Abstract
Breast cancer is a heterogeneous malignancy in which integrated clinicopathological assessment and receptor-based classification are essential for prognostic evaluation and treatment planning. This retrospective descriptive study evaluated the clinicopathological characteristics and hormone receptor/HER2-defined subtype distribution of 75 histologically confirmed breast cancer cases from an institutional cohort. Data on age, tumor site, breast laterality, histological type, histological grade, T stage, N stage, AJCC stage, ER/PR status, HER2 status, HER2-low status, and combined receptor-defined subtype were extracted from clinical, histopathological, and immunohistochemistry records and summarized using frequencies and percentages. Most patients were aged >46 years (43/75, 57.0%), followed by 36-45 years (26/75, 35.0%) and <35 years (6/75, 8.0%). The upper outer quadrant was the most frequent tumor site (30/75, 40.0%), and right breast involvement was slightly more common than left-sided disease (43/75, 57.0% vs. 32/75, 42.66%). Invasive ductal carcinoma was the predominant histological type (70/75, 93.33%). Grade II tumors were most frequent (46/75, 61.33%), followed by grade III tumors (25/75, 33.33%). T2 was the dominant T stage (49/75, 65.0%), while N1 was the most common nodal stage (30/75, 40.0%). According to AJCC staging, stage IIB was the most frequent individual stage (19/75, 25.33%), followed by IIA (16/75, 21.33%) and IIIA (15/75, 20.0%). ER−/PR− tumors represented the largest ER/PR category (31/75, 41.33%), whereas HER2-negative disease was predominant (51/75, 68.0%). Overall subtype analysis showed that triple-negative breast cancer was the most frequent receptor-defined subtype (28/75, 37.33%), followed by HR+/HER2− disease (23/75, 30.66%) and HR+/HER2+ disease (9/75, 12.0%); HER2-low tumors were uncommon (2/75, 2.66%). These findings indicate that the cohort was characterized by predominance of invasive ductal carcinoma, intermediate-to-high histological grade, T2 disease, frequent nodal involvement, and a substantial burden of TNBC and HR+/HER2− tumors, underscoring the importance of complete histopathological staging and standardized receptor profiling for subtype-aware breast cancer assessment in institutional settings.
1. Introduction
Breast cancer remains a leading global malignancy and continues to impose a substantial clinical and public health burden. In 2022, approximately 2.3 million women were diagnosed with breast cancer worldwide, and nearly 670,000 deaths were attributed to the disease
| [1] | World Health Organization. Breast Cancer. Available from:
https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed 6 May 2026). |
| [2] | Bray, F., Laversanne, M., Sung, H., Ferlay, J., Siegel, R. L., Soerjomataram, I., et al. Global Cancer Statistics 2022: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer Journal for Clinicians. 2024, 74(3), 229-263.
https://doi.org/10.3322/caac.21834 |
[1, 2]
. Although improvements in early detection, pathology services, and systemic therapy have contributed to better outcomes in many high-resource settings, survival disparities remain substantial in low- and middle-income countries, where diagnosis is often delayed and access to comprehensive cancer care may be limited
| [3] | World Health Organization. Global Breast Cancer Initiative Implementation Framework: Assessing, Strengthening and Scaling up Services for the Early Detection and Management of Breast Cancer. Available from:
https://www.who.int/publications/i/item/9789240067134
(accessed 6 May 2026). |
[3]
. The World Health Organization Global Breast Cancer Initiative emphasizes early detection, timely diagnosis, and complete multimodal treatment as core strategies to reduce global breast cancer mortality by 2.5% per year
| [3] | World Health Organization. Global Breast Cancer Initiative Implementation Framework: Assessing, Strengthening and Scaling up Services for the Early Detection and Management of Breast Cancer. Available from:
https://www.who.int/publications/i/item/9789240067134
(accessed 6 May 2026). |
[3]
. These priorities are especially relevant for countries such as Bangladesh, where IARC-linked data identify breast cancer as the most common cancer by incidence among women
.
Breast cancer is a heterogeneous disease, and its clinical behavior cannot be adequately described by tumor burden alone. Conventional clinicopathological parameters, including patient age, tumor site, laterality, histological type, histological grade, tumor size, nodal involvement, and AJCC stage, remain essential for prognosis and treatment planning
| [6] | World Health Organization Classification of Tumours Editorial Board. Breast Tumours. 5th ed. Lyon, France: International Agency for Research on Cancer; 2019. |
[6]
. Histological type provides information on morphological classification, with invasive ductal carcinoma or invasive carcinoma of no special type being the most common subtype, while less frequent variants such as invasive lobular, mucinous, apocrine, and other uncommon tumors may have distinct pathological and clinical implications
| [7] | Elston, C. W., Ellis, I. O. Pathological Prognostic Factors in Breast Cancer. I. The Value of Histological Grade in Breast Cancer: Experience from a Large Study with Long-Term Follow-Up. Histopathology. 1991, 19(5), 403-410.
https://doi.org/10.1111/j.1365-2559.1991.tb00229.x |
[7]
. Histological grade, commonly assessed using the Nottingham grading system, reflects tumor differentiation through tubule formation, nuclear pleomorphism, and mitotic activity, and remains a well established prognostic marker in invasive breast cancer
| [8] | Rakha, E. A., El-Sayed, M. E., Lee, A. H. S., Elston, C. W., Grainge, M. J., Hodi, Z., et al. Prognostic Significance of Nottingham Histologic Grade in Invasive Breast Carcinoma. Journal of Clinical Oncology. 2008, 26(19), 3153-3158.
https://doi.org/10.1200/JCO.2007.15.5986 |
| [9] | Amin, M. B., Edge, S. B., Greene, F. L., Byrd, D. R., Brookland, R. K., Washington, M. K., et al., Eds. AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2017. |
[8, 9]
. Similarly, nodal involvement and AJCC stage provide critical information regarding disease extent, recurrence risk, and treatment intensity
| [10] | Weiss, A., Chavez-MacGregor, M., Lichtensztajn, D. Y., Yi, M., Tadros, A., Hortobagyi, G. N., et al. Validation Study of the American Joint Committee on Cancer Eighth Edition Prognostic Stage Compared with Anatomic Stage in Breast Cancer. JAMA Oncology. 2018, 4(2), 203-209.
https://doi.org/10.1001/jamaoncol.2017.4298 |
[10]
. The eighth edition of the AJCC breast cancer staging system represents an important shift from purely anatomic staging toward biologically informed prognostic staging. In addition to tumor size, nodal status, and distant metastasis, prognostic staging incorporates tumor grade, estrogen receptor, progesterone receptor, and HER2 status, reflecting the clinical importance of tumor biology in outcome prediction
| [11] | Allison, K. H., Hammond, M. E. H., Dowsett, M., McKernin, S. E., Carey, L. A., Fitzgibbons, P. L., et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. Journal of Clinical Oncology. 2020, 38(12), 1346-1366. https://doi.org/10.1200/JCO.19.02309 |
[11]
. Therefore, an integrated clinicopathological profile that includes T stage, N stage, AJCC stage, histological type, histological grade, and receptor expression can provide a more clinically meaningful characterization of breast cancer presentation than isolated descriptive variables. This is particularly important in institutional cohorts from resource-variable settings, where structured reporting may support improved clinical documentation, multidisciplinary planning, and future comparative research.
