Department of Obstetrics, Gynecology and Reproductive Health, University of Health Sciences - Vietnam National University Ho Chi Minh City, Ho Chi Minh City, Vietnam
Department of Obstetrics, Gynecology and Reproductive Health, University of Health Sciences - Vietnam National University Ho Chi Minh City, Ho Chi Minh City, Vietnam
Background: The management of term pregnancy complicated by active maternal skin infection at the surgical site, bacterial colonization, and fetal anomalies presents a significant therapeutic challenge. Incising through infected tissue for a cesarean section increases the risk of surgical site infection and wound dehiscence. This report analyzes the management of a high-risk pregnancy complicated by secondarily infected Atopic Eruption of Pregnancy (AEP), Group B Streptococcus (GBS) colonization, and oligohydramnios. Case Presentation: A 30-year-old primigravida at 39 weeks and 4 days of gestation presented to a tertiary care center with severe, exudative abdominal dermatitis suggestive of secondary Staphylococcus aureus superinfection and recto-vaginal GBS colonization. Obstetric assessment revealed oligohydramnios (Maximum Vertical Pocket 1.8 cm), an estimated fetal weight of 3950g, and a prenatal diagnosis of cleft lip and palate. To avoid surgical incision through the infected abdominal wall, labor was induced using a Foley catheter. The patient achieved a successful vaginal delivery of a male infant weighing 3900g, with Apgar scores of 6 and 8 at 1 and 5 minutes, respectively. Postpartum management included intravenous Cefotaxime and topical corticosteroids. Conclusion: Vaginal delivery via mechanical induction is a viable strategy to mitigate surgical risks in patients with extensive abdominal skin infection and borderline macrosomia. A multidisciplinary approach utilizing broad-spectrum antibiotics and dermatological therapy resulted in favorable maternal and neonatal outcomes.
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
Impetiginized Atopic Eruption, Group B Streptococcus, Oligohydramnios, Foley Catheter Induction, Cefotaxime,
Cleft Lip and Palate
1. Introduction
The simultaneous presentation of conflicting obstetric and dermatological pathologies at term requires deviation from standard protocols to minimize maternal and neonatal morbidity. This case report examines a scenario where the indication for delivery (oligohydramnios at term) was complicated by a significant contraindication to cesarean section (active abdominal skin infection) and risks associated with vaginal delivery (fetal size, craniofacial malformation).
Hormonal and immunologic changes during pregnancy can contribute to the development of different dermatoses
[1]
Munera-Campos M, Carrascosa JM. Atopic Dermatitis: Fertility, Pregnancy, and Treatment Perspectives. Am J Clin Dermatol. 2024; 25(1): 55-66.
An abdominal incision through such infected tissue is classified as a Class IV wound, significantly elevating the risk of necrotizing fasciitis and sepsis
[7]
Olsen MA, Butler AM, Willers DM, Devkota P, Gross GA, Fraser VJ. Risk Factors for Surgical Site Infection After Low Transverse Cesarean Section. Infect Control Hosp Epidemiol. 2008; 29(6): 477-484.
Concomitant maternal colonization with Group B Streptococcus (GBS) further exacerbates the risk of neonatal sepsis
[8]
Dhudasia MB, Flannery DD, Pfeifer MR, Puopolo KM. Updated Guidance: Prevention and Management of Perinatal Group B Streptococcus Infection. NeoReviews. 2021; 22(3): e177-e188.
Additionally, the presence of oligohydramnios and a fetus with cleft lip and palate necessitates careful delivery planning to manage potential airway compromise and shoulder dystocia.
2. Case Presentation
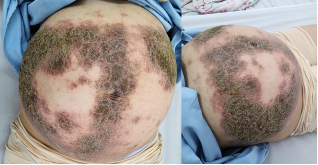
A 30-year-old primigravida presented to the emergency department at 39 weeks and 4 days of gestation with a chief complaint of severe, generalized pruritus and exudative skin lesions. The patient reported a one-month history of pruritus initially localized to the abdomen, which subsequently disseminated. In the days preceding admission, the abdominal lesions began to exude serous fluid, indicating a disrupted skin barrier and secondary infection (impetiginized eczema). The patient had not sought prior dermatological care. Her obstetric history was significant for a prenatal diagnosis of fetal cleft lip and palate and a positive screening result for GBS.
