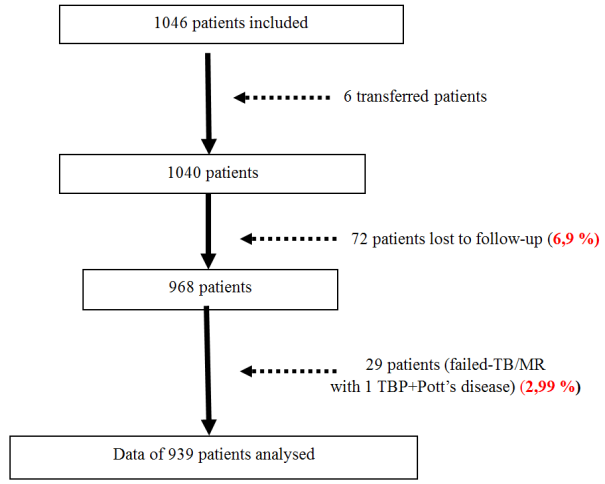
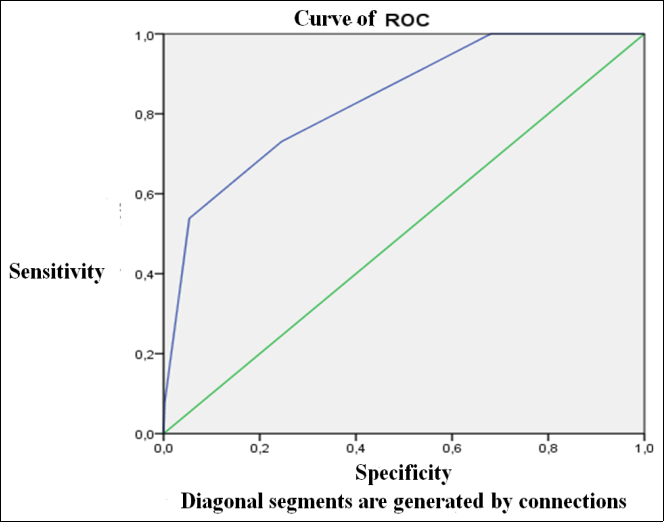
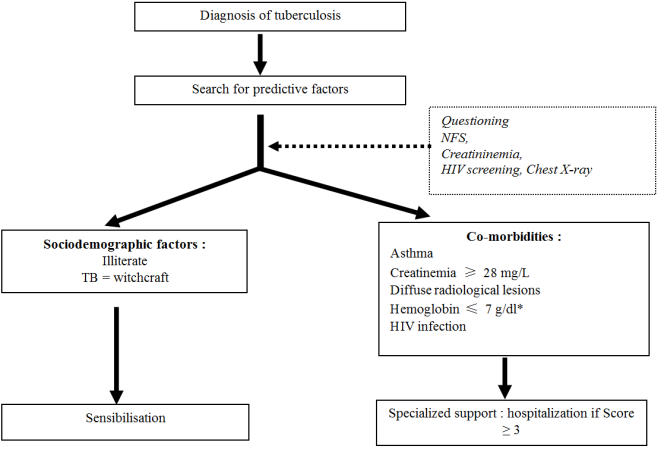
Introduction: study of the predictive factors of the deaths of tuberculosis patients to propose a decision tree for their best care in ambulatory TB centers. Methods: Prospective and observational survey, on a sample of 939 tuberculosis patients recruited in 30 CAT/CDT, carried out during supervision using collection tools such as survey forms and tuberculosis patient files. Results: 55 patients were notified dead. The mortality rate during tuberculosis was 5.9%. The Independent Factors Inducing Death (IFID) of TB were illiteracy, asthma associated with tuberculosis, assimilation of tuberculosis to witchcraft, radiological involvement of the pulmonary territories, serum creatinine ≥ 28 mg/L, HIV infection associated with TB. Associated with severe anemia for clinical concern, these factors allowed the development of the predictive score of death from TB. The ROC curve of the predictive score at death estimated the relevance of the predictive value of death with an area under the curve of 0.834 (0.755 – 0.912) (p < 0.001). The negative predictive value (NPV) of the predictive score for death during TB varied between 94.08% and 98.95%. This score is calculated on two groups of IFID. The 1st group is made up of socio-demographic factors. The 2nd group is made up of morbid situations requiring care in a specialized environment. Conclusion: The IFID imposes a management based on the use of the interrogation and the minimal radiological and biological assessment (the chest X-ray, the blood count, the dosage of creatinine and HIV serology). The decision tree-based death reduction strategy will contribute to better referral and management of patients.