Immunohistochemical assessment of estrogen receptor, progesterone receptor, and HER2 is now indispensable in routine breast cancer evaluation. The ASCO/CAP guideline recommends standardized ER and PR testing, with tumors showing 1% to 100% positive tumor nuclei considered receptor positive, because hormone receptor status directly determines eligibility for endocrine therapy
| [12] | Wolff, A. C., Somerfield, M. R., Dowsett, M., Hammond, M. E. H., Hayes, D. F., McShane, L. M., et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: ASCO-CAP Guideline Update. Journal of Clinical Oncology. 2023, 41(22), 3867-3872.
https://doi.org/10.1200/JCO.22.02864 |
[12]
. HER2 testing is similarly essential because HER2 protein overexpression or ERBB2 gene amplification identifies patients who may benefit from HER2-targeted treatment
. These biomarkers also define clinically relevant subgroups, including HR+/HER2−, HR+/HER2+, HR−/HER2+, and triple-negative breast cancer
| [14] | Perou, C. M., Sørlie, T., Eisen, M. B., van de Rijn, M., Jeffrey, S. S., Rees, C. A., et al. Molecular Portraits of Human Breast Tumours. Nature. 2000, 406(6797), 747-752.
https://doi.org/10.1038/35021093 |
| [15] | Lehmann, B. D., Bauer, J. A., Chen, X., Sanders, M. E., Chakravarthy, A. B., Shyr, Y., et al. Identification of Human Triple-Negative Breast Cancer Subtypes and Preclinical Models for Selection of Targeted Therapies. Journal of Clinical Investigation. 2011, 121(7), 2750-2767.
https://doi.org/10.1172/JCI45014 |
[14, 15]
. Triple-negative breast cancer is particularly important because it lacks ER, PR, and HER2 expression and is often associated with more aggressive clinical behavior and fewer conventional targeted treatment options compared with hormone receptor-positive disease
| [15] | Lehmann, B. D., Bauer, J. A., Chen, X., Sanders, M. E., Chakravarthy, A. B., Shyr, Y., et al. Identification of Human Triple-Negative Breast Cancer Subtypes and Preclinical Models for Selection of Targeted Therapies. Journal of Clinical Investigation. 2011, 121(7), 2750-2767.
https://doi.org/10.1172/JCI45014 |
| [16] | Modi, S., Jacot, W., Yamashita, T., Sohn, J., Vidal, M., Tokunaga, E., et al. Trastuzumab Deruxtecan in Previously Treated HER2-Low Advanced Breast Cancer. New England Journal of Medicine. 2022, 387(1), 9-20.
https://doi.org/10.1056/NEJMoa2203690 |
[15, 16]
.
HER2-low breast cancer has recently gained clinical importance, particularly after evidence from DESTINY-Breast04 showed benefit of trastuzumab deruxtecan in previously treated HER2-low advanced breast cancer
. The US Food and Drug Administration subsequently approved fam-trastuzumab deruxtecan-nxki for eligible patients with unresectable or metastatic HER2-low breast cancer, reinforcing the therapeutic relevance of carefully documenting HER2 expression categories
| [18] | von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gøtzsche, P. C., Vandenbroucke, J. P., et al. The Strengthening the Reporting of Observational Studies in Epidemiology Statement: Guidelines for Reporting Observational Studies. Annals of Internal Medicine. 2007, 147(8), 573-577.
https://doi.org/10.7326/0003-4819-147-8-200710160-00010 |
[18]
. However, the 2023 ASCO/CAP HER2 testing update continues to emphasize standardized HER2 interpretation and reporting, underscoring the need for accurate and consistent receptor assessment in both clinical and research datasets
.
Despite the established prognostic and therapeutic importance of these variables, local descriptive data integrating clinicopathological features with hormone receptor and HER2-defined subtypes remain valuable, particularly in Bangladesh and similar settings. Such data may identify the dominant histological patterns, the distribution of tumor grade and stage at presentation, the burden of nodal involvement, and the relative frequency of receptor-defined subtypes, including TNBC and HER2-low disease. These patterns can help contextualize local breast cancer biology and may inform pathology reporting priorities, clinical risk stratification, and future multicenter studies.
Therefore, this study aimed to characterize the clinicopathological and receptor-status profile of breast cancer patients in an institutional cohort, with emphasis on age distribution, tumor laterality, tumor site, histological type, histological grade, T stage, N stage, AJCC stage, ER/PR status, HER2 status, HER2-low status, and combined hormone receptor/HER2-defined subtypes. By integrating conventional pathological parameters with biomarker-based classification, this study provides a structured overview of breast cancer presentation and subtype distribution that may support local prognostic assessment, treatment planning, and future comparative breast cancer research.
Figure 1. Distribution of Patients by age group and T Stage.
Figure 2. Distribution of Patients by tumor site and breast involvement.
Figure 3. Clinico-pathological stage by AJCC.
Figure 4. Histological grade distribution.
Figure 5. Hormone receptor status in breast cancer.
Figure 6. Overall hormone receptor status in Breast Cancer.
Figure 7. HER2 status in Breast Cancer.
Figure 8. Age wise distribution of histological grade in Breast Cancer.
Figure 9. Age wise distribution of hormone receptor subtype in Breast Cancer.
Figure 10. Distribution of Histological Types and N stage in Breast Cancer.
Table 1. Distribution of Hormone Receptor Status According to Histological Grade in Breast Cancer Patients.
