Abstract
Background: Gastroesophageal reflux disease (GERD) is a prevalent condition with significant impact on quality of life. When medical therapy fails, surgical intervention—most commonly Nissen (NF) or Toupet fundoplication (TF)—is indicated. The optimal technique, however, remains debated. Aim: To compare the efficacy, functional outcomes, and complication profiles of Nissen and Toupet fundoplication in the surgical management of GERD. Methods: A systematic review was conducted in accordance with PRISMA guidelines. PubMed/MEDLINE, Cochrane, SciELO, and LILACS databases were searched for studies published between 2002 and 2025. Randomized controlled trials and cohort studies comparing NF and TF with at least 12 months of follow-up were included. Primary outcomes were postoperative dysphagia and reflux control. Secondary outcomes included proton pump inhibitor (PPI) use, quality of life (QoL), patient satisfaction, and reoperation rates. Results: Nine studies comprising 2,130 patients were included, including six randomized controlled trials. Both techniques provided effective and sustained reflux control. Nissen fundoplication demonstrated higher postoperative lower esophageal sphincter pressure and slightly better objective acid suppression in some studies; however, this did not translate into superior long-term clinical outcomes. Toupet fundoplication was associated with lower rates of early postoperative dysphagia and better preservation of esophageal motility. Long-term outcomes—including PPI use, QoL, and patient satisfaction—were comparable between techniques. Differences in dysphagia diminished over time. Conclusion: Nissen and Toupet fundoplication offer equivalent long-term control of GERD. While NF provides greater sphincter augmentation, TF achieves similar clinical outcomes with fewer early functional side effects. Surgical decision-making should prioritize esophageal motility and patient-specific characteristics rather than maximal acid suppression alone.
|
Published in
|
Journal of Surgery (Volume 14, Issue 3)
|
|
DOI
|
10.11648/j.js.20261403.12
|
|
Page(s)
|
49-59 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2026. Published by Science Publishing Group
|
Keywords
Gastroesophageal Reflux Disease, Nissen Fundoplication, Toupet Fundoplication
1. Introduction
Gastroesophageal reflux disease (GERD) is a chronic digestive condition characterized by the abnormal backflow of gastric contents into the esophagus, leading to symptoms such as heartburn, regurgitation, chest pain, and, in more severe cases, complications such as esophagitis, esophageal stricture, and Barrett’s esophagus
| [8] | Fass R, Fennerty MB, Vakil N. Nonerosive reflux disease: current concepts and dilemmas. Am J Gastroenterol. 2001; 96(2): 303–14. |
| [23] | Shaqran TM, Ismaeel MM, Alnuaman AA, et al. Epidemiology, causes, and management of gastro-esophageal reflux disease: a systematic review. Cureus. 2023; 15(10): e47420. |
[8, 23]
. Additionally, extra-gastrointestinal complications may occur, including dental erosions, laryngitis, chronic cough, asthma, sinusitis, and idiopathic pulmonary fibrosis, highlighting the systemic nature of this condition.
The prevalence of GERD has been increasing globally, particularly in Western countries, and is currently considered one of the most common gastrointestinal disorders. It is estimated that the prevalence reaches approximately 20% of the population in countries such as the United States, with a progressive increase also observed in developing countries, possibly associated with the westernization of dietary habits and the rising rates of obesity
| [6] | Dent J, El-Serag HB, Wallander MA, Johansson S. Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2005; 54(5): 710–7. |
| [7] | Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of gastro-oesophageal reflux disease: a meta-analysis. Gut. 2018; 67(3): 430–40.
https://doi.org/10.1136/gutjnl-2016-313589 |
| [30] | Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006; 101(8): 1900–20. |
[6, 7, 30]
. Studies also report a significant impact of GERD on quality of life, increased healthcare costs, and higher incidence of complications such as Barrett’s esophagus and esophageal adenocarcinoma
.
GERD primarily involves dysfunction and transient relaxations of the lower esophageal sphincter (LES), hiatal hernia, and increased intra-abdominal pressure, along with factors such as esophageal hypersensitivity and delayed gastric emptying
. Risk factors for this condition include age, obesity, and Western dietary habits
| [6] | Dent J, El-Serag HB, Wallander MA, Johansson S. Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2005; 54(5): 710–7. |
| [30] | Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006; 101(8): 1900–20. |
| [32] | Zhang M, Hou ZK, Huang ZB, Chen XL, Liu FB. Dietary and lifestyle factors related to gastroesophageal reflux disease: a systematic review. Ther Clin Risk Manag. 2021; 17: 305–23. |
[6, 30, 32]
.
Among the most commonly performed surgical procedures for GERD treatment are fundoplication techniques, which involve reconfiguring the gastric fundus to wrap it circumferentially or partially around the distal esophagus, creating an effective valvular mechanism that restores the anti-reflux barrier function
| [24] | Sharma P, Yadlapati R. Pathophysiology and treatment options for gastroesophageal reflux disease: looking beyond acid. Ann N Y Acad Sci. 2021; 1486(1): 3–14. |
| [27] | Stein HJ, Castell DO, Sifrim D, et al. Surgical management of gastroesophageal reflux disease: consensus statement of the International Society for Diseases of the Esophagus. Dis Esophagus. 2018; 31(1): 1–16. |
[24, 27]
. The two main techniques are the Nissen total fundoplication and the Toupet posterior partial fundoplication.
Nissen fundoplication (NF), first described in 1956, consists of a 360° wrap of the distal esophagus with the gastric fundus, forming an anti-reflux valve that reinforces the LES
| [3] | Bonavina L, Bona D, Aiolfi A, Shabat G, Annese V, Galassi L. Fundoplication: old concept for novel challenges? Visc Med. 2024; 40(5): 236–41. |
| [19] | Nissen R. A simple surgical procedure to treat reflux esophagitis. Swiss Medical Weekly.. 1956; 86: 590–2. |
[3, 19]
. This procedure can be performed via a laparoscopic approach, which is associated with lower morbidity rates, shorter hospital stays, and faster recovery
| [25] | Song KY. Complications after antireflux surgery (ARS) and their management. Foregut Surg. 2022; 2(1): 1–7. |
[25]
.
As an alternative to the Nissen technique, Toupet posterior partial fundoplication (270°) was described in 1961 and is particularly indicated for patients with esophageal motility disorders or those at higher risk of postoperative dysphagia
| [4] | Bonavina L. Toupet versus Nissen fundoplication for gastroesophageal reflux disease: are the outcomes different? Dig Med Res. 2023; 6: 4. https://doi.org/10.1159/000531234 |
| [29] | Toupet A. Surgical technique for the treatment of gastroesophageal reflux. Mem Acad Chir (Paris). 1961; 87: 164–7. |
[4, 29]
. In this technique, the gastric fundus is partially wrapped around the posterior aspect of the esophagus, leaving the anterior aspect free. This approach aims to minimize side effects associated with total fundoplication, such as dysphagia and gas-bloat syndrome, while maintaining effective reflux control
| [5] | Carlson MA, Frantzides CT. Complications and results of primary minimally invasive antireflux procedures: a review of 10,735 reported cases. J Am Coll Surg. 2001; 193: 428–39. |
| [10] | Frazzon O, Wada M, Cambruzzi E. Comparative evaluation between total and partial posterior fundoplication in the surgical treatment of gastroesophageal reflux disease.. Arq Bras Cir Dig. 2013; 26(2): 116–21. |
[5, 10]
.