Upon physical examination, the patient was alert and afebrile (37°C), with a pulse of 100 beats per minute and blood pressure of 104/63 mmHg. Dermatological assessment revealed widespread eczematous plaques with significant exudation and crusting, heavily localized to the abdominal wall, directly compromising the potential Pfannenstiel incision site. Obstetric examination demonstrated a uterine fundal height of 32 cm and a fetal heart rate of 136 beats per minute. The cervix was closed, and the cephalic presentation was confirmed.
The Estimated Fetal Weight (EFW) was 3950g. Amniotic fluid assessment revealed oligohydramnios, with a Maximum Vertical Pocket (MVP) measuring 1.8 cm. The diagnosis of cleft lip and palate was reconfirmed. Laboratory investigations showed a white blood cell count of 8.75 K/uL with 4.6% eosinophils. Renal and liver function tests were within normal limits, and screening for gestational diabetes was negative.
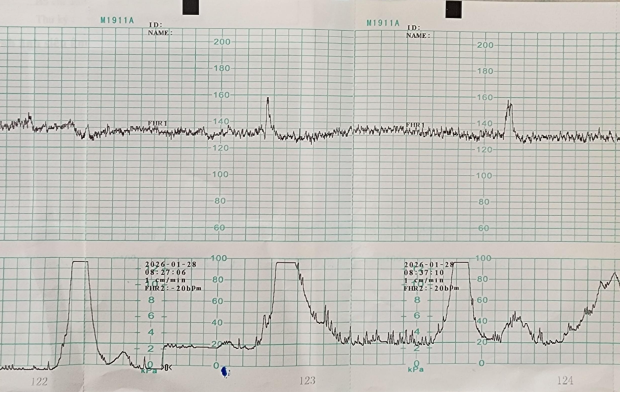
Figure 2. Cardiotocography (CTG) tracing following mechanical induction of labor using a Foley catheter.
Given the extensive infection of the abdominal skin, cesarean section was deemed to carry a prohibitive risk for surgical site infection and wound complications. Consequently, a multidisciplinary decision was made to attempt vaginal delivery. Induction of labor was initiated using a Foley catheter for mechanical cervical ripening. Simultaneously, systemic antibiotic therapy was commenced with Cefotaxime (1g IV). This regimen was selected to provide immediate therapeutic coverage for the Staphylococcus aureus skin superinfection and prophylactic coverage for GBS and potential intra-amniotic infection, given the induction devices.
The induction process was successful, establishing regular uterine contractions and progressive cervical dilation. The patient proceeded to a normal vaginal delivery of a live male infant weighing 3900g. The neonate had Apgar scores of 6 at 1 minute and 8 at 5 minutes. No shoulder dystocia occurred.
Postpartum management focused on continued infection control and dermatological rehabilitation. The patient continued intravenous Cefotaxime (1g every 8 hours) for a total course of 5 days. Concurrently, the skin lesions were treated with topical corticosteroids and intensive emollients. The patient’s condition improved significantly, with resolution of the exudative phase and reduction in erythema. She remained stable and were discharged on postpartum day 4.
3. Discussion
3.1. Surgical Site Integrity and Delivery Mode
The primary clinical dilemma in this case was the management of delivery in the presence of active skin infection at the operative site. Incising through S. aureus-colonized, exudative tissue circumvents the skin's natural barrier defense, exposing the fascial and subcutaneous layers to high bacterial loads. By prioritizing vaginal delivery through mechanical induction, the integrity of the abdominal wall was preserved, preventing potential complications such as necrotizing fasciitis or complex wound dehiscence. The finding of an MVP of 1.8 cm confirmed significant oligohydramnios, necessitating prompt delivery despite the unfavorable cervix
[9]
Borovac-Pinheiro A, Inversetti A, Di Simone N, Barnea ER, the FIGO Childbirth and Postpartum Hemorrhage Committee. FIGO good practice recommendations for induced or spontaneous labor at term: Prep‐for‐Labor triage to minimize risks and maximize favorable outcomes. Int J Gynecol Obstet. 2023; 163(S2): 51-56.
The selection of Cefotaxime, a third-generation cephalosporin, provided effective coverage for the suspected pathogens. Unlike standard GBS prophylaxis or surgical prophylaxis, Cefotaxime was chosen for its broader spectrum and tissue penetration
[10]
Dave D, Mittal DrI. A Comprehensive Review of Cephalosporin Antibiotics: Pharmacokinetic/Pharmacodynamic Considerations, Extended Infusion Strategies, and Clinical Outcomes. PEXACY International Journal of Pharmaceutical Science. Preprint posted online January 14, 2025.
