Circulating tumor DNA (ctDNA) has emerged as a transformative biomarker in tumor precision medicine, enabling noninvasive insights into tumor genetics and dynamics across the entire disease continuum from diagnosis to treatment monitoring. Over the past two decades, significant advances from early cell-free DNA discovery to sophisticated high-sensitivity digital PCR and next-generation sequencing technologies have successfully facilitated the accurate detection and precise quantification of ctDNA at extremely low variant allele frequencies in peripheral blood samples. Comprehensive mechanistic studies reveal that ctDNA release reflects multiple biological processes including tumor cell apoptosis, necrosis, active secretion mechanisms, and complex microenvironmental influences that affect circulating DNA stability. Recent analytical innovations—including advanced droplet digital PCR platforms, targeted deep sequencing approaches, sophisticated variant-filtering algorithms, miniaturized microfluidic devices, and integrated artificial intelligence/machine learning pipelines—have substantially enhanced both sensitivity and specificity for ctDNA detection across diverse clinical scenarios. Current clinical applications span multiple domains including early cancer detection, minimal residual disease assessment, real-time tumor progression monitoring, comprehensive heterogeneity profiling, and personalized treatment guidance across multiple cancer types including colorectal, lung, breast, pancreatic, melanoma, hematologic, and gynecologic malignancies. Ongoing collaborative efforts in standardization protocols, analytical optimization, and comprehensive ethical governance frameworks aim to systematically address persistent challenges including low ctDNA abundance in early-stage disease, false positives/negatives, patient data privacy concerns, and ensuring equitable global access to these advanced diagnostic technologies. Future research directions emphasize developing ultrasensitive nanotechnology platforms, implementing long-read sequencing methodologies, advancing multi-omics integration strategies, and deploying AI-driven interpretation systems to fully realize ctDNA's transformative potential in precision oncology.
| Published in | Science Journal of Clinical Medicine (Volume 14, Issue 4) |
| DOI | 10.11648/j.sjcm.20251404.12 |
| Page(s) | 78-94 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2025. Published by Science Publishing Group |
ctDNA, Liquid Biopsy, Digital PCR, Next-generation Sequencing, Minimal Residual Disease, Tumor Heterogeneity, Precision Oncology
cfDNA | Cell-Free DNA |
ctDNA | Circulating Tumor DNA |
PCR | Polymerase Chain Reaction |
dPCR | Digital PCR |
ddPCR | Droplet Digital PCR |
NGS | Next-Generation Sequencing |
VAF | Variant Allele Frequency |
AI | Artificial Intelligence |
ML | Machine Learning |
CRC | Colorectal Cancer |
NSCLC | Non-Small Cell Lung Cancer |
SCLC | Small-Cell Lung Cancer |
HCC | Hepatocellular Carcinoma |
CTCs | Circulating Tumor Cells |
CNV | Copy-Number Variation |
SNV | Single-Nucleotide Variant |
indel | Insertion/Deletion |
CHIP | Clonal Hematopoiesis of Indeterminate Potential |
EGFR | Epidermal Growth Factor Receptor |
KRAS | Kirsten Rat Sarcoma Viral Oncogene Homolog |
ESR1 | Estrogen Receptor 1 |
BRAF | B-Raf Proto-Oncogene |
TP53 | Tumor Protein p53 |
RB1 | Retinoblastoma 1 |
DDR | DNA Damage Response |
TMTV | Total Metabolic Tumor Volume |
TKIs | Tyrosine Kinase Inhibitors |
OS | Overall Survival |
PFS | Progression-Free Survival |
MRD | Minimal Residual Disease |
WES | Whole Exome Sequencing |
PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
AI/ML | Artificial Intelligence/Machine Learning |
SERD | Selective Estrogen Receptor Degrader |
CA-125 | Cancer Antigen 125 |
PET-CT | Positron Emission Tomography–Computed Tomography |
TKIs | Tyrosine Kinase Inhibitors |
TER | Tumor Clonal Evolution Rate |
HSP90AA1 | Heat Shock Protein 90 Alpha Family A Member 1 |
POTS | Postural Orthostatic Tachycardia Syndrome |
SES | Socioeconomic Status |
VR | Virtual Reality |
| [1] | Auer Martina, Belic Jelena, Heitzer Ellen, et al: Advances in Circulating Tumor DNA Analysis. ADVANCES IN CLINICAL CHEMISTRY 2017. |