Comparative studies between the Nissen and Toupet fundoplication techniques have shown similar results in terms of GERD symptom control. However, they differ in the frequency of adverse effects: the Nissen technique is more often associated with persistent dysphagia, whereas the Toupet technique tends to better preserve esophageal function
| [13] | Håkanson BS, Lundell L, Öberg S, Ruth M. Comparison of laparoscopic 270° posterior partial fundoplication vs total fundoplication for treatment of gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2019; 154(6): 479–86.
https://doi.org/10.1001/jamasurg.2019.0262 |
| [28] | Strate U, Emmermann A, Fibbe C, Layer P, Zornig C. Laparoscopic fundoplication: Nissen versus Toupet two-year outcome of a prospective randomized study of 200 patients regarding preoperative esophageal motility. Surg Endosc. 2008; 22(1): 21–30. |
| [34] | Wang B, Yin J, Cui L, et al. A Chinese randomized prospective trial of floppy Nissen and Toupet fundoplication for gastroesophageal disease. Int J Surg. 2015; 23: 35–40. |
[13, 28, 34]
. These differences in outcomes make it difficult to establish a definitive consensus on the superiority of one technique over the other, highlighting the need for individualized surgical approaches based on each patient's clinical and functional characteristics.
The choice between techniques often depends on the surgeon’s experience, the patient’s clinical status, and the presence of functional abnormalities such as esophageal motility disorders, in which partial fundoplication may be preferable to reduce dysphagia symptoms
| [9] | Franco MC, Campos JM, Dantas RO. Preoperative esophageal manometry predicts outcome of laparoscopic antireflux surgery. Arq Gastroenterol. 2013; 50(1): 12–7. |
| [17] | Lee Y, Tahir U, Tessier L, Yang K, Hassan T, Dang J, et al. Long-term outcomes following Dor, Toupet, and Nissen fundoplication: a network meta-analysis of randomized controlled trials. Surg Endosc. 2023; 37(7): 5052–64. |
[9, 17]
. Preoperative esophageal manometry thus becomes an essential tool for appropriately selecting the surgical technique.
Given the clinical relevance of GERD and the need to understand the technical aspects, advantages, and limitations of NF and TF, this study aims to conduct a systematic review of the literature regarding these two surgical approaches. The objective is to provide an updated comparative analysis, grounded in the available evidence, to support a better understanding of the indication criteria and outcomes associated with each technique.
2. Methods
This is a systematic literature review aiming to compare the Nissen and Toupet fundoplication techniques in the surgical treatment of gastroesophageal reflux disease (GERD), based on clinical evidence available in the literature.
2.1. Study Type
This review considered studies that compared the Nissen and Toupet fundoplication techniques and their respective outcomes in adult patients diagnosed with GERD.
2.2. Inclusion Criteria
Studies that met the following criteria were included:
1) Direct comparison between Nissen fundoplication and Toupet fundoplication;
2) Randomized clinical trials (RCTs) or cohort studies;
3) Population composed of adults (≥18 years) with a confirmed diagnosis of GERD;
4) Minimum postoperative follow-up of 12 months;
5) Presentation of quantitative data related to at least one of the following outcomes: postoperative dysphagia, reflux control, continued use of PPIs, quality of life and satisfaction, and reoperations;
6) Publications in Portuguese, English, or Spanish, with access to the full text.
2.3. Exclusion Criteria
The following were excluded:
1) Studies with inadequate design;
2) Studies with a pediatric population (age <18 years);
3) Duplicate studies;
4) Studies with insufficient or incomplete data, or that did not present relevant information for the outcomes of interest;
5) Studies without a direct comparison between Nissen fundoplication and Toupet fundoplication;
6) Publications in languages other than Portuguese, English, or Spanish, or without access to the full text.
2.4. Search Strategy
The search strategy was designed to identify studies that directly compared the Nissen and Toupet fundoplication techniques in the surgical treatment of gastroesophageal reflux disease (GERD). A systematic search was conducted in the PubMed/MEDLINE, Cochrane, SciELO, and LILACS databases, including publications from January 2002 to July 2025, in Portuguese, English, and Spanish.
The strategy was developed using a combination of controlled descriptors (DeCS/MeSH) and free-text keywords, applying the Boolean operators AND and OR to refine the results. The search terms included: ‘Nissen fundoplication’, ‘Toupet fundoplication’, ‘posterior partial fundoplication’, ‘posterior total fundoplication’, ‘laparoscopic Nissen’, ‘laparoscopic Toupet’, ‘laparoscopic fundoplication’, ‘gastroesophageal reflux disease’, ‘GERD’, ‘antireflux surgery’, ‘surgical treatment of GERD’, ‘fundoplication techniques’, ‘fundoplication outcomes’, ‘fundoplication comparison’, ‘Nissen versus Toupet’, and their equivalents in the selected search languages.
Search expressions were adapted to the specifications of each database. In PubMed/MEDLINE, Medical Subject Headings (MeSH) terms were prioritized; in Cochrane, specific filters for systematic reviews and randomized controlled trials available on the platform were applied; while in SciELO and LILACS, Descritores em Ciências da Saúde (DeCS) and their respective translations were used. Filters for study type (randomized controlled trials), language, and full-text availability were also applied.
The selection of studies retrieved followed the eligibility criteria previously defined in this methodology.
2.5. Study Selection
Screening was performed in two stages by two independent reviewers: initial assessment of titles and abstracts, followed by full-text evaluation of potentially eligible articles. In cases of disagreement between reviewers, a third reviewer was consulted.
2.6. Data Extraction and Analysis
The extracted data included the number of participants per group, incidence of persistent dysphagia, recurrence of GERD symptoms, continuous use of proton pump inhibitors (PPIs), and patient satisfaction levels. The information was organized into tables and analyzed descriptively and comparatively across the included studies.
2.7. Assessed Outcomes
1) Primary outcomes: postoperative dysphagia and reflux control;
2) Secondary outcomes: continued PPI use, quality of life and satisfaction, and reoperations.
