Abstract
Cancer is a growing public health concern worldwide, particularly in low and middle-income countries such as Bangladesh. Lifestyle factors, including dietary habits, smoking, and obesity, play a crucial role in cancer development. To provide updated insights for risk prediction and public health interventions this study aims is to collect and analyze patient data from the National Institute of Cancer Research and Hospital (NICRH) to identify and evaluate the association of lifestyle risk factors with cancer incidence in Bangladesh. This study investigates the prevalence of different cancers and their association with modifiable risk factors among Bangladeshi cancer patients. A cross-sectional study was conducted at the NICRH where two-thirds (201) of the cancer patients’ data were involving to dominate the result. Data were collected using a structured questionnaire, and logistic regression analysis was performed by SPSS (Statistical Package for the Social Sciences), version 26 (SPSS Inc., Chicago, IL, USA) to assess the relationship between cancer and lifestyle factors. The findings indicate that breast cancer (18.9%) was the most prevalent cancer, followed by lung (15.9%), stomach (12.9%), cervix uteri (12.9%), and esophageal cancer (6.5%). Lung cancer was most common in males (27.5%), whereas breast cancer was the most frequent in females (34.5%). The highest cancer incidents were observed in individuals aged 40-60 years. Smoking showed a significant association with lung cancer (OR: 1.230, P = 0.001), while obesity was strongly associated with breast cancer (OR: 1.43, P = 0.006). These findings highlight the urgent need for public health intervention, including tobacco control, obesity prevention, dietary modifications, and expanded cancer screening programs, to reduce cancer incidence in Bangladesh. Addressing these risk factors through policy-driven strategies and awareness initiatives could significantly improve cancer prevention and early detection efforts.
|
Published in
|
Science Journal of Public Health (Volume 13, Issue 4)
|
|
DOI
|
10.11648/j.sjph.20251304.14
|
|
Page(s)
|
196-204 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2025. Published by Science Publishing Group
|
Keywords
Cancer, Smoking, Obesity, Diet, Public Health, Bangladesh
1. Introduction
Cancer is a leading cause of morbidity and mortality worldwide, with its burden increasing at an alarming rate, particularly in low and middle-income countries (LMICs) such as Bangladesh. Despite advancements in medical science, the global cancer incidence continues to rise, posing significant challenges to healthcare systems, economies, and public health policies
| [1] | Eldridge, L., Cira, M. K., Duncan, K., Pearlman, P., & Gopal, S. (2020). The 8th Symposium on Global Cancer Research: Recognizing creativity and collaboration to support global cancer research and control. JCO Global Oncology, 6, GO-20. |
[1]
. Historically, cancer was primarily considered a disease of high-income nations, but over 55% of global cancer cases were recorded in developing countries by 2010, a figure expected to surpass 70% by 2040
| [2] | Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide 36 cancers in 185 Countries. CA Cancer J Clin. 2021; 71(3): 209-249. |
[2]
. Given its increasing incidence, cancer is projected to be a major contributor to global mortality, there will be 26 million new cancer cases with 17 million deaths annually by 2030, of which more than 50% will occur in LMICs
| [3] | Thun MJ, DeLancey JO, Center MM, Jemal A, Ward EM. The global burden of cancer: priorities for prevention. Carcinogenesis. 2010; 31(1): 100-110. https://doi.org/10.1093/carcin/bgp263 |
[3]
.
The United Nations (UN) Sustainable Development Goals (SDGs) recognize cancer as a major non-communicable disease (NCD), emphasizing the need for interventions under Target 3.4, which aims to reduce premature mortality from NCDs by one-third by 2030 through prevention and treatment
. As the global cancer burden shifts towards developing nations, it is imperative to investigate modifiable risk factors, particularly diet, smoking, and obesity, which play a significant role in cancer development and prevention.
Bangladesh has witnessed a rapid increase in cancer incidence and mortality in recent years. According to GLOBOCAN 2022, the country recorded 1,67,256 new cancer cases and 1,16,598 cancer-related deaths, with an age-standardized mortality rate of 75.3 per 100,000 individuals
. In 2020, the global cancer burden escalated, with an estimated 19.3 million new cases and 10.0 million cancer related deaths, highlighting a growing public health crisis
| [6] | Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Pineros M, Znaor A. et al. cancer statistics for the year 2020: An overview. Int J Cancer Prev. 2021; 149(4): 778-789. |
[6]
. Despite the growing burden, cancer remains underdiagnosed and undertreated due to limited healthcare infrastructure, high costs of treatment, and inadequate cancer screening programs
| [7] | Iqbal J. (2025). National Cancer Registries in Bangladesh and Social Determinants of Health: Challenging Cancer Disparities. Cancer control: journal of the Moffitt Cancer Center, 32, 10732748251323757. https://doi.org/10.1177/10732748251323757 |
[7]
. Additionally, many patients go for treatment or seek care abroad, leading to financial strain and foreign currency outflow
.
