Objectives In Africa, profound social inequalities exist in access to oral health care, with one of the principal determinants being financial factors. To overcome this financial barrier, Senegal has implemented the Program for Support of Supply and Demand for Care (PAODES). Therefore, the aim of this study was to evaluate the impact of the program on improving access to oral health for affected people. Methods This study was conducted in the health districts of Sokone, the intervention site where PAODES was established, and Bambey, the control site where routine activities were maintained. A quasi-experimental study was conducted on 110 patients at each site who were consulted in oral health services. A questionnaire allowed us to collect sociodemographic data and data on the evaluation of intervention effects, including the renouncement of oral health and the cost of care. The relative risk (RR) and the attributable fraction (AF) were calculated. Results There was a significant difference of 13.6% at the intervention site compared to 39.1% at the control site (p=0.0001). The relative risk (RR) was 0.33 (0.19-0.57). The fraction attributable to the intervention was 33.42% (21.77-42.05) among the general population and 67.14% (43.52-80.89) among those who received the intervention. Conclusion The results of the study showed that a flat-rate pricing program aimed at reducing the financial burden on access to oral health care services had a positive impact. This demonstrated that a decrease in social inequalities regarding access to oral health can surpass financial barriers.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Social Inequality, Dental Care, Evaluation, Renunciation, Program
1. Introduction
In Africa, there are strong social health disparities and inequalities in access to oral health care. The underserved population is facing social barriers to accessing care, particularly financial barriers leading to the renunciation of care or the risk of household impoverishment
[1]
Ajayi DM, Arigbede AO. Barriers to oral health care utilization in Ibadan, South West Nigeria. Afr Health Sci. 2012; 12(4): 507‑13.
Dieng SN, Kanouté A, Azogui-Levy S, Lombrail P. Determinants of maternal and household social inequalities of dental caries among Senegalese children in the Department of Pikine. Pan Afr Med J. 2023; 44: 23.
Onyejaka NK, Folayan MO, Folaranmi N. Barriers and facilitators of dental service utilization by children aged 8 to 11 years in Enugu State, Nigeria. BMC Health Serv Res. 2016; 16: 93.
. The World Health Organization (WHO) estimated that 1.4 to 1.9 billion individuals were affected by financial difficulties in 2017. Low-income countries account for 33.4% of the population who fall into or further sink into relative poverty due to out-of-pocket health expenses
[4]
Organization mondiale de la santé. Rapport mondial de suivi sur la protection financière en santé 2021 [Global monitoring report on financial protection in health 2021]. Genève: OMS/BM; 2022. 128p. Report No.: CC BY-NC-SA 3.0 IGO.
[4]
. Dental care presents among the highest levels of financial barriers compared to other healthcare services
[5]
Vujicic M, Buchmueller T, Klein R. Dental Care Presents The Highest Level Of Financial Barriers, Compared To Other Types Of Health Care Services. Health Aff (Millwood). 2016; 35(12): 2176‑82.
. They are expensive and underfunded. In fact, nearly 70% of sub-Saharan African countries allocated less than one dollar per person per year to dental care in 2019
[6]
Organization mondiale de la santé – Région Afrique. L’Afrique est confrontée à la plus forte hausse des maladies bucco-dentaires dans le monde. [cité 17 janv 2024]. Disponible sur:
. To protect populations from financial risk, the principle of prepayment through pooling resources and abolishing direct payment for care has been instituted in several countries
[7]
Ridde V, Meessen B, Kouanda S. L’abolition sélective du paiement direct en Afrique subsaharienne : une opportunité pour le renforcement des systèmes de santé ? Santé Publique. 2011; 23(1): 61‑7.
[7]
. Health insurance schemes or programs are developed to facilitate better access to dental care for populations. In Rwanda, members of health insurance schemes visit health services 4 to 8 times more often than nonmembers do
[8]
Alenda J, Boidin B. L’extension de l’assurance-maladie au Sénégal : avancées et obstacles. Médecine Santé Trop. 2012; 22(4): 364‑9.
. In Kano State, Nigeria, the Idon et al. study in 2021 supported that 87% of insured patients preferred endodontic treatment, even if it is more expensive, over tooth extraction compared to uninsured individuals
[9]
Idon PI, Sotunde OA, Ogundare TO, Yusuf J, Makanjuola JO, Mohammed A, et al. Access to root canal treatment in a Nigerian subpopulation: assessment of the effect of dental health insurance. Afr Health Sci. 2021; 21(1): 470‑7.