Histological Grading | Cases | Hormone Receptor Status |
HR+/HER2- | HR-/HER2+ | HR+/HER2+ | TNBC | Note Done |
I | 3 | 17 | 0 | 1 | 0 | 1 |
II | 45 | 6 | 1 | 6 | 16 | 5 |
III | 26 | 0 | 1 | 2 | 13 | 4 |
Ungraded | 1 | 2 | 0 | 0 | 0 | 1 |
Total: 75 | | | | | |
Table 2. Distribution of Hormone Receptor Status According to AJCC Stage in Breast Cancer Patients.
AJCC Staging | Cases | Hormone Receptor Status |
HR+/ HER2- | HR-/ HER2+ | HR+/ HER2+ | TNBC | Note Done |
I | 2 | 1 | 0 | 0 | 1 | 0 |
II (A+B) | 35 | 13 | 2 | 5 | 13 | 2 |
IIIA | 15 | 5 | 0 | 1 | 5 | 4 |
IIIB | 6 | 3 | 0 | 1 | 1 | 1 |
IIIC | 1 | 0 | 0 | 0 | 1 | 0 |
IV | 3 | 1 | 0 | 0 | 1 | 1 |
Unstage | 13 | 1 | 0 | 2 | 7 | 3 |
Total: | 75 | 24 | 2 | 9 | 29 | 11 |
2. Materials and Methods
2.1. Study Design and Reporting Framework
This was a retrospective, descriptive, cross-sectional study conducted among patients with breast cancer who underwent histopathological and immunohistochemical evaluation at [name of hospital/institute], Bangladesh. The study was designed to characterize the clinicopathological and receptor-status profile of breast cancer patients, including age distribution, tumor laterality, tumor site, histological type, histological grade, T stage, N stage, AJCC stage, ER/PR status, HER2 status, HER2-low status, and combined hormone receptor/HER2-defined molecular subtypes. The reporting of this observational study was guided by the Strengthening the Reporting of Observational Studies in Epidemiology statement
| [6] | World Health Organization Classification of Tumours Editorial Board. Breast Tumours. 5th ed. Lyon, France: International Agency for Research on Cancer; 2019. |
[6]
.
2.2. Study Setting and Study Period
The study was conducted at [department name, hospital/institute name], Bangladesh. Data were collected from routinely maintained histopathology, immunohistochemistry, and clinical records of breast cancer patients evaluated between [start month/year] and [end month/year]. All available records during the study period were reviewed using a standardized data-extraction form.
2.3. Study Population
The study population consisted of patients with histologically confirmed breast cancer who had available clinicopathological and/or receptor-status information during the study period. A total of 75 eligible breast cancer cases were included in the final analysis.
2.4. Eligibility Criteria
Patients were included if they had:
1) Histologically Confirmed Breast Carcinoma;
2) Available Clinicopathological Information, Including Age and Histological Diagnosis; and
3) Available Histological Grading, Staging, or Immunohistochemical Receptor-status Data.
Patients were excluded if records were duplicated, if the diagnosis represented metastatic disease to the breast from a non-breast primary, or if the available record was insufficient to confirm breast carcinoma. Cases with missing information for specific variables were not excluded from the overall analysis; instead, they were categorized as “Not Done,” “Unstage,” “Ungraded,” or “Not Identified,” as applicable.
2.5. Sample Size and Sampling Technique
Because this was a retrospective descriptive analysis of available institutional records, no formal sample-size calculation was performed. All eligible breast cancer cases identified during the study period were included using a consecutive sampling approach. The final analytical cohort comprised 75 patients.
2.6. Data Sources and Data Collection
Data were extracted from histopathology reports, immunohistochemistry reports, clinical records, and departmental registers. The extracted variables included age, breast laterality, tumor site, histological type, histological grade, T stage, N stage, AJCC stage, ER status, PR status, HER2 status, HER2-low status, and combined hormone receptor/HER2-defined subtype. Data were entered into a structured spreadsheet and checked for internal consistency before analysis.
Age was categorized into three groups: <35 years, 36-45 years, and >46 years. Tumor site was recorded as central, lower inner, lower outer, upper inner, upper outer, or not identified. Breast laterality was recorded as right or left. Histological types included invasive ductal carcinoma, invasive lobular carcinoma, mucinous carcinoma, non-Hodgkin lymphoma, and apocrine carcinoma, according to the diagnostic categories recorded in the pathology reports.
2.7. Histopathological Assessment
Histopathological diagnosis was based on formalin-fixed, paraffin-embedded tissue sections stained with hematoxylin and eosin as part of routine diagnostic practice. Histological typing was performed according to standard breast tumor classification principles, consistent with the World Health Organization classification framework
| [7] | Elston, C. W., Ellis, I. O. Pathological Prognostic Factors in Breast Cancer. I. The Value of Histological Grade in Breast Cancer: Experience from a Large Study with Long-Term Follow-Up. Histopathology. 1991, 19(5), 403-410.
https://doi.org/10.1111/j.1365-2559.1991.tb00229.x |
[7]
. Histological grading was recorded as grade I, grade II, grade III, or ungraded. Where grading information was available, grading was based on the Nottingham modification of the Scarff-Bloom-Richardson system, which assesses tubule formation, nuclear pleomorphism, and mitotic activity
| [8] | Rakha, E. A., El-Sayed, M. E., Lee, A. H. S., Elston, C. W., Grainge, M. J., Hodi, Z., et al. Prognostic Significance of Nottingham Histologic Grade in Invasive Breast Carcinoma. Journal of Clinical Oncology. 2008, 26(19), 3153-3158.
https://doi.org/10.1200/JCO.2007.15.5986 |
| [9] | Amin, M. B., Edge, S. B., Greene, F. L., Byrd, D. R., Brookland, R. K., Washington, M. K., et al., Eds. AJCC Cancer Staging Manual. 8th ed. New York, NY: Springer; 2017. |
[8, 9]
.
2.8. Staging Assessment
Tumor stage, nodal stage, and overall clinico-pathological stage were recorded from available clinical, imaging, operative, and histopathological information. T stage was categorized as T1, T2, T3, T4, or unstage. N stage was categorized as N0, N1, N2, N3, Nx, or unstage. Overall clinico-pathological stage was classified according to the AJCC staging framework and recorded as stage I, IIA, IIB, IIIA, IIIB, IIIC, IV, or unstage
| [11] | Allison, K. H., Hammond, M. E. H., Dowsett, M., McKernin, S. E., Carey, L. A., Fitzgibbons, P. L., et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. Journal of Clinical Oncology. 2020, 38(12), 1346-1366. https://doi.org/10.1200/JCO.19.02309 |
[11]
. Cases with insufficient information for definitive staging were retained in the analysis and categorized as unstage rather than excluded.