| Published in | World Journal of Public Health (Volume 10, Issue 1) |
| DOI | 10.11648/j.wjph.20251001.17 |
| Page(s) | 61-76 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
Risk Factor, Deaths of Tuberculosis, Tuberculosis Patients, Predictive Score, Decision Tree
Inclusion criteria | Non-inclusion criteria | Exclusion criteria |
|---|---|---|
Cases of TPB (+) starting first-line treatment | Subject < 15 years old | Patients who died from accidents, for causes other than TB and documented (stroke with brain CT, MI with ECG) |
Chest X-ray available | Proven and progressive psychiatric disorders | Patients lost to follow-up |
HIV serology available, CD4 if HIV positive | Non-consenting patients | Patients who discontinued treatment (due to major side effects or on their own) |
Standard biological assessment available (NFS, Urea creatinine, Glycemia TGP, proteinemia, ionogram ) |
Variables | Become | P | OR, 95% CI | ||
|---|---|---|---|---|---|
Death | Success | ||||
Brutal start | Yes | 4.5% (11/246) | 95.5% (235/246) | 0.261 | 0.763 0.396 – 1.468 |
No | 5.9% (38/648) | 94.1% (610/648) | |||
Duration of signs ≥ 90 days | Yes | 7.8% (15/193) | 92.2% (178/193) | 0.098 | 1,552 0.868 – 2.775 |
No | 5% (36/719) | 95% (683/719) | |||
Cough | Yes | 5.7% (49/866) | 94.3% (817/866) | 0.063 | 0.943 0.928 – 0.959 |
No | 0% (0/49) | 100% (49/49) | |||
Hemoptysis | Yes | 2.4% (3/124) | 97.6% (121/124) | 0.057 | 0.384 0.121 – 1.218 |
No | 6.3% (45/715) | 93.7% (670/715) | |||
Chest pain | Yes | 5.9% (37/631) | 94.1% (594/931) | 0.307 | 1,246 0.661 – 2.351 |
No | 4.7% (12/255) | 95.3% (243/255) | |||
Dyspnea | Yes | 6.7% (21/312) | 93.3% (291/312) | 0.218 | 1,302 0.746 – 2.274 |
No | 5.2% (26/503) | 94.8% (477/503) | |||
Variables | Become | P | OR, 95% CI | ||
|---|---|---|---|---|---|
Death | Success | ||||
Fever | Yes | 5.4% (36/667) | 94.6% (631/667) | 0.364 | 0.864 0.482 – 1.549 |
No | 6.2% (15/240) | 93.8% (225/240) | |||
Asthenia | Yes | 6.1% (39/636) | 93.9% (597/636) | 0.248 | 1,327 0.691 – 2.547 |
No | 4.6% (11/238) | 95.4% (227/238) | |||
Anorexia | Yes | 6.5% (36/550) | 93.5% (514/550) | 0.112 | 1,497 0.832 – 2.692 |
No | 4.4% (15/343) | 95.6% (328/343) | |||
Weight loss | Yes | 5.5% (43/787) | 94.5% (744/787) | 0.367 | 0.826 0.398 – 1.715 |
No | 6.6% (8/121) | 93.4% (113/121 | |||
Night sweats | Yes | 6.2% (36/576) | 93.8% (540/576) | 0.249 | 1,283 0.714 – 2.306 |
No | 4.9% (15/308) | 95.1% (293/308) | |||
Variables | Become | p | OR, 95% CI | ||
|---|---|---|---|---|---|
Death | Success | ||||
Diarrhea | Yes | 7.9% (8/101) | 92.1% (93/101) | 0.202 | 1,473 0.714 – 3.039 |
No | 5.4% (44/818) | 94.6% (774/818) | |||
Nausea | Yes | 6.1% (13/213) | 93.9% (200/213) | 0.431 | 1,103 0.600 – 2.028 |
No | 5.5% (39/705) | 94.5% (666/705) | |||
Abdominal pain | Yes | 7.3% (17/232) | 92.7% (215/232) | 0.121 | 1,470 0.837 – 2.580 |
No | 5% (34/682) | 95% (648/682) | |||
Vomiting | Yes | 8.6% (15/174) | 91.4% (159/174) | 0.054 | 1,715 0.963 – 3.053 |
No | 5% (37/736) | 95% (699/736) | |||
Headaches | Yes | 5.1% (27/531) | 94.9% (504/531) | 0.230 | 0.789 0.465 – 1.338 |
No | 6.4% (25/388) | 93.6% (363/388) | |||
Insomnia | Yes | 7.8% (37/476) | 92.2% (439/476) | 0.004 | 2,228 1,241 – 4,002 |
No | 3.5% (15/430) | 96.5% (415/430) | |||
Variables | Become | P | OR, 95% CI | ||
|---|---|---|---|---|---|
Death | Success | ||||
BMI < 18.5 | Yes | 7.4% (28/377) | 92.6% (349/377) | 0.067 | 1,589 0.911 – 2.774 |
No | 4.7% (20/428) | 95.3% (408/428) | |||