. In Senegal, to overcome the financial barrier to accessing care, the Ministry of Health, with the support of the Belgian Technical Cooperation, is implementing the Program for Support of Supply and Demand for Care (PAODES). It is a financing program integrated into a healthcare coverage strategy aimed at sustainably and comprehensively strengthening the healthcare sector in Senegal, particularly in the five targeted medical regions (Diourbel, Kaffrine, Kaolack, Fatick, and Thiès). PAODES applies subsidized flat-rate pricing at the level of the health district in these regions
[10]
Ministère de la Santé et de l’Action Sociale. Dossier Technique et Financier du Programme d’Appui à l’Offre et à la Demande de soins (PAODES). 2011.
[10]
. However, dental care is only integrated into the package offered in the municipalities of Sokone and Koungueul. Thus, the objective of this work was to evaluate the impact of the PAODES intervention on improving accessibility to dental care for affected populations.
2. Method
2.1. Study Design
The study was conducted in the health districts of Sokone and Bambey. Sokone is a commune with a population of 14745 inhabitants situated in the region of Fatick, in the center-west of Senegal. In terms of health, Sokone has a health district of the same name covering 17 health centers. Bambey has a population of 28908 individuals in the region of Diourbel in the center of Senegal. It has a health district with the same name and encompasses 25 health centers. In both communes, the primary economic activity consists mainly of subsistence agriculture and trade. In its report on poverty in Senegal in 2019, the National Agency of Statistics and Demographics (NASD) estimated an incidence rate of 43.9 in the region of Diourbel where Bambey is located and 49.2 in the region of Fatick where Sokone is located
[11]
Agence Nationale de la Statistique et de la Démographie. Enquête harmonisée sur les conditions de Vie des Ménages (EHCVM) au Sénégal. Dakar: ANSD; 2021. 181p.
[11]
.
2.2. Study Population
A quasi-experimental study was conducted. The study population consisted of all individuals who visited the oral care services of both health districts, agreed to participate in the study, and whose health conditions allowed for data collection.
2.3. Sampling and Sample Size
Stratified sampling based on age and sex was chosen with proportional allocation to the weight of the age and sex categories for both the intervention and control districts. To determine the sample size for each group, the following formula was used:ni=nt=2P(1-P)(Zα+Z2β)2/(Pi-Pt)2; n= number of individuals in each group (ni= intervention and nt=control); Zα=1.96 when alpha is 5%; power=80% is equal to Z2β=0.84; theoretical dropout=50% for the control site; and an odd-ratio (OR)=0.4 is expected. Thus, the sample size in each group was 106 participants. An increase of 5% allowed us to reach a sample size of 111 participants per site, rounded to 110 per site. As a result, the total sample size was 220 participants, with 110 patients per site.
2.4. Intervention and Control Sites
Two sites were chosen: oral care services in Sokone’s health district as the intervention site and those located in Bambey as the control site. At the intervention site, the PAODES program was established considering the cost of care of patients at the health centers following subsidized flat-rate pricing. It is a fixed rate that includes all aspects of treating the illness episode and covers 100% of the costs of dental care, 99% of medications, and 22% of additional examinations. At the control site, routine dental care activities were studied.
2.5. Study Variables
Two types of variables were defined in this study: sociodemographic variables and those linked to access to care. The sociodemographic variables included age, sex, employment, capacity to pay for care services, and the impact of dropout and appreciation of the cost of care. Sex is a binary variable (male, female), and age is defined in years old and categorized into four groups: 18 years old and less, 19-35 years old, 36-60 years old, and 60 years old and plus. The employment sector of activity is defined by four modalities: informal sector, formal sector, individuals in training, unemployed, and others. The ability to pay for care is a dichotomous variable (yes, no) in response to the following question: Can you afford to pay for your dental care?
Variables related to access to care are composed of the renunciation of care and the impression of the affordability of care. Renunciation of care was the dependent variable dichotomized as yes/no. It is defined as abstaining from seeking care, for specific reasons, when needed. Negative responses at the intervention site are considered indicative of a positive impact of the intervention. The assessment of the cost of dental care is another criterion for evaluating the program's impact. It refers to the patient's impression of the affordability of care and medication. This variable had three modalities: very expensive, expensive, and affordable. Impressions of affordable care costs are considered to reflect a positive impact of the intervention.