Among the key modifiable risk factors, diet plays a crucial role in cancer prevention and progression. Unhealthy dietary habits, including excessive consumption of processed foods, red meat, and trans fats, have been linked to colorectal, gastric, liver, and breast cancers
| [9] | Bangladesh Medical Research Council Bulletin. The impact of tobacco uses on cancer rates in Bangladesh. 2021; 47(2): 112-119. |
[9]
. The International Agency for Research on Cancer (IARC) classifies processed meats as Group l carcinogens, associating them with an increased risk of colorectal cancer
. In South Asian countries like Bangladesh, rapid urbanization has led to increased consumption of Westernized diets, contributing to a rise in diet-related cancers, particularly affecting the gastrointestinal tract
| [11] | Shiraj-Um-Mahmuda S, Begum F, Rahman MM, Rahman P, Islam T, et al. (2023) Demographic and Clinicopathological Evaluation of Colorectal Adenocarcinoma in Bangladesh at a Tertiary Level Hospital. Cancer Stud Ther J Volume 8(1): 1–8. https://doi.org/10.31038/CST.2023811 |
[11]
. Furthermore, arsenic-contaminated drinking water, a long-standing public health issue in Bangladesh, has been linked to elevated risks of skin, lung, and bladder cancers
.
Similarly, tobacco use remains the single most preventable cause of cancer, contributing to nearly 25% of all cancer-related deaths globally
| [13] | The Lancet Global Health. Health Impact of Arsenic Contamination in Bangladesh. 2019; 7(6): e785-e796. |
[13]
. Bangladesh has one of the highest smoking rates in South Asia, with 35% of adult men and 10% of women engaged in tobacco use, significantly increasing the risk of lung, oral, and esophageal cancers
| [14] | Islami F, Goding Sauer A, Miller KD, Siegel RL, Fedewa SA, Jacobs EJ, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018; 68(1): 31-54. |
[14]
.
Obesity, another critical risk factor, has been strongly linked to hormone-dependent cancers, including breast, endometrial, prostate, and colorectal cancers
. Excessive body fat promotes chronic inflammation, insulin resistance, and hormonal imbalances, all of which contribute to tumor progression and metastasis
| [16] | Abu-Abid, S., Szold, A., & Klausner, J. (2002). Obesity and cancer. Journal of medicine, 33(1-4), 73–86. |
[16]
. In Bangladesh, sedentary life styles and high-calorie diets are increasingly contributing to obesity-related cancers, particularly in postmenopausal breast cancer, endometrial cancer, and colorectal cancer
| [17] | Environmental Health Perspective. Air Pollution and Cancer Risk in Dhaka. 2022; 130(4): 410-422. |
[17]
.
The primary objectives of this study is to collect and analyze patient data from the NICRH to identify and evaluate the association of dietary habits, smoking, and obesity with cancer incidence in Bangladesh, providing updated insights for risk prediction and public health interventions.
2. Materials and Methods
2.1. Study Design
This study was conducted as a cross-sectional survey to assess the association of dietary habits, smoking and obesity with cancer incidence in Bangladesh. It was carried out using a structured questionnaire designed to collect relevant socio-demographic, lifestyle, and clinical data from cancer patients.
2.2. Study Subjects
The study population consisted of cancer patients admitted to the National Institute of Cancer Research and Hospital (NICRH), Mohakhali, Dhaka-1212, the country's leading 300 bedded specialized cancer hospital that provides treatment to thousands of patients annually. The respondents were selected from diverse socioeconomic, occupational, and geographical backgrounds, representing various types of cancer. Only inpatient cancer patients were included in this study. A total of 201 cancer patients were randomly selected from 300 patients; two-thirds of the total inpatient cancer patients are sufficient to support our research claims by dominating the results. Patients were interviewed using a random sampling technique to ensure a preventative sample of different cancer conditions and associated risk factors. The research was conducted over a six-month period, from July 2024 to December 2024.
2.3. Data Collection Method
Data were collected through face-to-face interviews with patients using a standardized questionnaire designed to capture relevant information. The questionnaire covered socio-demographic factors, including age, gender, occupation, residence, and economic background, as well as cancer diagnosis details, such as type, stage, and duration since diagnosis. Additionally, data on lifestyle risk factors were gathered, focusing on dietary habits (frequency of processed food consumption, fruit and vegetable intake, and high-risk food consumption), smoking status (current or former smoker, frequency, duration, and type of tobacco used), and obesity-related parameters (Who classified BMI, physical activity level, and weight gain history).
2.4. Ethical Considerations
This study was conducted following strict ethical standards to ensure the protection of participants rights and well-being. Ethical approval was obtained from the Institutional Review Board (IRB) of the National Institute of Cancer Research and Hospital (NICRH), Dhaka, Bangladesh, prior to the commencement of the research. Informed written consent was obtained from all participants after providing a clear explanation of the study objectives, procedures, potentials risk, and benefits. Participants were assured of the confidentially of their personal information, and their involvement in the study was entirely voluntary, with the right to withdraw at any stage without any consequences. All data were anonymized and securely stored in compliance with institutional and international ethical guideline.
