Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive technique proposed for recovery of gait and balance in patients with Parkinson's disease (PD). Our aim was to evaluate the effects of rTMS in PD patients by clinical evaluation and computerized gait analysis. Ten patients were recruited. Each patient was assessed before and after a single session of rTMS by: Berg Scale, Unified Parkinson Disease Rating Scale (UPDRS), 6 Minute Walking Test (6MWT), 10MWT, Time Up and Go (TUG) and spatial-temporal gait analysis by Pablo Gait Assessment sensor. We availed of STM 9000, stimulating with 2000 pulses of 20 Hz rTMS, delivered in 5-second trains with 25 seconds between trains, on the hand area of the motor cortex at 90% resting motor threshold (RMT) on each hemisphere, with 5 minutes pause between hemispheres. Eighty percent of the patient reported subjective benefits, corroborated by objective examination of the results. A significant improvement on the Berg scale was observed. Moreover, a tendence to a significant decrease of stiffness at the lower limbs was evident at UPDRS. Gait analysis showed not significant improvements of evaluated parameters. Although it is premature to draw conclusions, because of the small number of patients, underwent to a single session of rTMS, we confirm the possible beneficial effects and the safety of rTMS. Further studies are needed to validate our findings by clinical evaluation and gait analysis at short, medium, and long term. These may be different in relation to the age, duration and stage of the disease, prevalence of tremor or akinesia and rigidity.
| Published in | Rehabilitation Science (Volume 9, Issue 2) |
| DOI | 10.11648/j.rs.20240902.11 |
| Page(s) | 13-20 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Parkinson Disease, Transcranial Magnetic Stimulation, Unified Parkinson Disease Rating Scale, Berg Balance Scale, 6- and 10-Minute Walking Test, Time Up and Go, Space-Temporal Gait Analysis
Age | 55.9±6.89 |
Sex | M: F (5:5) |
Age of onset of PD | 50.2±8.13 |
Mean duration of the disease | 5.7±3.16 |
Score of Hoehn and Yahr scale | 2.1±0.53 |
Score of MDS-UPDRS III scale | 25.5±11.48 |
Pre-TMS | Post-TMS | |
|---|---|---|
Correlations disease duration | ||
UPDRS | r 0.28 | r 0.38 |
Berg scale | r -0.47 | r -0.37 |
Correations Hoehn Yahr scale | ||
UPDRS | r 0.33 | r 0.41 |
Berg scale | r -0.66 | r -0.60 |
TUG | r 0.31 | r 0.40 |
10MWT | r -0.38 | r -0.61 |
PD | Parkinson Disease |
rTMS | repetitive Transcranial Magnetic Stimulation |
UPDRS | Unified Parkinson Disease Rating Scale |
HY | Hoehn Yahr |
TUG | Time Up and Go |
MWT | Minute Walking Test |
| [1] | GBD 206 Neurology Collaborators. Global, regional and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019, 18, 459-480. |
| [2] | Tysnes O. B., Storstein A. Epidemiology of Parkinson’s disease. J Neural Transm, 124, 901-905. |
| [3] | Tolosa E., Garrido A., Scholz S. W., Poewe W. Challenges in the diagnosis of Parkinson’s disease. Lancet. 2021, 20, 385-397. |
| [4] | Marsden C. D.: Parkinson’s disease. J Neurol Neurosurg Psy. 1994, 57, 672-681. |
| [5] | Chaudhuri K. R., Healy D. G., Schapira A. H. Non-motor symptoms of Parkinson’s disease: diagnosis and management. Lancet Neurol. 2006, 5, 235-245. |
| [6] | Jankovic J. Parkinson’s disease: clinical features and diagnosis. J Neurol Neurosurg Psy 2008, 79, 368–37., |
| [7] | Kerr G. K., Worringham C. J., Cole M. H., Lacerez P. F., Wood J. M., Silburn P. A. Predictors of future falls in Parkinson disease. Neurol. 2010, 75, 116-124. |
| [8] | Braak H., Del Tredici K., Rub U., de VOS RAI, Steur ENHJ, Braak E. Staging of brain pathology related to sporadic Parkinson’s disease. Neurobiol Aging. 2003 24, 197. |
| [9] | Rietdijk C. D., Perez-Pardo P., Garssen J., van Wezel R. J. A. and Kraneveld A. D. Exploring Braak’s Hypothesis pf Parkinson’s Disease. Front Neurol. 2017, 8, 37. |
| [10] | Grimes D., Fitzpatrick M., Gordon J., Miyasaki J., Fon E. A., Schlossmacher M., Suchowersky O., Rajput A., Lafontaine A. L., Mestre T., Appel-Cresswell S., Kalia S. K., Schoffer K., Zurowski M., Postuma R. B., Udow S., Fox S., Barbeau P., Hutton B. Canadian guideline for Parkinson disease. CMAJ. 2019, 191(36), E989-E1004. |