3. Results
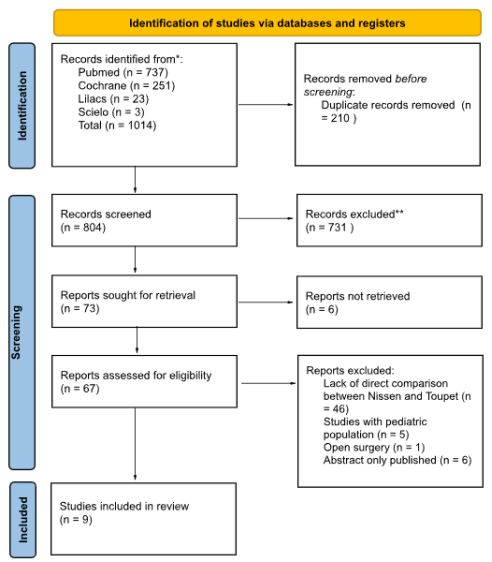
A total of 1,014 records were identified across the PubMed, Cochrane, LILACS, and SciELO databases. After the removal of 210 duplicates, 804 records were screened, of which 731 were excluded based on titles and abstracts. Seventy-three studies were selected for full-text assessment; however, 6 could not be retrieved. Of the 67 full-text articles assessed, 58 were excluded for meeting exclusion criteria. Thus, 9 studies were included in the present systematic review. The complete selection process is illustrated in the PRISMA flow diagram (
Figure 1), which details the identification, screening, eligibility, and inclusion phases.
The included studies were published between 2002 and 2022 and were conducted in six different countries. The total sample comprised 2,130 patients, of whom 1,140 underwent Toupet fundoplication and 990 underwent Nissen fundoplication. Methodological designs included three cohort studies and six randomized controlled trials (RCTs).
The mean age of patients ranged from 46.6 to 57 years. Sample sizes varied between 84 and 456 participants, and follow-up periods ranged from 12 months to 16 years, indicating variability in study objectives and approaches. The characteristics of the studies included in this review are summarized in
Table 1.
Figure 1. PRISMA flow diagram of this review.
3.1. Characteristics of the Included Studies
Table 1. Description of studies included in the review.
Author/Year | Type of Study | Country | Number of patients (Toupet/Nissen) | Average age (Toupet/Nissen) (years) | Follow-up |
Zügel et al. (2002) | Retrospective cohort | Germany | 162 (122 T / 40 N) | 46.6 (±1.6) / 45.2 (±3.2) | 19 months (average) |
Radajewski et al. (2009) | Prospective cohort | Austria | 94 (43 T / 51 N) | 54.0 / 47.0 | 12 months |
Gunter et al. (2017) | Retrospective cohort | USA | 316 (155 T / 161 N) | 56.6±14.6 / 51.6±13.8 | 1, 3 and 5 years |
Strate et al. (2008) | RCT | Germany | 200 (100 T / 100 N) | Average of 56 (20-80) | 2 years |
Qin et al. (2013) | RCT | China | 383 (168 T / 215 N) | Average of 56.3 (34-82) | 5.6 years (average) |
Koch et al. (2013) | RCT | Austria | 125 (63 T / 62 N) | 51.87 (25-81) / 50.32 (20-76) | 1 year |
Wang et al. (2015) | RCT | China | 84 (41 T / 43 N) | 57.0±10.8 / 57.0±13.2 | 2 years |
Håkanson et al. (2019) | RCT | Sweden | 456 (229 T / 227 N) | 47.9±11.7 / 50.2±11.7 | 5 years |
Analatos et al. (2022) | RCT | Sweden | 310 (159 T / 151 N) | 65 (±11.0) / 67 (±11.3) | 16 years (average) |
3.2. Reflux Control
Table 2. Reflux control according to fundoplication technique.
Study (Year) | Type of Fundoplication | Outcome: DeMeester Score (pre vs post) | P-value | Remarks |
Koch et al. (2013) | Toupet | 24.69±18.0 vs. 6.94±13.72 | <0.01 | No significant differences |
Koch et al. (2013) | Nissen | 25.15±21.69 vs. 7.99±22.30 | <0.01 | |
Wang et al. (2015) | Toupet | 42.58±39.38 vs. 12.03±2.18 | <0.05 | |
Wang et al. (2015) | Nissen | 43.0±42.1 vs. 10.37±3.10 | <0.05 | Lower in Nissen group |
Analatos et al. (2022) | Toupet | GSRS Reflux: 1.4±0.7 (1 year); 1.9±1.2 (15 years) | 0.18 (15 years) | Symptoms are equally well controlled |
Analatos et al. (2022) | Nissen | GSRS Reflux: 1.3±0.7 (1 year); 1.7±1.1 (15 years) | | |
The analyzed studies demonstrated that both surgical techniques, Nissen fundoplication (NF) and Toupet fundoplication (TF), provide effective control of gastroesophageal reflux symptoms. These findings are detailed in
Table 2, which presents reflux scores (DeMeester and GSRS) comparing pre- and postoperative periods between the evaluated techniques.
Koch et al. (2013) and Wang et al. (2015) reported significant improvements in DeMeester scores in both groups, with lower postoperative values observed in the Nissen group. Specifically, Wang et al. found a significantly lower final score in the Nissen group (p = 0.007), suggesting a potential superiority in acid suppression. However, Strate et al. (2008) and Analatos et al. (2022) found no significant differences between the groups during medium- and long-term follow-up. Qin et al. (2013), in a study involving 383 patients with a mean follow-up of 5.6 years, reported complete symptom resolution in both groups, although recurrence occurred in 18 patients in the Toupet group.
3.3. Use of Proton Pump Inhibitors
Table 3. Postoperative use of proton pump inhibitors (PPIs).
Study (Year) | Surgical Technique | No. of Patients | Follow-up | PPI Use (%) | Remarks |
Koch et al (2013) | Nissen and Toupet | 125 (T=63 e N=62) | 1 year | | Both groups showed normalized pH levels and reflux episodes; equivalent effectiveness |
Qin et al. (2013) | Nissen | 215 | Average 5.6 years | 0% symptomatic recurrence | High endoscopic cure rate (88.4%); no additional use reported |
Qin et al. (2013) | Toupet | 168 | Average 5.6 years | ≈10.7% (18 patients) | Recurrence treated with PPIs; objective parameters normalized |
Gunter et al. (2017) | Nissen | 161 | 1, 3, and 5 years | 22% at 5 years | Gradual increase in use; satisfaction similar between NF and TF |
Gunter et al. (2017) | Toupet | 155 | 1, 3, and 5 years | 27% at 5 years | More frequent use in the Toupet group, but no statistical difference (p>0.05) |
Analatos et al. (2022) | Nissen | 151 | >15 years | | Effective symptom control; similar use of PPIs among groups |
Analatos et al. (2022) | Toupet | 159 | >15 years | | Differences in dysphagia disappear over the long term; equally reflux controlled |
The postoperative use of proton pump inhibitors (PPIs) was evaluated as an indirect indicator of symptomatic recurrence.
Table 3 provides a summary of PPI usage rates at different follow-up intervals according to the surgical technique performed.