2.6. Data Collection
The data were collected by a soon-to-graduate student who was trained and calibrated to complete the survey. A structured questionnaire enabled them to collect data on the defined variables. Data collection was performed between September 2016 and April 2017.
2.7. Analysis Plan
The collected data were entered into Excel and analyzed using SPSS version 19 software. The results are presented with a 5% alpha error risk. The percentages of the variables in both groups were compared using the chi-square test at a significance threshold of p lower than 0.05. The relative risk (RR) and the attributable preventive fraction (APF) due to the intervention were calculated.
2.8. Ethical Consideration
Facilitating informed consent was systematically obtained from the participants. The confidentiality of the data was strictly monitored. This study was approved by the ethical committee of the faculty of medicine.
3. Results
3.1. Sociodemographic Characteristics
The study population consisted predominantly of females (57.3%) at both the intervention and control sites. The mean age was 23.3±17.8 years at the intervention site and 23.6±17.8 years at the control site. The age categories of 6-18 years old and 19-35 years old represented approximately 80% of the sample at each site, with 83.7% at the intervention site and 78.2% at the control site. Over half of the population was inactive or in training at the intervention (53.6%) and control (51.8%) sites; the informal sector represented 12% at the intervention site and 29% at the control site. Eighty percent of the sample at the intervention site reported being able to afford the cost of care, compared to 77.3% at the control site (Table 1).
Table 1. Sample characteristics.
Variables N=110
Intervention N (%)
Control N (%)
Sex
Female
63 (57.3%)
63 (57.3%)
Male
47 (42.7%)
47 (42.7%)
Age group
≤ 18 years old
54 (49.1%)
56 (50.9%)
19 – 35 years old
38 (34.6%)
30 (27.3%)
36 – 60 years old
12 (10.9%)
18 (16.4%)
> 60 years old
6 (5.4%)
6 (5.4%)
Employment
Formal
4 (3.6%)
8 (7.3%)
Informal
14 (12.7%)
32 (29.1%)
Inactive
59 (53.6%)
57 (51.8%)
Others
33 (30.1%)
13 (11.8%)
Capacity to pay for care services
Yes
88 (80%)
85 (77.3%)
No
22 (20%)
25 (22.7%)
3.2. Impact of the Intervention
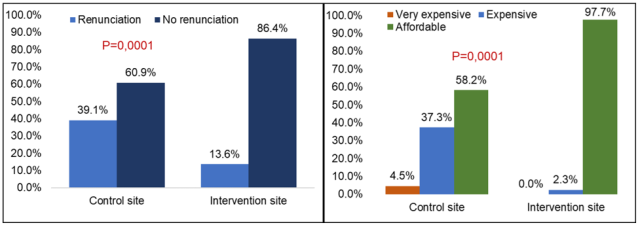
At the site covered by the program, only 13.6% of the population had renounced care compared to 39.1% at the control site, which was a statistically significant difference (p=0.0001) (Figure 1).
Table 2. Program impact measurements.
Renunciation
Yes
No
RR (IC95%)
PFA (IC95%)
Intervention site
14 (13.6%)
95 (86.4%)
0.33(19.11- 56.48)
67.14(43.52-80.89)
Control site
43 (39.1%)
67 (60.9%)
The relative risk (RR) was 0.33 (0.19-0.57). The percentage of preventive fraction attributable (PFA) to the intervention was estimated to be 33.42% (21.77-42.05) in the general population and 67.14% (43.52-80.89) in the intervention beneficiaries (Table 2). The results also showed that 97.7% of patients considered the overall cost of care to be affordable at the intervention site compared to 58.2% at the control site, which was a statistically significant difference (p=0.0001) (Figure 1).
Figure 1. Comparison between the two groups in terms of renunciation and appreciation of the cost of care.
4. Discussion
The collected data are both internally valid and external. The internal validity of this study was ensured through a rigorous methodological approach. The data were collected by a calibrated investigator with a certain understanding of the sociocultural context of the populations under investigation. The surveys were conducted face-to-face with the patient or their guardian (for minors), allowing for reformulations or follow-ups to obtain precise answers and thus reducing the risk of social desirability bias. Additionally, the choice of comparison sites was based on the similarity of their social and demographic contexts. These sites are located in the central and central-western regions of the country, with predominantly rural and young populations. The generalization of the results (external validity) is possible to all health districts in the central and central-western regions of the country that will have benefited from a program similar to PAODES.
