Trigeminal neuralgia (TN) is a debilitating neurological disorder characterized by sudden, severe facial pain along the distribution of the trigeminal nerve. It may significantly affect a patient’s quality of life. Stereotactic radiosurgery (SRS) is a non-invasive therapeutic option for managing TN, providing targeted precision and minimal side effects. The long-term benefits of SRS are noteworthy, as pain relief often persists for several years after the procedure. The authors aim to present a rare case of a reirradiation of a recurrent trigeminal neuralgia case. This is a case of a 74-year-old female who has had symptoms of TN for more than twenty years before undergoing gamma-knife SRS in 2017 with a dose of 90 Gray (Gy). Post SRS had good pain control for the next five years until in 2022 when she had increasing intensity of the pain no longer tolerable by medications. She was then treated in our institution using a linac-based SRS for a dose of 70 Gy. Post-second SRS, she reported no recurrence of severe pain. Twelve month follow-up noted no recurrence of severe pain with good quality of life and the only complication is unilateral left facial numbness. Repeat radiation with stereotactic radiosurgery with different techniques is feasible in refractory case of trigeminal neuralgia.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Stereotactic Radiosurgery, Trigeminal Neuralgia, Reirradiation, Case Report
1. Introduction
Trigeminal neuralgia is disorder characterized by recurrent unilateral brief pains resembling electric shocks, abrupt in onset and termination, confined to the distribution of one or more divisions of the trigeminal nerve, and provoked by innocuous stimuli. It may develop without apparent cause or as a consequence of another disorder
[1]
Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018; 38(1): 1-211.
. The condition can significantly diminish patients' quality of life, making effective treatment essential. It was initially described by Nicolas André in 1756 and he coined the term "tic douloureux" due to the nature of the pain as short intermittent painful tics. He believed that facial sensory peripheral nerve compression was the cause of the pain
[2]
Brown JA, Coursaget C, Preul MC, Sangvai D. Mercury water and cauterizing stones: Nicolas André and tic douloureux. J Neurosurg. 1999; 90(5): 977-981.
. Gamma-knife SRS has been the most popular method of radiosurgery for TN since it was first used by Leksell in 1951
[3]
Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. 1951; 102(4): 316-319.
[3]
. However, recent advances in techniques have paved the way for linac-based SRS to be an alternative method for treatment due in part to the use of cones which can mimic the pencil-beam approach of gamma-knife. Most articles on radiosurgery, however, are limited to retrospective studies thus prospective studies are warranted to ascertain long-term follow up and prognostic factors following treatment.
2. Case Presentation
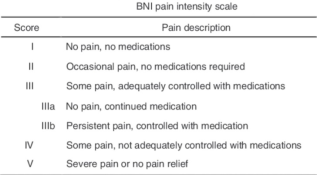
This is a case of a 76-year-old female, widowed, Filipino, housewife from Sta. Rosa, who is hypertensive, controlled, and non-diabetic diagnosed with classical TN for more than 20 years, who underwent Gamma Knife stereotactic radiosurgery (GKSR) in 2017. The patient has been experiencing intermittent left facial pain, lasting from seconds to minutes and spontaneously abating, allegedly for more than 20 years now. The patient is maintained on carbamazepine 100 mg daily and had been to different physicians during the 20 years. She was also not very compliant with her intake. Her Barrow Neurological Institute (BNI) pain intensity score ranged from II-IV.
In 2017, due to persistence and increase in severity of the pain now with a BNI V, patient was advised surgical intervention with microvascular decompression however patient refused any invasive procedure. As such, patient underwent one session of GKSR with a dose of 90 Gy delivered to the isocenter with 45 Gy to the 50% isodose line using a Leksell Gamma Knife PERFEXION. Dose to the brainstem was kept below the maximum dose of 16 Gy with 0% of the volume receiving more than 10 Gy. Post treatment was unremarkable however patient was lost to follow up. Patient was allegedly pain free for the next 2-3 years still with the maintenance carbamazepine now increased to 200 mg daily, achieving a BNI of I-II to which the patient stopped taking her medication.