Qin et al. (2013) reported that none of the patients in the Nissen group resumed PPI use, whereas approximately 10.7% of patients in the Toupet group required medication. Gunter et al. (2017) observed a gradual increase in PPI use over a five-year follow-up: 22% in the Nissen group and 27% in the Toupet group, with no statistically significant difference (p > 0.05). Similar findings were reported by Analatos et al. (2022) after more than 15 years of follow-up. Koch et al. (2013) confirmed normalization of pH monitoring results in both groups.
3.4. Postoperative Dysphagia
Table 4. Postoperative dysphagia.
Study (Year) | Type of Fundoplication | Dysphagia Incidence/Score (post-op) | P-value | Remarks |
Qin et al. (2013) | Nissen | 27.9% (4 days); 1.4% (12 months) | | The difference significantly decreases over time |
Qin et al. (2013) | Toupet | 16.7% (4 days); 0% (12 months) | | |
Wang et al. (2015) | Nissen | 22.5% (last follow-up) | P=0.023 | Higher in the Nissen group |
Wang et al. (2015) | Toupet | 5.0% (last follow-up) | | Lower rate in the Toupet group in the short term |
Analatos et al. (2022) | Nissen (liquids) | 1.1 (0.4) (1 year); 1.2 (0.5) (15 years) | | |
Analatos et al. (2022) | Toupet (liquids) | 1.0 (0.3) (1 year); 1.2 (0.5) (15 years) | P=0.58 (15 years) | Initial difference favoring TF disappears over time |
Analatos et al. (2022) | Nissen (solids) | 1.3 (0.6) (1 year); 1.3 (0.5) (15 years) | | |
Analatos et al. (2022) | Toupet (solids) | 1.1 (0.4) (1 year); 1.3 (0.6) (15 years) | P=0.97 (15 years) | |
Dysphagia was more prevalent in the group undergoing Nissen fundoplication, particularly during the immediate postoperative period. Complete data on dysphagia incidence and scores are presented in
Table 4, detailing results according to food consistency and follow-up duration.
Qin et al. (2013) reported an incidence of 27.9% in the Nissen group and 16.7% in the Toupet group during the first four days, which declined to 1.4% and 0%, respectively, at 12 months. Wang et al. (2015) observed persistent dysphagia in 22.5% of Nissen patients compared to only 5% in the Toupet group (p = 0.023). Gunter et al. (2017) recorded a higher dysphagia score in the first year for the Nissen group (Eckardt 2.35 vs. 1.61), a difference that disappeared in subsequent years. In a 15-year follow-up, Analatos et al. (2022) found no significant differences between groups regarding dysphagia for solids or liquids (p > 0.5).
3.5. Quality of Life and Satisfaction
Table 5. Quality of life and satisfaction.
Study (Year) | Type of Fundoplication | % Satisfaction (Post-op) | QoL Outcome (Post-op) | P-value (between groups) | Remarks |
Zügel et al. (2002) | Nissen | 85% | GIQLI: 87.2 → 118.2 (8 months) | | High satisfaction; significant improvement in QoL |
Zügel et al. (2002) | Toupet | 85% | GIQLI: 86.6 / 89.2 → 123.4 / 122.3 (22-23 months) | | High satisfaction; especially used for esophageal motility disorders |
Radajewski et al. (2009) | Nissen | 90% (12 months) | Reflux symptoms improved in 92% | P=0.21 (satisfaction) | No significant difference in satisfaction |
Radajewski et al. (2009) | Toupet | 98% (12 months) | Reflux symptoms improved by 95% | | |
Gunter et al. (2017) | Nissen | 87.0% (1 year); 77.4% (5 years) | GERD-HRQL: 3.48±5.29 (1 year); Eckardt: 2.35±1.58 (1 year) | P=0.67 (satisfaction, 5 years); P=0.03 (Eckardt, 1 year) | Higher initial dysphagia with Nissen, but decreases |
Gunter et al. (2017) | Toupet | 86.8% (1 year); 70.0% (5 years) | GERD-HRQL: 2.45±4.08 (1 year); Eckardt: 1.61±1.98 (1 year) | | |
Håkanson et al. (2019) | Nissen | N/A | Solid dysphagia: 1.3±1.0 (12 months); 1.3±0.9 (24 months) | P<0.001 (solids, 12 months); P=0.001 (solids, 24 months) | Less dysphagia in TF |
Håkanson et al. (2019) | Toupet | N/A | Solid dysphagia: 1.9±1.4 (12 months); 1.7±1.2 (24 months) | | |
Analatos et al. (2022) | Nissen | N/A | SF-36 PCS: 44.4±11.4 (15 years); SF-36 MCS: 48.2±11.1 (15 years) | No significant difference | QoL equally well controlled |
Analatos et al. (2022) | Toupet | N/A | SF-36 PCS: 44.1±13.1 (15 years); SF-36 MCS: 48.5±11.9 (15 years) | | |
Both techniques were effective in improving patient quality of life and satisfaction.
Table 5 summarizes the findings related to patient satisfaction and quality of life, including GIQLI, GERD-HRQL, SF-36, and Eckardt scores.
Zügel et al. (2002) reported an increase in GIQLI scores from 87 to 118 in the Nissen group and from 88 to 123 in the Toupet group, with 85% satisfaction in both. Radajewski et al. (2009) reported 98% satisfaction in the Toupet group and 90% in the Nissen group (p = 0.21), with symptomatic improvement exceeding 90% in both groups. Gunter et al. (2017) presented similar results using the GERD-HRQL scores, with 77.4% satisfaction in the Nissen group and 70% in the Toupet group after five years (p = 0.67). Analatos et al. (2022) found no significant differences in SF-36 or GSRS scores between the groups after 15 years of follow-up.
3.6. Reoperations
The need for reoperation was more common following Nissen fundoplication. Koch et al. (2013) reported that 9.7% of patients in the Nissen group required reintervention within the first year, compared to no cases in the Toupet group. Strate et al. (2008) observed 15 reoperations in the Nissen group and only 4 in the Toupet group. Gunter et al. (2017) found no statistically significant difference (p = 0.14). Wang et al. (2015) reported only one case of hiatal hernia recurrence in each group. Analatos et al. (2022), with follow-up exceeding 15 years, reported reoperation rates of 7% for Nissen and 3% for Toupet (p = 0.08).