2.9. Immunohistochemistry and Receptor-status Assessment
Immunohistochemical receptor-status data were abstracted from the original pathology reports. ER, PR, and HER2 results were recorded as reported by the diagnostic laboratory. ER and PR status were interpreted according to ASCO/CAP guidance, in which tumors showing nuclear staining in ≥1% of invasive tumor cells are considered receptor positive
| [12] | Wolff, A. C., Somerfield, M. R., Dowsett, M., Hammond, M. E. H., Hayes, D. F., McShane, L. M., et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: ASCO-CAP Guideline Update. Journal of Clinical Oncology. 2023, 41(22), 3867-3872.
https://doi.org/10.1200/JCO.22.02864 |
[12]
. HER2 status was interpreted according to ASCO/CAP HER2 testing recommendations, using standard immunohistochemical scoring categories and available in situ hybridization results where applicable
| [19] | Giuliano, A. E., Connolly, J. L., Edge, S. B., Mittendorf, E. A., Rugo, H. S., Solin, L. J., et al. Breast Cancer: Major Changes in the American Joint Committee on Cancer Eighth Edition Cancer Staging Manual. CA: A Cancer Journal for Clinicians. 2017, 67(4), 290-303. https://doi.org/10.3322/caac.21393 |
[19]
.
HER2-positive disease was defined as HER2 IHC 3+ or HER2 IHC 2+ with gene amplification by in situ hybridization when confirmatory testing was available. HER2-negative disease was defined as HER2 IHC 0 or non-amplified HER2 status according to the original report. HER2-low status was recorded when the report documented HER2 IHC 1+ or HER2 IHC 2+ without gene amplification, consistent with contemporary reporting approaches for HER2-low breast cancer
| [20] | Ivanova, M., Künstlinger, H., Marques, A., et al. Standardized Pathology Report for HER2 Testing in Compliance with 2023 ASCO/CAP Updates and 2023 ESMO Consensus Statements on HER2-Low Breast Cancer. Virchows Archiv. 2024, 484(1), 3-14. https://doi.org/10.1007/s00428-023-03656-w |
| [21] | Hossain, M. S., Ferdous, S., Karim-Kos, H. E. Breast Cancer in South Asia: A Bangladeshi Perspective. Cancer Epidemiology. 2014, 38(5), 465-470.
https://doi.org/10.1016/j.canep.2014.08.004 |
[20, 21]
. Cases without receptor testing were categorized as “Not Done.”
2.10. Definition of Hormone Receptor and Molecular Subtype Groups
Hormone receptor positivity was defined as ER positivity and/or PR positivity. Based on ER, PR, and HER2 status, cases were categorized into the following receptor-defined groups: HR+/HER2−, HR−/HER2+, HR+/HER2+, HR−/HER2-low, HR+/HER2-low, triple-negative breast cancer, and not done. Triple-negative breast cancer was defined as ER-negative, PR-negative, and HER2-negative disease. For ER/PR-specific analysis, cases were categorized as ER+/PR+, ER+/PR−, ER−/PR+, ER−/PR−, or not done.
2.11. Data Management and Quality Control
All extracted data were reviewed for completeness, consistency, and logical agreement across variables. Category labels were standardized before analysis; for example, “Note Done” was harmonized as “Not Done,” and “No” nodal stage was recorded as N0. Row and column totals were cross-checked against the final sample size of 75 patients. Any discrepancies between summary tables and original records were resolved by rechecking the source document.
2.12. Outcome Variables
The primary outcomes were the frequency and percentage distributions of clinicopathological characteristics and receptor-status categories among breast cancer patients. These included age group, tumor laterality, tumor site, histological type, histological grade, T stage, N stage, AJCC stage, ER/PR status, HER2 status, and combined hormone receptor/HER2-defined subtypes. Secondary descriptive outputs included age-wise distribution of receptor-defined subtypes, age-wise distribution of histological grade, histological grade-wise distribution of receptor status, and AJCC stage-wise distribution of receptor status.
2.13. Statistical Analysis
Data were analyzed using Microsoft Excel 2019, SPSS 2022. Categorical variables were summarized as frequencies and percentages. Percentages were calculated using the total study population as the denominator unless otherwise specified. Missing, unstaged, ungraded, not identified, and not-done categories were retained as separate descriptive groups to preserve the completeness of the institutional dataset. No inferential statistical testing was performed because the objective of the study was descriptive characterization rather than hypothesis testing. All tables and figures were generated from the finalized cleaned dataset.
2.14. Ethical Considerations
The study protocol was reviewed and approved by the Institutional Review Board/Ethics Review Committee of Rajshahi Medical College. Approval number: C2110-RT7. Because this was a retrospective analysis of routinely collected, de-identified clinical and pathology records, the requirement for individual written informed consent was waived by the ethics committee. Patient confidentiality was maintained throughout the study, and no personally identifiable information was used in the analysis or presentation.
3. Results
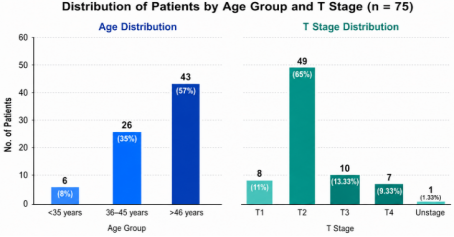
Figure 1 shows the distribution of patients according to age group and T stage. Most patients were aged >46 years (57%), followed by 36-45 years (35%) and <35 years (8%). In terms of tumor stage, T2 was the dominant category, comprising nearly two-thirds of the cohort (65%), whereas T1, T3, and T4 accounted for 11%, 13.33%, and 9.33% of cases, respectively. Only one patient was classified as unstaged (1.33%). These findings indicate that the cohort was largely composed of older patients and that T2 disease was the most common tumor stage at presentation.
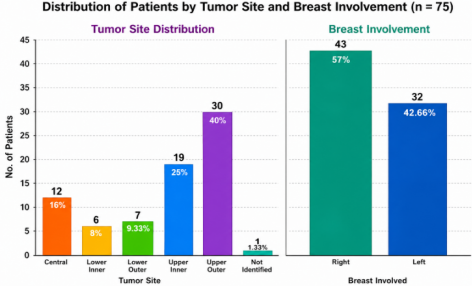
The distribution of tumor location and laterality is shown in
Figure 2. Among the 75 patients included in the analysis, tumors were most frequently located in the upper outer quadrant, observed in 30 patients (40.0%). This was followed by the upper inner quadrant in 19 patients (25.0%) and the central region in 12 patients (16.0%). Lower outer and lower inner quadrant tumors were less common, accounting for 7 cases (9.33%) and 6 cases (8.0%), respectively. Tumor site was not identified in 1.
patient (1.33%). Regarding breast involvement, right-sided breast cancer was more frequent than left-sided disease, with 43 patients (57.0%) having right breast involvement compared with 32 patients (42.66%) having left breast involvement. Overall, the findings demonstrate that the upper outer quadrant was the predominant tumor site, with a modest predominance of right breast involvement in the study cohort.