| [2] | Roosan Moom R, Mambetsariev Isa, Pharaon Rebecca, et al: Usefulness of Circulating Tumor DNA in Identifying Somatic Mutations and Tracking Tumor Evolution in Patients with Non-Small Cell Lung Cancer. CHEST 2021. |
| [3] | Chen Qian, Lang Jing-He, Wang Shu, et al: Circulating Cell-Free DNA or Circulating Tumor DNA in the Management of Ovarian and Endometrial Cancer. ONCOTARGETS AND THERAPY 2020. |
| [4] | Shulman David S, Crompton Brian D: Using Liquid Biopsy in the Treatment of Patient with OS. ADVANCES IN EXPERIMENTAL MEDICINE AND BIOLOGY 2020. |
| [5] | Aikata Hiroshi, Akamatsu Shusuke, Chayama Kazuaki, et al: eVIDENCE: a practical variant filtering for low-frequency variants detection in cell-free DNA. SCIENTIFIC REPORTS 2019. |
| [6] | Nishida Naoshi, Kudo Masatoshi: Alteration of Epigenetic Profile in Human Hepatocellular Carcinoma and Its Clinical Implications. LIVER CANCER 2015. |
| [7] | Ramalingam Naveen, Jeffrey Stefanie S: Future of Liquid Biopsies With Growing Technological and Bioinformatics Studies: Opportunities and Challenges in Discovering Tumor Heterogeneity With Single-Cell Level Analysis. CANCER JOURNAL 2018. |
| [8] | Dardiotis Efthimios, Grivas Petros D, Mentis Alexios-Fotios A, et al: Circulating tumor cells as Trojan Horse for understanding, preventing, and treating cancer: a critical appraisal. CELLULAR AND MOLECULAR LIFE SCIENCES 2020. |
| [9] | Pal Sumanta K, Sonpavde Guru, Agarwal Neeraj, et al: Evolution of Circulating Tumor DNA Profile from First-line to Subsequent Therapy in Metastatic Renal Cell Carcinoma. EUROPEAN UROLOGY 2017. |
| [10] | Papadopoulos Nickolas: Pathophysiology of ctDNA Release into the Circulation and Its Characteristics: What Is Important for Clinical Applications. 2019. |
| [11] | Wang Peilu, Bahreini Amir, Gyanchandani Rekha, et al: Sensitive Detection of Mono- and Polyclonal ESR1 Mutations in Primary Tumors, Metastatic Lesions, and Cell-Free DNA of Breast Cancer Patients. CLINICAL CANCER RESEARCH 2015. |
| [12] | Takai Erina, Totoki Yasushi, Nakamura Hiromi, et al: Clinical utility of circulating tumor DNA for molecular assessment in pancreatic cancer. SCIENTIFIC REPORTS 2015. |
| [13] | Sherwood James L, Corcoran Claire, Brown Helen, et al: Optimised Pre-Analytical Methods Improve KRAS Mutation Detection in Circulating Tumour DNA (ctDNA) from Patients with Non-Small Cell Lung Cancer (NSCLC). PLOS ONE 2016. |
| [14] | Dwivedi Dhruva J, Fox-Robichaud Alison E, Gould Travis J, et al: A microfluidic device for rapid quantification of cell-free DNA in patients with severe sepsis. LAB ON A CHIP 2015. |
| [15] | Morelli M P, Overman M J, Dasari A, et al: Characterizing the patterns of clonal selection in circulating tumor DNA from patients with colorectal cancer refractory to anti-EGFR treatment. ANNALS OF ONCOLOGY 2015. |
| [16] | Sato Kei A, Hachiya Tsuyoshi, Iwaya Takeshi, et al: Individualized Mutation Detection in Circulating Tumor DNA for Monitoring Colorectal Tumor Burden Using a Cancer-Associated Gene Sequencing Panel. PLOS ONE 2016. |
| [17] | Yang Xue, Zhuo Minglei, Ye Xin, et al: Quantification of mutant alleles in circulating tumor DNA can predict survival in lung cancer. 2016. |
| [18] | Schiavon Gaia, Hrebien Sarah, Garcia-Murillas Isaac, et al: Analysis of ESR1 mutation in circulating tumor DNA demonstrates evolution during therapy for metastatic breast cancer. SCIENCE TRANSLATIONAL MEDICINE 2015. |
| [19] | Fernandez-Cuesta Lynnette, Perdomo Sandra, Avogbe Patrice H, et al: Identification of Circulating Tumor DNA for the Early Detection of Small-cell Lung Cancer. EBIOMEDICINE 2016. |
| [20] | Li Shunying, Li Yudong, Wei Wei, et al: Dynamic ctDNA tracking stratifies relapse risk for triple negative breast cancer patients receiving neoadjuvant chemotherapy. NATURE COMMUNICATIONS 2025. |
| [21] | Ciardullo Carmela, Tobalina Luis, Carr T Hedley, et al: Early ctDNA dynamics inform first-line therapy in patients with extensive-stage small cell lung cancer. CLINICAL CANCER RESEARCH 2025. |
