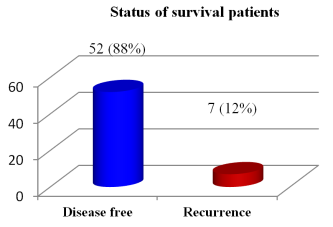
Cervical cancer remains a significant health burden, particularly in low- and middle-income countries, where over 85% of cases occur. Bangladesh exhibits crude incidence and mortality rates of 10.2 and 6.1 per 100,000, respectively, highlighting the impact of cervical cancer. This retrospective study, conducted at Rajshahi Medical College Hospital, assessed 141 cervical cancer patients treated with brachytherapy between December 2016 and December 2020. The primary objective was to examine survival outcomes and associated mortality factors in relation to the stage of cervical cancer at diagnosis. The study revealed that 59 patients (42%) were alive at the time of analysis, of which 88% had achieved disease-free survival. Conversely, 35 patients (25%) were deceased, with advanced-stage disease being predominant among them. Renal failure was identified as the leading cause of death (37%). Results suggest that early-stage cervical cancer correlates with improved survival outcomes, underscoring the necessity of early detection and prompt treatment. Despite the curative potential of brachytherapy when combined with external beam radiotherapy and cisplatin-based chemotherapy, global disparities in access to brachytherapy hinder effective cervical cancer management, particularly in low-resource settings. Enhanced screening programs, vaccination efforts, and broader access to advanced treatment modalities, including brachytherapy, are critical in reducing cervical cancer-related mortality in low- and middle-income countries.
| Published in | Radiation Science and Technology (Volume 10, Issue 4) |
| DOI | 10.11648/j.rst.20241004.11 |
| Page(s) | 56-65 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Cervical Cancer, Brachytherapy, Survival Outcomes, Low- and Middle-Income Countries, Renal Failure, Radiotherapy, HPV
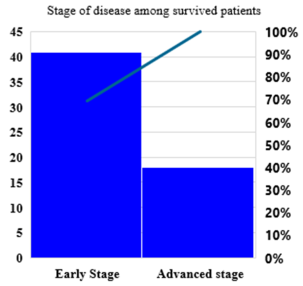
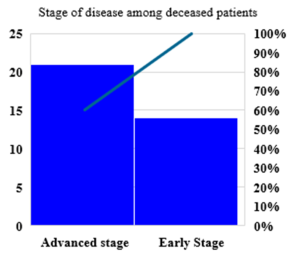
Early stage | Advanced stage | P-value | |
|---|---|---|---|
Survived patient | 41 | 18 | 0.009626 |
Deceased | 14 | 21 | |
Total | 55 | 39 |
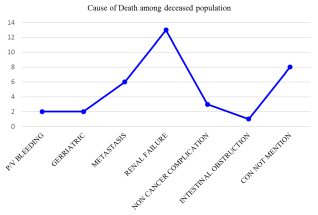
Cause of Death | RMCH (%) | Global Study A (%) | Global Study B (%) |
|---|---|---|---|
Renal Failure | 37% | 30% | 35% |
Metastatic Complications | 17% | 25% | 20% |
Geriatric | 6% | 10% | 8% |
P/V Bleeding | 6% | 8% | 5% |
Intestinal Obstruction | 3% | 5% | 3% |
Non-Cancer Related Issues | 9% | 12% | 15% |
Unspecified | 23% | 10% | 14% |
Treatment Modality | Disease-Free Survival (%) | Overall Survival (%) | Recurrence Rate (%) |
|---|---|---|---|
Intracavitary Brachytherapy | 88% | 75% | 12% |
Interstitial Brachytherapy | 92% | 80% | 8% |
Combined Modality | 95% | 82% | 5% |
HPV | Human Papillomavirus |
EBRT | External Beam Radiation Therapy |
GLOBOCAN | Global Cancer Incidence, Mortality and Prevalence Database |
RMCH | Rajshahi Medical College & Hospital |
RT | Radiotherapy |
BT | Brachytherapy |
| [1] | Arbyn M, Weiderpass E, Bruni L, de Sanjosé S, Saraiya M, Ferlay J, Bray F. Estimates of incidence and mortality of cervical cancer in 2018: a worldwide analysis. Lancet Glob Health. 2020, 8(2), e191-e203. |
| [2] | Stelze, Dominik et al. Estimates of the global burden of cervical cancer associated with HIV. The Lancet. 2020. |
| [3] | Guida F, Kidman R, Ferlay J, et al. Global and regional estimates of orphans attributed to maternal cancer mortality in 2020. Nat Med. 2022, 28, 2563–2572. |
| [4] | Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021, 71(3), 209-249. |
| [5] | Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018, 68(6), 394-424. |
| [6] | Song J, Alyamani N, Bhattacharya G, Le T, E C, Samant R. The Impact of High-Dose-Rate Brachytherapy: Measuring Clinical Outcomes in the Primary Treatment of Cervical Cancer. Adv Radiat Oncol. 2020, 5(3), 419-425. |