| [11] | Morris M. E., Huxham F. E., McGinley J., Iansek, R. Gait disorders and gait rehabilitation in Parkinson’s disease. Adv. Neurol. 2001, 87, 347–361. |
| [12] | Fisicaro F., Lanza G., Grasso A. A., Pennisi G., Bella R., Paulus W. and Pennisi M. Repetitive transcraniak magnetic stimulation in stroke rehabilitation: reviw of the current evidence and pitfalls. Ther Adv Neurol Dis, 2019, 12. |
| [13] | Abdulhameed T., Abdul Hanif Khan Y. K., Liyana Najwa I. M., Hamidon B. and Wan Aliaa Wan S. Repetitive Transcranial Magnetic Stimulation of the Primary Motor Cortex beyond Motor Rehabilitation: A Review of the Current Evidence. Brain Sci. 2022, 12, 761. |
| [14] | Yang C., Guo Z., Peng H., Xing G., Chen H., McClure M., He B., He L., Du F., Xiong L., Mu Q. Repetitive transcranial magnetic stimulation therapy for motor recovery in Parkinson’s disease: a metanalysis. Brain and Behavior 2018, 8, 1-17. |
| [15] | Chen R., Classen J., Gerloff C., Celnik P., Wassermann E. M., Hallett M. et al.. Depression of motor cortex excitability by low-frequency transcranial magnetic stimulation. Neurology. 1997, 48, 1398–403. |
| [16] | Leone A., Valls-Solé J., Wassermann E. M., Hallett M. (Responses to rapid-rate transcranial magnetic stimulation of the human motor cortex. Brain. 1994, 117(Pt4), 847–858. |
| [17] | Huang Y., Edwards M. J., Rounis E., Bhatia K. P., Rothwell J. C. Theta burst stimulation of the human motor cortex. Neuron. 2005, 45, 2016. |
| [18] | Deng S., Dong Z., Pan L., Liu Y., Ye Z., Qin L., Liu Q., Qin C. Effects of repetitive transcranialmagnetic stimulation on gait disorders and cognitive dysfunction in Parkinson’s disease: A systematic review with meta-analysis. Brain Behav. 2022, 12, e2697. |
| [19] | Zhou J, Chen Y., MA, Gin T., Bao D, and Zhou J. The Effects of Repetitive Transcranial Magnetic Stimulation on Standing Balance and Walking in Older Adults with Age-related Neurological Disorders: A Systematic Review and Meta-analysis. Gerontol A Biol Sci Med Sci. 2023, 78, 842–852. |
| [20] | Li S., Jiao R., Zhou X., Chen S. Motor recovery and antidepressant effects of repetitive transcranial magnetic stimulation on Parkinson disease A. PRISMA-compliant meta-analysis. Medicine 2020, 99, 18, |
| [21] | Dong K., Zhu X., Xiao W., Gan C., Luo Y., Jiang M., Liu H. and Chen X. Comparative efficacy of transcranial magnetic stimulation on different targets in Parkinson’s disease: A Bayesian network meta-analysis. Frontiers in Aging Neuroscience. 2023. |
| [22] | Zhang W., Deng B., Xie F., Zhou H., Guo J. F., Jiang H., Sim A., Tang B., and Wang Q.: Efficacy of repetitive transcranial magnetic stimulation in Parkinson’s disease: A systematic review and meta-analysis of randomised controlled trials. EClinicalMedicine. 2022, 52, 101589. |
| [23] | Dias A. E., Barbosa E. R., Coracini, K., Maia, F.: Marcolin M. A., Fregni F. Effects of repetitive transcranial magnetic stimulation on voice and speech in Parkinson’s disease. Acta Neurol. Scand. 2006, 113, 92–99. |
| [24] | Eliasova I., Mekyska J., Kostalova M., Marecek R., Smekal Z., Rektorova I. Acoustic evaluation of short-term effects of repetitive transcranial magnetic stimulation on motor aspects of speech in Parkinson’s disease. J. Neural Transm. 2013, 120, 597–605. |
| [25] | Brabenec L., Klobusiakova P., Barton M., Mekyska J., Galaz Z., Zvoncak V., Kiska, T., Mucha J., Smekal Z., Kostalova M. et al. Non-invasive stimulation of the auditory feedback area for improved articulation in Parkinson’s disease. Parkinsonism Relat Disord. 2019, 61, 187–192. |
| [26] | Wu† Y. I., Cao† X. B., Zeng W. Q., Zhai H., Zhang X. Q., Yang X. M., Cheng C., Wang J. L., Yang X. M. and Xu Y. Transcranial Magnetic Stimulation Alleviates Levodopa-Induced Dyskinesia in Parkinson’s Disease and the Related Mechanisms: A Mini-Review. Frontiers in Neurology. 2021, 12, 758345. |
| [27] | Brusa L., Versace V., Koch G., Iani C., Stanzione P., Bernardi G., Centonze D.: Low frequency rTMS of the SMA transiently ameliorates peak-dose LID in Parkinson’s disease. Clin Neurophys. 2006, 117, 1917-1921. |
