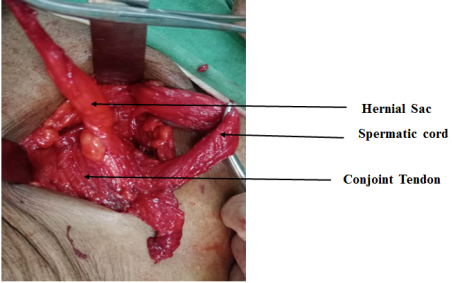
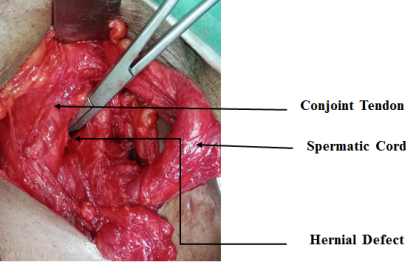
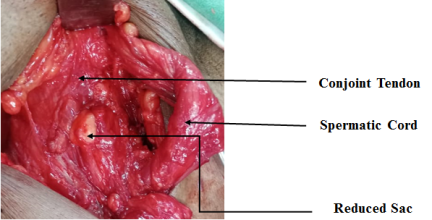
Inguinal hernia stands as a prevalent surgical concern, often addressed either through elective procedures or as emergencies by surgeons. The indirect hernia has high propensity to bowel obstruction due to narrow constrictive ring. Direct hernia is comparatively safe from complications owing to the larger defect. Busoga hernia (BH), alternatively referred to as Gill-Ogilvie hernia, represents a seldom-seen variation of direct inguinal hernia affecting the conjoint tendon. This hernia type arises due to a weakness in the conjoint tendon and tends to manifest more frequently among young athletes. Some authors described herniation in the weakened conjoint tendon secondary to rigorous training, kicking, running and sharp turn. Busoga hernia (BH) represents an uncommon subtype of direct inguinal hernia, characterized by a heightened risk of strangulation of its contents. This risk is attributed to an exceptionally narrow neck under constant tension within a resilient fascial sling. BH may migrate into labia majora in female and rarely migrate to the scrotum in male. We encountered a case involving a male patient aged 64 years who arrived with a small painful inflammation in his right groin. Surgical exploration under general anesthesia, revealed a 1cm defect in the medial aspect of the conjoint tendon. Subsequent procedures included herniotomy and herniorrhaphy, wherein the hernial contents consisted of pre-vesical fats and a portion of the urinary bladder. Surgeons must possess a thorough understanding of the anatomy of the inguinal region to effectively manage situations with confidence. The postoperative recovery period progressed satisfactorily with good outcomes. Patient is under regular follow up.
| Published in | Journal of Surgery (Volume 12, Issue 3) |
| DOI | 10.11648/j.js.20241203.11 |
| Page(s) | 71-74 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2024. Published by Science Publishing Group |
Busoga, Direct Inguinal Hernia, Gill-Ogilvie, Funicular, Herniotomy, Herniorrhaphy, Strangulation, Hesselbach’s Triangle
| [1] | King M, Bewes P, Cairns j, et al. Primary Surgery, Vol 1: Non-trauma. Oxford University Press; 1990. Page 199. |
| [2] | Wagner JP, Brunicardi FC, Amid PK, Chen DC. Inguinal hernias. In: Brunicardi FC, Dana K. Anderson DK, Billiar TR. Dunn DL, Hunter JG, et al, eds. Schwartz’s Principles of Surgey. 10th edition. Mc Graw Hill Inc; 2015: 1495. |
| [3] | Gill WG. Direct inguinal hernia. BMJ 1939: 263-4. |
| [4] | Paajanen H, Hermunen H, Ristolainen L, Branci S. Long-standing groin pain in contact sports: A Prospective case-control and MRI study. BMJ Open Sport Exerc Med. 2019; 5(1): e000507. [PMC free article] [Pub Med]. |
| [5] | Cole GJ. Strangulated hernia in Ibadan. A survey of 165 patients. Trans R Soc Trop Med Hyg 1964; 58: 441-7. |
| [6] | Hancock BD. Busoga hernia prevalence in abdominal emergencies in Busoga. Uganda. Trop Geogr Med 1974; 26: 15-25. |
| [7] | Claxton RC. “Busoga hernia”. J. R. Coll Surg Edin 1973; 18: 115-9. |
| [8] | Fellows GJ. Observations on strangulated direct inguinal hernia at Kampala and Jinja. EastAfr Med J 1968; 45: 516-22. |
| [9] | Read T, Maguire E. Busoga hernia: a hernia of the conjoint tendon. ANZ J Surg. 2013 Apr; 83(4): 296. [Pub Med]. |
| [10] | Piozzi GN, Cirelli R, Salati I, Maino MEM, Leopaldi E, Lenna G, Combi F, Sansonetti GM. Laparoscopic Approach to Inguinal Disruption in Athletes: a Retrospective 13-year Analysis of 198 Patients in a single surgeon Setting. Sports Med Open. 2019 Jun24; 5(1): 25. [PMC] [Pub Med]. |
| [11] | Ogilvie H, ed. Maingot R. Post-Graduate Surgery. Vol. 3. London: Medical Publications; 1937. P.3.620. |
| [12] | Zivanovic S. The anatomical basis for the high frequency of inguinal and femoral hernia in Uganda. East Afr Med J 1968; 45: 41-6. |
| [13] | Crag C. A note on Ogilvie’s tubular direct hernia. Med J Augt. 1946; 2(20): 705. |
| [14] | Jain R, Venkatesh K. Management of various rare and atypical hernias: experience at a tertiary care Centre in central India. Int Surg J. 2016: 3; 146-52. |
| [15] | Ogilvie H, Hattingh PW. An unusual type of hernia. Lancet. 1953; 261(6767): 950-1. |
| [16] | Codognotto E, Kiss A, MeoG, OliveroG, TalienteP. Rare abdominal wall hernias in South Sudan. South Sudan Med J. 2013; 6(2): 28-30. |
APA Style
Kumar, R. R. (2024). A Busoga Hernia: A Rare Case Report in India. Journal of Surgery, 12(3), 71-74. https://doi.org/10.11648/j.js.20241203.11