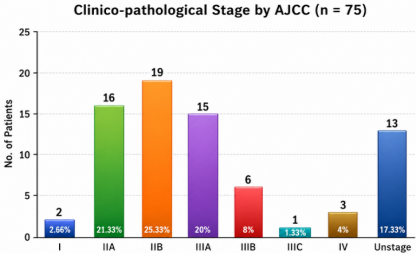
The clinico-pathological stage distribution according to AJCC classification is presented in
Figure 3. Among the 75 patients included in the study, stage IIB was the most frequently observed category, accounting for 19 cases (25.33%), followed by stage IIA in 16 cases (21.33%) and stage IIIA in 15 cases (20.0%). A considerable proportion of patients were classified as unstaged, representing 13 cases (17.33%). Less frequent categories included stage IIIB in 6 patients (8.0%), stage IV in 3 patients (4.0%), stage I in 2 patients (2.66%), and stage IIIC in 1 patient (1.33%). Overall, the distribution indicates that most staged patients presented with stage II to stage III disease, with stage IIB being the predominant clinico-pathological stage in this cohort.
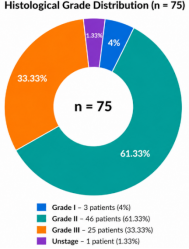
The histological grade distribution of the study cohort is shown in
Figure 4. Among the 75 patients, grade II tumors were the predominant histological category, identified in 46 cases (61.33%). Grade III tumors represented the second most frequent group, comprising 25 cases (33.33%), whereas grade I tumors were uncommon, accounting for only 3 cases (4.0%). One patient (1.33%) was recorded as unstaged. Overall, the cohort demonstrated a marked predominance of intermediate-grade disease, with grade II tumors comprising nearly two-thirds of all cases, while grade III tumors also accounted for a substantial proportion of the study population.
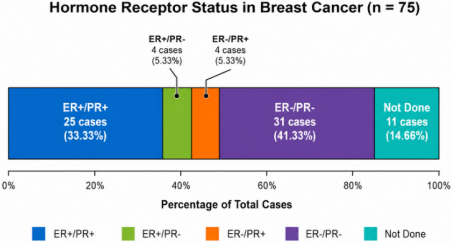
Hormone receptor status distribution is summarized in
Figure 5. Among the 75 breast cancer cases, ER-/PR- tumors represented the largest receptor-defined subgroup, comprising 31 cases (41.33%). Concordant ER+/PR+ expression was observed in 25 cases (33.33%), making it the second most common profile. Discordant hormone receptor phenotypes were infrequent, with ER+/PR- and ER-/PR+ patterns each identified in 4 cases (5.33%). Hormone receptor testing was not performed in 11 cases (14.66%). Overall, the cohort demonstrated a predominance of ER/PR-negative tumors, while approximately one-third of patients showed dual hormone receptor positivity, and discordant ER/PR expression patterns were uncommon.
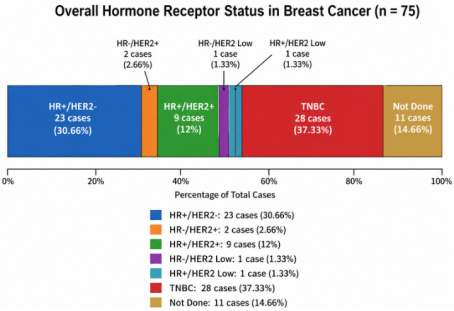
The overall hormone receptor and HER2-based subtype distribution is presented in
Figure 6. Among the 75 breast cancer cases, triple-negative breast cancer (TNBC) represented the largest subgroup, comprising 28 cases (37.33%). HR+/HER2− tumors were the second most frequent subtype, identified in 23 cases (30.66%), followed by HR+/HER2+ tumors in 9 cases (12.0%). HR−/HER2+ disease was relatively uncommon, accounting for 2 cases (2.66%). HER2-low categories were infrequently observed, with both HR−/HER2-low and HR+/HER2-low subtypes represented by 1 case each (1.33% each). Receptor testing or subtype classification was not completed in 11 cases (14.66%). Overall, the cohort showed a predominance of TNBC and HR+/HER2− disease, while HER2-positive and HER2-low subtypes accounted for comparatively smaller proportions of the study population.
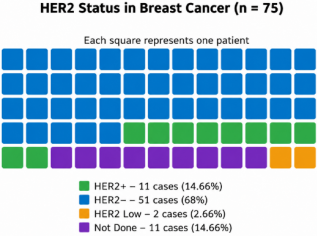
The HER2 status distribution of the study cohort is shown in
Figure 7. Among the 75 breast cancer cases, HER2-negative tumors constituted the predominant subgroup, accounting for 51 cases (68.0%). HER2-positive disease was identified in 11 patients (14.66%), while HER2-low status was observed in only 2 cases (2.66%). HER2 testing was not performed in 11 cases (14.66%). Overall, the cohort demonstrated a marked predominance of HER2-negative disease, whereas HER2-positive and HER2-low tumors represented comparatively smaller proportions of the study population.
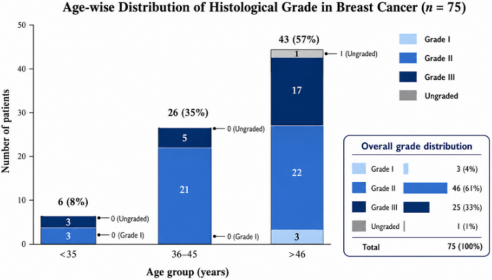
The age-stratified distribution of histological grade is shown in
Figure 8. Most patients were aged >46 years (43/75, 57.0%), followed by 36-45 years (26/75, 35.0%) and <35 years (6/75, 8.0%). Overall, grade II tumors were most frequent (46/75, 61.33%), followed by grade III tumors (25/75, 33.33%), while grade I and ungraded tumors were uncommon, accounting for 3 cases (4.0%) and 1 case (1.33%), respectively. Grade II predominated in both the 36-45-year and >46-year groups, whereas grade II and grade III tumors were equally distributed among patients aged <35 years.