| [28] | Lohse A., Meder D., Nielsen S., Lund A. E., Herz D. M., Løkkegaard A. et al. Low frequency transcranial stimulation of pre-supplementary motor area alleviates levodopa-induced dyskinesia in Parkinson’s disease: a randomized crossover trial. Brain Commun. 2020, 2, 1-15, fcaa147. |
| [29] | Khedr E. M., Mohamed K. O., Ali A. M., Hasan A. M. The effect of repetitive transcranial magnetic stimulation on cognitive impairment in Parkinson’s disease with dementia: Pilot study. Restor Neurol Neurosci. 2020, 38, 55–66. |
| [30] | Fuggetta G., Pavone E. F., Fiaschi A., Manganotti P. Acute modulation of cortical oscillatory activities during short trains of high-frequency repetitive transcranial magnetic stimulation of the human motor cortex: A combined EEG and TMS study. Hum Brain Mapp. 2008, 29, 1–13. |
| [31] | Bestmann S., Baudewig J., Siebner H. R., Rothwell J. C., Frahm J.. Functional MRI of the immediate impact of transcranial magnetic stimulation on cortical and subcortical motor circuits. Eur J Neurosci. 2004, 19, 1950–1962. |
| [32] | Keck M. E., Welt T., Muller M. B., Erhardt A., Ohl F., Toschi N., Holsboer F., Sillaber I. Repetitive transcranial magnetic stimulation increases the release of dopamnine in the mesolimbic and mesostriatal system. Comparative Study, Neuropharmacology. 2002, 43, 101-109. |
| [33] | Strafella A. P., Ko J. H., Grant J., Fraraccio M., and Monchi O. Corticostriatal functional interactions in Parkinson’s disease: a rTMS / [11C] raclopride PET study. Eur J Neurosci. 2005, 22, 2946–2952. |
| [34] | Kim J. Y., Chung E. J., Lee W. Y., Shin H. Y., Lee G. H., Choe Y. S. et al. Therapeutic effect of repetitive transcranial magnetic stimulation in Parkinson’s disease: analysis of [11C] raclopride PET study. Mov Disord. 2008, 23, 207–211. |
| [35] | Peng Z., Zhou C., Xue S., Bai J., Yu S., Wang H. and Tan Q. Mechanisms pf repetitive transcranial magnetic stimulation for depression. Shanghai Arch Psy. 2018, 30, 84-92. |
| [36] | Aceves-Serrano L., Neva J. L. and Doudet D. J.. Insight Into the Effects of Clinical Repetitive Transcranial Magnetic Stimulation on the Brain From Positron Emission Tomography and Magnetic Resonance Imaging Studies: A Narrative Review. Frontiers in Neuroscience. 2022, 16, Article 787403. |
| [37] | Chou Y. H., Hickey P. T., Sundman M., Song A. W. and Chen N. K. Effects of Repetitive Transcranial Magnetic Stimulation on Motor Symptoms in Parkinson Disease: A Systematic Review and Meta-analysis. JAMA Neurol. 2015, 72, 432–440. |
APA Style
Teresa, D. P. M., Alfredo, L. C., Maria, S., Raffaele, G., Francesca, T., et al. (2024). Effects of a Single Session of Repetitive Transcranial Stimulation in Parkinson Disease. Rehabilitation Science, 9(2), 13-20. https://doi.org/10.11648/j.rs.20240902.11
ACS Style
Teresa, D. P. M.; Alfredo, L. C.; Maria, S.; Raffaele, G.; Francesca, T., et al. Effects of a Single Session of Repetitive Transcranial Stimulation in Parkinson Disease. Rehabil. Sci. 2024, 9(2), 13-20. doi: 10.11648/j.rs.20240902.11
AMA Style
Teresa DPM, Alfredo LC, Maria S, Raffaele G, Francesca T, et al. Effects of a Single Session of Repetitive Transcranial Stimulation in Parkinson Disease. Rehabil Sci. 2024;9(2):13-20. doi: 10.11648/j.rs.20240902.11
@article{10.11648/j.rs.20240902.11,
author = {Del Prete Maria Teresa and Lerin Calvo Alfredo and Sanchez Maria and Gizzi Raffaele and Tecce Francesca and Moretti Antimo and Fiori Patrizia},
title = {Effects of a Single Session of Repetitive Transcranial Stimulation in Parkinson Disease
},
journal = {Rehabilitation Science},
volume = {9},
number = {2},
pages = {13-20},
doi = {10.11648/j.rs.20240902.11},
url = {https://doi.org/10.11648/j.rs.20240902.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.rs.20240902.11},
