.2 | 63.5-72.8 |
NAPHS relevant to Nigeria | 343 | 90.3 | 87.3-93.2 |
Moderate/high alignment with national policy priorities | 308 | 81.1 | 77.1-85.0 |
Moderate/high alignment with international frameworks | 307 | 80.8 | 76.8-84.8 |
Very/moderately effective implementation | 264 | 69.5 | 64.8-74.1 |
Significant/moderate preparedness improvement | 303 | 79.7 | 75.7-83.8 |
NAPHS adequately funded | 50 | 13.2 | 9.8-16.6 |
Aware of formal One Health mechanism | 133 | 35.0 | 30.2-39.8 |
Received NAPHS-related training | 190 | 50.0 | 45.0-55.0 |
4.3. Policy Perception Indicators and Implementation Effectiveness
The highest mean scores were recorded for clarity of the NAPHS framework and policymaker understanding, each with a mean score of 4.15. Preparedness support also recorded a high mean score of 4.13, followed by IHR alignment with a mean score of 4.06. Multisectoral collaboration recorded a moderate score of 3.51, while frontline understanding recorded the weakest score of 2.59. This indicates that respondents perceived NAPHS as clear and policy-relevant, but less well understood at frontline implementation levels.
Table 3. Mean scores for selected NAPHS policy perception indicators.
Indicator | Mean | Standard deviation |
Framework clarity | 4.15 | 0.93 |
Policymaker understanding | 4.15 | 0.90 |
Preparedness support | 4.13 | 0.91 |
IHR alignment | 4.06 | 0.99 |
Multisectoral collaboration | 3.51 | 1.05 |
Frontline understanding | 2.59 | 1.10 |
NAPHS implementation was perceived as moderately effective. Only 9.2% of respondents rated implementation as very effective, while 60.3% rated it as moderately effective. In contrast, 20.3% rated implementation as slightly effective, 7.4% rated it as not effective, and 2.9% were not sure. Overall, 69.5% of respondents rated implementation as either very or moderately effective.
Table 4. Perceived implementation effectiveness of NAPHS.
Implementation effectiveness | Frequency | Percentage |
Very effective | 35 | 9.2 |
Moderately effective | 229 | 60.3 |
Slightly effective | 77 | 20.3 |
Not effective | 28 | 7.4 |
Not sure | 11 | 2.9 |
Total | 380 | 100.0 |
4.4. Health Security Preparedness Improvement
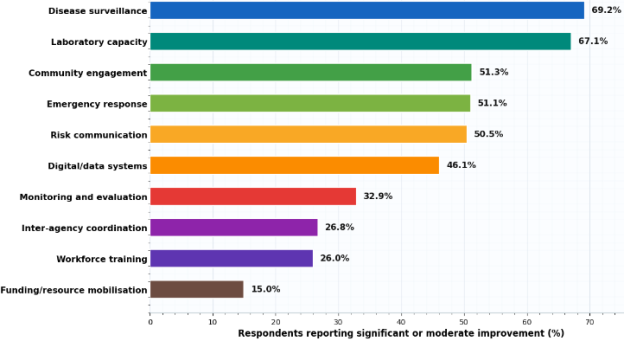
Overall, 79.7% of respondents reported significant or moderate improvement in Nigeria’s health security preparedness under NAPHS. At the domain level, improvement was strongest in disease surveillance and laboratory capacity. Disease surveillance recorded 69.2% significant/moderate improvement, while laboratory capacity recorded 67.1%. Community engagement, emergency response and risk communication recorded moderate levels of perceived improvement, each slightly above 50%. The weakest domains were funding/resource mobilisation, workforce training and inter-agency coordination. Funding/resource mobilisation recorded only 15.0% significant/moderate improvement, while workforce training and inter-agency coordination recorded 26.0% and 26.8%, respectively.
Figure 3. Perceived improvement in selected health security domains under NAPHS implementation.
Note: Mean scores were calculated using the following coding: 1 = no improvement, 2 = minimal improvement, 3 = moderate improvement, and 4 = significant improvement. “Not sure” responses were excluded from mean-score computation.