Pulse ≥ 125 beats/min | Yes | 7.1% (1/14) | 92.9% (13/14 | 0.543 | 1,333 0.197 – 9.018 |
No | 5.4% (41/765) | 94.6% (724/765) | |||
Conjunctival pallor | Yes | 15.1% (14/93) | 84.9% (79/93) | <0.001 | 3,214 1,806 – 5,719 |
No | 4.7% (37/790) | 95.3% (753/790) | |||
Jaundice | Yes | 18.8% (3/16) | 81.2% (13/16) | 0.054 | 3,529 1,224 – 10,175 |
No | 5.3% (45/847) | 94.7% (802/847) | |||
IMO | Yes | 11.9% (5/42) | 88.1% (37/42) | 0.077 | 2,276 0.949 – 5.461 |
No | 5.2% (41/784) | 94.8% (743/784) | |||
Crackling rales | Yes | 10.2% (13/128) | 89.8% (115/128) | 0.015 | 2,213 1,179 – 4,153 |
No | 4.6% (28/610) | 95.4% (582/610) | |||
Variables | Become | P | OR, 95% CI | ||
|---|---|---|---|---|---|
Death | Success | ||||
Site of injury | Unilateral | 5.3% (17/322) | 94.7% (305/322) | 0.362 | 0.850 0.459 – 1.571 |
Bilateral | 6.2% (22/354) | 93.8% (332/354) | |||
Topography | Apical | 1.9% (5/264) | 98.1% (259/264) | 0.01 | ----------------- |
Basal | 8.1% (7/86) | 91.9% (79/86) | |||
All territories | 9.8% (26/265) | 90.2% (239/265) | |||
Lung destruction | No destruction | 4.7% (22/465) | 95.3% (443/465) | 0.071 | ------------------ |
Destroyed lung | 10.3% (12/116) | 89.7% (104/116) | |||
Destroyed lobe | 6% (6/100) | 94% (94/100) | |||
All territories reached | Yes | 9.8% (26/265) | 90.2% (239/265) | 0.001 | 2,862 1,471 – 5,565 |
No | 3.4% (12/350) | 96.6% (338/350) | |||
Variable | Become | p | OR, 95% CI | ||
|---|---|---|---|---|---|
Death | Success | ||||
TGP ≥ 80 IU/L | Yes | 5.7% (42/740) | 94.3% (698/740) | 0.467 | 0.766 0.196 – 3.002 |
No | 7.4% (2/27) | 92.6% (25/27) | |||
Creatinemia ≥ 28 mg/L | Yes | 37.5% (3/8) | 62.5% (5/8) | 0.007 | 7,256 2,823 – 18,653 |
No | 5.2% (40/774) | 94.8% (734/774) | |||
Hemoglobin ≥ 7 g/dl | Yes | 19% (4/21) | 81% (17/21) | 0.029 | 3,482 1,370 – 8,853 |
No | 5.5% (39/713) | 94.5% (674/713) | |||
Positive HIV serology | Yes | 15.6% (15/96) | 84.4% (81/96) | <0.001 | 3,990 2,194 – 7,259 |
No | 3.9% (26/664) | 96.1% (638/664) | |||
p | GOLD | IC OR, 95% | |
|---|---|---|---|
Illiteracy | 0.003 | 4,059 | 1,599 - 10,304 |
"Tuberculosis is witchcraft" | 0.011 | 3,816 | 1,360 - 10,705 |
Asthma | 0.029 | 5,933 | 1,200 - 29,333 |
Radiological damage to all pulmonary territories | 0.008 | 3,857 | 1,413 - 10,529 |
Creatinine > 28 mg/l | 0.004 | 23,651 | 2,788 - 200,650 |
HIV infection | 0.007 | 4,096 | 1,480 - 11,332 |
Total score | Staff | Proportions (%) |
|---|---|---|
0 | 143 | 30.2 |
1 | 202 | 42.6 |
2 | 91 | 19.2 |
3 | 35 | 7.4 |
4 | 3 | 0.6 |
Total | 474 | 100.0 |
Total score | Become | P | OR, 95% CI | |
|---|---|---|---|---|
Death | Not deceased | |||
= 0 | 0 % (0/143) | 100% (143/143) | <0.001 | 3,480 E -011 3,480 E -011- 3,480 E -011 |
≥ 1 | 7.9 % (26/305) | 92.1% (305/331) | <0.001 | 0.018 0.001 - 222 |
≥ 2 | 14.7% (19/129) | 85.3% (110/129) | <0.001 | 0.29 0.002 – 0.378 |
≥ 3 | 36.8% (14/38) | 63.2% (24/38) | 0.002 | 0.261 0.021 – 3.178 |
= 4 | 66.7% (2/3) | 33.3% (1/3) | - | - |
Predictive score | Sensitivity | Specificity | VPP | VPN |
|---|---|---|---|---|
≥ 1 | 100% | 31.92% | 7.85% | 100% |
≥ 2 | 53.85% | 94.64% | 36.84% | 97.25% |
≥ 3 | 7.69% | 99.78% | 66.67% | 94.9% |
HTA | High Blood Pressure |
HIV | Human ImmunoVirus |
IFID | Independent Factors Inducing Death |
TB | Tuberculosis |
Variables | Become | p | OR, 95% CI | ||
|---|---|---|---|---|---|
Death | Success | ||||
Sex | Man | 4.9% (30/618) | 95.1% (588/618) | 0.064 | 0.637 0.377 – 1.078 |
Women | 7.6% (23/302) | 92.4% (279/302) | |||