4. Discussion
4.1. Reflux Control
The effectiveness of Nissen (NF) and Toupet (TF) fundoplication in controlling acid reflux has been extensively documented in the literature, with both techniques resulting in a significant reduction in reflux episodes and improvement in pH monitoring scores, such as the DeMeester score
| [14] | Katayama Y, Nishikawa K, Shiraishi K, et al. Long-term efficacy of total and partial posterior fundoplication to treat gastroesophageal reflux disease. Dig Med Res. 2022; 5: 5. |
| [16] | Koch OO, Kaindlstorfer A, Antoniou SA, Luketina RR, Berger J, Pointner R. Comparison of results from a randomized trial 1 year after laparoscopic Nissen and Toupet fundoplications. Surg Endosc. 2013; 27(7): 2383–90.
https://doi.org/10.1007/s00464-013-2791-7 |
| [20] | Qin M, Ding G, Yang H. A clinical comparison of laparoscopic Nissen and Toupet fundoplication for gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2013; 23(7): 601–4. https://doi.org/10.1089/lap.2013.0032 |
| [34] | Wang B, Yin J, Cui L, et al. A Chinese randomized prospective trial of floppy Nissen and Toupet fundoplication for gastroesophageal disease. Int J Surg. 2015; 23: 35–40. |
[14, 16, 20, 34]
. Although some studies, such as Wang et al.
| [34] | Wang B, Yin J, Cui L, et al. A Chinese randomized prospective trial of floppy Nissen and Toupet fundoplication for gastroesophageal disease. Int J Surg. 2015; 23: 35–40. |
[34]
, have reported slightly more favorable final pH monitoring values in the NF group, this finding did not necessarily translate into greater clinical efficacy. Long-term follow-up studies, such as Analatos et al.
| [1] | Analatos A, Arvidsson D, Fridriksson J, Lundell L. Clinical outcomes of a laparoscopic total vs a 270° posterior partial fundoplication in chronic gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2022; 157(6): 473–80.
https://doi.org/10.1001/jamasurg.2022.0805 |
[1]
, demonstrated comparable symptomatic control between the techniques, with similar GSRS scores and overall patient satisfaction after 15 years.
Strate et al.
| [28] | Strate U, Emmermann A, Fibbe C, Layer P, Zornig C. Laparoscopic fundoplication: Nissen versus Toupet two-year outcome of a prospective randomized study of 200 patients regarding preoperative esophageal motility. Surg Endosc. 2008; 22(1): 21–30. |
[28]
emphasized that despite technical differences, symptom recurrence after two years did not differ significantly between groups. This suggests that the effectiveness of reflux control should be evaluated not only by objective parameters, but also by the clinical improvement perceived by patients. Furthermore, the data indicate that the choice of surgical technique should not rely solely on postoperative pH monitoring values, but rather on a comprehensive assessment of long-term clinical response and quality of life
| [13] | Håkanson BS, Lundell L, Öberg S, Ruth M. Comparison of laparoscopic 270° posterior partial fundoplication vs total fundoplication for treatment of gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2019; 154(6): 479–86.
https://doi.org/10.1001/jamasurg.2019.0262 |
[13]
.
4.2. Use of Proton Pump Inhibitors
The use of proton pump inhibitors (PPIs) after antireflux surgery has been interpreted by some authors as a possible indicator of therapeutic failure. However, several studies have shown that resumption of PPI use is not necessarily associated with objective recurrence of reflux
| [18] | Lundell L, Bell M, Ruth M. Systematic review: laparoscopic fundoplication for gastroesophageal reflux disease in partial responders to proton pump inhibitors. World J Gastroenterol. 2014; 20(3): 804–13. |
[18]
. Gunter et al.
| [11] | Gunter RL, Talamini MA, Duncan MD, Haskins IN, Truitt MS. Long-term quality of life outcomes following Nissen versus Toupet fundoplication in patients with gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2017; 27(9): 931–6. https://doi.org/10.1089/lap.2017.0123 |
[11]
and Analatos et al.
| [1] | Analatos A, Arvidsson D, Fridriksson J, Lundell L. Clinical outcomes of a laparoscopic total vs a 270° posterior partial fundoplication in chronic gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2022; 157(6): 473–80.
https://doi.org/10.1001/jamasurg.2022.0805 |
[1]
observed that even among patients with normalized pH monitoring, a proportion resumed medication use, which may be explained by functional mechanisms such as visceral hypersensitivity, functional dyspepsia, or negative placebo response.
Studies such as that by Spechler and Hunter
| [26] | Spechler SJ, Hunter JG. Medical and surgical treatment of GERD. N Engl J Med. 2015; 373(8): 756–65. |
[26]
reinforce that up to 30% of patients may resume PPI therapy after fundoplication, even in the absence of endoscopic evidence of GERD recurrence. Thus, although the rate of PPI use may appear slightly higher in the TF group, the difference is not statistically significant and does not compromise the clinical efficacy of the techniques. The long-term follow-up (>15 years) by Analatos et al.
| [1] | Analatos A, Arvidsson D, Fridriksson J, Lundell L. Clinical outcomes of a laparoscopic total vs a 270° posterior partial fundoplication in chronic gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2022; 157(6): 473–80.
https://doi.org/10.1001/jamasurg.2022.0805 |
[1]
demonstrates that PPI use rates tend to equalize over time, confirming that both techniques maintain effective disease control.
4.3. Postoperative Dysphagia
Dysphagia is one of the main postoperative concerns following fundoplication, particularly after the Nissen technique. The literature suggests that a 360° total fundoplication may exert increased pressure on the distal esophagus, impairing bolus transit, especially in patients with borderline esophageal motility
| [4] | Bonavina L. Toupet versus Nissen fundoplication for gastroesophageal reflux disease: are the outcomes different? Dig Med Res. 2023; 6: 4. https://doi.org/10.1159/000531234 |
| [28] | Strate U, Emmermann A, Fibbe C, Layer P, Zornig C. Laparoscopic fundoplication: Nissen versus Toupet two-year outcome of a prospective randomized study of 200 patients regarding preoperative esophageal motility. Surg Endosc. 2008; 22(1): 21–30. |
[4, 28]
. Studies such as those by Qin et al.
| [20] | Qin M, Ding G, Yang H. A clinical comparison of laparoscopic Nissen and Toupet fundoplication for gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2013; 23(7): 601–4. https://doi.org/10.1089/lap.2013.0032 |
[20]
and Wang et al.
| [34] | Wang B, Yin J, Cui L, et al. A Chinese randomized prospective trial of floppy Nissen and Toupet fundoplication for gastroesophageal disease. Int J Surg. 2015; 23: 35–40. |
[34]
confirm a higher incidence of early postoperative dysphagia in NF, with significantly lower rates in the TF group.
However, there is consensus that dysphagia tends to improve over time. Gunter et al.
| [11] | Gunter RL, Talamini MA, Duncan MD, Haskins IN, Truitt MS. Long-term quality of life outcomes following Nissen versus Toupet fundoplication in patients with gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2017; 27(9): 931–6. https://doi.org/10.1089/lap.2017.0123 |
[11]
and Analatos et al.
| [1] | Analatos A, Arvidsson D, Fridriksson J, Lundell L. Clinical outcomes of a laparoscopic total vs a 270° posterior partial fundoplication in chronic gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2022; 157(6): 473–80.
https://doi.org/10.1001/jamasurg.2022.0805 |
[1]
demonstrated that, after a follow-up period of 3 to 5 years, dysphagia scores become similar between the two techniques. This reinforces the notion that transient dysphagia may be expected in the immediate postoperative period, particularly following NF, but rarely persists in the long term. Preoperative manometric evaluation remains an essential tool to tailor the surgical approach and avoid suboptimal outcomes in patients with impaired motility
| [9] | Franco MC, Campos JM, Dantas RO. Preoperative esophageal manometry predicts outcome of laparoscopic antireflux surgery. Arq Gastroenterol. 2013; 50(1): 12–7. |
[9]
.