There was a gradual resurgence of pain achieving a highest BNI of IIIb. The patient then resumed her intake of carbamazepine at 100 mg daily in late December 2021. Three months thereafter, the pain has been increasing in frequency and intensity (up to a pain score of 10/10) for which she sought consult at our institution. She had a consult at ambulatory care and she was started on carbamazepine 200 mg twice daily and gabapentin. The patient was given options of surgery or repeat SRS; hence the patient was referred to our service.
Figure 1. Barrow Neurological Institute pain intensity scale for Trigeminal Neuralgia.
The patient underwent a cranial magnetic resonance imaging (MRI) with intravenous contrast the day prior to admission. The patient was scheduled for linac-based SRS with a dose of 70 Gy to the isocenter (56 Gy to the 80% isodose line) the following day. The patient was then discharged one day after with no complications.
2.1. Radiation Therapy Planning and Treatment
Prior to radiation therapy planning, the patient underwent a high-resolution MRI scan consisting of 1 mm thin slices with T1-weighted, T2-weighted contrast enhanced sequences with emphasis on the cerebello-pontine angle regions using 1.5 Tesla unit in multiplanar views. On the day of treatment, an experienced neurosurgeon placed and secured a BrainLAB stereotactic frame on the patient’s head after application of a local anesthetic. The patient was then set up for the planning computed tomography (CT) simulation which was performed on a 16 slice Phillips Brilliance Big Bore CT scanner and BrainLAB CT localizer. CT simulation images were acquired with pixel size of 1.1719 mm at 1 mm slice thickness and 1 mm slice spacing following departmental SRS scanning protocol.
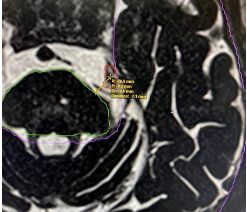
After CT simulation, the MRI was co-registered with the planning CT images and an experienced radiation oncologist and neurosurgeon contoured the trigeminal nerve root ganglion for isocenter placement. The target was localized to the base of the trigeminal nerve root at the left of the pons. Organs at risk (OAR) were then delineated such as the brainstem, optic chiasm, bilateral optic nerves, bilateral eyes, and the normal brain parenchyma.
Figure 2. The left trigeminal nerve root ganglion contoured on MRI (red), brainstem (green), normal brain parenchyma (purple).
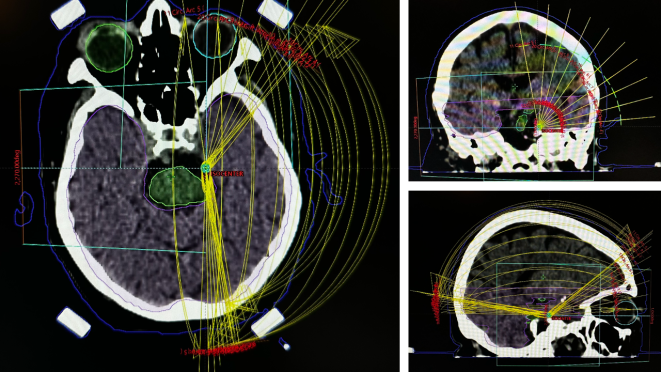
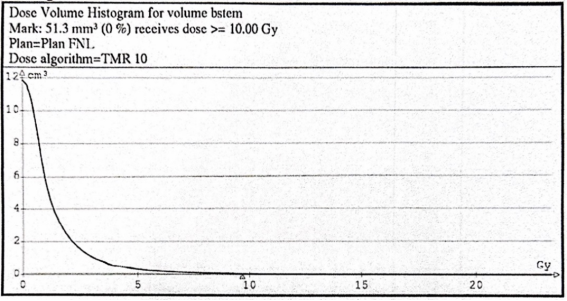
The treatment planning consisted of using a ten-arc plan in iPlan BrainLAB to deliver the single fraction prescription dose of 70 Gy to the isocenter (56 Gy to the 80% isodose line) using 6 megavoltage photn beams with a dose-rate of 600 MU/min and a 4 mm diameter cone size using a Varian iX linear accelerator. Optimization for critical organ structures were done to minimize unwanted doses to OARs specifically the brainstem to achieve a cumulative maximum point dose of less than 16 Gy considering the patient already had a prior SRS in 2017. Actual brainstem dose from the Gamma-knife SRS was not readily available however a dose-volume histogram (DVH) was provided which showed that 0% of the volume of brainstem received no more than 10 Gy.