2.5. Data Analysis
Descriptive statistics were employed to summarize the demographic characteristics of the study participants and the distribution of relevant risk factors. Categorical variables were expressed as frequencies and percentages, while continues variables were presented as means with standard deviations. Association between categorical variables were examines using Chi-square tests. To identify factors independently associated with the outcome of interest, multivariable logistic regression models were applied, adjusting for potential confounders. Statistical significance was set at P<0.05. all analysis was performed using SPSS (Statistical Package for the Social Sciences), version 26 (SPSS Inc., Chicago, IL, USA).
2.6. Patients and Public Involvement
Patients or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
3. Results
3.1. Cancer Distribution Among Patients
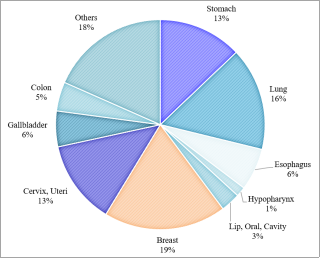
The study analyzed a total of 201 cancer patients admitted to the NICRH, Dhaka, to assess the prevalence and distribution of various cancer types. Among the total patient population, breast cancer emerged as the most prevalent, accounting for 18.9% of cases, followed by lung cancer (15.9%), stomach cancer (12.9%), cervix uteri cancer (12.9%), and esophageal cancer (6.5%). Other notable cancers identified in the study included hypo pharynx, lip and oral cavity, and gallbladder cancers, though with lower prevalence rates.
Figure 1. Overall Distribution of Cancer Among Study Participants.
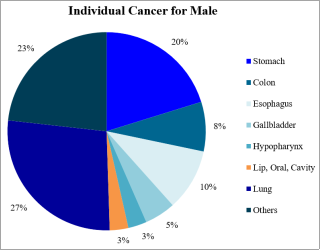
When cancer prevalence was examined by gender, significant differences were observed. In male patients, lung cancer accounted for the highest proportion, representing 27.5% of cases. This was followed by stomach cancer at 19.8%, esophageal cancer at 9.9%, and colon cancer at 7.7%.
Figure 2. Frequency of Different Cancers in Male Patients.
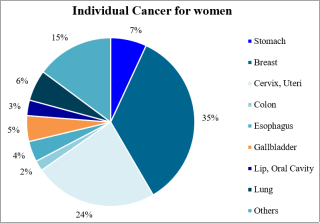
Among female patients, breast cancer was found to be the most dominant type, representing 34.5% of all female cancer cases. Cervix uteri cancer followed at 23.6%, while stomach cancer accounted for 7.3% of cases. Additionally, lung cancer (6.4%), gallbladder cancer (5.5%), and esophageal cancer (3.6%) were also present in notable proportions.
Figure 3. Frequency of Different Cancers in Female Patients.
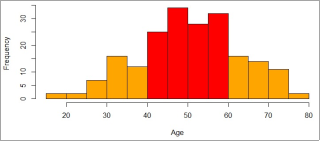
Age was also identified as a crucial factor in cancer prevalence. The highest proportion of cases was recorded in the 46-55 years age group, accounting for 30.8% of the total study population. This was followed by the 56-65 years age group, which comprised 23.9% of cases, and the 36-45 years age group, which constituted 18.4%. The lowest incidence was observed among patients younger than 25 years (2%), while only one patient was recorded in the above-80 years category. This data suggests that individuals aged 40-60 years are at the highest risk of developing cancer compared to other age groups.
Figure 4. Distribution of cancer patients across different age groups.
3.2. Demographic Characteristics of the Study Population
The demographic characteristics of the study population, including age distribution, gender composition, WHO BMI classification, and cancer type prevalence, are summarized in
Table 1. The findings indicate that the majority of cancer patients belonged to the age group of 46-55 years (30.8%), followed by the 56-65 years group (23.9%). A relatively smaller proportion of patients (2%) were aged below 25 years, while 13.4% were aged above 65 years.
In terms of gender distribution, female patients accounted for a higher proportion of cases, representing 54.7% (n=110), while male patients comprised 45.3% (n=91). Regarding BMI classification, 15.4% of patients were underweight, 55.77% were classified as having a normal BMI, and 28.9% were overweight. Cancer type prevalence showed that breast cancer was the most frequently diagnosed (19%), followed by lung cancer (16%), stomach cancer (13%), and cervix uteri cancer (13%). Other cancer types, including esophageal (6%), gallbladder (5%), and colon (4%) cancers, were also observed in the study population.
Table 1. Demographic information of cancer patients included in the study.