The overall domain improvement index had a mean of 2.51 and a standard deviation of 0.29 on a four-point scale. This shows that respondents’ overall assessment clustered between minimal and moderate improvement, confirming that NAPHS was perceived to have made progress but not yet reached strong implementation impact across all health security domains.
4.5. Financing, Coordination, One Health and Training Capacity
Financing emerged as one of the weakest implementation areas. Only 13.2% of respondents stated that NAPHS was adequately funded, while 86.8% reported inadequate funding. International donors/partners were the most frequently reported funding source, followed by federal government budgetary support. This indicates that NAPHS implementation remains strongly dependent on external financing. Coordination was also mixed. Only 6.3% of respondents rated coordination as very effective, while 40.0% rated it as moderately effective. However, 37.4% rated coordination as slightly effective, and 12.4% as ineffective. Awareness of formal One Health mechanisms was low, with only 35.0% of respondents reporting awareness. Training coverage was also limited, as only 50.0% had received NAPHS-related training.
Table 5. Implementation capacity indicators.
Indicator | Strong/positive response (%) |
NAPHS adequately funded | 13.2 |
Coordination very/moderately effective | 46.3 |
Aware of formal One Health mechanism | 35.0 |
Received NAPHS-related training | 50.0 |
Community involvement moderate/very high | 41.1 |
Risk communication very/moderately effective | 55.5 |
Clear M&E indicators available | 46.6 |
M&E very/moderately effective | 46.0 |
4.6. Barrier Burden and Implementation Constraints
Respondents reported multiple barriers to NAPHS implementation. The mean number of barriers identified per respondent was 4.62 out of 8, with a standard deviation of 1.34. The median number of barriers was 5, indicating that most respondents perceived NAPHS implementation as constrained by several simultaneous institutional and operational weaknesses.
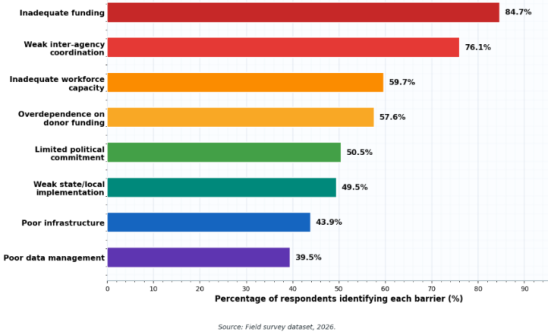
The most frequently reported barrier was inadequate funding, identified by 84.7% of respondents. This was followed by weak inter-agency coordination at 76.1%, inadequate workforce capacity at 59.7%, and overdependence on donor funding at 57.6%. Limited political commitment and weak state/local implementation were also reported by approximately half of respondents.
Barrier co-occurrence analysis showed that inadequate funding and weak coordination were jointly reported by 62.9% of respondents. Inadequate funding also co-occurred with inadequate workforce capacity among 50.8% and with donor dependence among 50.3%. This indicates that the implementation problem is not limited to one isolated constraint but reflects a combined financing, coordination and capacity gap.
Figure 4. Major barriers to effective NAPHS implementation in Nigeria.
4.7. Work-Level Differences in NAPHS Familiarity and Implementation Capacity
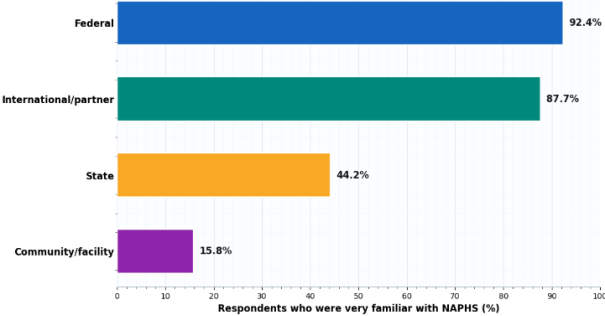
Familiarity with NAPHS varied sharply by work level. Federal-level respondents recorded the highest familiarity, with 92.4% reporting that they were very familiar with NAPHS. International/partner respondents followed closely at 87.7%. However, only 44.2% of state-level respondents and 15.8% of community/facility-level respondents reported being very familiar with NAPHS. The association between work level and NAPHS familiarity was statistically significant, χ2(3) = 153.48, p < 0.001. The effect size was large, Cramér’s V = 0.636. This indicates a strong relationship between respondents’ location in the health security system and their familiarity with NAPHS.