Figure 4. Dose-volume histogram of the brainstem from the first treatment using Gamma-knife SRS in 2017.
A dose-volume histogram (DVH) was then generated in the iPlan BrainLAB treatment planning system and subsequently evaluated by a radiation oncologist, neurosurgeon, and a medical physicist to ensure quality of the plan.
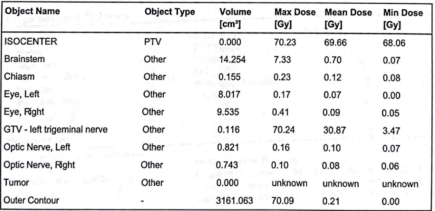
Figure 5. Dose-volume characteristics of the target isocenter and the OARs.
Prior to treatment delivery, kilo-voltage x-ray images were taken to verify stereotactic frame placement, head position, and isocenter localization. This was repeated on a per-arc basis to ensure accuracy and precision of treatment delivery. The treatment was completed with no complications.
2.2. Follow-up
Immediately post SRS, the patient had no grimacing from the pain and was clinically stable. Patient was able to go home after an observation period of two hours. One week post treatment patient had no recurrence of BNI score of IV-V. No other associated symptoms such as facial numbness noted at this time. Six months post-treatment, patient had BNI score of III with intermittent mild facial numbness on the left maxillary and mandibular area with intact motor function. One-year post-treatment, patient had stable BNI score of II-III now with facial numbness on the left side still with intact motor function. Patient is generally relieved that there has been no recurrence of BNI score of IV-V since SRS treatment and is having a better quality of life.
3. Discussion
In 2005, Burchiel et al described a classification that characterizes TN according to its symptomatology whether the cause was idiopathic, trigeminal injury, associated with multiple sclerosis, resulting from an outbreak of facial herpes zoster, or a somatoform pain disorder. For the purposes of this review, we will only be discussing the idiopathic type, of which there are two. Type 1, usually referred to as classical or typical TN is described as an idiopathic sharp, shooting, electrical-like, episodic pain lasting several seconds, with pain-free intervals between attacks. In contrast, type 2 TN describes idiopathic trigeminal facial pain that is aching, throbbing, or burning for more than 50% of the time and is constant in nature (constant background pain being the most significant attribute)
[4]
Eller JL, Raslan AM, Burchiel KJ. Trigeminal neuralgia: definition and classification. Neurosurg Focus. 2005; 18(5): 1-3.
There is still no consensus on the exact pathologic mechanism for TN however, majority of cases can be related to neurovascular etiologies such as compression of the trigeminal nerve particularly near the dorsal root entry which is seen in more than 80% of type 1 TN which would explain why microvascular decompression is that surgical treatment modality for TN
[5]
Marchetti M, Pinzi V, De Martin E, Ghielmetti F, Fariselli L. Radiosurgery for trigeminal neuralgia: the state of art. Neurol Sci. 2019; 40(S1): 153-157.
Pharmacological treatment with carbamazepine or oxcarbazepine is the initial treatment of choice for the majority of patients with classic TN. Surgical intervention such as rhizotomy or microvascular decompression is reserved for patients who are resistant to medical treatment. Stereotactic radiosurgery is an alternative as a non-invasive procedure that uses high-energy radiation to target specific areas in the brain, and it has been shown to be effective in the management of TN since being first described by Leksell in 1951
[3]
Leksell L. The stereotaxic method and radiosurgery of the brain. Acta Chir Scand. 1951; 102(4): 316-319.