Variables | Numbers of cancer patients (n) | % |
Age |
Less than 25 | 4 | 2.0% |
26-35 | 23 | 11.4% |
36-45 | 37 | 18.4% |
46-55 | 62 | 30.8% |
56-65 | 48 | 23.9% |
Above 65 | 27 | 13.4% |
Gender |
Female | 110 | 54.7% |
Male | 91 | 45.3% |
BMI |
Underweight | 31 | 15.4% |
Normal | 112 | 55.7% |
Overweight | 58 | 28.9% |
Types of Cancer |
Stomach | 26 | 12.9% |
Lung | 32 | 15.9% |
Esophagus | 13 | 6.5% |
Hypopharynx | 3 | 1.5% |
Lip, Oral, Cavity | 6 | 3.0% |
Breast | 38 | 18.9% |
Cervix, Uteri | 26 | 12.9% |
Gallbladder | 11 | 5.5% |
Colon | 9 | 4.5% |
Others | 37 | 18.4% |
3.3. Association Between Diet and Smoking & Lung Cancer
The study further analyzed the association between lifestyle factors, particularly dietary habits, smoking, and lung cancer risk. The odds ratio (OR) and P-values obtained for different factors are presented in
Table 2. A statistically significant association was observed between smoking and lung cancer, with an odds ratio of 1.230 and a P-value of 0.001, indicating a strong correlation. The use of tobacco-like products was also positively associated with lung cancer (OR: 1.389, P- value: 0.627), though this association was not statistically significant. Other dietary risk factors, such as processed food (OR: 0.482, P-value: 0.134) and alcohol consumption (OR: 0.245, P-value: 0.168), demonstrated negative correlations with lung cancer risk and also lacked statistical significance.
Table 2. Association between diet, smoking, and lung cancer risk.
Association of diet and smoking with lung cancer |
Factors | Odds Ratio | P-value | 95% C.I. |
(Lower) | (Upper) |
Processed Food | 0.482 | 0.134 | 0.186 | 1.251 |
Refined Sugar | 0.886 | 0.821 | 0.309 | 2.538 |
Alcohol | 0.245 | 0.168 | 0.033 | 1.810 |
Sugary Drinks | 1.635 | 0.281 | 0.668 | 4.000 |
Smoking | 1.230 | 0.001 | 0.097 | 0.546 |
Tobacco-like Products | 1.389 | 0.627 | 0.370 | 5.217 |
3.4. Association Between Diet and Obesity & Breast Cancer
Similarly, the study assessed the relationship between dietary patterns, obesity, and breast cancer risk. The results indicate that obesity was significantly associated with breast cancer, with an odds ratio of 1.43 and a P-value of 0.006. Alcohol consumption is negatively correlated with breast cancer incidence but statistically significant (OR: 0.071, P-value: 0.015). Additionally, tobacco-like products were not significantly associated with breast cancer but statistically highly significant (OR: 0.276, P-value: 0.005). Other dietary factors such as processed food (OR: 0.740, P-value: 0.507) and sugary drinks (OR: 0.927, P-value: 0.859) showed negative and statistically non-significant correlations with breast cancer.
Table 3. Association between diet, obesity, and breast cancer risk.
Association of Diet and obesity with Breast Cancer |
Factors | Odds Ratio | P-value | 95%C.I. |
Lower | Upper |
Red Meat | 0.524 | 0.560 | 0.059 | 4.611 |
Processed Food | 0.740 | 0.507 | 0.305 | 1.799 |
Refined Sugar | 0.437 | 0.125 | 0.151 | 1.260 |
Alcohol | 0.071 | 0.015 | 0.008 | 0.600 |
Obesity | 1.43 | 0.006 | 2.335 | 3.349 |
Tobacco-like Products | 0.276 | 0.005 | 0.112 | 0.680 |
This study highlights significant associations between modifiable lifestyle factors and cancer prevalence, reinforcing the need for targeted public health interventions aimed at reducing obesity, tobacco consumption, and unhealthy dietary habits.
4. Discussion
This study provides a comprehensive overview of different types of cancers and their association with modifiable lifestyle factors, including dietary habits, smoking, and obesity, among cancer patients in Bangladesh. The findings reveal significant associations between these risk factors and cancer incidence, highlighting the urgent need for targeted public health interventions.
4.1. Prevalence and Distribution of Cancer in Bangladesh
The study found that breast cancer was the most prevalent cancer type, followed by lung, stomach, cervix uteri, and esophageal cancers. This distribution aligns with global cancer statistics, which indicate that breast and lung cancers are among the most commonly diagnosed malignancies worldwide
| [18] | Sung H, Ferlay J, Siegel RL et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209-249. |
[18]
. The high prevalence of breast cancer among female patients (35%) is consistent with findings from previous research (32.8%) in Bangladesh, where hormonal, genetic, and lifestyle factors have been implicated in increasing incidence rates
. The burden of cervix uteri cancer (24%) among women also highlights the need for improved cervical cancer screening and HPV vaccination programs, as HPV infection remains a major risk factor in developing countries
| [20] | WHO. Cancer Prevention Strategies: Global initiatives and progress. |
[20]
.
Among male patients, lung cancer accounted for the highest proportion (27%), followed by stomach and esophageal cancers. This trend is strongly linked to high smoking prevalence in Bangladesh, where over 35% of men use tobacco products, including cigarettes and smokeless tobacco
| [14] | Islami F, Goding Sauer A, Miller KD, Siegel RL, Fedewa SA, Jacobs EJ, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018; 68(1): 31-54. |
[14]
. Previous studies have demonstrated that tobacco use is responsible for nearly 90% of lung cancer cases globally; reinforcing our finding that smoking is significantly associated with lung cancer risk
| [21] | ACS. The economic cost of tobacco uses in Bangladesh. |
[21]
.