The evaluation of the PAODES program revealed a positive impact on the population of beneficiaries. Indeed, the relative risk is protective against the renunciation of care, and the fraction of non-renunciation of dental care attributable to the program is high. The percentage of renunciation at the intervention site was significantly lower than that at the control site. Compared with those at the control site, the program beneficiaries considered the proposed care to be affordable. The program has led to a decrease in the renunciation rate of care because of its action in favor of reducing financial barriers to the use of healthcare services. In 2018, Pegon-Macht et al. suggested that in the context of financial uncertainty, vulnerable patients renounce dental care even before entering the healthcare system
[12]
Pegon-Machat E, Jourdan D, Tubert-Jeannin S. Inégalités en santé orale : déterminants de l’accès à la prévention et aux soins en France. Santé Publique. 2018; 30(2): 243‑51.
[12]
. Financial factors thus explain inequalities in the use or renunciation of dental care, as supported by previous studies
[13]
De Rubeis V, Jiang Y, de Groh M, Dufour L, Bronsard A, Morrison H, et al. Barriers to oral care: a cross-sectional analysis of the Canadian longitudinal study on aging (CLSA). BMC Oral Health. 2023; 23: 294.
Blasi PR, Krakauer C, Anderson ML, Nelson J, Bush T, Catz SL, et al. Factors associated with future dental care utilization among low-income smokers overdue for dental visits. BMC Oral Health. 2018; 18(1): 183.
. In France, even though 70% of health insurance covers some procedures, out-of-pocket expenses and/or fees are problematic, especially for patients without supplementary insurance, resulting in care renunciation behaviors
[12]
Pegon-Machat E, Jourdan D, Tubert-Jeannin S. Inégalités en santé orale : déterminants de l’accès à la prévention et aux soins en France. Santé Publique. 2018; 30(2): 243‑51.
[15]
Sass C, Runfola S. Rapport sur le renoncement aux soins des bénéficiaires de la CMU-c : Enquête dans les CES de l’Assurance maladie. Paris; 2011. 46p.
[12, 15]
. A systematic review of studies on health insurance policy and dental care in Australia conducted in 2018 revealed that all publications concluded that the use of preventive and curative care services was systematically significantly associated with being insured
[16]
Gnanamanickam E, Teusner D, Arrow P, Brennan D. Dental insurance, service use and health outcomes in Australia: a systematic review. Aust Dent J. 2018; 63(1): 4‑13.
. A recent study in the United States in Washington state examining the relationship between health insurance and the use of preventive dental care among students showed that students with private health insurance were 3.9 times more likely to receive preventive care than students without health insurance
[17]
Hill CM, Kerr D, Chi DL. Health insurance is associated with dental care use among university students in Washington State. BMC Oral Health. 2023; 23(1): 26.
. These studies, like ours, demonstrate that prepayment policies significantly contribute to increasing the utilization rate and non-renunciation of dental care.
The impact of health programs can also be measured based on patients' perceptions of the costs of care. At the intervention site, 97.7% of patients believed that the costs of care were affordable, compared to 58.2% at the control site. These results suggest that patients' perceptions of the sustainability of dental care costs were significantly more favorable at the intervention site than at the control site. In a qualitative study in Ibadan, Nigeria, Osuh et al. reported that participants believed that dental care costs were generally unaffordable in the area and constituted a barrier to seeking care
[18]
Osuh ME, Oke GA, Lilford RJ, Osuh JI, Lawal FB, Gbadebo SO, et al. Oral health in an urban slum, Nigeria: residents’ perceptions, practices and care-seeking experiences. BMC Oral Health. 2023; 23(1): 657.
. In conclusion, inequalities in the use or renunciation of care have social, particularly financial, determinism. PAODES is an example, in this context, of a policy favoring the reduction of these inequalities.
These results have clear implications for public health policies in Senegal and beyond, in countries with scarce resources. In many sub-Saharan African countries, characterised by a fragile economy and low purchasing power, many people are pushed into poverty by health costs. Pre-payment policies for health care need to be strengthened in order to achieve a coverage rate that will facilitate access to care for the needy.