| [22] | Vimalathas Gayaththri, Hansen Marcus Høy, Cédile Oriane Marie Louise, et al: Monitoring ctDNA in Aggressive B-cell Lymphoma: A Prospective Correlative Study of ctDNA Kinetics and PET-CT Metrics. BLOOD ADVANCES 2025. |
| [23] | Tatalovic Stefan, Doleschal Bernhard, Kupferthaler Alexander, et al: Circulating Tumor DNA (ctDNA) Dynamics Predict Early Response to Treatment in Metastasized Gastroesophageal Cancer (mGEC) After 2 Weeks of Systemic Treatment. CANCERS 2024. |
| [24] | Aldea Cornel, Lupan Iulia: Liquid biopsy challenge and hope in colorectal cancer. EXPERT REVIEW OF MOLECULAR DIAGNOSTICS 2019. |
| [25] | Rong Guohua, Yi Zongbi, Ma Fei, et al: DNA damage response as a prognostic indicator in metastatic breast cancer via mutational analysis. ANNALS OF TRANSLATIONAL MEDICINE 2021. |
| [26] | Jiang Xiu-Feng, Zhang Bo-Miao, Du Fen-Qi, et al: Exploring biomarkers for prognosis and neoadjuvant chemosensitivity in rectal cancer: Multi-omics and ctDNA sequencing collaboration. FRONTIERS IN IMMUNOLOGY 2022. |
| [27] | Lv Dan, Lan Bo, Guo Qihan, et al: Exploration of the clonal evolution and construction of the tumor clonal evolution rate as a prognostic indicator in metastatic breast cancer. BMC MEDICINE 2025. |
| [28] | Lee Jee Soo, Han Youngmin, Yun Won Gun, et al: Parallel Analysis of Pre- and Postoperative Circulating Tumor DNA and Matched Tumor Tissues in Resectable Pancreatic Ductal Adenocarcinoma: A Prospective Cohort Study. CLINICAL CHEMISTRY 2022. |
| [29] | Zhang Hehua, Gao Hongmin, Mu Wendi, et al: Electrochemical-Fluorescent Bimodal Biosensor Based on Dual CRISPR-Cas12a Multiple Cascade Amplification for ctDNA Detection. ANALYTICAL CHEMISTRY 2024. |
| [30] | Bièche Ivan, Carrière Christelle, Cyrta Joanna, et al: Highly Sensitive Detection Method of DICER1 Tumor Hotspot Mutations by Drop-off Droplet Digital PCR. CLINICAL CHEMISTRY 2021. |
| [31] | Battaglin Francesca, Lenz Heinz-Josef: Clinical Applications of Circulating Tumor DNA Profiling in GI Cancers. JCO ONCOLOGY PRACTICE 2024. |
| [32] | Alsop Kathryn, Arnau Gisela Mir, Bowtell David D, et al: Circulating Tumor DNA Analysis and Functional Imaging Provide Complementary Approaches for Comprehensive Disease Monitoring in Metastatic Melanoma. JCO PRECISION ONCOLOGY 2022. |
| [33] | Zaikova Elena, Cheng Brian Y C, Cerda Viviana, et al: Circulating tumour mutation detection in triple-negative breast cancer as an adjunct to tissue response assessment. NPJ BREAST CANCER 2024. |
| [34] | Wang Hsin-Yi, Ho Chao-Chi, Lin Yen-Ting, et al: Comprehensive Genomic Analysis of Patients With Non-Small-Cell Lung Cancer Using Blood-Based Circulating Tumor DNA Assay: Findings From the BFAST Database of a Single Center in Taiwan. JCO PRECISION ONCOLOGY 2024. |
| [35] | Eckhoff Austin M, Kanu Elishama, Fletcher Ashley, et al: Initial Report: Personalized Circulating Tumor DNA and Survival in Patients with Resectable Pancreatic Cancer. ANNALS OF SURGICAL ONCOLOGY 2024. |
| [36] | Wang De-Shen, Yang Hui, Liu Xiao-Yun, et al: Dynamic monitoring of circulating tumor DNA to predict prognosis and efficacy of adjuvant chemotherapy after resection of colorectal liver metastases. THERANOSTICS 2021. |
| [37] | Cani Andi K, Hayes Daniel F: Breast Cancer Circulating Tumor Cells: Current Clinical Applications and Future Prospects. CLINICAL CHEMISTRY 2024. |
| [38] | Chen Kezhong, Zhao Heng, Yang Fan, et al: Dynamic changes of circulating tumour DNA in surgical lung cancer patients: protocol for a prospective observational study. BMJ OPEN 2018. |
| [39] | Liu Lipeng, Zong Suyu, Zhang Aoli, et al: Early Detection of Molecular Residual Disease and Risk Stratification for Children with Acute Myeloid Leukemia via Circulating Tumor DNA. CLINICAL CANCER RESEARCH 2024. |
| [40] | Baenke Franziska, Brady Ged, Dhomen Nathalie, et al: Application of Sequencing, Liquid Biopsies, and Patient-Derived Xenografts for Personalized Medicine in Melanoma. CANCER DISCOVERY 2015. |
| [41] | Pereira Elena, Camacho-Vanegas Olga, Anand Sanya, et al: Personalized Circulating Tumor DNA Biomarkers Dynamically Predict Treatment Response and Survival In Gynecologic Cancers. PLOS ONE 2015. |