Age also played a crucial role in cancer susceptibility, with the highest prevalence observed in individuals aged 40-60 years. This is consistent with research suggesting that cancer incidence increases with age due to cumulative exposure to carcinogens, genetic mutations, and weakened immune function
| [6] | Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Pineros M, Znaor A. et al. cancer statistics for the year 2020: An overview. Int J Cancer Prev. 2021; 149(4): 778-789. |
[6]
. There natively low number of cancer cases among individuals younger than 25 and older than 80 may indicate lower exposure to carcinogenic risk factors in younger individuals and underreporting in elderly populations due to healthcare accessibility issues.
4.2. Association of Lifestyle Factors with Cancer
4.2.1. Smoking and Lung Cancer
Our study found a statistically significant association between smoking and lung cancer, with an odds ratio of 1.230 (P-value: 0.001). This finding aligns with extensive literature showing that tobacco smoke contains more than 60 known carcinogens, including polycyclic aromatic hydrocarbons (PAHs), nitrosamines, and benzene, which induce DNA damage and promote malignant transformation
| [22] | IARC. Tobacco smoke and cancer risk. |
[22]
. The observed positive association between tobacco-like product use and lung cancer (OR: 1.389, P-value: 0.627) was not statistically significant, potentially due to the small sample size and variability in tobacco consumption patterns.
Despite global efforts to reduce tobacco consumption, Bangladesh continues to experience high smoking rates, largely due to cultural acceptance, affordability, and weak regulatory enforcement
| [23] | WHO. Global tobacco report 2022. |
[23]
. These findings reinforce the urgent need for strengthened tobacco control policies, increased taxation on tobacco products, and awareness campaigns to mitigate the growing burden of tobacco-related cancers.
4.2.2. Obesity and Breast Cancer
The study also found a strong correlation between obesity and breast cancer, with an odds ratio of 1.43 (P-value: 0.006), indicating that overweight and obese women are at significantly higher risk of developing breast cancer. Similar associations have been reported in international studies, where excess adipose tissue is known to increase estrogen production, leading to hormone-driven tumor development
| [24] | Torre LA, Siegel RL, Ward EM et al. Global cancer incidence and mortality rates and trends—an update. Cancer Epidemiol Biomarkers Prev 2016; 25: 16-27. |
[24]
. Obesity also contributes to chronic inflammation, insulin resistance, and oxidative stress, further promoting cancer progression.
A significant association between alcohol consumption and breast cancer (OR: 1.071, P-value: 0.015) was also observed, supporting findings that alcohol acts as a carcinogen by increasing estrogen levels and promoting DNA mutations
| [25] | NCI. Alcohol and cancer risk: A review of evidence. |
[25]
. Given that alcohol consumption is increasing in Bangladesh, particularly among urban populations, targeted interventions are needed to address this emerging risk factor.
4.2.3. Dietary Factors and Cancer Risk
Although this study did not establish statistically significant associations between processed food, refined sugar, and cancer risk, previous research has linked diets high in processed meats, red meat, and sugary beverages with an increased risk of colorectal, gastric, and breast cancers, due to their role in inflammation, insulin resistance, and exposure to carcinogenic additives
| [13] | The Lancet Global Health. Health Impact of Arsenic Contamination in Bangladesh. 2019; 7(6): e785-e796. |
[13]
. The high prevalence of gastric and colorectal cancers observed in our study may be partially attributed to changing dietary patterns in Bangladesh, where fast food as well as high ultra-processed food consumption has increased significantly due to urbanization
| [26] | Meine, G. C., Picon, R. V., Espírito Santo, P. A., & Sander, G. B. (2024). Ultra-Processed Food Consumption and Gastrointestinal Cancer Risk: A Systematic Review and Meta-Analysis. The American journal of gastroenterology, 119(6), 1056–1065. |
[26]
.
In addition to diet, environmental exposure to arsenic-contaminated water in Bangladesh is another critical risk factor. Arsenic has been classified as a Group 1 human carcinogen, with chronic exposure linked to lung, skin, and bladder cancers
| [17] | Environmental Health Perspective. Air Pollution and Cancer Risk in Dhaka. 2022; 130(4): 410-422. |
[17]
. The findings from this study highlight the urgent need for improved water purification systems and stricter regulation of groundwater contamination.
4.3. Public Health Implications
The findings of this study highlight the urgent need for national cancer prevention strategies in Bangladesh, focusing on modifiable lifestyle risk factors. The significant association between smoking and lung cancer, as well as obesity and breast cancer, underscores the importance of early intervention programs aimed at reducing exposure to known carcinogens. Tobacco control policies must be reinforced by implementing higher taxation on tobacco products, stricter smoking bans, and nationwide awareness campaigns
. Additionally, breast cancer screening programs should be expanded, particularly for high-risk populations, such as obese women and those with a family history of breast cancer
| [27] | BMC Cancer. The role of obesity in cancer risk: Evidence from Bangladesh. BMC Cancer 2021; 21: 745. |
[27]
.