5. Conclusion
The results of the study showed that a flat-rate pricing program aimed at reducing the financial burden of the renunciation of oral care services has a positive impact. This demonstrates that a decrease in social disparities in access to oral health care can be achieved through action on financial barriers. Thus, in low-resources countries such as Senegal, several policy options can be considered in this regard. This may be to expand oral health coverage, ensuring that it can provide improved financial protection. Subsidizing the costs of care or exploring options other than curative care are urgently needed. Specifically, it involves developing programs for promoting oral health. In addition, it would be interesting to set up longitudinal studies on the impact of the current health coverage policy in Senegal on the renunciation of oral health care, particularly in rural areas. It is also likely that there is a sociological or sociocultural determinism to the renunciation of oral health care, which a qualitative study would help to better understand.
Dieng SN, Kanouté A, Azogui-Levy S, Lombrail P. Determinants of maternal and household social inequalities of dental caries among Senegalese children in the Department of Pikine. Pan Afr Med J. 2023; 44: 23.
Onyejaka NK, Folayan MO, Folaranmi N. Barriers and facilitators of dental service utilization by children aged 8 to 11 years in Enugu State, Nigeria. BMC Health Serv Res. 2016; 16: 93.
Organization mondiale de la santé. Rapport mondial de suivi sur la protection financière en santé 2021 [Global monitoring report on financial protection in health 2021]. Genève: OMS/BM; 2022. 128p. Report No.: CC BY-NC-SA 3.0 IGO.
[5]
Vujicic M, Buchmueller T, Klein R. Dental Care Presents The Highest Level Of Financial Barriers, Compared To Other Types Of Health Care Services. Health Aff (Millwood). 2016; 35(12): 2176‑82.
Organization mondiale de la santé – Région Afrique. L’Afrique est confrontée à la plus forte hausse des maladies bucco-dentaires dans le monde. [cité 17 janv 2024]. Disponible sur:
Ridde V, Meessen B, Kouanda S. L’abolition sélective du paiement direct en Afrique subsaharienne : une opportunité pour le renforcement des systèmes de santé ? Santé Publique. 2011; 23(1): 61‑7.
[8]
Alenda J, Boidin B. L’extension de l’assurance-maladie au Sénégal : avancées et obstacles. Médecine Santé Trop. 2012; 22(4): 364‑9.
Idon PI, Sotunde OA, Ogundare TO, Yusuf J, Makanjuola JO, Mohammed A, et al. Access to root canal treatment in a Nigerian subpopulation: assessment of the effect of dental health insurance. Afr Health Sci. 2021; 21(1): 470‑7.
Ministère de la Santé et de l’Action Sociale. Dossier Technique et Financier du Programme d’Appui à l’Offre et à la Demande de soins (PAODES). 2011.
[11]
Agence Nationale de la Statistique et de la Démographie. Enquête harmonisée sur les conditions de Vie des Ménages (EHCVM) au Sénégal. Dakar: ANSD; 2021. 181p.
[12]
Pegon-Machat E, Jourdan D, Tubert-Jeannin S. Inégalités en santé orale : déterminants de l’accès à la prévention et aux soins en France. Santé Publique. 2018; 30(2): 243‑51.
[13]
De Rubeis V, Jiang Y, de Groh M, Dufour L, Bronsard A, Morrison H, et al. Barriers to oral care: a cross-sectional analysis of the Canadian longitudinal study on aging (CLSA). BMC Oral Health. 2023; 23: 294.
Blasi PR, Krakauer C, Anderson ML, Nelson J, Bush T, Catz SL, et al. Factors associated with future dental care utilization among low-income smokers overdue for dental visits. BMC Oral Health. 2018; 18(1): 183.
Sass C, Runfola S. Rapport sur le renoncement aux soins des bénéficiaires de la CMU-c : Enquête dans les CES de l’Assurance maladie. Paris; 2011. 46p.
[16]
Gnanamanickam E, Teusner D, Arrow P, Brennan D. Dental insurance, service use and health outcomes in Australia: a systematic review. Aust Dent J. 2018; 63(1): 4‑13.
Hill CM, Kerr D, Chi DL. Health insurance is associated with dental care use among university students in Washington State. BMC Oral Health. 2023; 23(1): 26.
Osuh ME, Oke GA, Lilford RJ, Osuh JI, Lawal FB, Gbadebo SO, et al. Oral health in an urban slum, Nigeria: residents’ perceptions, practices and care-seeking experiences. BMC Oral Health. 2023; 23(1): 657.