ACS Style
Kumar, R. R. A Busoga Hernia: A Rare Case Report in India. J. Surg. 2024, 12(3), 71-74. doi: 10.11648/j.js.20241203.11
AMA Style
Kumar RR. A Busoga Hernia: A Rare Case Report in India. J Surg. 2024;12(3):71-74. doi: 10.11648/j.js.20241203.11
@article{10.11648/j.js.20241203.11,
author = {Raj Ranjan Kumar},
title = {A Busoga Hernia: A Rare Case Report in India
},
journal = {Journal of Surgery},
volume = {12},
number = {3},
pages = {71-74},
doi = {10.11648/j.js.20241203.11},
url = {https://doi.org/10.11648/j.js.20241203.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20241203.11},
abstract = {Inguinal hernia stands as a prevalent surgical concern, often addressed either through elective procedures or as emergencies by surgeons. The indirect hernia has high propensity to bowel obstruction due to narrow constrictive ring. Direct hernia is comparatively safe from complications owing to the larger defect. Busoga hernia (BH), alternatively referred to as Gill-Ogilvie hernia, represents a seldom-seen variation of direct inguinal hernia affecting the conjoint tendon. This hernia type arises due to a weakness in the conjoint tendon and tends to manifest more frequently among young athletes. Some authors described herniation in the weakened conjoint tendon secondary to rigorous training, kicking, running and sharp turn. Busoga hernia (BH) represents an uncommon subtype of direct inguinal hernia, characterized by a heightened risk of strangulation of its contents. This risk is attributed to an exceptionally narrow neck under constant tension within a resilient fascial sling. BH may migrate into labia majora in female and rarely migrate to the scrotum in male. We encountered a case involving a male patient aged 64 years who arrived with a small painful inflammation in his right groin. Surgical exploration under general anesthesia, revealed a 1cm defect in the medial aspect of the conjoint tendon. Subsequent procedures included herniotomy and herniorrhaphy, wherein the hernial contents consisted of pre-vesical fats and a portion of the urinary bladder. Surgeons must possess a thorough understanding of the anatomy of the inguinal region to effectively manage situations with confidence. The postoperative recovery period progressed satisfactorily with good outcomes. Patient is under regular follow up.
},
year = {2024}
}
TY - JOUR T1 - A Busoga Hernia: A Rare Case Report in India AU - Raj Ranjan Kumar Y1 - 2024/05/24 PY - 2024 N1 - https://doi.org/10.11648/j.js.20241203.11 DO - 10.11648/j.js.20241203.11 T2 - Journal of Surgery JF - Journal of Surgery JO - Journal of Surgery SP - 71 EP - 74 PB - Science Publishing Group SN - 2330-0930 UR - https://doi.org/10.11648/j.js.20241203.11 AB - Inguinal hernia stands as a prevalent surgical concern, often addressed either through elective procedures or as emergencies by surgeons. The indirect hernia has high propensity to bowel obstruction due to narrow constrictive ring. Direct hernia is comparatively safe from complications owing to the larger defect. Busoga hernia (BH), alternatively referred to as Gill-Ogilvie hernia, represents a seldom-seen variation of direct inguinal hernia affecting the conjoint tendon. This hernia type arises due to a weakness in the conjoint tendon and tends to manifest more frequently among young athletes. Some authors described herniation in the weakened conjoint tendon secondary to rigorous training, kicking, running and sharp turn. Busoga hernia (BH) represents an uncommon subtype of direct inguinal hernia, characterized by a heightened risk of strangulation of its contents. This risk is attributed to an exceptionally narrow neck under constant tension within a resilient fascial sling. BH may migrate into labia majora in female and rarely migrate to the scrotum in male. We encountered a case involving a male patient aged 64 years who arrived with a small painful inflammation in his right groin. Surgical exploration under general anesthesia, revealed a 1cm defect in the medial aspect of the conjoint tendon. Subsequent procedures included herniotomy and herniorrhaphy, wherein the hernial contents consisted of pre-vesical fats and a portion of the urinary bladder. Surgeons must possess a thorough understanding of the anatomy of the inguinal region to effectively manage situations with confidence. The postoperative recovery period progressed satisfactorily with good outcomes. Patient is under regular follow up. VL - 12 IS - 3 ER -
Surgery Department, Durgapur Steel Plant Hospital & Research Centre, Durgapur, India
Information