Public health initiatives should also focus on dietary interventions, discouraging processed food and sugary beverage consumption, while rooming higher intake of fiber-rich foods, vegetables, and antioxidant –rice fruits. Obesity prevention programs should be integrated into national healthcare strategies, promoting physical activity, balanced nutrition, and community-based weight management programs
| [28] | Asian Pac J Cancer Prev. The role of lifestyle factors in cancer prevention in South Asia. Asian Pac J Cancer Prev 2022; 23: 1123-1130. |
[28]
.
5. Conclusions
This study provides crucial insights into the prevalence of different cancer types and their association with lifestyle risk factors, including diet, smoking, and obesity, among cancer patients in Bangladesh. The findings reveal that breast cancer is the most common malignancy among females, while lung cancer remains the leading cancer among males, emphasizing the need for targeted cancer prevention strategies. Additionally, the study highlights the strong correlation between smoking and lung cancer, as well as obesity and breast cancer, underlining the significant role of modifiable risk factors in cancer development.
The results of this study reinforce the need for national-level public health interventions to reduce cancer-related morbidity and mortality in Bangladesh. Tobacco control measures, obesity prevention programs, and dietary modifications should be prioritized to mitigate the increasing burden of cancer. Expanding cancer screening programs, particularly for breast and lung cancer, and promoting early detection and lifestyle interventions are essential steps toward reducing cancer incidence. Furthermore, environmental pollution control and access to clean drinking water must be strengthened to reduce exposure to known carcinogens such as arsenic, which has been linked to multiple cancer types.
Despite its valuable contributions, this study acknowledges some limitations, including a cross-sectional design that restricts causal inferences, a relatively small sample size, and potential recall bias in self-reported dietary and smoking habits. Future research with larger sample sizes and prospective cohort studies is needed to validate these associations further and develop comprehensive cancer prevention strategies tailored to the Bangladeshi population.
In conclusion, this study highlights the urgent need for cancer awareness, prevention, and screening programs in Bangladesh. By addressing modifiable lifestyle factors, strengthening public health policies, and improving healthcare accessibility, it is possible to reduce the burden of cancer and enhance overall population health. Multisectoral collaboration involving healthcare professionals, policymakers, researchers, and community stakeholders is essential to implement effective strategies that can lower cancer incidence and improve treatment outcomes in Bangladesh.
Abbreviations
NICRH | National Institute of Cancer Research and Hospital |
LMICs | Low and Middle-income Countries |
UN | United Nations |
SDGs | Sustainable Development Goals |
NCD | Non-communicable Disease |
BMI | Body Mass Index |
Acknowledgments
The authors sincerely thank the National Institute of Cancer Research and Hospital (NICRH), Dhaka, for their support in facilitating this research. We also appreciate the participation of all patients and their families; whose contributions were invaluable.
Special thanks to the Islamic University, Kushtia-7003, Bangladesh, for funding this study and to the Department of Applied Nutrition and Food Technology for their guidance. We also acknowledge their efforts of research assistants and hospital staff for their assistance in data collection and management. Finally, we are grateful to colleagues and reviewers for their valuable insights, which have helped refine this study.
Author Contributions
Amanullah Marof: Data curation, Formal Analysis, Funding acquisition, Methodology, Project administration
Md. Al-Amin: Investigation, Software, Visualization, Writing – review & editing
Mst. Sabiha Sultana: Conceptualization, Data curation, Formal Analysis, Software, Visualization, Writing – review & editing
Kamrun Nahar Konika: Investigation, Software, Writing – review & editing
Md. Shaheduzzaman Roky: Software, Writing – review & editing
Shahat Shiddiqe: Software, Writing – review & editing
Asad Ud-Daula: Conceptualization, Resources, Supervision, Validation, Writing – original draft
Funding
This work is supported by research grants from Islamic University, Kushtia-7003, Bangladesh during the 2024–2025 fiscal year.
Data Availability Statement
The data is available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Eldridge, L., Cira, M. K., Duncan, K., Pearlman, P., & Gopal, S. (2020). The 8th Symposium on Global Cancer Research: Recognizing creativity and collaboration to support global cancer research and control. JCO Global Oncology, 6, GO-20.
|
| [2] |
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide 36 cancers in 185 Countries. CA Cancer J Clin. 2021; 71(3): 209-249.
|
| [3] |
Thun MJ, DeLancey JO, Center MM, Jemal A, Ward EM. The global burden of cancer: priorities for prevention. Carcinogenesis. 2010; 31(1): 100-110.
https://doi.org/10.1093/carcin/bgp263
|
| [4] |
United Nations. Sustainable development Goals Report 2023. Available at:
https://unstats.un.org/sdgs/report/2023/
|
| [5] |
GLOBOCAN 2022: Cancer in Bangladesh – Global Cancer Observatory. Available at:
https://gco.iarc.who.int/media/globocan/factsheets/populations/50-bangladesh-fact-sheet.pdf
|
| [6] |
Ferlay J, Colombet M, Soerjomataram I, Parkin DM, Pineros M, Znaor A. et al. cancer statistics for the year 2020: An overview. Int J Cancer Prev. 2021; 149(4): 778-789.