Age ≥ 45 years | Yes | 10.3% (19/184) | 89.7% (165/184) | 0.004 | 2,254 1,316 – 3,858 |
No | 4.6% (34/742) | 95.4% (708/742) | |||
CAT Residence | Commune | 5% (35/701) | 95% (666/701) | 0.049 | 0.580 0.329 – 1.090 |
Out of town | 8.6% (16/186) | 91.4% (170/186) | |||
Type of habitat | Villa | 4.3% (7/163) | 95.7% (156/163) | 0.841 | ---------------- |
Studio | 6.9% (15/217) | 93.1% (202/217 | |||
Apartment | 5.4% (23/425) | 94.6% (402/425) | |||
Hut | 6.2% (5/81) | 93.8% (76/81) | |||
homeless | 0% (0/2) | 100% (2/2) | |||
Common courtyard | Yes | 6.5% (35/539) | 93.5% (504/539) | 0.182 | 1,352 0.770 – 2.376 |
No | 4.8% (17/354) | 95.2% (337/354) | |||
Professional sector | Public service | 0 (0 %) | 100% (19/19) | 0.382 | ---------------- |
Private sector | 4.3% (7/161) | 95.7% (154/161) | |||
Informal sector | 5.7% (22/389) | 94.3% (367/389) | |||
Unemployed | 7.4% (20/270) | 92.6% (250/270) | |||
Monthly income | Regular | 4.6% (7/151) | 95.4% (144/151) | 0.674 | ----------------- |
Irregular | 4.7% (15/317) | 95.3% (302/317) | |||
No income | 6.1% (22/361) | 93.9% (339/361) | |||
Level of education | Primary | 5.9% (14/236) | 94.1% (222/236) | 0.012 | ----------------- |
Secondary | 4.5% (13/292) | 95.5% (279/292) | |||
Superior | 0.9% (1/108) | 99.1% (107/108) | |||
Not in school | 9% (25/278) | 91% (253/278) | |||
Variables | Become | p | OR, 95% CI | ||
|---|---|---|---|---|---|
Death | Success | ||||
Tuberculosis infection | Yes | 5.2% (15/286) | 94.8% (271/286) | 0.363 | 0.852 0.465 – 1.561 |
No | 6.2% (29/471) | 93.8% (442/471) | |||
Hypertensive (HTA) | Yes | 21.4% (6/28) | 78.6% (22/28) | 0.003 | 4,237 1,971 – 9,110 |
No | 5.1% (44/870) | 94.9% (826/870) | |||
Diabetes | Yes | 0% (0/14) | 100% (14/14) | 0.465 | 1,057 1,040 – 1,074 |
No | 5.4% (47/875) | 94.6% (828/875) | |||
UGD | Yes | 5.7% (5/88) | 94.3% (83/88) | 0.515 | 1,071 0.435 – 2.637 |
No | 5.3% (42/792) | 94.7% (750/792) | |||
Sickle cell disease | Yes | 12.5% (1/8) | 87.5% (7/8) | 0.357 | 2,364 0.370 – 15.103 |
No | 5.3% (47/889) | 94.7% (842/889) | |||
Known HIV infection | Yes | 15.4% (21/136) | 84.6% (115/136) | <0.001 | 3,160 1,852 – 5,390 |
No | 4.9% (28/573) | 95.1% (545/573) | |||
Asthma | Yes | 17.4% (4/23) | 82.6% (19/23) | 0.029 | 3,516 1,374 – 8,996 |
No | 4.9% (41/829) | 95.1% (188/829) | |||
Psychiatric disorders | Yes | 5.9% (1/17) | 94.1% (16/17) | 0.635 | 1,031 0.151 – 7.039 |
No | 5.7% (49/859) | 94.3% (810/859) | |||
Alcoholism | Yes | 3.3% (8/239) | 96.7% (231/239) | 0.033 | 0.493 0.236 – 1.032 |
No | 6.8% (44/648) | 93.2% (604/648) | |||
Smoking | ≥ 1 cigarette/day | 4.1% (6/147) | 95.9% (141/147) | 0.621 | ---------------- |
Weaned | 5.6% (6/107) | 94.4% (101/107 | |||
Never | 6.2% (37/600) | 93.8% (563/600) | |||
| [1] | Getahun B, Ameni G, Biadgilign S. et al. Mortality and associated risk factors in a cohort of tuberculosis patients treated under DOTS program in Addis Ababa, Ethiopia. BMC Infect Dis 2011; 11, 127. |
| [2] | WHO. Global tuberculosis control 2010, Geneva, World health organization, 2010. |
| [3] | Rubin SA. Tuberculosis: Captain of all these men of death. Radiol Clin North Am. 1995; 33: 619–39. |
| [4] | Sundre P, ten Dam G, Kochi A. Tuberculosis: A global overview of the situation today. Bull World Health Organ. 1992; 70: 149–59. |
| [5] | WHO/40. Tuberculosis, the leading cause of death in women of reproductive age, WHO, Gothenburg, Geneva. |
| [6] | Côte d’Ivoire, Annual Report of the National Tuberculosis Control Program, 2011. |