Figure 5. Variation in NAPHS familiarity by respondents’ work level.
Table 6. Work-level differences in selected NAPHS indicators.
Work level | Very familiar with NAPHS (%) | Implementation very/moderately effective (%) | Preparedness significant/moderate improvement (%) | Aware of One Health mechanism (%) | Received training (%) |
Federal | 92.4 | 69.6 | 76.6 | 48.5 | 53.2 |
International / partner | 87.7 | 63.2 | 80.7 | 35.1 | 56.1 |
State | 44.2 | 73.7 | 82.1 | 20.0 | 51.6 |
Community / facility | 15.8 | 68.4 | 84.2 | 19.3 | 31.6 |
Work level was not significantly associated with perceived implementation effectiveness, χ2(3) = 1.90, p = 0.594, or perceived preparedness improvement, χ2(3) = 2.10, p = 0.551. However, it was significantly associated with NAPHS-related training, χ2(3) = 9.40, p = 0.024, Cramér’s V = 0.157, and awareness of formal One Health mechanisms, χ2(3) = 29.35, p < 0.001, Cramér’s V = 0.278.
4.8. Association Between Direct Involvement and Perceived Improvement
Direct involvement in NAPHS-related activities was not significantly associated with perceived preparedness improvement. Among respondents directly involved in NAPHS-related activities, 77.8% reported significant or moderate improvement. Among respondents not directly involved, 84.5% reported significant or moderate improvement. The association was not statistically significant, χ2(1) = 1.82, p = 0.178, Cramér’s V = 0.069.
This suggests that perceived preparedness improvement was broadly shared across respondents, rather than being limited only to those directly involved in NAPHS-related activities.
4.9. Stakeholder Recommendations
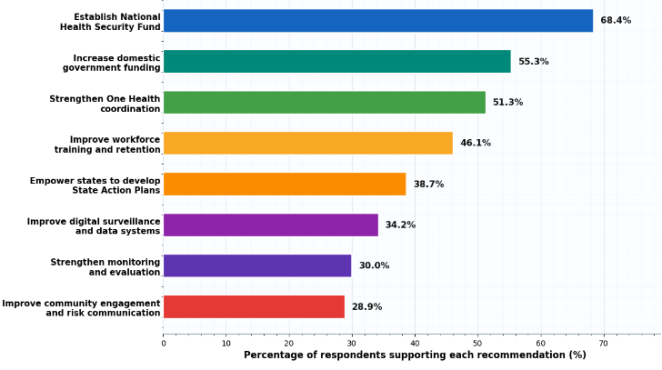
The mean number of recommendations selected per respondent was 3.53 out of 8, with a standard deviation of 1.29. The most frequently selected recommendation was the establishment of a dedicated National Health Security Fund, supported by 68.4% of respondents. This was followed by increased domestic government funding at 55.3%, stronger One Health coordination at 51.3%, and improved workforce training and retention at 46.1%.
Figure 6. Stakeholder recommendations for strengthening NAPHS implementation in Nigeria.
4.10. Inferential Summary
The strongest statistically significant association observed in the study was between work level and NAPHS familiarity, indicating that awareness is highly concentrated at federal and partner levels. Work level was also significantly associated with One Health awareness and NAPHS-related training, suggesting uneven distribution of implementation knowledge and capacity. However, work level was not significantly associated with perceived implementation effectiveness or perceived preparedness improvement.
Table 7. Summary of inferential tests.