| [7] | Arbyn M, Castellsagué X, de Sanjosé S, Bruni L, Saraiya M, Bray F, Ferlay J. Worldwide burden of cervical cancer in 2008. Ann Oncol. 2011, 22(12), 2675-2686. |
| [8] | Chino J, Annunziata CM, Beriwal S, et al. Radiation Therapy for Cervical Cancer: Executive Summary of an ASTRO Clinical Practice Guideline. Pract Radiat Oncol. 2020, 10(4), 220-234. |
| [9] | Lichter K, Anakwenze Akinfenwa C, MacDuffie E, et al. Treatment of cervical cancer: overcoming challenges in access to brachytherapy. Expert Rev Anticancer Ther. 2022, 22(4), 353-359. |
| [10] | Chakrabarty N, Chung HJ, Alam R, et al. Chemico-Pharmacological Screening of the Methanol Extract of Gynura nepalensis D.C. Deciphered Promising Antioxidant and Hepatoprotective Potentials: Evidenced from in vitro, in vivo, and Computer-Aided Studies. Molecules. 2022, 27(11), 3474. |
| [11] | Karim MA, Ghosh AK, Khatun RA, Khatun J, Chakrabarty N. Comparative Study of Two Thoracic External Beam Radiotherapy Regimen 30Gy in 10 Fractions Versus 20Gy in 5 Fractions for Palliation of Symptoms in Non-Small Cell Lung Cancer. Radiation Science and Technology. 2024; 10(3): 43-55. |
| [12] | Skowronek J, Malicki J, Piotrowski T. Values of biologically equivalent doses in healthy tissues: comparison of PDR and HDR brachytherapy techniques. Brachytherapy. 2010, 9(2), 165-170. |
| [13] | Skowronek J. Low-dose-rate or high-dose-rate brachytherapy in treatment of prostate cancer - between options. J Contemp Brachytherapy. 2013, 5(1), 33-41. |
| [14] | Chin J, Rumble RB, Kollmeier M, et al. Brachytherapy for Patients With Prostate Cancer: American Society of Clinical Oncology/Cancer Care Ontario Joint Guideline Update. J Clin Oncol. 2017, 35(15), 1737-1743. |
| [15] | Viswanathan AN, Erickson BA, Ibbott GS, et al. The American College of Radiology and the American Brachytherapy Society practice parameter for the performance of low-dose-rate brachytherapy. Brachytherapy. 2017, 16(1), 68-74. |
| [16] | Hsu IC, Yamada Y, Assimos DG, et al. ACR Appropriateness Criteria high-dose-rate brachytherapy for prostate cancer. Brachytherapy. 2014, 13(1), 27-31. |
| [17] | Erickson BA, Bittner NH, Chadha M, et al. The American College of Radiology and the American Brachytherapy Society practice parameter for the performance of radionuclide-based high-dose-rate brachytherapy. Brachytherapy. 2017, 16(1), 75-84. |
| [18] | Skowronek J. Pulsed dose rate brachytherapy - is it the right way? J Contemp Brachytherapy. 2010, 2(3), 107-113. |
| [19] | Haie-Meder, C., Pötter, R., Van Limbergen, E., Briot, E., De Brabandere, M., Dimopoulos, J., et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiotherapy and Oncology. 2010, 74(3), 235–245. |
| [20] | Nag, S., Erickson, B., Thomadsen, B., Orton, C., Demanes, J. D., & Petereit, D. The American Brachytherapy Society recommendations for high-dose-rate brachytherapy for carcinoma of the cervix. International Journal of Radiation Oncology, Biology, Physics. 2004, 58(2), 885–888. |
| [21] | Viswanathan, A. N., Beriwal, S., De Los Santos, J. F., Demanes, D. J., Gaffney, D., Hansen, J., et al. American Brachytherapy Society consensus guidelines for locally advanced carcinoma of the cervix. Part I: General principles. Brachytherapy. 2012, 11(1), 33–46. |
| [22] | Pötter, R., Haie-Meder, C., Van Limbergen, E., Barillot, I., De Brabandere, M., Dimopoulos, J., et al. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy—3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiotherapy and Oncology. 2006, 78(1), 67–77. |
| [23] | Kim, Y. J., Kang, H. C., & Kim, Y. S. Impact of brachytherapy technique (2D versus 3D) on outcomes of cervical cancer: A systematic review and meta-analysis. Research Square. 2017. |