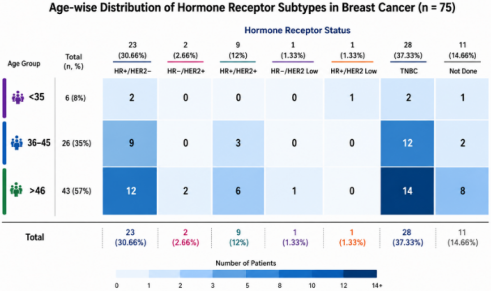
The age-stratified distribution of hormone receptor subtypes is shown in
Figure 9. Of the 75 breast cancer patients, most were aged >46 years (43/75, 57.0%), followed by those aged 36-45 years (26/75, 35.0%) and <35 years (6/75, 8.0%). Overall, TNBC was the most common subtype, identified in 28 patients (37.33%), followed by HR+/HER2− disease in 23 patients (30.66%) and HR+/HER2+ disease in 9 patients (12.0%). Within the <35-year age group, HR+/HER2− and TNBC were equally represented, each accounting for 2 cases, while HR+/HER2-low and not-done status accounted for 1 case each. Among patients aged 36-45 years, TNBC was the predominant subtype, observed in 12 cases, followed by HR+/HER2− in 9 cases and HR+/HER2+ in 3 cases. In the >46-year group, TNBC remained the most frequent subtype, comprising 14 cases, followed by HR+/HER2− in 12 cases, not-done status in 8 cases, and HR+/HER2+ in 6 cases. HR−/HER2+ and HR−/HER2-low tumors were detected only in the >46-year group, accounting for 2 and 1 case, respectively. Collectively, the data demonstrate that the study cohort was predominantly composed of older patients, with TNBC and HR+/HER2− tumors representing the principal receptor-defined subtypes. The concentration of TNBC across the 36-45-year and >46-year age groups, together with the low frequency of HER2-low and HR−/HER2+ tumors, highlights the heterogeneous but predominantly hormone receptor-negative subtype distribution within this cohort.
As shown in
Table 1, grade II tumors were the most frequent histological category (45 cases), followed by grade III (26 cases), grade I (3 cases), and ungraded tumors (1 case). Overall, TNBC was the most common receptor subtype (29 cases), followed by HR+/HER2− (24 cases), HR+/HER2+ (9 cases), HR−/HER2+ (2 cases), and not-done status (11 cases).
As shown in
Table 2, most patients were classified as stage II (A+B), accounting for 35 cases, followed by stage IIIA with 15 cases and unstaged disease with 13 cases. Across receptor subtypes, TNBC and HR+/HER2− were the most frequent categories, with 29 and 24 cases, respectively. Stage II (A+B) showed the highest burden of both HR+/HER2− and TNBC tumors, with 13 cases each, while advanced stages III and IV showed comparatively smaller numbers across receptor subtypes.
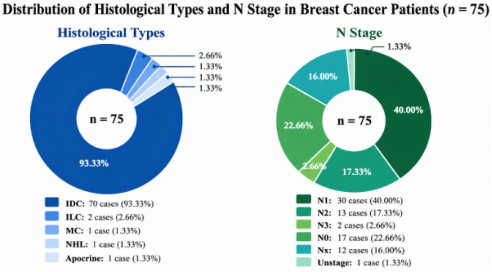
The merged
Figure 10, shows that IDC was the predominant histological type, accounting for 70 of 75 cases (93.33%), while ILC was uncommon 2 cases (2.66%), and MC, NHL, and apocrine carcinoma each represented 1 case (1.33%). Regarding nodal status, N1 was the most frequent N stage with 30 cases (40.0%), followed by N0 with 17 cases (22.66%), N2 with 13 cases (17.33%), Nx with 12 cases (16.0%), N3 with 2 cases (2.66%), and unstaged disease with 1 case (1.33%).
4. Discussion
In this institutional cohort of 75 breast cancer patients, the clinicopathological profile was characterized by predominance of older age, invasive ductal carcinoma, intermediate to high histological grade, T2 disease, nodal involvement, and a high proportion of TNBC and HR+/HER2− tumors. Patients aged >46 years constituted the largest age group, while histologically, invasive ductal carcinoma was overwhelmingly predominant. Most tumors were grade II or grade III, and stage II disease represented the largest AJCC stage category. Receptor-based classification showed that TNBC was the most frequent subtype, followed by HR+/HER2− disease. Together, these findings indicate that the study cohort was enriched for biologically and clinically important disease patterns, particularly intermediate to high grade tumors and hormone receptor/HER2-defined subtypes with distinct therapeutic implications. The age distribution observed in this cohort showed that 57.0% of patients were older than 46 years, whereas 35.0% were aged 36-45 years and 8.0% were younger than 35 years. This pattern is broadly consistent with the established observation that breast cancer incidence increases with age, although breast cancer in South Asian and Bangladeshi populations is often reported at relatively younger ages compared with many Western populations
| [22] | Zohora, F. T., Rabbi, M. F. Study on Epidemiology, Risk Factors and Clinical Characteristics of Triple Negative Breast Cancer in Bangladesh. International Journal of Research in Medical Sciences. 2018, 6(8), 2554-2561.
https://doi.org/10.18203/2320-6012.ijrms20183232 |
| [23] | Fredholm, H., Eaker, S., Frisell, J., Holmberg, L., Fredriksson, I., Lindman, H. Breast Cancer in Young Women: Poor Survival Despite Intensive Treatment. PLOS ONE. 2009, 4(11), e7695. https://doi.org/10.1371/journal.pone.0007695 |
[22, 23]
.
In the present cohort, the substantial proportion of patients aged 36-45 years suggests that a clinically meaningful fraction of cases occurred during the premenopausal or perimenopausal period. This is relevant because younger age at diagnosis may be associated with more aggressive tumor biology, delayed presentation, and distinct receptor patterns in several populations
| [24] | Badowska-Kozakiewicz, A. M., Liszcz, A., Sobol, M., Patera, J. Retrospective Evaluation of Histopathological Examinations in Invasive Ductal Breast Cancer of No Special Type: An Analysis of 691 Patients. Archives of Medical Science. 2017, 13(6), 1408-1415. https://doi.org/10.5114/aoms.2016.60076 |
| [25] | Weigelt, B., Geyer, F. C., Reis-Filho, J. S. Histological Types of Breast Cancer: How Special Are They? Molecular Oncology. 2010, 4(3), 192-208.
https://doi.org/10.1016/j.molonc.2010.04.004 |
[24, 25]
. However, because this study was descriptive and did not include survival or treatment-response data, the age-related distribution should be interpreted as a presentation pattern rather than a prognostic association.