[3]
. A systematic review done by Rheaume et al found that while approximately half of TN patients (49.6%) maintained complete pain relief at an average 3-year follow-up after repeat surgery across all modalities, microvascular decompression (MVD) and percutaneous rhizotomy were statistically superior to SRS in achieving both initial and long-term complete pain relief
[6]
Rheaume AR, Pietrosanu M, Ostertag C, Sankar T. Repeat Surgery for Recurrent or Refractory Trigeminal Neuralgia: A Systematic Review and Meta-Analysis. World Neurosurg. 2024; 185: 370-380.e2.
. McBenedict et al did a review on the outcomes of various surgical interventions for TN which included GKSR. The review highlights that MVD offers high initial pain relief and substantial long-term effectiveness, while GKSR provides significant pain relief with a favorable adverse event profile, though recurrence rates may increase over time
[7]
McBenedict B, Hauwanga WN, Yau MCY, et al. Outcomes of Different Surgical Interventions for Treating Trigeminal Neuralgia: A Review. Cureus. Published online August 12, 2024.
. For TN patients where the initial GKSR failed, a meta-analysis and institutional study found MVD offered a better chance of complete pain relief than repeat GKRS. Other outcomes like adequate pain relief, facial numbness, and retreatment rates were comparable
[8]
Patra DP, Savardekar AR, Dossani RH, Narayan V, Mohammed N, Nanda A. Repeat Gamma Knife radiosurgery versus microvascular decompression following failure of GKRS in trigeminal neuralgia: a systematic review and meta-analysis. J Neurosurg. 2019; 131(4): 1197-1206.
By employing highly focused radiation beams, SRS delivers a precisely calibrated dose to the affected trigeminal nerve root, while sparing surrounding healthy tissues. The efficacy of SRS in TN treatment has been well-documented, with numerous studies reporting significant pain reduction and improved quality of life in the majority of treated patients. Gamma-knife was the first machine in which TN was treated on and it had significant pain relief of about 80%
[9]
Kondziolka D. Gamma Knife Radiosurgery for Trigeminal Neuralgia: Results and Expectations. ARCH NEUROL. 1998; 55: 6.
[9]
. Patients treated with CyberKnife SRS also had favorable outcomes of around 87% pain-free response. Linac-based SRS also had similar outcomes with a pain-free response rate of 82%. Lee et al did a review and update on GKSR which indicated that GKSR is a first-line treatment for medically refractory TN, offering a favorable short-term pain control rate (BNI I-IIIb) of over 75%, with long-term efficacy around 50–60% at 5 years
[10]
Lee S, Lee JI. Gamma Knife Radiosurgery for Trigeminal Neuralgia : Review and Update. J Korean Neurosurg Soc. 2022; 65(5): 633-639.
Goel et al. found that repeat SRS effectively relieved pain in 80-90% of trigeminal neuralgia (TN) patients within 1-4 months, with 50-90% achieving excellent relief. Recurrence occurred in 20-40% after one year. Common side effects included facial numbness and corneal dryness. The study concluded that repeat SRS is a safe and effective option for recurrent TD pain
[11]
Goel M, Patil NU, Singh R, John J, Upadhyay BR. Retreatment of Classical Tic Douloureux With Stereotactic Radiosurgery: A Scoping Review. Cureus. Published online September 18, 2023.
. Helis et al reported outcomes of a cohort of patients who relapsed and have undergone repeat gamma-knife SRS. The effectiveness of SRS as treatment modality for TN has been reported in the past, with multiple studies noting pain reduction in 81% to 96% of patients. Patients receiving repeat SRS reported pain reduction between 68% to 95%. The most common complication from SRS is unilateral facial numbness notably along the major trigeminal nerve tracts owing to the damage to the nerve. Most patients would rather prefer having the facial numbness as opposed to the pain from TN. They also described five predictive factors for pain relief following a second bout of gamma-knife SRS. These are response to first SRS, facial numbness after first SRS, hypertension, time between first and second SRS, and non-SRS procedure between first and second SRS. Presence of facial numbness and positive pain response after the first SRS were the two dominant factors that would have a better outcome on the second SRS.