| [7] | Côte d’Ivoire, National Tuberculosis Control Program, Strategic Plan 2013-2015, Abidjan, PNLT-CI. |
| [8] | Oursler KK, Moore RD, Bishai WR, et al. Survival of patients with pulmonary tuberculosis: clinical and molecular epidemiologic factors. Clin Infect Dis 2002; 34: 752-9. |
| [9] | Waitt, CJ, & Squire, SB A systematic review of risk factors for death in adults during and after tuberculosis treatment. The international journal of tuberculosis and lung disease, Int J Tuberc Lung Dis, 2011; 15(7): 871–885. |
| [10] | Sklom D, Melamed D, Friedman A. The effect of varying levels of dietary vitamin A on immune response in the chick. Poult Sci. 1994; 73: 843–7. |
| [11] | Slama K, Chiang CY, Enarson DA. Introducing brief advice in tuberculosis services. Int J Tuberc Lung Dis 2007; 11: 496-9. |
| [12] | Paton NI, Castello-Bramco LR, Jennings G, et al. Impact of tuberculosis on the body composition of HIV-infected men in Brazil. J Acquir Immune Diefic Syndr Hum Retrovirol. 1999; 20: 265–71. |
| [13] | Shor-Posner G, Miguez MJ, Pineda LM, Rodriguez A, Ruiz P, Castillo G, et al. Impact of selenium status on the pathogenesis of mycobacterial disease on HIV-infected drug users during the era of highly active antiretroviral therapy. J Acquir Immune DeficSyndr.; 2002; 29: 169–73. |
| [14] | Pablos-Méndez, A., Sterling, TR, & Frieden, TR The relationship between delayed or incomplete treatment and all-cause mortality in patients with tuberculosis. JAMA, 1996; 276(15): 1223–1228. |
| [15] | WHO. Annual report 2015, Geneva, WHO. |
| [16] | Leung CC, Li T, Lam TH, et al. Smoking and tuberculosis among the elderly in Hong Kong. Am J RespirCrit Care Med 2004; 170: 1027-33. |
| [17] | Ramin B, Kam D, Feleke B, Jacob B, Jha P. Smoking, HIV and non-fatal tuberculosis in an urban African population. Int J Tuberc Lung Dis 2008; 12: 695-7. |
| [18] | Pednekar, M. S., & Gupta, P. C. (2007). Prospective study of smoking and tuberculosis in India. Prev med, 2007; 44(6): 496–498. |
| [19] | Lin, HH, Ezzati, M., & Murray, M. Tobacco smoke, indoor air pollution and tuberculosis: a systematic review and meta-analysis. PLoS medicine, 2007; 4(1), e20. |
| [20] | Byrd, RP, Jr, Mehta, JB, & Roy, TM Malnutrition and pulmonary tuberculosis. Clin Infect Dis, 2002; 35(5), 634–636. |
| [21] | Gupta, K. B, Gupta, R., Atreja, A., et al. Tuberculosis and nutrition. Lung India Chest Society, 2009; 26(1): 9-16. |
| [22] | Madebo T, Lindtjørn B, Aukrust P, Berge RK. Circulating antioxidants and lipid peroxidation products in untreated tuberculosis patients in Ethiopia. Am J Clin Nutr. 2003; 78: 117–22. |
| [23] | Whalen C, Semba RD. Tuberculosis. In: Semba RD, Bloem MV, (eds). Nutrition and health in developing countries. Totowa, NJ: Human Press; 2001. pp. 209–35. |
| [24] | Miller, LG, Asch, SM, Yu, EI, et al. A population-based survey of tuberculosis symptoms: how atypical are atypical presentations?. Clin Infect Dis, 2000; 30(2), 293–299. |
| [25] | Rakotondramarina D. Epidemiological aspects of tuberculosis in the middle west of Madagascar, Public Health, n°2021, 2000. |
| [26] | WHO. Tuberculosis. Fact Sheet 2011; No. 104. |
| [27] | Kayantao D. et al. Microscopy-negative pulmonary tuberculosis in a specialized hospital setting in Bamako. Méd Afr N 2001; 48(6): 243-245. |
| [28] | Gustafson, P., Gomes, VF, Vieira, CS, et al. Clinical predictors for death in HIV-positive and HIV-negative tuberculosis patients in Guinea-Bissau. Infection, 2007; 35(2): 69-80. |