| [42] | Tjensvoll Kjersti, Lapin Morten, Buhl Tove, et al: Clinical relevance of circulating KRAS mutated DNA in plasma from patients with advanced pancreatic cancer. MOLECULAR ONCOLOGY 2016. |
| [43] | Park Cheol-Kyu, Cho Hyun-Ju, Choi Yoo-Duk, et al: A Phase II Trial of Osimertinib in the Second-Line Treatment of Non-small Cell Lung Cancer with the EGFR T790M Mutation, Detected from Circulating Tumor DNA: LiquidLung-O-Cohort 2. CANCER RESEARCH AND TREATMENT 2018. |
| [44] | Birkenkamp-Demtröder Karin, Christensen Emil, Nordentoft Iver, et al: Monitoring Treatment Response and Metastatic Relapse in Advanced Bladder Cancer by Liquid Biopsy Analysis. EUROPEAN UROLOGY 2017. |
| [45] | Hrebien S, Citi V, GarciaMurillas I, et al: Early ctDNA dynamics as a surrogate for progression-free survival in advanced breast cancer in the BEECH trial. ANNALS OF ONCOLOGY 2019. |
| [46] | Nakamura Tomomi, Nakashima Chiho, Komiya Kazutoshi, et al: Mechanisms of acquired resistance to afatinib clarified with liquid biopsy. PLOS ONE 2018. |
| [47] | Bardelli Alberto, Bartolini Alice, Bianchi Andrea Sartore, et al: Acquired Resistance to the TRK Inhibitor Entrectinib in Colorectal Cancer. CANCER DISCOVERY 2015. |
| [48] | Daga Haruko, Imamura Fumio, Inoue Takako, et al: Diagnostic Accuracy of Noninvasive Genotyping of EGFR in Lung Cancer Patients by Deep Sequencing of Plasma Cell-Free DNA. CLINICAL CHEMISTRY 2015. |
| [49] | Gilson Pauline, Saurel Chloé, Salleron Julia, et al: Evaluation of the Idylla ctEGFR mutation assay to detect EGFR mutations in plasma from patients with non-small cell lung cancers. SCIENTIFIC REPORTS 2021. |
| [50] | Toro Patricia Valda, Erlanger Bracha, Beaver Julia A, et al: Comparison of cell stabilizing blood collection tubes for circulating plasma tumor DNA. CLINICAL BIOCHEMISTRY 2015. |
| [51] | Whiley Phillip J, de la Hoya Miguel, Thomassen Mads, et al: Comparison of mRNA splicing assay protocols across multiple laboratories: recommendations for best practice in standardized clinical testing. CLINICAL CHEMISTRY 2013. |
| [52] | Godsey James H, Silvestro Angela, Barrett J Carl, et al: Generic Protocols for the Analytical Validation of Next-Generation Sequencing-Based ctDNA Assays: A Joint Consensus Recommendation of the BloodPAC's Analytical Variables Working Group. CLINICAL CHEMISTRY 2020. |
| [53] | Müller Petra, Sell Christian, Hadrys Thorsten, et al: Inter-laboratory study on standardized MPS libraries: evaluation of performance, concordance, and sensitivity using mixtures and degraded DNA. INTERNATIONAL JOURNAL OF LEGAL MEDICINE 2019. |
| [54] | Boissan Mathieu, Denis Jérôme Alexandre, Guenoun Alexandre, et al: [Moving towards a personalized oncology: The contribution of genomic techniques and artificial intelligence in the use of circulating tumor biomarkers]. BULLETIN DU CANCER 2022. |
| [55] | Kasi Pashtoon Murtaza, Sawyer Sarah, Guilford Jessica, et al: BESPOKE study protocol: a multicentre, prospective observational study to evaluate the impact of circulating tumour DNA guided therapy on patients with colorectal cancer. BMJ OPEN 2021. |
| [56] | Akolekar R, Gil M M, Nicolaides K H, et al: Clinical implementation of routine screening for fetal trisomies in the UK NHS: cell-free DNA test contingent on results from first-trimester combined test. ULTRASOUND IN OBSTETRICS & GYNECOLOGY 2015. |
| [57] | Fiala Clare, Diamandis Eleftherios P: Utility of circulating tumor DNA in cancer diagnostics with emphasis on early detection. BMC MEDICINE 2018. |
| [58] | Fu Xin, Yang Mei, Zhang He, et al: Microfluidic bead-based biosensor: Ultrasensitive ctDNA detection based on duplex-functional split-DNAzyme and dendritic enzyme-free signal amplification. ANALYTICAL BIOCHEMISTRY 2024. |
| [59] | Gilson Pauline: Enrichment and Analysis of ctDNA. 2019. |
| [60] | She Wei, Garitaonaindia Yago, Lin Yun: The latest advances in liquid biopsy for lung cancer-a narrative review. TRANSLATIONAL LUNG CANCER RESEARCH 2024. |
| [61] | Hussain Md Sadique, Rejili Mokhtar, Khan Amna, et al: AI-powered liquid biopsy for early detection of gastrointestinal cancers. CLINICA CHIMICA ACTA 2025. |
| [62] | Yu Baofa, Shao Shengwen, Ma Wenxue: Frontiers in pancreatic cancer on biomarkers, microenvironment, and immunotherapy. CANCER LETTERS 2024. |