Relationship tested | χ2 | p-value | Cramér’s V | Interpretation |
Work level × NAPHS familiarity | 153.48 | <0.001 | 0.636 | Significant, large association |
Work level × implementation effectiveness | 1.90 | 0.594 | 0.071 | Not significant |
Work level × preparedness improvement | 2.10 | 0.551 | 0.074 | Not significant |
Work level × One Health awareness | 29.35 | <0.001 | 0.278 | Significant, moderate association |
Work level × NAPHS-related training | 9.40 | 0.024 | 0.157 | Significant, weak association |
Direct involvement × preparedness improvement | 1.82 | 0.178 | 0.069 | Not significant |
5. Discussion
The findings show that NAPHS is widely recognised as a relevant policy framework for strengthening health security in Nigeria. Most respondents considered the plan aligned with national and international health security priorities, confirming its importance as a tool for implementing IHR core capacities
| [11] | World Health Organization. International Health Regulations. Geneva: WHO; 2005. |
| [16] | World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024. |
| [20] | Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018. |
[11, 16, 20]
. The study found that NAPHS contributed most strongly to improvements in disease surveillance and laboratory capacity. This suggests that the plan has supported key technical areas needed for early detection, diagnosis and outbreak response. These findings are consistent with the literature, which identifies surveillance and laboratory systems as central pillars of health security preparedness
| [31] | Nsubuga P, White ME, Thacker SB, Anderson MA, Blount SB, Broome CV, et al. Public health surveillance: a tool for targeting and monitoring interventions. In: Jamison DT, Breman JG, Measham AR, et al., editors. Disease control priorities in developing countries. 2nd ed. Washington, DC: World Bank; 2006. |
| [32] | Woolhouse MEJ, Gowtage-Sequeria S. Host range and emerging and reemerging pathogens. Emerg Infect Dis. 2005; 11(12): 1842-1847. https://doi.org/10.3201/eid1112.050997 |
[31, 32]
. However, implementation effectiveness was rated mainly as moderate. This indicates that although NAPHS has policy relevance, its operational impact remains limited. The major constraints were inadequate funding, weak inter-agency coordination, limited workforce capacity and donor dependence. These challenges reflect broader concerns that national preparedness plans may remain weak if they are not supported by sustainable financing and strong implementation systems
| [13] | Kandel N, Chungong S, Omaar A, Xing J. Health security capacities in the context of COVID-19 outbreak: an analysis of International Health Regulations annual report data from 182 countries. Lancet. 2020; 395(10229): 1047-1053.
https://doi.org/10.1016/S0140-6736(20)30551-7 |
| [14] | Oppenheim B, Gallivan M, Madhav NK, Brown N, Serhiyenko V, Wolfe ND, et al. Assessing global preparedness for the next pandemic: development and application of an Epidemic Preparedness Index. BMJ Glob Health. 2019; 4(1): e001157.
https://doi.org/10.1136/bmjgh-2018-001157 |
| [28] | Resolve to Save Lives. Developing the 2024 National Action Plan for Health Security annual operational plan, Lagos, Nigeria. New York: Resolve to Save Lives; 2024. |
[13, 14, 28]
.
The results also show that familiarity with NAPHS was higher among federal and international/partner-level respondents than among state and community/facility-level respondents. This is a major concern because public health threats are often first detected at subnational and community levels. Therefore, low awareness at these levels may weaken early detection and response capacity. The low awareness of formal One Health mechanisms also suggests that multisectoral coordination has not been fully institutionalised. Since many health threats involve human, animal and environmental systems, stronger One Health collaboration is necessary for effective preparedness and response
| [17] | Zinsstag J, Schelling E, Waltner-Toews D, Tanner M. From “one medicine” to “one health” and systemic approaches to health and well-being. Prev Vet Med. 2011; 101(3-4): 148-156. https://doi.org/10.1016/j.prevetmed.2011.05.008 |
| [18] | Mackenzie JS, Jeggo M. The One Health approach: why is it so important? Trop Med Infect Dis. 2019; 4(2): 88.
https://doi.org/10.3390/tropicalmed4020088 |
| [30] | Destoumieux-Garzón D, Mavingui P, Boëtsch G, Boissier J, Darriet F, Duboz P, et al. The One Health concept: 10 years old and a long road ahead. Front Vet Sci. 2018; 5: 14.
https://doi.org/10.3389/fvets.2018.00014 |
[17, 18, 30]
. Overall, the findings suggest that NAPHS has strengthened Nigeria’s health security policy architecture, but its effectiveness depends on improved financing, workforce development, state-level implementation, One Health coordination and monitoring systems. The next phase of NAPHS should focus less on policy design and more on practical implementation across all levels of the health system.