Histological analysis demonstrated a marked predominance of invasive ductal carcinoma, accounting for 70 of 75 cases (93.33%). This finding is consistent with the broader literature, where invasive ductal carcinoma or invasive carcinoma of no special type is recognized as the most common histological type of invasive breast cancer
. The proportion observed in this cohort appears higher than the commonly reported global range, which may reflect the small sample size, institutional case mix, diagnostic referral pattern, or lower representation of special histological subtypes. Less common histological categories, including invasive lobular carcinoma, mucinous carcinoma, apocrine carcinoma, and non-Hodgkin lymphoma, were infrequent. The dominance of invasive ductal carcinoma is clinically relevant because it is a heterogeneous category that includes tumors across a wide range of grades, stages, and receptor-defined subtypes
| [26] | Sohn, V. Y., Arthurs, Z. M., Sebesta, J. A., Brown, T. A. Primary Tumor Location Impacts Breast Cancer Survival. American Journal of Surgery. 2008, 195(5), 641-644.
https://doi.org/10.1016/j.amjsurg.2007.12.039 |
| [27] | Noman, A. S. M., Uddin, M., Rahman, M. Z., Nayeem, M. J., Alam, S. S., Khatun, Z., et al. Overexpression of Sonic Hedgehog in the Triple Negative Breast Cancer: Clinicopathological Characteristics of High Burden Breast Cancer Patients from Bangladesh. Scientific Reports. 2016, 6, 18830.
https://doi.org/10.1038/srep18830 |
[26, 27]
.
Histological grade was another important feature of this cohort. Grade II tumors accounted for 61.33% of cases, followed by grade III tumors in 33.33%, whereas grade I tumors were uncommon. This distribution indicates that most tumors were moderately or poorly differentiated. The Nottingham histological grading system remains a robust and reproducible prognostic tool in invasive breast cancer, and higher grade is associated with more aggressive tumor behavior and poorer clinical outcome
| [7] | Elston, C. W., Ellis, I. O. Pathological Prognostic Factors in Breast Cancer. I. The Value of Histological Grade in Breast Cancer: Experience from a Large Study with Long-Term Follow-Up. Histopathology. 1991, 19(5), 403-410.
https://doi.org/10.1111/j.1365-2559.1991.tb00229.x |
| [8] | Rakha, E. A., El-Sayed, M. E., Lee, A. H. S., Elston, C. W., Grainge, M. J., Hodi, Z., et al. Prognostic Significance of Nottingham Histologic Grade in Invasive Breast Carcinoma. Journal of Clinical Oncology. 2008, 26(19), 3153-3158.
https://doi.org/10.1200/JCO.2007.15.5986 |
[7, 8]
. In this cohort, grade II predominated across age groups and receptor categories, while grade III tumors also represented a substantial fraction, particularly among older patients and TNBC cases. These findings suggest that the cohort was largely composed of tumors with intermediate to high proliferative and morphological aggressiveness, although mitotic index, Ki-67, and outcome data were not available for direct biological correlation.
The anatomical distribution of disease further supports the clinical relevance of the cohort. T2 tumors were the most frequent T stage, representing 65.0% of patients, while T3 and T4 tumors together accounted for more than one-fifth of cases. Similarly, nodal involvement was common: N1, N2, and N3 categories together comprised 45 cases, indicating that a large proportion of patients had regional nodal disease at presentation. In the AJCC distribution, stage II disease was the most frequent overall stage group, followed by stage III disease and a sizeable unstaged subgroup. Since AJCC staging incorporates tumor size, nodal status, distant metastasis, and, in contemporary prognostic staging, biological factors such as grade and receptor status, these findings highlight the importance of integrated stage and biomarker documentation
| [28] | Denkert, C., Seither, F., Schneeweiss, A., Link, T., Blohmer, J. U., Just, M., et al. Clinical and Molecular Characteristics of HER2-Low-Positive Breast Cancer: Pooled Analysis of Individual Patient Data from Four Prospective Neoadjuvant Clinical Trials. The Lancet Oncology. 2021, 22(8), 1151-1161.
https://doi.org/10.1016/S1470-2045(21)00301-6 |
[28]
. The predominance of T2 and node-positive disease may also suggest delayed clinical presentation or referral, although this cannot be confirmed without data on symptom duration, screening history, diagnostic interval, or treatment pathway.
The tumor site distribution showed that the upper outer quadrant was the most common tumor location, accounting for 40.0% of cases, followed by the upper inner quadrant and central region. This pattern is compatible with the recognized tendency for breast tumors to arise more frequently in the upper outer quadrant, which has often been attributed to the greater volume of glandular tissue in that region
. Right-sided tumors were slightly more frequent than left-sided tumors in this cohort, although the difference was modest and should not be overinterpreted in a small descriptive sample. Laterality is generally less prognostically important than stage, grade, nodal status, and receptor profile, but its documentation remains necessary for clinical completeness, surgical planning, and radiotherapy records.
Receptor-status analysis showed that ER−/PR− tumors were the most frequent ER/PR category, accounting for 41.33% of cases, followed by ER+/PR+ tumors in 33.33%. Discordant ER/PR phenotypes were uncommon. The high proportion of ER−/PR− tumors is clinically important because hormone receptor negativity reduces eligibility for endocrine therapy and often overlaps with more aggressive molecular phenotypes, particularly TNBC
| [11] | Allison, K. H., Hammond, M. E. H., Dowsett, M., McKernin, S. E., Carey, L. A., Fitzgibbons, P. L., et al. Estrogen and Progesterone Receptor Testing in Breast Cancer: ASCO/CAP Guideline Update. Journal of Clinical Oncology. 2020, 38(12), 1346-1366. https://doi.org/10.1200/JCO.19.02309 |
| [14] | Perou, C. M., Sørlie, T., Eisen, M. B., van de Rijn, M., Jeffrey, S. S., Rees, C. A., et al. Molecular Portraits of Human Breast Tumours. Nature. 2000, 406(6797), 747-752.
https://doi.org/10.1038/35021093 |
[11, 14]
. Current ASCO/CAP guidance emphasizes standardized ER and PR testing and recommends that tumors with 1% to 100% positive tumor nuclei be interpreted as receptor positive
| [14] | Perou, C. M., Sørlie, T., Eisen, M. B., van de Rijn, M., Jeffrey, S. S., Rees, C. A., et al. Molecular Portraits of Human Breast Tumours. Nature. 2000, 406(6797), 747-752.
https://doi.org/10.1038/35021093 |
[14]
. Therefore, complete and accurate hormone receptor assessment is essential not only for prognostic stratification but also for treatment selection. In this cohort, receptor testing was not performed in 14.66% of cases, which represents an important practical limitation and highlights the need for universal biomarker testing in breast cancer care.