abstract = {Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive technique proposed for recovery of gait and balance in patients with Parkinson's disease (PD). Our aim was to evaluate the effects of rTMS in PD patients by clinical evaluation and computerized gait analysis. Ten patients were recruited. Each patient was assessed before and after a single session of rTMS by: Berg Scale, Unified Parkinson Disease Rating Scale (UPDRS), 6 Minute Walking Test (6MWT), 10MWT, Time Up and Go (TUG) and spatial-temporal gait analysis by Pablo Gait Assessment sensor. We availed of STM 9000, stimulating with 2000 pulses of 20 Hz rTMS, delivered in 5-second trains with 25 seconds between trains, on the hand area of the motor cortex at 90% resting motor threshold (RMT) on each hemisphere, with 5 minutes pause between hemispheres. Eighty percent of the patient reported subjective benefits, corroborated by objective examination of the results. A significant improvement on the Berg scale was observed. Moreover, a tendence to a significant decrease of stiffness at the lower limbs was evident at UPDRS. Gait analysis showed not significant improvements of evaluated parameters. Although it is premature to draw conclusions, because of the small number of patients, underwent to a single session of rTMS, we confirm the possible beneficial effects and the safety of rTMS. Further studies are needed to validate our findings by clinical evaluation and gait analysis at short, medium, and long term. These may be different in relation to the age, duration and stage of the disease, prevalence of tremor or akinesia and rigidity.
},
year = {2024}
}
TY - JOUR T1 - Effects of a Single Session of Repetitive Transcranial Stimulation in Parkinson Disease AU - Del Prete Maria Teresa AU - Lerin Calvo Alfredo AU - Sanchez Maria AU - Gizzi Raffaele AU - Tecce Francesca AU - Moretti Antimo AU - Fiori Patrizia Y1 - 2024/07/23 PY - 2024 N1 - https://doi.org/10.11648/j.rs.20240902.11 DO - 10.11648/j.rs.20240902.11 T2 - Rehabilitation Science JF - Rehabilitation Science JO - Rehabilitation Science SP - 13 EP - 20 PB - Science Publishing Group SN - 2637-594X UR - https://doi.org/10.11648/j.rs.20240902.11 AB - Repetitive transcranial magnetic stimulation (rTMS) is a non-invasive technique proposed for recovery of gait and balance in patients with Parkinson's disease (PD). Our aim was to evaluate the effects of rTMS in PD patients by clinical evaluation and computerized gait analysis. Ten patients were recruited. Each patient was assessed before and after a single session of rTMS by: Berg Scale, Unified Parkinson Disease Rating Scale (UPDRS), 6 Minute Walking Test (6MWT), 10MWT, Time Up and Go (TUG) and spatial-temporal gait analysis by Pablo Gait Assessment sensor. We availed of STM 9000, stimulating with 2000 pulses of 20 Hz rTMS, delivered in 5-second trains with 25 seconds between trains, on the hand area of the motor cortex at 90% resting motor threshold (RMT) on each hemisphere, with 5 minutes pause between hemispheres. Eighty percent of the patient reported subjective benefits, corroborated by objective examination of the results. A significant improvement on the Berg scale was observed. Moreover, a tendence to a significant decrease of stiffness at the lower limbs was evident at UPDRS. Gait analysis showed not significant improvements of evaluated parameters. Although it is premature to draw conclusions, because of the small number of patients, underwent to a single session of rTMS, we confirm the possible beneficial effects and the safety of rTMS. Further studies are needed to validate our findings by clinical evaluation and gait analysis at short, medium, and long term. These may be different in relation to the age, duration and stage of the disease, prevalence of tremor or akinesia and rigidity. VL - 9 IS - 2 ER -

Rey Juan Carlos University, Neuron Center, Madrid, Spain
Biography: Lerin Calvo Alfredo: He graduated in Physiotherapy at the Superior Centre of University Studies, “La Salle,” Madrid, in 2018. He got a Master Degree in Advanced Physiotherapy and Treatment of Pain in 2019. He has been charged of the Degree of Professor of Physiotherapy and Health Sciences at the above-mentioned University since February 2022. He is also physiotherapist at the Neuron Centre, Madrid (Spain).