6. Conclusion and Recommendations
6.1. Conclusion
This study examined the role of health policy in enhancing health security in Nigeria, using the National Action Plan for Health Security (NAPHS) as a case study. The findings show that NAPHS is widely recognised as a relevant and strategically aligned policy framework for strengthening Nigeria’s preparedness and response capacity. The plan was perceived to have contributed most strongly to disease surveillance and laboratory capacity, which are essential for early detection and confirmation of public health threats. However, the study also found that NAPHS implementation remains moderate rather than strong. The main weaknesses include inadequate funding, weak inter-agency coordination, limited workforce capacity, donor dependence, low awareness of One Health mechanisms and weak state/local implementation. Familiarity with NAPHS was also concentrated among federal and partner-level stakeholders, while state and community/facility-level actors showed lower awareness. This suggests that the policy has not been fully operationalised across all levels of Nigeria’s health system. The study concludes that health policy is essential for strengthening health security, but policy design alone is insufficient. For NAPHS to achieve stronger impact, it must be supported by sustainable financing, effective coordination, trained personnel, clear monitoring systems and stronger subnational implementation. Nigeria’s NAPHS provides an important foundation for national health security, but its long-term success depends on moving from strategic planning to practical, funded and measurable implementation.
6.2. Recommendations
1) The Federal Government should establish a dedicated National Health Security Fund to provide predictable and sustainable financing for NAPHS implementation.
2) NAPHS should be integrated into federal and state annual health budgets to reduce overdependence on donor support.
3) State governments should be supported to develop State Action Plans for Health Security that align with the national NAPHS.
4) NAPHS implementation should be decentralised to state, local government and community/facility levels.
5) Inter-agency coordination should be strengthened through regular joint planning, simulation exercises, emergency preparedness reviews and accountability meetings.
6) One Health mechanisms should be institutionalised across human health, animal health, environmental health, agriculture and emergency management sectors.
7) Awareness of NAPHS should be improved among state-level and community/facility-level stakeholders.
8) Workforce development should be prioritised through regular training and retention of surveillance officers, laboratory personnel, field epidemiologists, emergency response teams, risk communication officers and community health workers.
9) Nigeria should strengthen laboratory networks, specimen referral systems and diagnostic capacity across states.
10) Digital surveillance platforms and real-time health information systems should be improved to support faster detection, reporting and response.
11) Monitoring and evaluation of NAPHS should be strengthened using clear performance indicators such as time to detection, time to notification, time to laboratory confirmation and time to response.
12) Community engagement and risk communication should be improved to strengthen public trust and community participation during health emergencies.
13) NAPHS should be linked with broader health-system strengthening, primary health care development and universal health coverage.
14) Future NAPHS reviews should use evidence from Joint External Evaluations, after-action reviews, outbreak reports and stakeholder feedback.
Abbreviations
CI | Confidence Interval |
IHR | International Health Regulations |
JEE | Joint External Evaluation |
M & E | Monitoring and Evaluation |
NAPHS | National Action Plan for Health Security |
NCDC | Nigeria Centre for Disease Control and Prevention |
NGO | Non-Governmental Organisation |
PHC | Primary Health Care |
SD | Standard Deviation |
WHO | World Health Organization |
Author Contributions
Paul Imolemen Irabor: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Resources, Software, Validation, Visualization, Writing - original draft, Writing - review & editing
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Gostin LO, Katz R. The International Health Regulations: the governing framework for global health security. Milbank Q. 2016; 94(2): 264-313.
https://doi.org/10.1111/1468-0009.12186
|
| [2] |
Morens DM, Fauci AS. Emerging infectious diseases: threats to human health and global stability. PLoS Pathog. 2013; 9(7): e1003467.
https://doi.org/10.1371/journal.ppat.1003467
|
| [3] |
Bloom DE, Cadarette D. Infectious disease threats in the twenty-first century: strengthening the global response. Front Immunol. 2019; 10: 549.
https://doi.org/10.3389/fimmu.2019.00549
|
| [4] |
Heymann DL, Chen L, Takemi K, Fidler DP, Tappero JW, Thomas MJ, et al. Global health security: the wider lessons from the West African Ebola virus disease epidemic. Lancet. 2015; 385(9980): 1884-1901.
https://doi.org/10.1016/S0140-6736(15)60858-3
|
| [5] |
Frieden TR, Damon I, Bell BP, Kenyon T, Nichol S. Ebola 2014: new challenges, new global response and responsibility. N Engl J Med. 2014; 371(13): 1177-1180.