Omar et al. (2019) reported on treatment outcomes and toxicity in 55 patients who underwent repeat GKSR for refractory TN
[12]
Omar NB, Amburgy JW, Self DM, et al. Repeat gamma knife stereotactic radiosurgery in the treatment of trigeminal neuralgia: A single-center experience and focused review of the literature. J Clin Neurosci. 2019; 70: 102-107.
. The study did a retrospective review of TN patients re-treated between 1996 and 2012, using the Leksell GKSR. Patients received a radiosurgical dose of 70–80 Gy delivered as a single fraction to the trigeminal nerve's dorsal root entry zone. Outcomes were assessed using the Modified Marseille Scale, and patient demographics (age, gender, comorbidities, symptom duration, interval between treatments) and prior treatments were correlated with outcomes and dysfunction. Patients were followed for a mean of 14.4 months. The results showed that 32 patients (58%) achieved excellent or good outcomes (Modified Marseille Scale classes I-IV) at mean follow-up, with no patients experiencing worsened symptoms. Twenty-five patients (45%) developed new trigeminal nerve dysfunction after re-treatment, with 21 (38%) developing it from GKSR retreatment alone, and 4 (7.3% of total, 16% of those with dysfunction) only after subsequent MVD for inadequate relief. Neither age, gender, duration of symptoms prior to initial GKSR, nor the interval between treatments had a statistically significant effect on outcomes. However, patients who had undergone other surgical treatments for TN prior to their first GKSR therapy demonstrated an overall poorer response to repeat GKSR, although without an increase in TN dysfunction. The study also suggested a trend towards increased risk of new trigeminal nerve dysfunction in patients undergoing MVD after GKSR re-treatment, implying that retreatment may sensitize the nerve to dysfunction during subsequent MVD.
Helis et al in 2021 reported on a series of patients treated with a third GKSR. The results indicated that a third GKRS is an effective treatment, with 18 out of 22 cases achieving successful pain relief (BNI score IIIb) and a median durability of pain relief of 3.88 years, which was not significantly different from the durability observed after first or second GKRS procedures
[13]
Helis CA, Hughes RT, Munley MT, et al. Results of a third Gamma Knife radiosurgery for trigeminal neuralgia. J Neurosurg. 2021; 134(4): 1237-1243.
. Delivery of a third GKSR was also reported by Lee et al, in which the was a reported achievable favorable pain control rates comparable to the second GKSR, albeit with a similar or potentially higher rate of trigeminal nerve dysfunction. Seventeen patients were treated with a third GKSR, with a favorable pain control rate (BNI I–IIIb) in 94% of the patients initially and 76.4% at a mean follow-up of 22.9 months (range, 3–60). The outcome of the third GKRS was comparable to the outcome of the second GKRS for TN
[10]
Lee S, Lee JI. Gamma Knife Radiosurgery for Trigeminal Neuralgia : Review and Update. J Korean Neurosurg Soc. 2022; 65(5): 633-639.
. Vasconcellos et al assessed the efficacy and safety of a third SRS for recurrent TN
[14]
De Nigris Vasconcellos F, Alzate JD, Mashiach E, et al. Efficacy and safety of a third stereotactic radiosurgery for recurrent trigeminal neuralgia: an international, multicenter study. Acta Neurochir (Wien). 2024; 166(1): 422.
. The retrospective analysis of 35 patients revealed that a third SRS provided sustained effectiveness in 82.7% of cases, with a median time to recurrence of 35.5 months. While new sensory dysfunction occurred in 22% of patients who preserved sensory function after the second procedure and affected 40% of the cohort who developed sensory dysfunction after the second procedure, there were no significant differences in pain recurrence intervals among the three procedures. The study concluded that a third SRS offers sustained effectiveness for TN, with an extended pain-free interval and manageable facial sensory dysfunction as the primary side effect.
The study by Guillemette et al. (2024) aimed to evaluate the clinical outcomes, efficacy, and safety of repeat CyberKnife radiosurgery (CKRS) for refractory TN, and to identify potential predictive factors for its efficacy
[15]
Guillemette A, Roberge D, Heymann S, Ménard C, Bahary JP, Fournier-Gosselin MP. Repeat CyberKnife Radiosurgery for Trigeminal Neuralgia: Outcomes and Complications. Can J Neurol Sci J Can Sci Neurol. 2024; 51(2): 272-277.