Initiating the antibiotic at the start of induction served a dual purpose: treating the active maternal soft tissue infection during the intrapartum period and providing robust prophylaxis against vertical transmission of GBS. This early initiation likely contributed to preventing ascending infection, particularly important given the presence of a foreign body (Foley catheter).
In addition to systemic antimicrobials, localized dermatological care was imperative. Concurrently, the skin lesions were treated with topical corticosteroids and intensive emollients. Emollients constitute the fundamental baseline therapy for AEP by helping restore the impaired epidermal barrier and preventing further fluid loss
[3]
Balakirski G, Novak N. Atopic dermatitis and pregnancy. J Allergy Clin Immunol. 2022; 149(4): 1185-1194.
Furthermore, the application of mild-to-moderate topical corticosteroids is a well-established, safe intervention during pregnancy; it effectively suppresses local inflammation and interrupts the pruritic itch-scratch cycle without the risks of severe systemic absorption or fetal growth restriction that are typically associated with prolonged use of potent systemic steroids
[11]
Chi CC, Wang SH, Wojnarowska F, Kirtschig G, Davies E, Bennett C. Safety of topical corticosteroids in pregnancy. Cochrane Skin Group, ed. Cochrane Database Syst Rev. 2015; 2015(10).
Following this dual-pronged pharmacological approach, the patient’s condition improved significantly, with resolution of the exudative phase and reduction in erythema.
4. Conclusion
This case demonstrates that induction of labor with a Foley catheter, combined with immediate therapeutic antibiotic coverage, is a safe and effective strategy for managing term pregnancies complicated by oligohydramnios and infected abdominal dermatoses. In the context of oligohydramnios, mechanical cervical ripening via a Foley catheter provides a significant safety advantage. It effectively promotes cervical dilation mechanically and through local endogenous prostaglandin release, thereby avoiding the higher risks of uterine hyperstimulation and non-reassuring fetal heart rate patterns that are more commonly associated with exogenous pharmacological induction agents
[12]
Zhang Y, Chen L, Yan G, et al. Comparison of the effectiveness and pregnancy outcomes of labor induction with dinoprostone or single-balloon catheter in term nulliparous women with borderline oligohydramnios. Chin Med J (Engl). 2022; 135(6): 681-690.
Furthermore, the avoidance of cesarean section significantly reduced maternal morbidity. By maintaining the intactness of the infected abdominal wall, the multidisciplinary team averted severe surgical site complications such as complex wound dehiscence or necrotizing fasciitis. The integrated use of systemic Cefotaxime starting from induction and topical dermatological therapy facilitated rapid recovery. Specifically, the adjunct use of safe topical corticosteroids and emollients ensured that the patient’s condition improved significantly, with resolution of the exudative phase and reduction in erythema prior to discharge. Ultimately, this report underscores the efficacy of combining obstetric interventions with tailored pharmacological and dermatological management to optimize both maternal and neonatal outcomes in complex clinical scenarios.
Dhudasia MB, Flannery DD, Pfeifer MR, Puopolo KM. Updated Guidance: Prevention and Management of Perinatal Group B Streptococcus Infection. NeoReviews. 2021; 22(3): e177-e188.
Borovac-Pinheiro A, Inversetti A, Di Simone N, Barnea ER, the FIGO Childbirth and Postpartum Hemorrhage Committee. FIGO good practice recommendations for induced or spontaneous labor at term: Prep‐for‐Labor triage to minimize risks and maximize favorable outcomes. Int J Gynecol Obstet. 2023; 163(S2): 51-56.
Dave D, Mittal DrI. A Comprehensive Review of Cephalosporin Antibiotics: Pharmacokinetic/Pharmacodynamic Considerations, Extended Infusion Strategies, and Clinical Outcomes. PEXACY International Journal of Pharmaceutical Science. Preprint posted online January 14, 2025.
Chi CC, Wang SH, Wojnarowska F, Kirtschig G, Davies E, Bennett C. Safety of topical corticosteroids in pregnancy. Cochrane Skin Group, ed. Cochrane Database Syst Rev. 2015; 2015(10).
Zhang Y, Chen L, Yan G, et al. Comparison of the effectiveness and pregnancy outcomes of labor induction with dinoprostone or single-balloon catheter in term nulliparous women with borderline oligohydramnios. Chin Med J (Engl). 2022; 135(6): 681-690.