| [63] | Prelaj Arsela, Ganzinelli Monica, Provenzano Leonardo, et al: APOLLO 11 Project, Consortium in Advanced Lung Cancer Patients Treated With Innovative Therapies: Integration of Real-World Data and Translational Research. CLINICAL LUNG CANCER 2024. |
| [64] | Qiu Peng, Yu Xiaopeng, Zheng Fushuang, et al: Advancements in liquid biopsy for breast Cancer: Molecular biomarkers and clinical applications. CANCER TREATMENT REVIEWS 2025. |
| [65] | Boldrini Luca, Chiloiro Giuditta, Di Franco Silvia, et al: MOREOVER: multiomics MR-guided radiotherapy optimization in locally advanced rectal cancer. RADIATION ONCOLOGY 2024. |
| [66] | Tie J, Kinde I, Wang Y, et al: Circulating tumor DNA as an early marker of therapeutic response in patients with metastatic colorectal cancer. ANNALS OF ONCOLOGY 2015. |
APA Style
Ruan, T., Li, M., Yan, Q., Zhang, J., Huang, Y. (2025). Fundamentals of ctDNA Biomarkers in Tumor Precision Medicine. Science Journal of Clinical Medicine, 14(4), 78-94. https://doi.org/10.11648/j.sjcm.20251404.12
ACS Style
Ruan, T.; Li, M.; Yan, Q.; Zhang, J.; Huang, Y. Fundamentals of ctDNA Biomarkers in Tumor Precision Medicine. Sci. J. Clin. Med. 2025, 14(4), 78-94. doi: 10.11648/j.sjcm.20251404.12
AMA Style
Ruan T, Li M, Yan Q, Zhang J, Huang Y. Fundamentals of ctDNA Biomarkers in Tumor Precision Medicine. Sci J Clin Med. 2025;14(4):78-94. doi: 10.11648/j.sjcm.20251404.12
@article{10.11648/j.sjcm.20251404.12,
author = {Tian Ruan and Minghang Li and Qiaohua Yan and Juan Zhang and Yue Huang},
title = {Fundamentals of ctDNA Biomarkers in Tumor Precision Medicine
},
journal = {Science Journal of Clinical Medicine},
volume = {14},
number = {4},
pages = {78-94},
doi = {10.11648/j.sjcm.20251404.12},
url = {https://doi.org/10.11648/j.sjcm.20251404.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sjcm.20251404.12},
abstract = {Circulating tumor DNA (ctDNA) has emerged as a transformative biomarker in tumor precision medicine, enabling noninvasive insights into tumor genetics and dynamics across the entire disease continuum from diagnosis to treatment monitoring. Over the past two decades, significant advances from early cell-free DNA discovery to sophisticated high-sensitivity digital PCR and next-generation sequencing technologies have successfully facilitated the accurate detection and precise quantification of ctDNA at extremely low variant allele frequencies in peripheral blood samples. Comprehensive mechanistic studies reveal that ctDNA release reflects multiple biological processes including tumor cell apoptosis, necrosis, active secretion mechanisms, and complex microenvironmental influences that affect circulating DNA stability. Recent analytical innovations—including advanced droplet digital PCR platforms, targeted deep sequencing approaches, sophisticated variant-filtering algorithms, miniaturized microfluidic devices, and integrated artificial intelligence/machine learning pipelines—have substantially enhanced both sensitivity and specificity for ctDNA detection across diverse clinical scenarios. Current clinical applications span multiple domains including early cancer detection, minimal residual disease assessment, real-time tumor progression monitoring, comprehensive heterogeneity profiling, and personalized treatment guidance across multiple cancer types including colorectal, lung, breast, pancreatic, melanoma, hematologic, and gynecologic malignancies. Ongoing collaborative efforts in standardization protocols, analytical optimization, and comprehensive ethical governance frameworks aim to systematically address persistent challenges including low ctDNA abundance in early-stage disease, false positives/negatives, patient data privacy concerns, and ensuring equitable global access to these advanced diagnostic technologies. Future research directions emphasize developing ultrasensitive nanotechnology platforms, implementing long-read sequencing methodologies, advancing multi-omics integration strategies, and deploying AI-driven interpretation systems to fully realize ctDNA's transformative potential in precision oncology.