The combined hormone receptor/HER2 classification identified TNBC as the largest subtype, representing 37.33% of cases, followed by HR+/HER2− disease in 30.66%. This finding is clinically notable because TNBC is generally associated with aggressive clinical behavior, higher histological grade, limited endocrine and HER2-targeted treatment options, and a need for chemotherapy-centered or emerging biomarker-directed treatment strategies
| [29] | Kim, E. S., Kim, J. S., Chakrabarty, N., Yun, C. H. Covalent Positioning of Single DNA Molecules for Nanopatterning. Nanomaterials. 2021, 11(7), 1725.
https://doi.org/10.3390/nano11071725 |
| [15] | Lehmann, B. D., Bauer, J. A., Chen, X., Sanders, M. E., Chakravarthy, A. B., Shyr, Y., et al. Identification of Human Triple-Negative Breast Cancer Subtypes and Preclinical Models for Selection of Targeted Therapies. Journal of Clinical Investigation. 2011, 121(7), 2750-2767.
https://doi.org/10.1172/JCI45014 |
[29, 15]
. Previous studies and reviews from Bangladesh and South Asian settings have emphasized the clinical importance of TNBC and the need for more locally generated evidence on its epidemiology and clinicopathological associations
| [10] | Weiss, A., Chavez-MacGregor, M., Lichtensztajn, D. Y., Yi, M., Tadros, A., Hortobagyi, G. N., et al. Validation Study of the American Joint Committee on Cancer Eighth Edition Prognostic Stage Compared with Anatomic Stage in Breast Cancer. JAMA Oncology. 2018, 4(2), 203-209.
https://doi.org/10.1001/jamaoncol.2017.4298 |
| [23] | Fredholm, H., Eaker, S., Frisell, J., Holmberg, L., Fredriksson, I., Lindman, H. Breast Cancer in Young Women: Poor Survival Despite Intensive Treatment. PLOS ONE. 2009, 4(11), e7695. https://doi.org/10.1371/journal.pone.0007695 |
[10, 23]
. In the present cohort, TNBC was common across the 36-45-year and >46-year age groups and was represented in both grade II and grade III tumors. However, because survival outcomes and recurrence data were not available, the prognostic implications of this high TNBC proportion cannot be directly assessed.
HER2 analysis showed that HER2-negative tumors constituted the largest HER2-defined group, accounting for 68.0% of cases, whereas HER2-positive tumors represented 14.66%. HER2-low disease was identified in only 2.66% of cases. The low frequency of HER2-low tumors should be interpreted cautiously because HER2-low classification depends on careful distinction between IHC 0, IHC 1+, and IHC 2+/ISH-negative categories, which may be affected by pre-analytical variables, antibody/platform differences, scoring reproducibility, and reporting practices
| [12] | Wolff, A. C., Somerfield, M. R., Dowsett, M., Hammond, M. E. H., Hayes, D. F., McShane, L. M., et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: ASCO-CAP Guideline Update. Journal of Clinical Oncology. 2023, 41(22), 3867-3872.
https://doi.org/10.1200/JCO.22.02864 |
| [17] | U.S. Food and Drug Administration. FDA Approves Fam-Trastuzumab Deruxtecan-nxki for HER2-Low Breast Cancer. Available from:
https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-fam-trastuzumab-deruxtecan-nxki-her2-low-breast-cancer (accessed 6 May 2026). |
[12, 17]
. HER2-low disease has gained clinical relevance following the DESTINY-Breast04 trial and subsequent FDA approval of trastuzumab deruxtecan for eligible patients with unresectable or metastatic HER2-low breast cancer. However, current ASCO/CAP updates emphasize standardized HER2 interpretation and reporting rather than unvalidated expansion of HER2 categories in routine pathology
| [12] | Wolff, A. C., Somerfield, M. R., Dowsett, M., Hammond, M. E. H., Hayes, D. F., McShane, L. M., et al. Human Epidermal Growth Factor Receptor 2 Testing in Breast Cancer: ASCO-CAP Guideline Update. Journal of Clinical Oncology. 2023, 41(22), 3867-3872.
https://doi.org/10.1200/JCO.22.02864 |
[12]
. Therefore, the HER2-low observation in this cohort should be considered descriptive and hypothesis-generating rather than definitive.
The age-wise subtype distribution provides additional context. TNBC was the most frequent subtype in both the 36-45-year and >46-year groups, whereas HR+/HER2− and TNBC were equally represented among patients aged <35 years. HR−/HER2+ and HR−/HER2-low tumors were observed only among patients aged >46 years. Although these findings suggest age-related variation in receptor-defined subtype distribution, the small number of patients in the youngest group limits meaningful comparison. Similarly, the stage-wise receptor distribution showed that stage II disease carried the largest burden of both HR+/HER2− and TNBC tumors. This may reflect the overall predominance of stage II cases rather than a true stage-specific enrichment of receptor subtypes. Larger studies with statistical testing would be required to determine whether receptor patterns are significantly associated with age, histological grade, nodal status, or AJCC stage.
The present study has several limitations. First, the sample size was relatively small, and the analysis was based on a single institutional cohort, limiting generalizability. Second, the retrospective descriptive design depended on the completeness and accuracy of available pathology and clinical records. Third, receptor testing and staging were incomplete in a subset of cases, leading to “Not Done”, “Unstage,” and “Ungraded” categories. Fourth, the study did not include survival, recurrence, treatment, Ki-67, genomic assay, or detailed imaging data, preventing assessment of prognostic outcomes or treatment-response associations. Fifth, no inferential statistics were performed, so observed differences across age, grade, and stage categories should be interpreted descriptively rather than causally.
Despite these limitations, the study provides a structured overview of clinicopathological and receptor-defined breast cancer patterns in an institutional cohort. Its strength lies in integrating multiple routinely available variables, including age, tumor site, laterality, histological type, histological grade, T stage, N stage, AJCC stage, ER/PR status, HER2 status, HER2-low status, and combined subtype categories. This integrated approach is clinically useful because modern breast cancer interpretation requires simultaneous consideration of anatomical disease burden, histological aggressiveness, and biomarker-defined therapeutic groups.