Ho, T., Nguyen, Y. (2026). Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report. Science Frontiers, 7(1), 40-43. https://doi.org/10.11648/j.sf.20260701.14
Ho, T.; Nguyen, Y. Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report. Sci. Front.2026, 7(1), 40-43. doi: 10.11648/j.sf.20260701.14
Ho T, Nguyen Y. Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report. Sci Front. 2026;7(1):40-43. doi: 10.11648/j.sf.20260701.14
@article{10.11648/j.sf.20260701.14,
author = {Tuan Ho and Yen Nguyen},
title = {Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report},
journal = {Science Frontiers},
volume = {7},
number = {1},
pages = {40-43},
doi = {10.11648/j.sf.20260701.14},
url = {https://doi.org/10.11648/j.sf.20260701.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sf.20260701.14},
abstract = {Background: The management of term pregnancy complicated by active maternal skin infection at the surgical site, bacterial colonization, and fetal anomalies presents a significant therapeutic challenge. Incising through infected tissue for a cesarean section increases the risk of surgical site infection and wound dehiscence. This report analyzes the management of a high-risk pregnancy complicated by secondarily infected Atopic Eruption of Pregnancy (AEP), Group B Streptococcus (GBS) colonization, and oligohydramnios. Case Presentation: A 30-year-old primigravida at 39 weeks and 4 days of gestation presented to a tertiary care center with severe, exudative abdominal dermatitis suggestive of secondary Staphylococcus aureus superinfection and recto-vaginal GBS colonization. Obstetric assessment revealed oligohydramnios (Maximum Vertical Pocket 1.8 cm), an estimated fetal weight of 3950g, and a prenatal diagnosis of cleft lip and palate. To avoid surgical incision through the infected abdominal wall, labor was induced using a Foley catheter. The patient achieved a successful vaginal delivery of a male infant weighing 3900g, with Apgar scores of 6 and 8 at 1 and 5 minutes, respectively. Postpartum management included intravenous Cefotaxime and topical corticosteroids. Conclusion: Vaginal delivery via mechanical induction is a viable strategy to mitigate surgical risks in patients with extensive abdominal skin infection and borderline macrosomia. A multidisciplinary approach utilizing broad-spectrum antibiotics and dermatological therapy resulted in favorable maternal and neonatal outcomes.},
year = {2026}
}
TY - JOUR
T1 - Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report
AU - Tuan Ho
AU - Yen Nguyen
Y1 - 2026/03/27
PY - 2026
N1 - https://doi.org/10.11648/j.sf.20260701.14
DO - 10.11648/j.sf.20260701.14
T2 - Science Frontiers
JF - Science Frontiers
JO - Science Frontiers
SP - 40
EP - 43
PB - Science Publishing Group
SN - 2994-7030
UR - https://doi.org/10.11648/j.sf.20260701.14
AB - Background: The management of term pregnancy complicated by active maternal skin infection at the surgical site, bacterial colonization, and fetal anomalies presents a significant therapeutic challenge. Incising through infected tissue for a cesarean section increases the risk of surgical site infection and wound dehiscence. This report analyzes the management of a high-risk pregnancy complicated by secondarily infected Atopic Eruption of Pregnancy (AEP), Group B Streptococcus (GBS) colonization, and oligohydramnios. Case Presentation: A 30-year-old primigravida at 39 weeks and 4 days of gestation presented to a tertiary care center with severe, exudative abdominal dermatitis suggestive of secondary Staphylococcus aureus superinfection and recto-vaginal GBS colonization. Obstetric assessment revealed oligohydramnios (Maximum Vertical Pocket 1.8 cm), an estimated fetal weight of 3950g, and a prenatal diagnosis of cleft lip and palate. To avoid surgical incision through the infected abdominal wall, labor was induced using a Foley catheter. The patient achieved a successful vaginal delivery of a male infant weighing 3900g, with Apgar scores of 6 and 8 at 1 and 5 minutes, respectively. Postpartum management included intravenous Cefotaxime and topical corticosteroids. Conclusion: Vaginal delivery via mechanical induction is a viable strategy to mitigate surgical risks in patients with extensive abdominal skin infection and borderline macrosomia. A multidisciplinary approach utilizing broad-spectrum antibiotics and dermatological therapy resulted in favorable maternal and neonatal outcomes.