},
year = {2025}
}
TY - JOUR T1 - Fundamentals of ctDNA Biomarkers in Tumor Precision Medicine AU - Tian Ruan AU - Minghang Li AU - Qiaohua Yan AU - Juan Zhang AU - Yue Huang Y1 - 2025/10/10 PY - 2025 N1 - https://doi.org/10.11648/j.sjcm.20251404.12 DO - 10.11648/j.sjcm.20251404.12 T2 - Science Journal of Clinical Medicine JF - Science Journal of Clinical Medicine JO - Science Journal of Clinical Medicine SP - 78 EP - 94 PB - Science Publishing Group SN - 2327-2732 UR - https://doi.org/10.11648/j.sjcm.20251404.12 AB - Circulating tumor DNA (ctDNA) has emerged as a transformative biomarker in tumor precision medicine, enabling noninvasive insights into tumor genetics and dynamics across the entire disease continuum from diagnosis to treatment monitoring. Over the past two decades, significant advances from early cell-free DNA discovery to sophisticated high-sensitivity digital PCR and next-generation sequencing technologies have successfully facilitated the accurate detection and precise quantification of ctDNA at extremely low variant allele frequencies in peripheral blood samples. Comprehensive mechanistic studies reveal that ctDNA release reflects multiple biological processes including tumor cell apoptosis, necrosis, active secretion mechanisms, and complex microenvironmental influences that affect circulating DNA stability. Recent analytical innovations—including advanced droplet digital PCR platforms, targeted deep sequencing approaches, sophisticated variant-filtering algorithms, miniaturized microfluidic devices, and integrated artificial intelligence/machine learning pipelines—have substantially enhanced both sensitivity and specificity for ctDNA detection across diverse clinical scenarios. Current clinical applications span multiple domains including early cancer detection, minimal residual disease assessment, real-time tumor progression monitoring, comprehensive heterogeneity profiling, and personalized treatment guidance across multiple cancer types including colorectal, lung, breast, pancreatic, melanoma, hematologic, and gynecologic malignancies. Ongoing collaborative efforts in standardization protocols, analytical optimization, and comprehensive ethical governance frameworks aim to systematically address persistent challenges including low ctDNA abundance in early-stage disease, false positives/negatives, patient data privacy concerns, and ensuring equitable global access to these advanced diagnostic technologies. Future research directions emphasize developing ultrasensitive nanotechnology platforms, implementing long-read sequencing methodologies, advancing multi-omics integration strategies, and deploying AI-driven interpretation systems to fully realize ctDNA's transformative potential in precision oncology. VL - 14 IS - 4 ER -
Basic and Pharmacy Department, Yunnan Medical Health College, Kunming, China
Basic and Pharmacy Department, Yunnan Medical Health College, Kunming, China
Basic and Pharmacy Department, Yunnan Medical Health College, Kunming, China
Clinical Medical College, Yunnan Medical Health College, Kunming, China
Basic and Pharmacy Department, Yunnan Medical Health College, Kunming, China
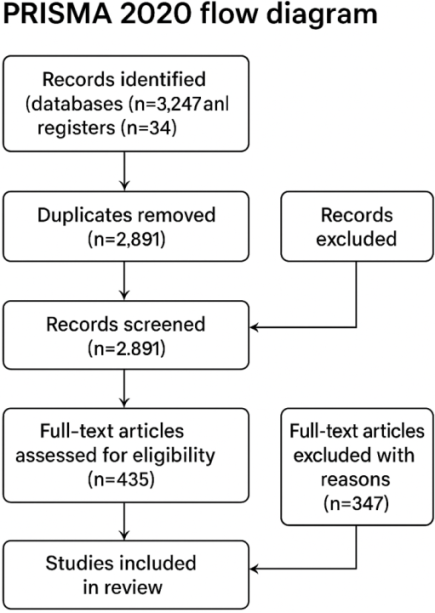
Figure 1. Complete PRISMA 2020 flow diagram with realistic numbers for ctDNA systematic review.
Figure 2. Schematic timeline of ctDNA biomarker discovery.
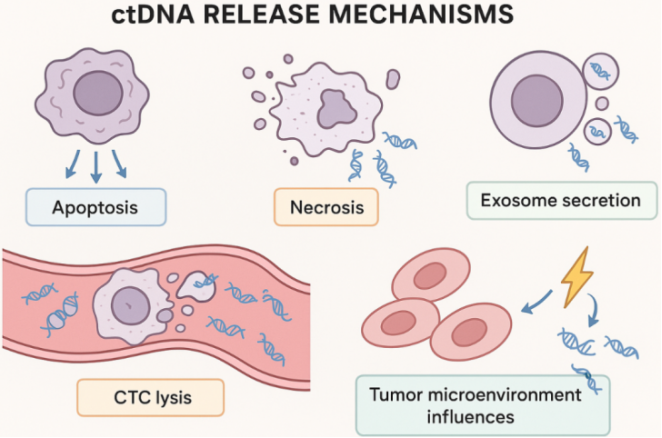
Figure 3. Mechanisms of ctDNA release in tumor biology.
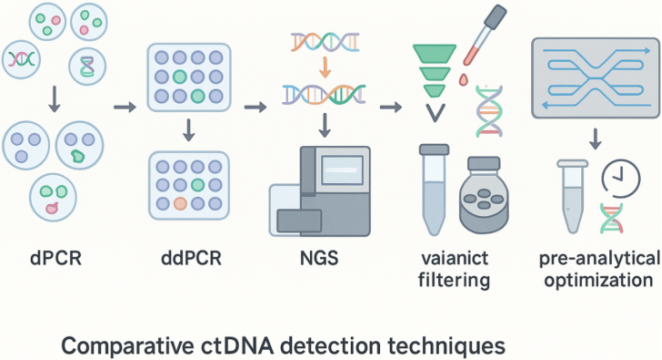
Figure 4. Overview of analytical techniques for ctDNA detection.