| [24] | Guedea F, Ventura M, Londres B, et al. Overview of brachytherapy resources in Latin America: a patterns-of-care survey. Brachytherapy. 2011, 10(5), 363-368. |
| [25] | Abdel-Wahab M, Gondhowiardjo SS, Rosa AA, et al. Global Radiotherapy: Current Status and Future Directions-White Paper. JCO Glob Oncol. 2021, 7, 827-842. |
| [26] | Chopra S, Shukla R, Budukh A, Shrivastava SK. External Radiation and Brachytherapy Resource Deficit for Cervical Cancer in India: Call to Action for Treatment of All. J Glob Oncol. 2019, 5, 1-5. |
| [27] | Small W Jr, Bacon MA, Bajaj A, et al. Cervical cancer: A global health crisis. Cancer. 2017, 123(13), 2404-2412. |
| [28] | Nath R, Anderson LL, Meli JA, et al. Code of practice for brachytherapy physics: Report of the AAPM Radiation Therapy Committee Task Group No. 56. Med Phys. 1997, 24(10), 1557-1598. |
| [29] | Pötter R, Tanderup K, Kirisits C, et al. The EMBRACE II study: the outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies. Clin Transl Radiat Oncol. 2018, 9, 48-60. |
| [30] | Fokdal, L., Sturdza, A., Mazeron, R., et al. Image guided adaptive brachytherapy with combined intracavitary and interstitial technique improves the therapeutic ratio in locally advanced cervical cancer: analysis from the retroEMBRACE study. Radiotherapy and Oncology. 2016, 120(3), 434–440. |
| [31] | Hatcher, J. B., Oladeru, O., Chang, B., Malhotra, S., Mcleod, M., Shulman, A., Dempsey, C., Mula-Hussain, L., Tassoto, M., Sandwall, P., Dieterich, S., Sulieman, L., Roa, D., Li, B. Impact of High-Dose-Rate Brachytherapy Training via Telehealth in Low- and Middle-Income Countries. JCO Global Oncology. 2020, 6, 1803-1812. |
| [32] | Petereit, D. G. Increasing global access to brachytherapy: the ABS 300 in 10 initiative and ongoing international efforts. Brachytherapy. 2022, 21(1), 1–3. |
| [33] | Croke, J., Fyles, A., Barbera, L., D'Souza, D., Pearcey, R., Stuckless, T., Bass, B., Brundage, M., Milosevic, M. Radiation therapy quality-of-care indicators for locally advanced cervical cancer: A consensus guideline. Practical Radiation Oncology. 2016, 6(5), 315-323. |
| [34] | Schad, M., Kowalchuk, R., Beriwal, S., Showalter, T. N. How might financial pressures have impacted brachytherapy? A proposed narrative to explain the declines in cervical and prostate brachytherapy utilization. Brachytherapy. 2019, 18(6), 780-786. |
| [35] | Bauer-Nilsen, K., Hill, C., Trifiletti, D. M., Libby, B., Lash, D. H., Lain, M., Christodoulou, D., Hodge, C., Showalter, T. N. Evaluation of Delivery Costs for External Beam Radiation Therapy and Brachytherapy for Locally Advanced Cervical Cancer Using Time-Driven Activity-Based Costing. International Journal of Radiation Oncology, Biology, Physics. 2018, 100(1), 88-94. |
| [36] | Schad, M. D., Patel, A. K., Glaser, S. M., Balasubramani, G. K., Showalter, T. N., Beriwal, S., Vargo, J. A. Declining brachytherapy utilization for cervical cancer patients - Have we reversed the trend? Gynecologic Oncology. 2020, 156(3), 583-590. |
| [37] | Lichter, K., Anakwenze Akinfenwa, C., MacDuffie, E., Bhatia, R., Small, C., Croke, J., Small, W. Jr., Chino, J., Petereit, D., Grover, S. Treatment of cervical cancer: overcoming challenges in access to brachytherapy. Expert Review of Anticancer Therapy. 2022, 22(4), 353-359. |
| [38] |
Medicare Program; Specialty Care Models To Improve Quality of Care and Reduce Expenditures. Federal Register. 2020. Available from:
https://www.federalregister.gov/documents/2020/09/29/2020-20907 |
| [39] | Hosen SMZ, Kabir MSH, Hasanat A, Chowdhury TA, Chakrabarty N, Sarker SK, Habib MR, Dash R. Docking and ADME/T Analysis of Silibinin as a Potential Inhibitor of EGFR Kinase for Ovarian Cancer Therapy. J Appl Pharm Sci. 2016; 6(8): 1-8. |