4.4. Quality of Life and Satisfaction
Improvement in quality of life is one of the primary objectives of anti-reflux surgery, and in this regard, both NF and TF have demonstrated favorable outcomes. Zügel et al.
| [33] | Zügel N, Lang H, Klinge U, Hellinger A, Hüttl TP. A comparison of laparoscopic Toupet versus Nissen fundoplication in gastroesophageal reflux disease. Langenbecks Arch Surg. 2002; 386(7): 494–8. |
[33]
and Radajewski et al.
| [21] | Radajewski R, Lange J, Köckerling F, Franke J. Short-term symptom and quality-of-life comparison between laparoscopic Nissen and Toupet fundoplications. Dis Esophagus. 2009; 22(1): 84–8. |
[21]
reported substantial improvements in GIQLI scores and high levels of satisfaction, regardless of the technique employed. These findings were corroborated by Gunter et al.
| [11] | Gunter RL, Talamini MA, Duncan MD, Haskins IN, Truitt MS. Long-term quality of life outcomes following Nissen versus Toupet fundoplication in patients with gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2017; 27(9): 931–6. https://doi.org/10.1089/lap.2017.0123 |
[11]
and Analatos et al.
| [1] | Analatos A, Arvidsson D, Fridriksson J, Lundell L. Clinical outcomes of a laparoscopic total vs a 270° posterior partial fundoplication in chronic gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2022; 157(6): 473–80.
https://doi.org/10.1001/jamasurg.2022.0805 |
[1]
, who found no statistical differences in quality of life or satisfaction in follow-up periods extending up to 15 years.
Although NF is associated with increased dysphagia in the short term, this does not appear to negatively impact patient satisfaction. The results suggest that the perception of symptom control and overall functional improvement carries more weight in the subjective assessment of patients than transient symptoms such as mild dysphagia. Therefore, the choice of technique should take into account the anatomical and functional aspects of the esophagus, but there is no evidence of superiority in terms of satisfaction between the two techniques
| [13] | Håkanson BS, Lundell L, Öberg S, Ruth M. Comparison of laparoscopic 270° posterior partial fundoplication vs total fundoplication for treatment of gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2019; 154(6): 479–86.
https://doi.org/10.1001/jamasurg.2019.0262 |
[13]
.
4.5. Reoperations
Reoperations following fundoplication are undesirable events that typically reflect technical failures, such as rupture of the cruroplasty or intrathoracic herniation of the valve
| [31] | Van Beek DB, Auyang ED, Soper NJ. A comprehensive review of laparoscopic redo fundoplication. Surg Endosc. 2011; 25(3): 706–12. |
[31]
. Koch et al.
| [16] | Koch OO, Kaindlstorfer A, Antoniou SA, Luketina RR, Berger J, Pointner R. Comparison of results from a randomized trial 1 year after laparoscopic Nissen and Toupet fundoplications. Surg Endosc. 2013; 27(7): 2383–90.
https://doi.org/10.1007/s00464-013-2791-7 |
[16]
and Strate et al.
| [28] | Strate U, Emmermann A, Fibbe C, Layer P, Zornig C. Laparoscopic fundoplication: Nissen versus Toupet two-year outcome of a prospective randomized study of 200 patients regarding preoperative esophageal motility. Surg Endosc. 2008; 22(1): 21–30. |
[28]
identified a higher need for reintervention in the NF group, with causes primarily related to persistent dysphagia and anatomical failures. Conversely, Gunter et al.
| [11] | Gunter RL, Talamini MA, Duncan MD, Haskins IN, Truitt MS. Long-term quality of life outcomes following Nissen versus Toupet fundoplication in patients with gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2017; 27(9): 931–6. https://doi.org/10.1089/lap.2017.0123 |
[11]
and Analatos et al.
| [1] | Analatos A, Arvidsson D, Fridriksson J, Lundell L. Clinical outcomes of a laparoscopic total vs a 270° posterior partial fundoplication in chronic gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2022; 157(6): 473–80.
https://doi.org/10.1001/jamasurg.2022.0805 |
[1]
found no statistically significant differences, despite a higher trend observed in the Nissen group.
The Toupet technique, being less restrictive, may provide greater long-term anatomical stability, particularly in patients with esophageal motility disorders. Rieger et al.
| [22] | Rieger NA, Jamieson GG, Duffy PR, Devitt PG. Reoperation after failed antireflux surgery. Br J Surg. 1994; 81(8): 1159–61. |
[22]
emphasize that the success of fundoplication is directly related to the integrity of the cruroplasty and the appropriate choice of technique based on functional assessments. Therefore, individualization of the surgical approach is essential to minimize reoperation rates and maximize long-term outcomes.
The present review reinforces that the long-standing debate between total and partial fundoplication should not be framed as a question of superiority, but rather of functional trade-offs. Although Nissen fundoplication may achieve slightly greater augmentation of the lower esophageal sphincter and improved acid suppression in selected studies, this advantage does not translate into superior long-term patient-centered outcomes.
5. Conclusion
This literature review demonstrated that both the Nissen and Toupet techniques are effective in the surgical treatment of GERD. Both Nissen and Toupet fundoplication are effective surgical options for GERD, providing durable symptom control and comparable long-term outcomes. However, their functional profiles differ, with Nissen associated with higher rates of early dysphagia and Toupet offering better preservation of esophageal motility.
These findings support a paradigm shift from a “one-size-fits-all” approach toward individualized surgical decision-making. Rather than prioritizing maximal acid suppression, the selection of fundoplication technique should be guided by esophageal function and patient-specific factors, aiming to optimize both efficacy and postoperative quality of life and patient satisfaction.
Abbreviations
GERD | Gastroesophageal Reflux Disease |
NF | Nissen Fundoplication |
TF | Toupet Fundoplication |
LES | Lower Esophageal Sphincter |
PPI | Proton Pump Inhibitor |
QoL | Quality of Life |
RCT | Randomized Controlled Trial |
GIQLI | Gastrointestinal Quality of Life Index |
GSRS | Gastrointestinal Symptom Rating Scale |
SF-36 | Short Form Health Survey |
Author Contributions
Fernando Freire Lisboa: Conceptualization, Project administration, Supervision, Writing – original draft
Gabriel Diniz Camara Dantas: Data curation, Methodology, Writing – review & editing
Angelo Felipe Lima de Araujo Alves: Investigation, Writing – original draft
Luanny Vitoria da Silva Oliveira: Resources, Validation
Conflicts of Interest
The authors have no conflicts of interest to declare.