. This was a retrospective review of 33 patients with medically refractory TN who underwent a second CKRS between 2009 and 2021. The median follow-up period after the second SRS was 26 months, with patients receiving a median repeat dose of 60 Gy (range 60–70 Gy). Pain relief was assessed using the BNI scale (I–V), with scores I to IIIb classified as adequate pain relief. Results showed that initial adequate pain relief was achieved in 87.9% of cases after the second SRS. The actuarial probabilities of maintaining adequate pain relief after the second SRS were 92.1% at 6 months, 74.0% at 12 months, and 58.2% at both 24 and 36 months. There was no significant difference in sustained pain relief between the first and the second SRS. Regarding complications, the onset of hypesthesia rate was the same after both the first and second SRS (21%). A significant finding was that sensory toxicity (hypesthesia onset/aggravation) after the first RS was predictive of a better outcome following the second SRS. The study concluded that repeat CKRS is an effective and safe method for treating refractory TN, with an efficacy and safety profile similar to that of the initial SRS treatment.
4. Conclusion
Retreatment of refractory TN employs different interventions with SRS being one of the primary treatments which is comparable with surgery. While MVD show superior long-term pain relief and lower recurrence rates compared to initial SRS, repeat SRS is also deemed a safe and effective option, achieving 50-90% excellent relief with good long-term outcomes. GKSR emerges as a first-line treatment for medically refractory TN, offering favorable long-term pain control over 75% for 5 years. Overall, the evidence suggests that repeat interventions with SRS, can provide significant and durable pain relief for TN patients, even after initial treatment failures.
Abbreviations
TN
Trigeminal Neuralgia
SRS
Stereotactic Radiosurgery
Gy
Gray
BNI
Barrow Neurological Institute
MRI
Magnetic Resonance Imaging
CT
Computed Tomography
OAR
Organs-at-risk
DVH
Dose Volume Histogram
GKSR
Gamma Knife Radiosurgery
MVD
Microvascular Decompression
CKRS
CyberKnife Radiosurgery
Author Contributions
Don Peter Santiago Dator: Investigation, methodology, writing – original draft, writing – review and editing
As the corresponding author, I confirm that the manuscript has been read by and approved for submission by all authors. Written informed consent was obtained from the patient for publication of this case report and all accompanying images.
Funding
This study did not receive any specific grant from the funding agencies in the public, commercial, or not-for-profit sector.
Conflicts of Interest
The authors declare no conflicts of interest.
References
[1]
Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia. 2018; 38(1): 1-211.
Marchetti M, Pinzi V, De Martin E, Ghielmetti F, Fariselli L. Radiosurgery for trigeminal neuralgia: the state of art. Neurol Sci. 2019; 40(S1): 153-157.
Rheaume AR, Pietrosanu M, Ostertag C, Sankar T. Repeat Surgery for Recurrent or Refractory Trigeminal Neuralgia: A Systematic Review and Meta-Analysis. World Neurosurg. 2024; 185: 370-380.e2.
McBenedict B, Hauwanga WN, Yau MCY, et al. Outcomes of Different Surgical Interventions for Treating Trigeminal Neuralgia: A Review. Cureus. Published online August 12, 2024.
Patra DP, Savardekar AR, Dossani RH, Narayan V, Mohammed N, Nanda A. Repeat Gamma Knife radiosurgery versus microvascular decompression following failure of GKRS in trigeminal neuralgia: a systematic review and meta-analysis. J Neurosurg. 2019; 131(4): 1197-1206.
Goel M, Patil NU, Singh R, John J, Upadhyay BR. Retreatment of Classical Tic Douloureux With Stereotactic Radiosurgery: A Scoping Review. Cureus. Published online September 18, 2023.
Omar NB, Amburgy JW, Self DM, et al. Repeat gamma knife stereotactic radiosurgery in the treatment of trigeminal neuralgia: A single-center experience and focused review of the literature. J Clin Neurosci. 2019; 70: 102-107.