| [29] | Lawn, SD, Obeng, J., Acheampong, JW, et al. Resolution of the acute-phase response in West African patients receiving treatment for pulmonary tuberculosis, Int J Tuberc Lung Dis, 2000; 4(4): 340–344. |
| [30] | Nils E. Costs for TB MDR-TB time to suit a HO Emergency committee on TB? Int. J Tuberc Lung Dis 20(4): 427. |
| [31] | Oursler KK, Moore RD, Bishai WR, Harrington SM, Pope DS, Chaisson RE, Survival of patients with pulmonary tuberculosis: clinical and molecular epidemiologic factors. Clin Infect Dis 2002; 34: 752-9. |
| [32] | Mehta JB, Shantaveerapa H, Byrd RP Jr, et al. Utility of rifampin blood levels in the treatment and follow-up of active pulmonary tuberculosis in patients who were slow to respond to routine directly observed therapy. Chest 2001; 120: 1520 - 4. |
| [33] | McMurray DN, Mintzer CL, Bartow RA, et al. Dietary protein deficiency and mycobacterium bovis BCG affect interleukin-2 activity in experimental pulmonary tuberculosis. Infect Immune. 1989; 57: 2606–11. |
| [34] | Sarraf P, Prederich RC, Turner EM, Ma G, Jaskowiak NT, Rivet DJ, 3rd, et al. Multiple cytokines and acute inflammation raise mouse leptin levels: Potential role in inflammatory anorexia. J Exp Med 1997; 185: 171–5. |
| [35] | Kuemmerer, J. M., & Comstock, G. W. (1967). Sociologic concomitants of tuberculin sensitivity, Am Rev Respir Dis, 96(5), 885–892. |
| [36] | Venkatarama KR, IademarcoEP, FrazerVJ, KollefMH, The impact of comorbidity on mortality following in-hospital diagnosis of tuberculosis. Chest 1998; 114: 1244-52. |
| [37] | Djika, M., Koudokpon, CH, Dougnon, VT, Sanoussi, N., Alphazazi, S., Ballé, B., Daouda, H., Assogba, P., Bankole, H., & Agbangla, C., Epidemiology, treatment outcome and resistance profile of pulmonary tuberculosis cases at the Niamey national anti-tuberculosis center in Niger: a retrospective study. The Pan African medical journal, 2024; 47, 214. |
APA Style
Kouamé, A., Adon, K. P., Adombi, E. M. C., Kouakou, J. (2025). Predictive Factors of Mortality of Tuberculosis Patients Dead of Tuberculosis in Côte d'Ivoire. World Journal of Public Health, 10(1), 61-76. https://doi.org/10.11648/j.wjph.20251001.17
ACS Style
Kouamé, A.; Adon, K. P.; Adombi, E. M. C.; Kouakou, J. Predictive Factors of Mortality of Tuberculosis Patients Dead of Tuberculosis in Côte d'Ivoire. World J. Public Health 2025, 10(1), 61-76. doi: 10.11648/j.wjph.20251001.17
AMA Style
Kouamé A, Adon KP, Adombi EMC, Kouakou J. Predictive Factors of Mortality of Tuberculosis Patients Dead of Tuberculosis in Côte d'Ivoire. World J Public Health. 2025;10(1):61-76. doi: 10.11648/j.wjph.20251001.17
@article{10.11648/j.wjph.20251001.17,
author = {Amenan Kouamé and Kouadio Patrick Adon and Elodie Michelle Claudia Adombi and Jacquemin Kouakou},
title = {Predictive Factors of Mortality of Tuberculosis Patients Dead of Tuberculosis in Côte d'Ivoire},
journal = {World Journal of Public Health},
volume = {10},
number = {1},
pages = {61-76},
doi = {10.11648/j.wjph.20251001.17},
url = {https://doi.org/10.11648/j.wjph.20251001.17},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251001.17},