https://doi.org/10.1056/NEJMra1411025
|
| [6] |
Moon S, Sridhar D, Pate MA, Jha AK, Clinton C, Delaunay S, et al. Will Ebola change the game? Ten essential reforms before the next pandemic. Lancet. 2015; 386(10009): 2204-2221.
https://doi.org/10.1016/S0140-6736(15)00946-0
|
| [7] |
World Bank. People, pathogens and our planet: the economics of One Health. Washington, DC: World Bank; 2012.
|
| [8] |
Kruk ME, Myers M, Varpilah ST, Dahn BT. What is a resilient health system? Lessons from Ebola. Lancet. 2015; 385(9980): 1910-1912.
https://doi.org/10.1016/S0140-6736(15)60755-3
|
| [9] |
Hanefeld J, Mayhew S, Legido-Quigley H, Martineau F, Karanikolos M, Blanchet K, et al. Towards an understanding of resilience: responding to health systems shocks. BMJ Glob Health. 2018; 3(1): e000688.
https://doi.org/10.1136/bmjgh-2017-000688
|
| [10] |
Lal A, Erondu NA, Heymann DL, Gitahi G, Yates R. Fragmented health systems in COVID-19: rectifying the misalignment between global health security and universal health coverage. Lancet. 2021; 397(10268): 61-67.
https://doi.org/10.1016/S0140-6736(20)32207-3
|
| [11] |
World Health Organization. International Health Regulations. Geneva: WHO; 2005.
|
| [12] |
World Health Organization. Joint External Evaluation tool: International Health Regulations. Geneva: WHO; 2016.
|
| [13] |
Kandel N, Chungong S, Omaar A, Xing J. Health security capacities in the context of COVID-19 outbreak: an analysis of International Health Regulations annual report data from 182 countries. Lancet. 2020; 395(10229): 1047-1053.
https://doi.org/10.1016/S0140-6736(20)30551-7
|
| [14] |
Oppenheim B, Gallivan M, Madhav NK, Brown N, Serhiyenko V, Wolfe ND, et al. Assessing global preparedness for the next pandemic: development and application of an Epidemic Preparedness Index. BMJ Glob Health. 2019; 4(1): e001157.
https://doi.org/10.1136/bmjgh-2018-001157
|
| [15] |
Katz R, Dowell SF. Revising the International Health Regulations: call for a 2017 review conference. Lancet Glob Health. 2015; 3(7): e352-e353.
https://doi.org/10.1016/S2214-109X(15)00009-7
|
| [16] |
World Health Organization. NAPHS for all: a country implementation guide for National Action Plan for Health Security. Geneva: WHO; 2024.
|
| [17] |
Zinsstag J, Schelling E, Waltner-Toews D, Tanner M. From “one medicine” to “one health” and systemic approaches to health and well-being. Prev Vet Med. 2011; 101(3-4): 148-156.
https://doi.org/10.1016/j.prevetmed.2011.05.008
|
| [18] |
Mackenzie JS, Jeggo M. The One Health approach: why is it so important? Trop Med Infect Dis. 2019; 4(2): 88.
https://doi.org/10.3390/tropicalmed4020088
|
| [19] |
Bell JA, Nuzzo JB. Global Health Security Index: advancing collective action and accountability amid global crisis. Washington, DC: Nuclear Threat Initiative; 2021.
|
| [20] |
Federal Republic of Nigeria. National Action Plan for Health Security, 2018-2022. Abuja: Nigeria Centre for Disease Control; 2018.
|
| [21] |
Nigeria Centre for Disease Control and Prevention. Nigeria commences its second Joint External Evaluation for the International Health Regulations core capacities. Abuja: NCDC; 2023.
|
| [22] |
Nkengasong JN, Maiyegun O, Moeti M. Establishing the Africa Centres for Disease Control and Prevention: responding to Africa’s health threats. Lancet Glob Health. 2017; 5(3): e246-e247.
https://doi.org/10.1016/S2214-109X(17)30025-6
|
| [23] |
World Health Organization. Joint external evaluation of the International Health Regulations core capacities of Nigeria: mission report, 14-18 August 2023. Geneva: WHO; 2024.