VL - 7
IS - 1
ER -
Department of Obstetrics, Gynecology and Reproductive Health, University of Health Sciences - Vietnam National University Ho Chi Minh City, Ho Chi Minh City, Vietnam
Department of Obstetrics, Gynecology and Reproductive Health, University of Health Sciences - Vietnam National University Ho Chi Minh City, Ho Chi Minh City, Vietnam
Ho, T., Nguyen, Y. (2026). Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report. Science Frontiers, 7(1), 40-43. https://doi.org/10.11648/j.sf.20260701.14
Ho, T.; Nguyen, Y. Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report. Sci. Front.2026, 7(1), 40-43. doi: 10.11648/j.sf.20260701.14
Ho T, Nguyen Y. Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report. Sci Front. 2026;7(1):40-43. doi: 10.11648/j.sf.20260701.14
@article{10.11648/j.sf.20260701.14,
author = {Tuan Ho and Yen Nguyen},
title = {Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report},
journal = {Science Frontiers},
volume = {7},
number = {1},
pages = {40-43},
doi = {10.11648/j.sf.20260701.14},
url = {https://doi.org/10.11648/j.sf.20260701.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sf.20260701.14},
abstract = {Background: The management of term pregnancy complicated by active maternal skin infection at the surgical site, bacterial colonization, and fetal anomalies presents a significant therapeutic challenge. Incising through infected tissue for a cesarean section increases the risk of surgical site infection and wound dehiscence. This report analyzes the management of a high-risk pregnancy complicated by secondarily infected Atopic Eruption of Pregnancy (AEP), Group B Streptococcus (GBS) colonization, and oligohydramnios. Case Presentation: A 30-year-old primigravida at 39 weeks and 4 days of gestation presented to a tertiary care center with severe, exudative abdominal dermatitis suggestive of secondary Staphylococcus aureus superinfection and recto-vaginal GBS colonization. Obstetric assessment revealed oligohydramnios (Maximum Vertical Pocket 1.8 cm), an estimated fetal weight of 3950g, and a prenatal diagnosis of cleft lip and palate. To avoid surgical incision through the infected abdominal wall, labor was induced using a Foley catheter. The patient achieved a successful vaginal delivery of a male infant weighing 3900g, with Apgar scores of 6 and 8 at 1 and 5 minutes, respectively. Postpartum management included intravenous Cefotaxime and topical corticosteroids. Conclusion: Vaginal delivery via mechanical induction is a viable strategy to mitigate surgical risks in patients with extensive abdominal skin infection and borderline macrosomia. A multidisciplinary approach utilizing broad-spectrum antibiotics and dermatological therapy resulted in favorable maternal and neonatal outcomes.},
year = {2026}
}
TY - JOUR
T1 - Management of a Term Pregnancy Complicated by Severe Impetiginized Atopic Eruption and Oligohydramnios:
A Case Report
AU - Tuan Ho
AU - Yen Nguyen
Y1 - 2026/03/27
PY - 2026
N1 - https://doi.org/10.11648/j.sf.20260701.14
DO - 10.11648/j.sf.20260701.14
T2 - Science Frontiers
JF - Science Frontiers
JO - Science Frontiers
SP - 40
EP - 43
PB - Science Publishing Group
SN - 2994-7030
UR - https://doi.org/10.11648/j.sf.20260701.14
AB - Background: The management of term pregnancy complicated by active maternal skin infection at the surgical site, bacterial colonization, and fetal anomalies presents a significant therapeutic challenge. Incising through infected tissue for a cesarean section increases the risk of surgical site infection and wound dehiscence. This report analyzes the management of a high-risk pregnancy complicated by secondarily infected Atopic Eruption of Pregnancy (AEP), Group B Streptococcus (GBS) colonization, and oligohydramnios. Case Presentation: A 30-year-old primigravida at 39 weeks and 4 days of gestation presented to a tertiary care center with severe, exudative abdominal dermatitis suggestive of secondary Staphylococcus aureus superinfection and recto-vaginal GBS colonization. Obstetric assessment revealed oligohydramnios (Maximum Vertical Pocket 1.8 cm), an estimated fetal weight of 3950g, and a prenatal diagnosis of cleft lip and palate. To avoid surgical incision through the infected abdominal wall, labor was induced using a Foley catheter. The patient achieved a successful vaginal delivery of a male infant weighing 3900g, with Apgar scores of 6 and 8 at 1 and 5 minutes, respectively. Postpartum management included intravenous Cefotaxime and topical corticosteroids. Conclusion: Vaginal delivery via mechanical induction is a viable strategy to mitigate surgical risks in patients with extensive abdominal skin infection and borderline macrosomia. A multidisciplinary approach utilizing broad-spectrum antibiotics and dermatological therapy resulted in favorable maternal and neonatal outcomes.
VL - 7
IS - 1
ER -