abstract = {Introduction: study of the predictive factors of the deaths of tuberculosis patients to propose a decision tree for their best care in ambulatory TB centers. Methods: Prospective and observational survey, on a sample of 939 tuberculosis patients recruited in 30 CAT/CDT, carried out during supervision using collection tools such as survey forms and tuberculosis patient files. Results: 55 patients were notified dead. The mortality rate during tuberculosis was 5.9%. The Independent Factors Inducing Death (IFID) of TB were illiteracy, asthma associated with tuberculosis, assimilation of tuberculosis to witchcraft, radiological involvement of the pulmonary territories, serum creatinine ≥ 28 mg/L, HIV infection associated with TB. Associated with severe anemia for clinical concern, these factors allowed the development of the predictive score of death from TB. The ROC curve of the predictive score at death estimated the relevance of the predictive value of death with an area under the curve of 0.834 (0.755 – 0.912) (p < 0.001). The negative predictive value (NPV) of the predictive score for death during TB varied between 94.08% and 98.95%. This score is calculated on two groups of IFID. The 1st group is made up of socio-demographic factors. The 2nd group is made up of morbid situations requiring care in a specialized environment. Conclusion: The IFID imposes a management based on the use of the interrogation and the minimal radiological and biological assessment (the chest X-ray, the blood count, the dosage of creatinine and HIV serology). The decision tree-based death reduction strategy will contribute to better referral and management of patients.},
year = {2025}
}
TY - JOUR T1 - Predictive Factors of Mortality of Tuberculosis Patients Dead of Tuberculosis in Côte d'Ivoire AU - Amenan Kouamé AU - Kouadio Patrick Adon AU - Elodie Michelle Claudia Adombi AU - Jacquemin Kouakou Y1 - 2025/03/18 PY - 2025 N1 - https://doi.org/10.11648/j.wjph.20251001.17 DO - 10.11648/j.wjph.20251001.17 T2 - World Journal of Public Health JF - World Journal of Public Health JO - World Journal of Public Health SP - 61 EP - 76 PB - Science Publishing Group SN - 2637-6059 UR - https://doi.org/10.11648/j.wjph.20251001.17 AB - Introduction: study of the predictive factors of the deaths of tuberculosis patients to propose a decision tree for their best care in ambulatory TB centers. Methods: Prospective and observational survey, on a sample of 939 tuberculosis patients recruited in 30 CAT/CDT, carried out during supervision using collection tools such as survey forms and tuberculosis patient files. Results: 55 patients were notified dead. The mortality rate during tuberculosis was 5.9%. The Independent Factors Inducing Death (IFID) of TB were illiteracy, asthma associated with tuberculosis, assimilation of tuberculosis to witchcraft, radiological involvement of the pulmonary territories, serum creatinine ≥ 28 mg/L, HIV infection associated with TB. Associated with severe anemia for clinical concern, these factors allowed the development of the predictive score of death from TB. The ROC curve of the predictive score at death estimated the relevance of the predictive value of death with an area under the curve of 0.834 (0.755 – 0.912) (p < 0.001). The negative predictive value (NPV) of the predictive score for death during TB varied between 94.08% and 98.95%. This score is calculated on two groups of IFID. The 1st group is made up of socio-demographic factors. The 2nd group is made up of morbid situations requiring care in a specialized environment. Conclusion: The IFID imposes a management based on the use of the interrogation and the minimal radiological and biological assessment (the chest X-ray, the blood count, the dosage of creatinine and HIV serology). The decision tree-based death reduction strategy will contribute to better referral and management of patients. VL - 10 IS - 1 ER -