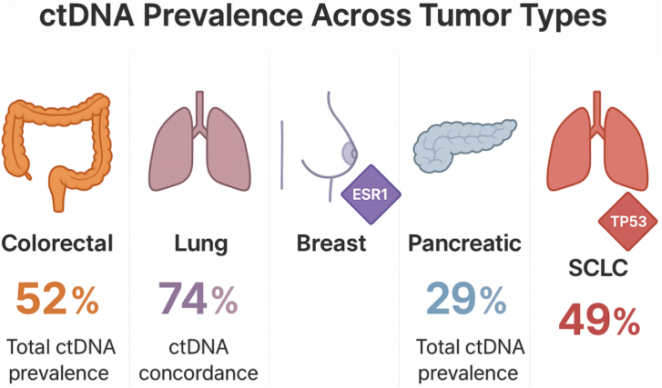
Figure 5. Prevalence of ctDNA in different tumor types.
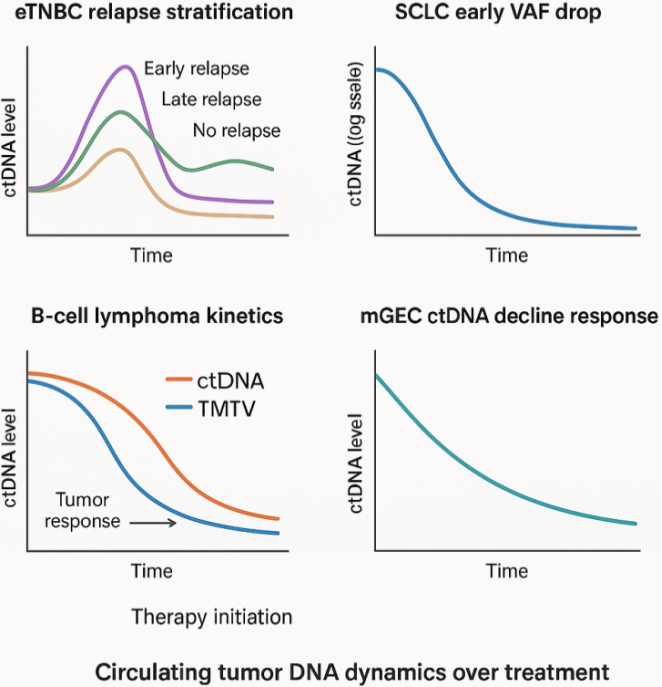
Figure 6. Pathophysiological insights into ctDNA dynamics.
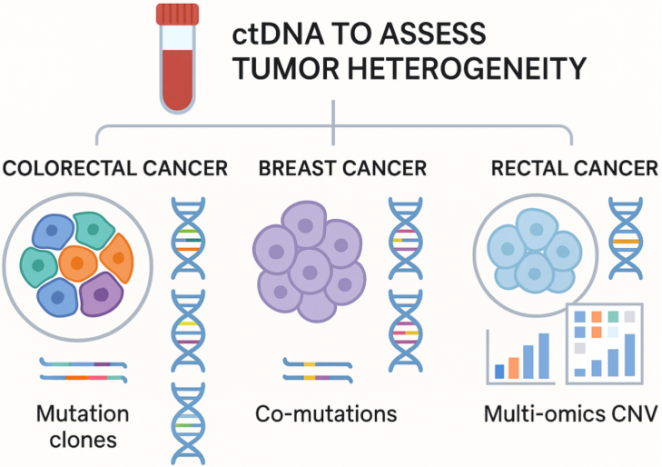
Figure 7. ctDNA as indicator of tumor heterogeneity.
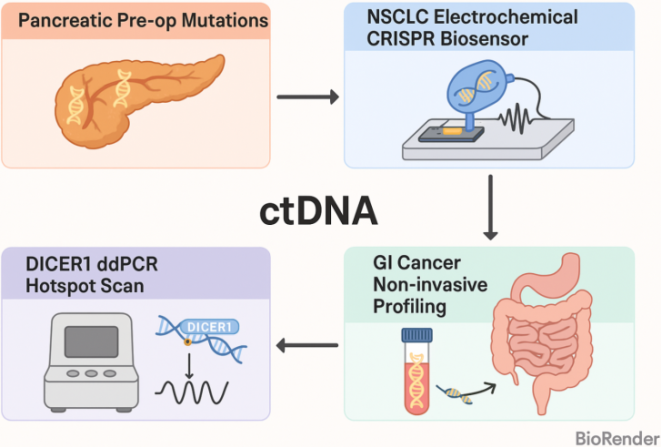
Figure 8. ctDNA for Monitoring Tumor Progression.