|
| [7] |
Iqbal J. (2025). National Cancer Registries in Bangladesh and Social Determinants of Health: Challenging Cancer Disparities. Cancer control: journal of the Moffitt Cancer Center, 32, 10732748251323757.
https://doi.org/10.1177/10732748251323757
|
| [8] |
International Agency for Research on Cancer (IARC). Processed Meat and Cancer risk. Available at:
https://www.iarc.who.int/processed-meat-and-cancer/
|
| [9] |
Bangladesh Medical Research Council Bulletin. The impact of tobacco uses on cancer rates in Bangladesh. 2021; 47(2): 112-119.
|
| [10] |
American Cancer Society (ACS). The Economic Cost of Tobacco Use in Bangladesh. Available at:
https://www.cancer.org/content/dam/cancer-org-/research/economic-and-healthy-policy/bangladesh-health-cost-full-report-2020.pdf
|
| [11] |
Shiraj-Um-Mahmuda S, Begum F, Rahman MM, Rahman P, Islam T, et al. (2023) Demographic and Clinicopathological Evaluation of Colorectal Adenocarcinoma in Bangladesh at a Tertiary Level Hospital. Cancer Stud Ther J Volume 8(1): 1–8.
https://doi.org/10.31038/CST.2023811
|
| [12] |
National Cancer Institute (NCI). Arsenic and Cancer Risk. Available at:
https://www.cancer.gov/about-cancer/causes-prevention/risk/substances/arsenic
|
| [13] |
The Lancet Global Health. Health Impact of Arsenic Contamination in Bangladesh. 2019; 7(6): e785-e796.
|
| [14] |
Islami F, Goding Sauer A, Miller KD, Siegel RL, Fedewa SA, Jacobs EJ, et al. Proportion and number of cancer cases and deaths attributable to potentially modifiable risk factors in the United States. CA Cancer J Clin. 2018; 68(1): 31-54.
|
| [15] |
World Health Organization (WHO). Tobacco Control in Bangladesh. Policies and Challenges. Available at:
https://www.who.int/news-room/fact-sheets/detail/tobacco
|
| [16] |
Abu-Abid, S., Szold, A., & Klausner, J. (2002). Obesity and cancer. Journal of medicine, 33(1-4), 73–86.
|
| [17] |
Environmental Health Perspective. Air Pollution and Cancer Risk in Dhaka. 2022; 130(4): 410-422.
|
| [18] |
Sung H, Ferlay J, Siegel RL et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71: 209-249.
|
| [19] |
Hussain S. M. (2013). Comprehensive update on cancer scenario of Bangladesh. South Asian journal of cancer, 2(4), 279–284.
https://doi.org/10.4103/2278-330X.119901
|
| [20] |
WHO. Cancer Prevention Strategies: Global initiatives and progress.
|
| [21] |
ACS. The economic cost of tobacco uses in Bangladesh.
|
| [22] |
IARC. Tobacco smoke and cancer risk.
|
| [23] |
WHO. Global tobacco report 2022.
|
| [24] |
Torre LA, Siegel RL, Ward EM et al. Global cancer incidence and mortality rates and trends—an update. Cancer Epidemiol Biomarkers Prev 2016; 25: 16-27.
|
| [25] |
NCI. Alcohol and cancer risk: A review of evidence.
|
| [26] |
Meine, G. C., Picon, R. V., Espírito Santo, P. A., & Sander, G. B. (2024). Ultra-Processed Food Consumption and Gastrointestinal Cancer Risk: A Systematic Review and Meta-Analysis. The American journal of gastroenterology, 119(6), 1056–1065.
|
| [27] |
BMC Cancer. The role of obesity in cancer risk: Evidence from Bangladesh. BMC Cancer 2021; 21: 745.
|
| [28] |
Asian Pac J Cancer Prev. The role of lifestyle factors in cancer prevention in South Asia. Asian Pac J Cancer Prev 2022; 23: 1123-1130.