De Nigris Vasconcellos F, Alzate JD, Mashiach E, et al. Efficacy and safety of a third stereotactic radiosurgery for recurrent trigeminal neuralgia: an international, multicenter study. Acta Neurochir (Wien). 2024; 166(1): 422.
Dator, D. P. S., Sy, K. C. (2025). Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia. World Journal of Medical Case Reports, 6(3), 31-37. https://doi.org/10.11648/j.wjmcr.20250603.13
Dator, D. P. S.; Sy, K. C. Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia. World J. Med. Case Rep.2025, 6(3), 31-37. doi: 10.11648/j.wjmcr.20250603.13
Dator DPS, Sy KC. Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia. World J Med Case Rep. 2025;6(3):31-37. doi: 10.11648/j.wjmcr.20250603.13
@article{10.11648/j.wjmcr.20250603.13,
author = {Don Peter Santiago Dator and Kenneth Cortez Sy},
title = {Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia
},
journal = {World Journal of Medical Case Reports},
volume = {6},
number = {3},
pages = {31-37},
doi = {10.11648/j.wjmcr.20250603.13},
url = {https://doi.org/10.11648/j.wjmcr.20250603.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjmcr.20250603.13},
abstract = {Trigeminal neuralgia (TN) is a debilitating neurological disorder characterized by sudden, severe facial pain along the distribution of the trigeminal nerve. It may significantly affect a patient’s quality of life. Stereotactic radiosurgery (SRS) is a non-invasive therapeutic option for managing TN, providing targeted precision and minimal side effects. The long-term benefits of SRS are noteworthy, as pain relief often persists for several years after the procedure. The authors aim to present a rare case of a reirradiation of a recurrent trigeminal neuralgia case. This is a case of a 74-year-old female who has had symptoms of TN for more than twenty years before undergoing gamma-knife SRS in 2017 with a dose of 90 Gray (Gy). Post SRS had good pain control for the next five years until in 2022 when she had increasing intensity of the pain no longer tolerable by medications. She was then treated in our institution using a linac-based SRS for a dose of 70 Gy. Post-second SRS, she reported no recurrence of severe pain. Twelve month follow-up noted no recurrence of severe pain with good quality of life and the only complication is unilateral left facial numbness. Repeat radiation with stereotactic radiosurgery with different techniques is feasible in refractory case of trigeminal neuralgia.},
year = {2025}
}
TY - JOUR
T1 - Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia
AU - Don Peter Santiago Dator
AU - Kenneth Cortez Sy
Y1 - 2025/07/30
PY - 2025
N1 - https://doi.org/10.11648/j.wjmcr.20250603.13
DO - 10.11648/j.wjmcr.20250603.13
T2 - World Journal of Medical Case Reports
JF - World Journal of Medical Case Reports
JO - World Journal of Medical Case Reports
SP - 31
EP - 37
PB - Science Publishing Group
SN - 2994-726X
UR - https://doi.org/10.11648/j.wjmcr.20250603.13
AB - Trigeminal neuralgia (TN) is a debilitating neurological disorder characterized by sudden, severe facial pain along the distribution of the trigeminal nerve. It may significantly affect a patient’s quality of life. Stereotactic radiosurgery (SRS) is a non-invasive therapeutic option for managing TN, providing targeted precision and minimal side effects. The long-term benefits of SRS are noteworthy, as pain relief often persists for several years after the procedure. The authors aim to present a rare case of a reirradiation of a recurrent trigeminal neuralgia case. This is a case of a 74-year-old female who has had symptoms of TN for more than twenty years before undergoing gamma-knife SRS in 2017 with a dose of 90 Gray (Gy). Post SRS had good pain control for the next five years until in 2022 when she had increasing intensity of the pain no longer tolerable by medications. She was then treated in our institution using a linac-based SRS for a dose of 70 Gy. Post-second SRS, she reported no recurrence of severe pain. Twelve month follow-up noted no recurrence of severe pain with good quality of life and the only complication is unilateral left facial numbness. Repeat radiation with stereotactic radiosurgery with different techniques is feasible in refractory case of trigeminal neuralgia.