Dieng, S. N., Dieng, A., Diallo, A., Diop, M., Kanouté, A., et al. (2025). Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level. World Journal of Public Health, 10(1), 13-18. https://doi.org/10.11648/j.wjph.20251001.12
Dieng, S. N.; Dieng, A.; Diallo, A.; Diop, M.; Kanouté, A., et al. Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level. World J. Public Health2025, 10(1), 13-18. doi: 10.11648/j.wjph.20251001.12
Dieng SN, Dieng A, Diallo A, Diop M, Kanouté A, et al. Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level. World J Public Health. 2025;10(1):13-18. doi: 10.11648/j.wjph.20251001.12
@article{10.11648/j.wjph.20251001.12,
author = {Serigne Ndame Dieng and Amadou Dieng and Alimatou Diallo and Mbathio Diop and Aïda Kanouté and Massamba Diouf},
title = {Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level},
journal = {World Journal of Public Health},
volume = {10},
number = {1},
pages = {13-18},
doi = {10.11648/j.wjph.20251001.12},
url = {https://doi.org/10.11648/j.wjph.20251001.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251001.12},
abstract = {Objectives In Africa, profound social inequalities exist in access to oral health care, with one of the principal determinants being financial factors. To overcome this financial barrier, Senegal has implemented the Program for Support of Supply and Demand for Care (PAODES). Therefore, the aim of this study was to evaluate the impact of the program on improving access to oral health for affected people. Methods This study was conducted in the health districts of Sokone, the intervention site where PAODES was established, and Bambey, the control site where routine activities were maintained. A quasi-experimental study was conducted on 110 patients at each site who were consulted in oral health services. A questionnaire allowed us to collect sociodemographic data and data on the evaluation of intervention effects, including the renouncement of oral health and the cost of care. The relative risk (RR) and the attributable fraction (AF) were calculated. Results There was a significant difference of 13.6% at the intervention site compared to 39.1% at the control site (p=0.0001). The relative risk (RR) was 0.33 (0.19-0.57). The fraction attributable to the intervention was 33.42% (21.77-42.05) among the general population and 67.14% (43.52-80.89) among those who received the intervention. Conclusion The results of the study showed that a flat-rate pricing program aimed at reducing the financial burden on access to oral health care services had a positive impact. This demonstrated that a decrease in social inequalities regarding access to oral health can surpass financial barriers.},
year = {2025}
}
TY - JOUR
T1 - Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level
AU - Serigne Ndame Dieng
AU - Amadou Dieng
AU - Alimatou Diallo
AU - Mbathio Diop
AU - Aïda Kanouté
AU - Massamba Diouf
Y1 - 2025/01/14
PY - 2025
N1 - https://doi.org/10.11648/j.wjph.20251001.12
DO - 10.11648/j.wjph.20251001.12
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 13
EP - 18
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20251001.12
AB - Objectives In Africa, profound social inequalities exist in access to oral health care, with one of the principal determinants being financial factors. To overcome this financial barrier, Senegal has implemented the Program for Support of Supply and Demand for Care (PAODES). Therefore, the aim of this study was to evaluate the impact of the program on improving access to oral health for affected people. Methods This study was conducted in the health districts of Sokone, the intervention site where PAODES was established, and Bambey, the control site where routine activities were maintained. A quasi-experimental study was conducted on 110 patients at each site who were consulted in oral health services. A questionnaire allowed us to collect sociodemographic data and data on the evaluation of intervention effects, including the renouncement of oral health and the cost of care. The relative risk (RR) and the attributable fraction (AF) were calculated. Results There was a significant difference of 13.6% at the intervention site compared to 39.1% at the control site (p=0.0001). The relative risk (RR) was 0.33 (0.19-0.57). The fraction attributable to the intervention was 33.42% (21.77-42.05) among the general population and 67.14% (43.52-80.89) among those who received the intervention. Conclusion The results of the study showed that a flat-rate pricing program aimed at reducing the financial burden on access to oral health care services had a positive impact. This demonstrated that a decrease in social inequalities regarding access to oral health can surpass financial barriers.