| [40] |
Brady, L. W., Micaily, B., Miyamoto, C. T., Heilmann, H. P., Montemaggi, P. Innovations in brachytherapy in gynecologic oncology. Cancer. 1995, 76(10 Suppl), 2143-2151.
https://doi.org/10.1002/1097-0142(19951115)76:10+<2143::aid-cncr2820761339>3.0.co;2 |
| [41] | Wit, E. M., Horenblas, S. Urological complications after treatment of cervical cancer. Nature Reviews Urology. 2014, 11(2), 110-117. |
| [42] | Siegel, R. L., Miller, K. D., Fuchs, H. E., Jemal, A. Cancer statistics, 2022. CA: A Cancer Journal for Clinicians. 2022, 72(1), 7-33. |
| [43] | Mishra, K., Desai, A., Patel, S., Mankad, M., Dave, K. Role of percutaneous nephrostomy in advanced cervical carcinoma with obstructive uropathy: a case series. Indian Journal of Palliative Care. 2009, 15(1), 37-40. |
APA Style
Julekha, K., Md. Abdul, K., Shahrin, J., Mawa, C. J., Saikat, B. (2024). Mortality Predictors and Survival Analysis in Cervical Cancer Patients Treated with Brachytherapy: A Retrospective Study at RMCH. Radiation Science and Technology, 10(4), 56-65. https://doi.org/10.11648/j.rst.20241004.11
ACS Style
Julekha, K.; Md. Abdul, K.; Shahrin, J.; Mawa, C. J.; Saikat, B. Mortality Predictors and Survival Analysis in Cervical Cancer Patients Treated with Brachytherapy: A Retrospective Study at RMCH. Radiat. Sci. Technol. 2024, 10(4), 56-65. doi: 10.11648/j.rst.20241004.11
AMA Style
Julekha K, Md. Abdul K, Shahrin J, Mawa CJ, Saikat B. Mortality Predictors and Survival Analysis in Cervical Cancer Patients Treated with Brachytherapy: A Retrospective Study at RMCH. Radiat Sci Technol. 2024;10(4):56-65. doi: 10.11648/j.rst.20241004.11
@article{10.11648/j.rst.20241004.11,
author = {Khatun Julekha and Karim Md. Abdul and Jahan Shahrin and Chowdhury Jannatul Mawa and Biswas Saikat},
title = {Mortality Predictors and Survival Analysis in Cervical Cancer Patients Treated with Brachytherapy: A Retrospective Study at RMCH
},
journal = {Radiation Science and Technology},
volume = {10},
number = {4},
pages = {56-65},
doi = {10.11648/j.rst.20241004.11},
url = {https://doi.org/10.11648/j.rst.20241004.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.rst.20241004.11},
abstract = {Cervical cancer remains a significant health burden, particularly in low- and middle-income countries, where over 85% of cases occur. Bangladesh exhibits crude incidence and mortality rates of 10.2 and 6.1 per 100,000, respectively, highlighting the impact of cervical cancer. This retrospective study, conducted at Rajshahi Medical College Hospital, assessed 141 cervical cancer patients treated with brachytherapy between December 2016 and December 2020. The primary objective was to examine survival outcomes and associated mortality factors in relation to the stage of cervical cancer at diagnosis. The study revealed that 59 patients (42%) were alive at the time of analysis, of which 88% had achieved disease-free survival. Conversely, 35 patients (25%) were deceased, with advanced-stage disease being predominant among them. Renal failure was identified as the leading cause of death (37%). Results suggest that early-stage cervical cancer correlates with improved survival outcomes, underscoring the necessity of early detection and prompt treatment. Despite the curative potential of brachytherapy when combined with external beam radiotherapy and cisplatin-based chemotherapy, global disparities in access to brachytherapy hinder effective cervical cancer management, particularly in low-resource settings. Enhanced screening programs, vaccination efforts, and broader access to advanced treatment modalities, including brachytherapy, are critical in reducing cervical cancer-related mortality in low- and middle-income countries.