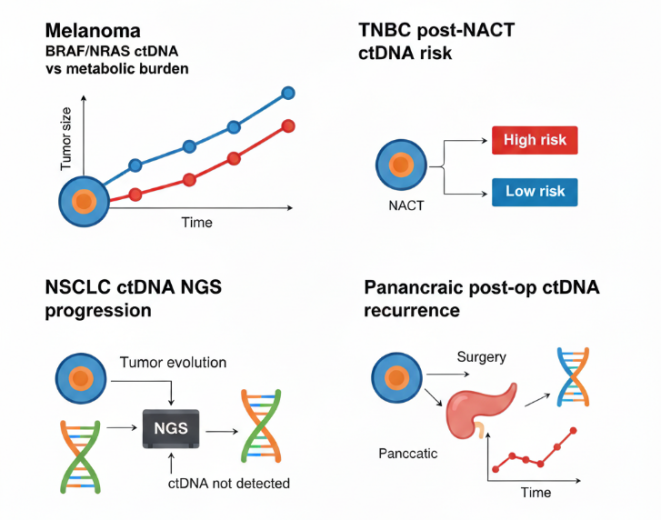
Figure 9. ctDNA for monitoring tumor progression.
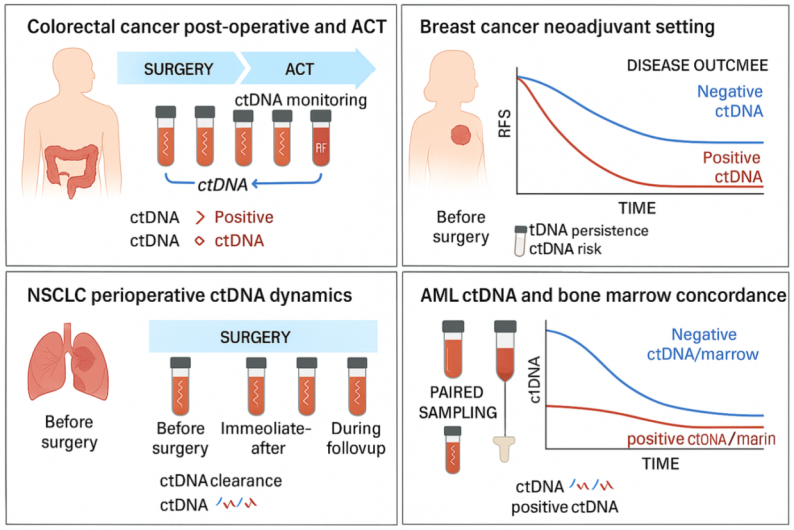
Figure 10. ctDNA in Minimal Residual Disease Assessment.
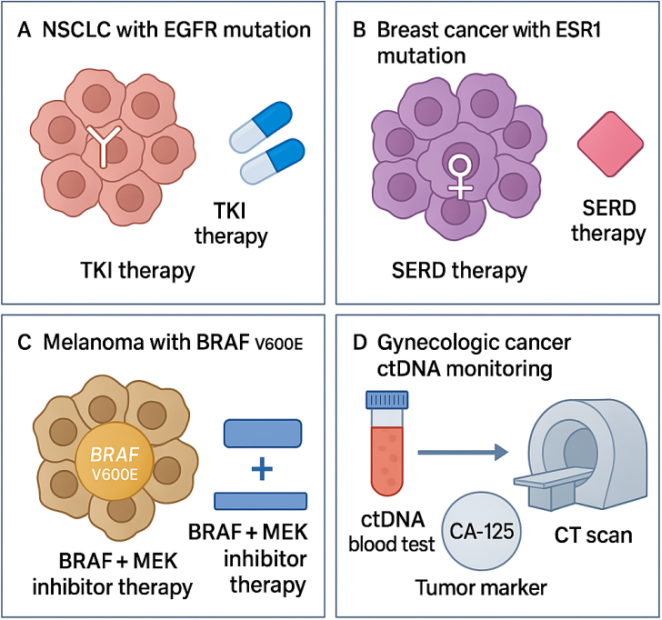
Figure 11. Improved ctDNA-guided personalized treatment schematic.
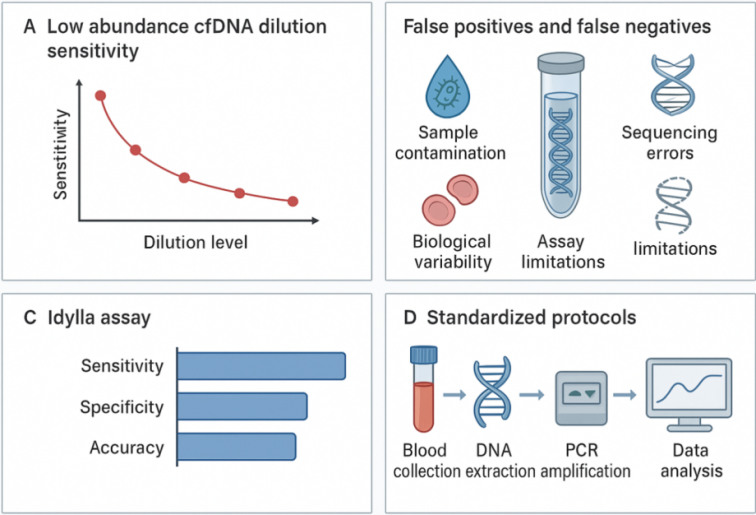
Figure 12. Sensitivity, Specificity, and Standardization in ctDNA Analysis.
Figure 13. Ethical considerations in ctDNA utilization.
Figure 14. Innovations in ctDNA detection technologies.
Information