VL - 10
IS - 1
ER -
Dieng, S. N., Dieng, A., Diallo, A., Diop, M., Kanouté, A., et al. (2025). Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level. World Journal of Public Health, 10(1), 13-18. https://doi.org/10.11648/j.wjph.20251001.12
Dieng, S. N.; Dieng, A.; Diallo, A.; Diop, M.; Kanouté, A., et al. Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level. World J. Public Health2025, 10(1), 13-18. doi: 10.11648/j.wjph.20251001.12
Dieng SN, Dieng A, Diallo A, Diop M, Kanouté A, et al. Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level. World J Public Health. 2025;10(1):13-18. doi: 10.11648/j.wjph.20251001.12
@article{10.11648/j.wjph.20251001.12,
author = {Serigne Ndame Dieng and Amadou Dieng and Alimatou Diallo and Mbathio Diop and Aïda Kanouté and Massamba Diouf},
title = {Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level},
journal = {World Journal of Public Health},
volume = {10},
number = {1},
pages = {13-18},
doi = {10.11648/j.wjph.20251001.12},
url = {https://doi.org/10.11648/j.wjph.20251001.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjph.20251001.12},
abstract = {Objectives In Africa, profound social inequalities exist in access to oral health care, with one of the principal determinants being financial factors. To overcome this financial barrier, Senegal has implemented the Program for Support of Supply and Demand for Care (PAODES). Therefore, the aim of this study was to evaluate the impact of the program on improving access to oral health for affected people. Methods This study was conducted in the health districts of Sokone, the intervention site where PAODES was established, and Bambey, the control site where routine activities were maintained. A quasi-experimental study was conducted on 110 patients at each site who were consulted in oral health services. A questionnaire allowed us to collect sociodemographic data and data on the evaluation of intervention effects, including the renouncement of oral health and the cost of care. The relative risk (RR) and the attributable fraction (AF) were calculated. Results There was a significant difference of 13.6% at the intervention site compared to 39.1% at the control site (p=0.0001). The relative risk (RR) was 0.33 (0.19-0.57). The fraction attributable to the intervention was 33.42% (21.77-42.05) among the general population and 67.14% (43.52-80.89) among those who received the intervention. Conclusion The results of the study showed that a flat-rate pricing program aimed at reducing the financial burden on access to oral health care services had a positive impact. This demonstrated that a decrease in social inequalities regarding access to oral health can surpass financial barriers.},
year = {2025}
}
TY - JOUR
T1 - Reducing Social Inequalities in Access to Dental Care in Senegal: Evaluation of a Flat-Rate Pricing Program at the Health District Level
AU - Serigne Ndame Dieng
AU - Amadou Dieng
AU - Alimatou Diallo
AU - Mbathio Diop
AU - Aïda Kanouté
AU - Massamba Diouf
Y1 - 2025/01/14
PY - 2025
N1 - https://doi.org/10.11648/j.wjph.20251001.12
DO - 10.11648/j.wjph.20251001.12
T2 - World Journal of Public Health
JF - World Journal of Public Health
JO - World Journal of Public Health
SP - 13
EP - 18
PB - Science Publishing Group
SN - 2637-6059
UR - https://doi.org/10.11648/j.wjph.20251001.12
AB - Objectives In Africa, profound social inequalities exist in access to oral health care, with one of the principal determinants being financial factors. To overcome this financial barrier, Senegal has implemented the Program for Support of Supply and Demand for Care (PAODES). Therefore, the aim of this study was to evaluate the impact of the program on improving access to oral health for affected people. Methods This study was conducted in the health districts of Sokone, the intervention site where PAODES was established, and Bambey, the control site where routine activities were maintained. A quasi-experimental study was conducted on 110 patients at each site who were consulted in oral health services. A questionnaire allowed us to collect sociodemographic data and data on the evaluation of intervention effects, including the renouncement of oral health and the cost of care. The relative risk (RR) and the attributable fraction (AF) were calculated. Results There was a significant difference of 13.6% at the intervention site compared to 39.1% at the control site (p=0.0001). The relative risk (RR) was 0.33 (0.19-0.57). The fraction attributable to the intervention was 33.42% (21.77-42.05) among the general population and 67.14% (43.52-80.89) among those who received the intervention. Conclusion The results of the study showed that a flat-rate pricing program aimed at reducing the financial burden on access to oral health care services had a positive impact. This demonstrated that a decrease in social inequalities regarding access to oral health can surpass financial barriers.
VL - 10
IS - 1
ER -