|
Cite This Article
-
APA Style
Marof, A., Al-Amin, M., Sultana, M. S., Konika, K. N., Roky, M. S., et al. (2025). Assessment of the Relationship Between Cancer Prevalence and Lifestyle Risk Factors in Bangladesh: A Cross-Sectional Study at a National Cancer Hospital. Science Journal of Public Health, 13(4), 196-204. https://doi.org/10.11648/j.sjph.20251304.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Marof, A.; Al-Amin, M.; Sultana, M. S.; Konika, K. N.; Roky, M. S., et al. Assessment of the Relationship Between Cancer Prevalence and Lifestyle Risk Factors in Bangladesh: A Cross-Sectional Study at a National Cancer Hospital. Sci. J. Public Health 2025, 13(4), 196-204. doi: 10.11648/j.sjph.20251304.14
Copy
|
Download
AMA Style
Marof A, Al-Amin M, Sultana MS, Konika KN, Roky MS, et al. Assessment of the Relationship Between Cancer Prevalence and Lifestyle Risk Factors in Bangladesh: A Cross-Sectional Study at a National Cancer Hospital. Sci J Public Health. 2025;13(4):196-204. doi: 10.11648/j.sjph.20251304.14
Copy
|
Download
-
@article{10.11648/j.sjph.20251304.14,
author = {Amanullah Marof and Md. Al-Amin and Mst. Sabiha Sultana and Kamrun Nahar Konika and Md. Shaheduzzaman Roky and Shahat Shiddiqe and Asad Ud-Daula},
title = {Assessment of the Relationship Between Cancer Prevalence and Lifestyle Risk Factors in Bangladesh: A Cross-Sectional Study at a National Cancer Hospital
},
journal = {Science Journal of Public Health},
volume = {13},
number = {4},
pages = {196-204},
doi = {10.11648/j.sjph.20251304.14},
url = {https://doi.org/10.11648/j.sjph.20251304.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjph.20251304.14},
abstract = {Cancer is a growing public health concern worldwide, particularly in low and middle-income countries such as Bangladesh. Lifestyle factors, including dietary habits, smoking, and obesity, play a crucial role in cancer development. To provide updated insights for risk prediction and public health interventions this study aims is to collect and analyze patient data from the National Institute of Cancer Research and Hospital (NICRH) to identify and evaluate the association of lifestyle risk factors with cancer incidence in Bangladesh. This study investigates the prevalence of different cancers and their association with modifiable risk factors among Bangladeshi cancer patients. A cross-sectional study was conducted at the NICRH where two-thirds (201) of the cancer patients’ data were involving to dominate the result. Data were collected using a structured questionnaire, and logistic regression analysis was performed by SPSS (Statistical Package for the Social Sciences), version 26 (SPSS Inc., Chicago, IL, USA) to assess the relationship between cancer and lifestyle factors. The findings indicate that breast cancer (18.9%) was the most prevalent cancer, followed by lung (15.9%), stomach (12.9%), cervix uteri (12.9%), and esophageal cancer (6.5%). Lung cancer was most common in males (27.5%), whereas breast cancer was the most frequent in females (34.5%). The highest cancer incidents were observed in individuals aged 40-60 years. Smoking showed a significant association with lung cancer (OR: 1.230, P = 0.001), while obesity was strongly associated with breast cancer (OR: 1.43, P = 0.006). These findings highlight the urgent need for public health intervention, including tobacco control, obesity prevention, dietary modifications, and expanded cancer screening programs, to reduce cancer incidence in Bangladesh. Addressing these risk factors through policy-driven strategies and awareness initiatives could significantly improve cancer prevention and early detection efforts.},
year = {2025}
}
Copy
|
Download
-
TY - JOUR
T1 - Assessment of the Relationship Between Cancer Prevalence and Lifestyle Risk Factors in Bangladesh: A Cross-Sectional Study at a National Cancer Hospital
AU - Amanullah Marof
AU - Md. Al-Amin
AU - Mst. Sabiha Sultana
AU - Kamrun Nahar Konika
AU - Md. Shaheduzzaman Roky
AU - Shahat Shiddiqe
AU - Asad Ud-Daula
Y1 - 2025/07/31
PY - 2025
N1 - https://doi.org/10.11648/j.sjph.20251304.14
DO - 10.11648/j.sjph.20251304.14
T2 - Science Journal of Public Health
JF - Science Journal of Public Health
JO - Science Journal of Public Health
SP - 196
EP - 204
PB - Science Publishing Group
SN - 2328-7950
UR - https://doi.org/10.11648/j.sjph.20251304.14
AB - Cancer is a growing public health concern worldwide, particularly in low and middle-income countries such as Bangladesh. Lifestyle factors, including dietary habits, smoking, and obesity, play a crucial role in cancer development. To provide updated insights for risk prediction and public health interventions this study aims is to collect and analyze patient data from the National Institute of Cancer Research and Hospital (NICRH) to identify and evaluate the association of lifestyle risk factors with cancer incidence in Bangladesh. This study investigates the prevalence of different cancers and their association with modifiable risk factors among Bangladeshi cancer patients. A cross-sectional study was conducted at the NICRH where two-thirds (201) of the cancer patients’ data were involving to dominate the result. Data were collected using a structured questionnaire, and logistic regression analysis was performed by SPSS (Statistical Package for the Social Sciences), version 26 (SPSS Inc., Chicago, IL, USA) to assess the relationship between cancer and lifestyle factors. The findings indicate that breast cancer (18.9%) was the most prevalent cancer, followed by lung (15.9%), stomach (12.9%), cervix uteri (12.9%), and esophageal cancer (6.5%). Lung cancer was most common in males (27.5%), whereas breast cancer was the most frequent in females (34.5%). The highest cancer incidents were observed in individuals aged 40-60 years. Smoking showed a significant association with lung cancer (OR: 1.230, P = 0.001), while obesity was strongly associated with breast cancer (OR: 1.43, P = 0.006). These findings highlight the urgent need for public health intervention, including tobacco control, obesity prevention, dietary modifications, and expanded cancer screening programs, to reduce cancer incidence in Bangladesh. Addressing these risk factors through policy-driven strategies and awareness initiatives could significantly improve cancer prevention and early detection efforts.
VL - 13
IS - 4
ER -
Copy
|
Download