Research Fields: Rehabilitation



Moscati Hospital, ASL AV, University of Campania “Luigi Vanvitelli”, Avellino, Italy
Biography: Moretti Antimo: He graduated in Medicine and Surgery at the II University of Naples in 2011. He got the European Certificate in Physical and Rehabilitation Medicine 2017. He has been charged of the role of Professor of Physical and Rehabilitation Medicine since 2018, Professor of General Methodology of Rehabilitation and Kinesiology, Biomechanics of Skeletal Muscles at the Bachelor Program of Physical Therapy from 2016 to 2018, Professor of Physical and Rehabilitation Medicine at the University of Campania, Vanvitelli from 2019. He is President of the Course of Physiotherapy, Management of Theoretical-Practical Teaching activities at the above-mentioned University, Caserta (Italy), from 2023. He has organized and attended several meetings and published on national and international journals.
Research Fields: Rehabilitation

Neurology, S. Ottone Frangipane Hospital, ASL AV, University of Campania “Luigi Vanvitelli”, Ariano Irpino, Italy
Biography: Fiori Patrizia: She graduated in Medicine and Surgery in 1991. She got the degree of Doctor of Philosophy in Neuroscience in 1995 and Neurology in 1999. She has been working as Physician in general and neurological centres from 2000 to June 2006, as Neurologist at S. Ottone Frangipane Hospital, Ariano irpino (Avellino) since June 2006. She has been charged of the role of Professor of Neurology at the II University of Naples, University of Campania, Vanvitelli, Criscuoli-Frieri Hospital, S. Angelo dei Lombardi (Avellino, Italy) since 2009. She has attended several congresses and published on national and international journals.
Research Fields: Neurology, Rehabilitation, Neuroscience

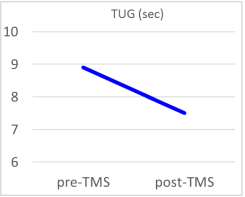
Figure 1. Pre-TMS (left) and post-TMS (right) TUG.
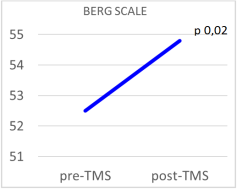
Figure 2. Pre-TMS (left) and post-TMS (right) Berg Scale.
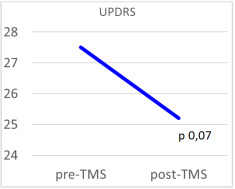
Figure 3. Pre-TMS (left) and post-TMS (right) UPDRS.
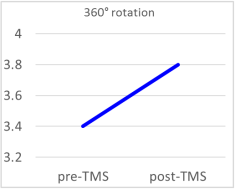
Figure 4. Pre-TMS (left) and post-TMS (right) 360° rotation.
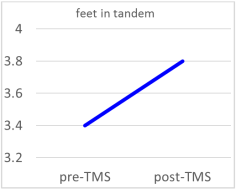
Figure 5. Pre-TMS (left) and post-TMS (right) feet in tandem.
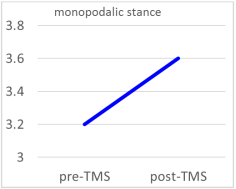
Figure 6. Pre-TMS (left) and post-TMS (right) monopodalic stance.
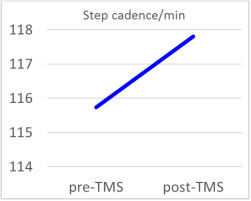
Figure 7. Pre-TMS (left) and post-TMS (right) step cadence.
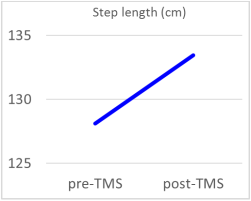
Figure 8. Pre-TMS (left) and post-TMS (right) step length.
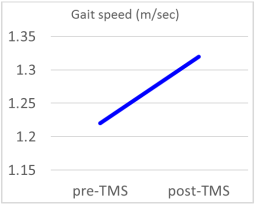
Figure 9. Pre-TMS (left) and post-TMS (right) gait speed.
Information