References
| [1] |
Analatos A, Arvidsson D, Fridriksson J, Lundell L. Clinical outcomes of a laparoscopic total vs a 270° posterior partial fundoplication in chronic gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2022; 157(6): 473–80.
https://doi.org/10.1001/jamasurg.2022.0805
|
| [2] |
Boeckxstaens GE, Rohof WO, Kessing BF. Fundamentals of GERD pathophysiology. Ann N Y Acad Sci. 2020; 1482(1): 19–33.
https://doi.org/10.1111/nyas.14369
|
| [3] |
Bonavina L, Bona D, Aiolfi A, Shabat G, Annese V, Galassi L. Fundoplication: old concept for novel challenges? Visc Med. 2024; 40(5): 236–41.
|
| [4] |
Bonavina L. Toupet versus Nissen fundoplication for gastroesophageal reflux disease: are the outcomes different? Dig Med Res. 2023; 6: 4.
https://doi.org/10.1159/000531234
|
| [5] |
Carlson MA, Frantzides CT. Complications and results of primary minimally invasive antireflux procedures: a review of 10,735 reported cases. J Am Coll Surg. 2001; 193: 428–39.
|
| [6] |
Dent J, El-Serag HB, Wallander MA, Johansson S. Epidemiology of gastro-oesophageal reflux disease: a systematic review. Gut. 2005; 54(5): 710–7.
|
| [7] |
Eusebi LH, Ratnakumaran R, Yuan Y, Solaymani-Dodaran M, Bazzoli F, Ford AC. Global prevalence of gastro-oesophageal reflux disease: a meta-analysis. Gut. 2018; 67(3): 430–40.
https://doi.org/10.1136/gutjnl-2016-313589
|
| [8] |
Fass R, Fennerty MB, Vakil N. Nonerosive reflux disease: current concepts and dilemmas. Am J Gastroenterol. 2001; 96(2): 303–14.
|
| [9] |
Franco MC, Campos JM, Dantas RO. Preoperative esophageal manometry predicts outcome of laparoscopic antireflux surgery. Arq Gastroenterol. 2013; 50(1): 12–7.
|
| [10] |
Frazzon O, Wada M, Cambruzzi E. Comparative evaluation between total and partial posterior fundoplication in the surgical treatment of gastroesophageal reflux disease.. Arq Bras Cir Dig. 2013; 26(2): 116–21.
|
| [11] |
Gunter RL, Talamini MA, Duncan MD, Haskins IN, Truitt MS. Long-term quality of life outcomes following Nissen versus Toupet fundoplication in patients with gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2017; 27(9): 931–6.
https://doi.org/10.1089/lap.2017.0123
|
| [12] |
Gyawali CP, Kahrilas PJ, Savarino E, Zerbib F, Mion F, Smout A, et al. Modern diagnosis of GERD: the Lyon Consensus. Gut. 2018; 67(7): 1351–62.
https://doi.org/10.1136/gutjnl-2017-314722
|
| [13] |
Håkanson BS, Lundell L, Öberg S, Ruth M. Comparison of laparoscopic 270° posterior partial fundoplication vs total fundoplication for treatment of gastroesophageal reflux disease: a randomized clinical trial. JAMA Surg. 2019; 154(6): 479–86.
https://doi.org/10.1001/jamasurg.2019.0262
|
| [14] |
Katayama Y, Nishikawa K, Shiraishi K, et al. Long-term efficacy of total and partial posterior fundoplication to treat gastroesophageal reflux disease. Dig Med Res. 2022; 5: 5.
|
| [15] |
Katz PO, Gerson LB, Vela MF. Guidelines for the diagnosis and management of gastroesophageal reflux disease. Am J Gastroenterol. 2022; 117(1): 27–56.
https://doi.org/10.14309/ajg.0000000000001538
|
| [16] |
Koch OO, Kaindlstorfer A, Antoniou SA, Luketina RR, Berger J, Pointner R. Comparison of results from a randomized trial 1 year after laparoscopic Nissen and Toupet fundoplications. Surg Endosc. 2013; 27(7): 2383–90.
https://doi.org/10.1007/s00464-013-2791-7
|
| [17] |
Lee Y, Tahir U, Tessier L, Yang K, Hassan T, Dang J, et al. Long-term outcomes following Dor, Toupet, and Nissen fundoplication: a network meta-analysis of randomized controlled trials. Surg Endosc. 2023; 37(7): 5052–64.
|
| [18] |
Lundell L, Bell M, Ruth M. Systematic review: laparoscopic fundoplication for gastroesophageal reflux disease in partial responders to proton pump inhibitors. World J Gastroenterol. 2014; 20(3): 804–13.
|
| [19] |
Nissen R. A simple surgical procedure to treat reflux esophagitis. Swiss Medical Weekly.. 1956; 86: 590–2.
|
| [20] |
Qin M, Ding G, Yang H. A clinical comparison of laparoscopic Nissen and Toupet fundoplication for gastroesophageal reflux disease. J Laparoendosc Adv Surg Tech A. 2013; 23(7): 601–4.
https://doi.org/10.1089/lap.2013.0032
|
| [21] |
Radajewski R, Lange J, Köckerling F, Franke J. Short-term symptom and quality-of-life comparison between laparoscopic Nissen and Toupet fundoplications. Dis Esophagus. 2009; 22(1): 84–8.
|
| [22] |
Rieger NA, Jamieson GG, Duffy PR, Devitt PG. Reoperation after failed antireflux surgery. Br J Surg. 1994; 81(8): 1159–61.
|
| [23] |
Shaqran TM, Ismaeel MM, Alnuaman AA, et al. Epidemiology, causes, and management of gastro-esophageal reflux disease: a systematic review. Cureus. 2023; 15(10): e47420.
|
| [24] |
Sharma P, Yadlapati R. Pathophysiology and treatment options for gastroesophageal reflux disease: looking beyond acid. Ann N Y Acad Sci. 2021; 1486(1): 3–14.
|
| [25] |
Song KY. Complications after antireflux surgery (ARS) and their management. Foregut Surg. 2022; 2(1): 1–7.
|
| [26] |
Spechler SJ, Hunter JG. Medical and surgical treatment of GERD. N Engl J Med. 2015; 373(8): 756–65.
|
| [27] |
Stein HJ, Castell DO, Sifrim D, et al. Surgical management of gastroesophageal reflux disease: consensus statement of the International Society for Diseases of the Esophagus. Dis Esophagus. 2018; 31(1): 1–16.
|
| [28] |
Strate U, Emmermann A, Fibbe C, Layer P, Zornig C. Laparoscopic fundoplication: Nissen versus Toupet two-year outcome of a prospective randomized study of 200 patients regarding preoperative esophageal motility. Surg Endosc. 2008; 22(1): 21–30.
|
| [29] |
Toupet A. Surgical technique for the treatment of gastroesophageal reflux. Mem Acad Chir (Paris). 1961; 87: 164–7.