|
| [24] |
World Health Organization Regional Office for Africa. NCDC/WHO map resources for NAPHS in 36 states and Federal Capital Territory. Brazzaville: WHO AFRO; 2019.
|
| [25] |
Federal Republic of Nigeria. Nigeria Centre for Disease Control and Prevention Establishment Act, 2018. Abuja: Federal Republic of Nigeria Official Gazette; 2018.
|
| [26] |
Balajee SA, Pasi OG, Etoundi AGM, Rzeszotarski P, Do TT, Hennessee I, et al. Sustainable model for public health emergency operations centers for global settings. Emerg Infect Dis. 2017; 23(13): S190-S195.
https://doi.org/10.3201/eid2313.170682
|
| [27] |
Nkengasong JN, Tessema SK. Africa needs a new public health order to tackle infectious disease threats. Cell. 2020; 183(2): 296-300.
https://doi.org/10.1016/j.cell.2020.09.004
|
| [28] |
Resolve to Save Lives. Developing the 2024 National Action Plan for Health Security annual operational plan, Lagos, Nigeria. New York: Resolve to Save Lives; 2024.
|
| [29] |
Nilsen P. Making sense of implementation theories, models and frameworks. Implement Sci. 2015; 10: 53.
https://doi.org/10.1186/s13012-015-0242-0
|
| [30] |
Destoumieux-Garzón D, Mavingui P, Boëtsch G, Boissier J, Darriet F, Duboz P, et al. The One Health concept: 10 years old and a long road ahead. Front Vet Sci. 2018; 5: 14.
https://doi.org/10.3389/fvets.2018.00014
|
| [31] |
Nsubuga P, White ME, Thacker SB, Anderson MA, Blount SB, Broome CV, et al. Public health surveillance: a tool for targeting and monitoring interventions. In: Jamison DT, Breman JG, Measham AR, et al., editors. Disease control priorities in developing countries. 2nd ed. Washington, DC: World Bank; 2006.
|
| [32] |
Woolhouse MEJ, Gowtage-Sequeria S. Host range and emerging and reemerging pathogens. Emerg Infect Dis. 2005; 11(12): 1842-1847.
https://doi.org/10.3201/eid1112.050997
|
| [33] |
Wenham C, Katz R, Birungi C, Boden L, Eccleston-Turner M, Gostin L, et al. Global health security and universal health coverage: from a marriage of convenience to a strategic, effective partnership. BMJ Glob Health. 2019; 4(1): e001145.
https://doi.org/10.1136/bmjgh-2018-001145
|
Cite This Article
-
APA Style
Irabor, P. I. (2026). The Role of Health Policy in Enhancing Health Security:
A Case Study of Nigeria’s National Action Plan for Health Security (NAPHS). World Journal of Public Health, 11(3), 234-248. https://doi.org/10.11648/j.wjph.20261103.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Irabor, P. I. The Role of Health Policy in Enhancing Health Security:
A Case Study of Nigeria’s National Action Plan for Health Security (NAPHS). World J. Public Health 2026, 11(3), 234-248. doi: 10.11648/j.wjph.20261103.12
Copy
|
Download
AMA Style
Irabor PI. The Role of Health Policy in Enhancing Health Security:
A Case Study of Nigeria’s National Action Plan for Health Security (NAPHS). World J Public Health. 2026;11(3):234-248. doi: 10.11648/j.wjph.20261103.12
Copy
|
Download
-
@article{10.11648/j.wjph.20261103.12,
author = {Paul Imolemen Irabor},
title = {The Role of Health Policy in Enhancing Health Security:
A Case Study of Nigeria’s National Action Plan for Health Security (NAPHS)},
journal = {World Journal of Public Health},
volume = {11},
number = {3},
pages = {234-248},
doi = {10.11648/j.wjph.20261103.12},
url = {https://doi.org/10.11648/j.wjph.20261103.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20261103.12},
abstract = {Health security remains a critical concern in global public health, particularly in low- and middle-income countries facing recurrent infectious disease outbreaks. National health security plans provide the policy architecture for translating international commitments into domestic preparedness capacities, yet their operational effectiveness depends on stakeholder awareness, financing, coordination and subnational implementation. This study examines the role of health policy in enhancing health security in Nigeria, using the National Action Plan for Health Security (NAPHS) as a case study. Specifically, it assesses stakeholders’ awareness of NAPHS, perceived relevance of the policy framework, implementation effectiveness, perceived improvements in health security domains, barriers to implementation and recommendations for strengthening Nigeria’s preparedness system. A quantitative cross-sectional survey design supported by documentary policy analysis was adopted. Data were collected from 380 purposively selected stakeholders using a structured questionnaire covering institutional