Service of Community Mobilization and Communication, National Tuberculosis Control Program (PNLT), Abidjan, Côte d’Ivoire
Biography: Amenan Kouame is a Doctor in Medicine & Health Economist. After a doctoral thesis in medicine (in 2000) at the University of Cocody (Côte d'Ivoire), she obtained a Master's degree in health economics at the African Center for Advanced Studies in Management (CESAG) in Dakar (Senegal) in 2004 and a Certificate of Specialized Studies in Infectious and Tropical Diseases. She is responsible for communication, community monitoring and operational researc, in charge of Operational Research & Study Officer at the National Tuberculosis Control Program (PNLT).
Research Fields: health management; health program; health financing; universal health coverage; chronic disease.
Department of Sociology, Félix Houphouët-Boigny University, Abidjan, Côte d’Ivoire
Biography: Kouadio Patrick Adon is Professor of Sociology at University Félix Houphouët-Boigny & member of the Technical Committee for Multi-Resistant Tuberculosis of the National Tuberclosis Control Program (PNLT). He defended a doctoral thesis (PhD) in sociology in 2006 after a Diploma of Advanced Specialized Studies (DESS) in Human Resources Engineering (2002) and a Master of Research (DEA) in sociology. He is a full professor of sociology at the Félix Houphouët-Boigny University where he was deputy director in charge of research at the Institute of Ethnosociology (2009-2010). He was also a senior consultant at UNFPA (2021) and an expert (2024) at the WHO office in Côte d'Ivoire.
Research Fields: health program evaluation, education for health, gender equity and rights; medical prevention, immunization, sexual and reproductive health, workforce health, disability, chronic diseases (cancers, tuberculosis, etc.).
Department of Anthropology and Sociology, Alassane Ouattara University, Bouaké, Côte d’Ivoire
Biography: Elodie Michelle Claudia Adombi is a Health Sociologist (PhD) and Lecturer at University Alassane Ouattara. Before this position, she is worked as a state-certified midwife. She holds a Master's degree in medical sociology and a state diploma in gyneco-obstetric sciences. She worked (2016-2024) as a state-certified midwife in the Abobo-est health district in Abidjan. In 2021, she defended a doctoral thesis (PhD) in medical sociology at the Félix Houphouët-Boigny University. She has been a teacher-researcher in health sociology since 2025.
Research Fields: sexual and reproductive health; maternal and child health; midwife; contraception; maternal deaths; nutrition, child and women diseases, midwife training.
Service of Coordination, National Tuberculosis Control Program (PNLT), Abidjan, Côte d’Ivoire
Biography: Jacquemin Kouakou is Doctor in Medicine & the Coordinating Director of the National Tuberculosis Control Program (PNLT), in Côte d’Ivoire. He holds a specialty degree in public health and epidemiology. He has proven expertise in infectious diseases within the framework of the Special Programme for Research and Training in Tropical Diseases (TDR) of the World Health Organization (WHO). For about fifteen years, he has held the position of Coordinating Director of the National Tuberculosis Control Programme (PNLT) in Côte d'Ivoire.
Research Fields: public health; health management; health program; medicines; health financing; universal health coverage; chronic disease.
Information