VL - 6
IS - 3
ER -
Dator, D. P. S., Sy, K. C. (2025). Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia. World Journal of Medical Case Reports, 6(3), 31-37. https://doi.org/10.11648/j.wjmcr.20250603.13
Dator, D. P. S.; Sy, K. C. Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia. World J. Med. Case Rep.2025, 6(3), 31-37. doi: 10.11648/j.wjmcr.20250603.13
Dator DPS, Sy KC. Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia. World J Med Case Rep. 2025;6(3):31-37. doi: 10.11648/j.wjmcr.20250603.13
@article{10.11648/j.wjmcr.20250603.13,
author = {Don Peter Santiago Dator and Kenneth Cortez Sy},
title = {Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia
},
journal = {World Journal of Medical Case Reports},
volume = {6},
number = {3},
pages = {31-37},
doi = {10.11648/j.wjmcr.20250603.13},
url = {https://doi.org/10.11648/j.wjmcr.20250603.13},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjmcr.20250603.13},
abstract = {Trigeminal neuralgia (TN) is a debilitating neurological disorder characterized by sudden, severe facial pain along the distribution of the trigeminal nerve. It may significantly affect a patient’s quality of life. Stereotactic radiosurgery (SRS) is a non-invasive therapeutic option for managing TN, providing targeted precision and minimal side effects. The long-term benefits of SRS are noteworthy, as pain relief often persists for several years after the procedure. The authors aim to present a rare case of a reirradiation of a recurrent trigeminal neuralgia case. This is a case of a 74-year-old female who has had symptoms of TN for more than twenty years before undergoing gamma-knife SRS in 2017 with a dose of 90 Gray (Gy). Post SRS had good pain control for the next five years until in 2022 when she had increasing intensity of the pain no longer tolerable by medications. She was then treated in our institution using a linac-based SRS for a dose of 70 Gy. Post-second SRS, she reported no recurrence of severe pain. Twelve month follow-up noted no recurrence of severe pain with good quality of life and the only complication is unilateral left facial numbness. Repeat radiation with stereotactic radiosurgery with different techniques is feasible in refractory case of trigeminal neuralgia.},
year = {2025}
}
TY - JOUR
T1 - Repeat LINAC Radiosurgery from Previously Treated Gamma Knife Radiosurgery on Medically Refractory Classical Trigeminal Neuralgia
AU - Don Peter Santiago Dator
AU - Kenneth Cortez Sy
Y1 - 2025/07/30
PY - 2025
N1 - https://doi.org/10.11648/j.wjmcr.20250603.13
DO - 10.11648/j.wjmcr.20250603.13
T2 - World Journal of Medical Case Reports
JF - World Journal of Medical Case Reports
JO - World Journal of Medical Case Reports
SP - 31
EP - 37
PB - Science Publishing Group
SN - 2994-726X
UR - https://doi.org/10.11648/j.wjmcr.20250603.13
AB - Trigeminal neuralgia (TN) is a debilitating neurological disorder characterized by sudden, severe facial pain along the distribution of the trigeminal nerve. It may significantly affect a patient’s quality of life. Stereotactic radiosurgery (SRS) is a non-invasive therapeutic option for managing TN, providing targeted precision and minimal side effects. The long-term benefits of SRS are noteworthy, as pain relief often persists for several years after the procedure. The authors aim to present a rare case of a reirradiation of a recurrent trigeminal neuralgia case. This is a case of a 74-year-old female who has had symptoms of TN for more than twenty years before undergoing gamma-knife SRS in 2017 with a dose of 90 Gray (Gy). Post SRS had good pain control for the next five years until in 2022 when she had increasing intensity of the pain no longer tolerable by medications. She was then treated in our institution using a linac-based SRS for a dose of 70 Gy. Post-second SRS, she reported no recurrence of severe pain. Twelve month follow-up noted no recurrence of severe pain with good quality of life and the only complication is unilateral left facial numbness. Repeat radiation with stereotactic radiosurgery with different techniques is feasible in refractory case of trigeminal neuralgia.
VL - 6
IS - 3
ER -