profile, familiarity with NAPHS, perceived relevance, implementation effectiveness, preparedness improvements, funding adequacy, inter-agency coordination, One Health awareness, training exposure, barriers and recommendations. Descriptive statistics, cross-tabulations, chi-square tests of independence and Cramér’s V were used for analysis. NAPHS was widely recognised as relevant (90.3%) and strategically aligned with national and international frameworks (81.1% and 80.8%, respectively). However, only 9.2% rated implementation as very effective, while 60.3% rated it moderately effective. Familiarity was strongly concentrated at the federal level (92.4%) compared with state (44.2%) and community/facility levels (15.8%). The strongest improvements were observed in disease surveillance (69.2%) and laboratory capacity (67.1%), whereas funding mobilisation (15.0%), workforce training (26.0%) and inter-agency coordination (26.8%) were the weakest domains. Inadequate funding (84.7%) and weak coordination (76.1%) were the most frequently reported barriers. While NAPHS provides a strong policy foundation for health security in Nigeria, its operational impact depends on sustainable domestic financing, decentralised implementation, strengthened coordination, workforce development and improved subnational awareness. The study contributes evidence-based recommendations for strengthening national preparedness planning in resource-constrained settings.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - The Role of Health Policy in Enhancing Health Security:
A Case Study of Nigeria’s National Action Plan for Health Security (NAPHS)
AU - Paul Imolemen Irabor
Y1 - 2026/07/11
PY - 2026
N1 - https://doi.org/10.11648/j.wjph.20261103.12
DO - 10.11648/j.wjph.20261103.12
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 234
EP - 248
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20261103.12
AB - Health security remains a critical concern in global public health, particularly in low- and middle-income countries facing recurrent infectious disease outbreaks. National health security plans provide the policy architecture for translating international commitments into domestic preparedness capacities, yet their operational effectiveness depends on stakeholder awareness, financing, coordination and subnational implementation. This study examines the role of health policy in enhancing health security in Nigeria, using the National Action Plan for Health Security (NAPHS) as a case study. Specifically, it assesses stakeholders’ awareness of NAPHS, perceived relevance of the policy framework, implementation effectiveness, perceived improvements in health security domains, barriers to implementation and recommendations for strengthening Nigeria’s preparedness system. A quantitative cross-sectional survey design supported by documentary policy analysis was adopted. Data were collected from 380 purposively selected stakeholders using a structured questionnaire covering institutional profile, familiarity with NAPHS, perceived relevance, implementation effectiveness, preparedness improvements, funding adequacy, inter-agency coordination, One Health awareness, training exposure, barriers and recommendations. Descriptive statistics, cross-tabulations, chi-square tests of independence and Cramér’s V were used for analysis. NAPHS was widely recognised as relevant (90.3%) and strategically aligned with national and international frameworks (81.1% and 80.8%, respectively). However, only 9.2% rated implementation as very effective, while 60.3% rated it moderately effective. Familiarity was strongly concentrated at the federal level (92.4%) compared with state (44.2%) and community/facility levels (15.8%). The strongest improvements were observed in disease surveillance (69.2%) and laboratory capacity (67.1%), whereas funding mobilisation (15.0%), workforce training (26.0%) and inter-agency coordination (26.8%) were the weakest domains. Inadequate funding (84.7%) and weak coordination (76.1%) were the most frequently reported barriers. While NAPHS provides a strong policy foundation for health security in Nigeria, its operational impact depends on sustainable domestic financing, decentralised implementation, strengthened coordination, workforce development and improved subnational awareness. The study contributes evidence-based recommendations for strengthening national preparedness planning in resource-constrained settings.
VL - 11
IS - 3
ER -
Copy
|
Download