|
| [30] |
Vakil N, van Zanten SV, Kahrilas P, Dent J, Jones R. The Montreal definition and classification of gastroesophageal reflux disease: a global evidence-based consensus. Am J Gastroenterol. 2006; 101(8): 1900–20.
|
| [31] |
Van Beek DB, Auyang ED, Soper NJ. A comprehensive review of laparoscopic redo fundoplication. Surg Endosc. 2011; 25(3): 706–12.
|
| [32] |
Zhang M, Hou ZK, Huang ZB, Chen XL, Liu FB. Dietary and lifestyle factors related to gastroesophageal reflux disease: a systematic review. Ther Clin Risk Manag. 2021; 17: 305–23.
|
| [33] |
Zügel N, Lang H, Klinge U, Hellinger A, Hüttl TP. A comparison of laparoscopic Toupet versus Nissen fundoplication in gastroesophageal reflux disease. Langenbecks Arch Surg. 2002; 386(7): 494–8.
|
| [34] |
Wang B, Yin J, Cui L, et al. A Chinese randomized prospective trial of floppy Nissen and Toupet fundoplication for gastroesophageal disease. Int J Surg. 2015; 23: 35–40.
|
Cite This Article
-
APA Style
Lisboa, F. F., Dantas, G. D. C., Alves, A. F. L. D. A., Oliveira, L. V. D. S. (2026). Nissen Versus Toupet Fundoplication in GERD: Comparable Long-term Outcomes with Distinct Functional Profiles. Journal of Surgery, 14(3), 49-59. https://doi.org/10.11648/j.js.20261403.12
 Copy
|
Copy
|
 Download
Download
ACS Style
Lisboa, F. F.; Dantas, G. D. C.; Alves, A. F. L. D. A.; Oliveira, L. V. D. S. Nissen Versus Toupet Fundoplication in GERD: Comparable Long-term Outcomes with Distinct Functional Profiles. J. Surg. 2026, 14(3), 49-59. doi: 10.11648/j.js.20261403.12
Copy
|
Download
AMA Style
Lisboa FF, Dantas GDC, Alves AFLDA, Oliveira LVDS. Nissen Versus Toupet Fundoplication in GERD: Comparable Long-term Outcomes with Distinct Functional Profiles. J Surg. 2026;14(3):49-59. doi: 10.11648/j.js.20261403.12
Copy
|
Download
-
@article{10.11648/j.js.20261403.12,
author = {Fernando Freire Lisboa and Gabriel Diniz Camara Dantas and Angelo Felipe Lima de Araujo Alves and Luanny Vitoria da Silva Oliveira},
title = {Nissen Versus Toupet Fundoplication in GERD: Comparable Long-term Outcomes with Distinct Functional Profiles},
journal = {Journal of Surgery},
volume = {14},
number = {3},
pages = {49-59},
doi = {10.11648/j.js.20261403.12},
url = {https://doi.org/10.11648/j.js.20261403.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20261403.12},
abstract = {Background: Gastroesophageal reflux disease (GERD) is a prevalent condition with significant impact on quality of life. When medical therapy fails, surgical intervention—most commonly Nissen (NF) or Toupet fundoplication (TF)—is indicated. The optimal technique, however, remains debated. Aim: To compare the efficacy, functional outcomes, and complication profiles of Nissen and Toupet fundoplication in the surgical management of GERD. Methods: A systematic review was conducted in accordance with PRISMA guidelines. PubMed/MEDLINE, Cochrane, SciELO, and LILACS databases were searched for studies published between 2002 and 2025. Randomized controlled trials and cohort studies comparing NF and TF with at least 12 months of follow-up were included. Primary outcomes were postoperative dysphagia and reflux control. Secondary outcomes included proton pump inhibitor (PPI) use, quality of life (QoL), patient satisfaction, and reoperation rates. Results: Nine studies comprising 2,130 patients were included, including six randomized controlled trials. Both techniques provided effective and sustained reflux control. Nissen fundoplication demonstrated higher postoperative lower esophageal sphincter pressure and slightly better objective acid suppression in some studies; however, this did not translate into superior long-term clinical outcomes. Toupet fundoplication was associated with lower rates of early postoperative dysphagia and better preservation of esophageal motility. Long-term outcomes—including PPI use, QoL, and patient satisfaction—were comparable between techniques. Differences in dysphagia diminished over time. Conclusion: Nissen and Toupet fundoplication offer equivalent long-term control of GERD. While NF provides greater sphincter augmentation, TF achieves similar clinical outcomes with fewer early functional side effects. Surgical decision-making should prioritize esophageal motility and patient-specific characteristics rather than maximal acid suppression alone.},
year = {2026}
}
Copy
|
Download
-
TY - JOUR
T1 - Nissen Versus Toupet Fundoplication in GERD: Comparable Long-term Outcomes with Distinct Functional Profiles
AU - Fernando Freire Lisboa
AU - Gabriel Diniz Camara Dantas
AU - Angelo Felipe Lima de Araujo Alves
AU - Luanny Vitoria da Silva Oliveira
Y1 - 2026/05/19
PY - 2026
N1 - https://doi.org/10.11648/j.js.20261403.12
DO - 10.11648/j.js.20261403.12
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 49
EP - 59
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20261403.12
AB - Background: Gastroesophageal reflux disease (GERD) is a prevalent condition with significant impact on quality of life. When medical therapy fails, surgical intervention—most commonly Nissen (NF) or Toupet fundoplication (TF)—is indicated. The optimal technique, however, remains debated. Aim: To compare the efficacy, functional outcomes, and complication profiles of Nissen and Toupet fundoplication in the surgical management of GERD. Methods: A systematic review was conducted in accordance with PRISMA guidelines. PubMed/MEDLINE, Cochrane, SciELO, and LILACS databases were searched for studies published between 2002 and 2025. Randomized controlled trials and cohort studies comparing NF and TF with at least 12 months of follow-up were included. Primary outcomes were postoperative dysphagia and reflux control. Secondary outcomes included proton pump inhibitor (PPI) use, quality of life (QoL), patient satisfaction, and reoperation rates. Results: Nine studies comprising 2,130 patients were included, including six randomized controlled trials. Both techniques provided effective and sustained reflux control. Nissen fundoplication demonstrated higher postoperative lower esophageal sphincter pressure and slightly better objective acid suppression in some studies; however, this did not translate into superior long-term clinical outcomes. Toupet fundoplication was associated with lower rates of early postoperative dysphagia and better preservation of esophageal motility. Long-term outcomes—including PPI use, QoL, and patient satisfaction—were comparable between techniques. Differences in dysphagia diminished over time. Conclusion: Nissen and Toupet fundoplication offer equivalent long-term control of GERD. While NF provides greater sphincter augmentation, TF achieves similar clinical outcomes with fewer early functional side effects. Surgical decision-making should prioritize esophageal motility and patient-specific characteristics rather than maximal acid suppression alone.
VL - 14
IS - 3
ER -
Copy
|
Download