},
year = {2024}
}
TY - JOUR T1 - Mortality Predictors and Survival Analysis in Cervical Cancer Patients Treated with Brachytherapy: A Retrospective Study at RMCH AU - Khatun Julekha AU - Karim Md. Abdul AU - Jahan Shahrin AU - Chowdhury Jannatul Mawa AU - Biswas Saikat Y1 - 2024/12/19 PY - 2024 N1 - https://doi.org/10.11648/j.rst.20241004.11 DO - 10.11648/j.rst.20241004.11 T2 - Radiation Science and Technology JF - Radiation Science and Technology JO - Radiation Science and Technology SP - 56 EP - 65 PB - Science Publishing Group SN - 2575-5943 UR - https://doi.org/10.11648/j.rst.20241004.11 AB - Cervical cancer remains a significant health burden, particularly in low- and middle-income countries, where over 85% of cases occur. Bangladesh exhibits crude incidence and mortality rates of 10.2 and 6.1 per 100,000, respectively, highlighting the impact of cervical cancer. This retrospective study, conducted at Rajshahi Medical College Hospital, assessed 141 cervical cancer patients treated with brachytherapy between December 2016 and December 2020. The primary objective was to examine survival outcomes and associated mortality factors in relation to the stage of cervical cancer at diagnosis. The study revealed that 59 patients (42%) were alive at the time of analysis, of which 88% had achieved disease-free survival. Conversely, 35 patients (25%) were deceased, with advanced-stage disease being predominant among them. Renal failure was identified as the leading cause of death (37%). Results suggest that early-stage cervical cancer correlates with improved survival outcomes, underscoring the necessity of early detection and prompt treatment. Despite the curative potential of brachytherapy when combined with external beam radiotherapy and cisplatin-based chemotherapy, global disparities in access to brachytherapy hinder effective cervical cancer management, particularly in low-resource settings. Enhanced screening programs, vaccination efforts, and broader access to advanced treatment modalities, including brachytherapy, are critical in reducing cervical cancer-related mortality in low- and middle-income countries. VL - 10 IS - 4 ER -
Department of Radiotherapy, Rajshahi Medical College Hospital, Rajshahi, Bangladesh
Biography: Khatun Julekha is a distinguished oncologist with over 6 years of experience specializing in the treatment and management of cancer. She is currently affiliated with the department of Radiotherapy Rajshahi Medical College Hospital. Specializing in the medical management of cancer through chemotherapy, targeted therapy, immunotherapy, and hormonal therapy, she has made significant contributions to the care and well-being of patients dealing with cancer. Dr. Julekha Khatun earned her medical degree MBBS from Rajshahi Medical College Hospital followed by FCPS in Radiotherapy from Bangladesh College of Physician & Surgeon (BCPS) in January 2019. She had training on brachytherapy in 2015 from India
Research Fields: Brachytherapy, Combination Therapies, Clinical Oncology.

Department of Radiotherapy, Rajshahi Medical College Hospital, Rajshahi, Bangladesh
Research Fields: Radiotherapy, Immunotherapy, Geriatric Oncology.
Sher-E-Bangla Medical College Hospital, Barishal, Bangladesh
Research Fields: Chemotherapy Optimization, Palliative Care & Management.
Exim Bank Hospital, Mirpur, Dhaka, Bangladesh
Research Fields: Non-Communicable disease, Patient Safety and Quality Improvement.
Department of Medicine, BGC Trust Medical College, Chittagong, Bangladesh
Research Fields: Connective tissue disease, Drug-drug/protein interaction, Infectious disease, Genetic disease.
Information