Abstract
Sternal fixation with steel wires or cerclages, is the gold standard for closing a midline sternotomy, the standard incision in cardiac surgery. Rare wound complications can occur following a sternotomy wire closure. The objective of this study is to establish that the clinical efficacy of the Steelex Sternum Set is equivalent to the results documented in existing literature. The cohorts of the previously conducted OPTICABG and PREMIVALVE studies served as a foundation for the design of this retrospective, bicentric, international, single-arm study. The purpose of the study was to evaluate the clinical performance of the Steelex Sternum Set for sternal closure after coronary artery bypass grafting or cardiac valve replacement/reconstruction surgery. The primary endpoint was the incidence of a composite consisting of sternum instability, sternum dehiscence, superficial and deep sternal wound infection up to six months after surgery. A quantitative summary of the available clinical literature has been conducted for comparison purposes. There were 229 patients in total (89 PREMIVALVE and 140 OPTICABG). The combined rate of surgical site infection and sternal dehiscence/instability was 3.49%, compared to 1.5 - 20% described in the literature. Severe complications such as mortality, stroke, myocardial infarction, and mediastinitis occurred in about 0.8 - 2% of cases. The Steelex Sternum Set is a safe and appropriate method for sternal closure in a diverse patient population undergoing cardiac valve replacement and/or reconstruction, as well as coronary artery bypass graft surgery, in routine clinical settings.
Keywords
Surgical Site Infection (SSI), Sternal Dehiscence, Sternal Instability, Sternal Wires, Cerclages
1. Introduction
In cardiac surgery, the midline sternotomy is the most common surgical approach
| [1] | Reser D, Caliskan E, Tolboom H, Guidotti A, Maisano F. Median sternotomy. Multimed Man Cardiothorac Surg. 2015 Jul 17; 2015: mmv017. https://doi.org/10.1093/mmcts/mmv017 |
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [4] | Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, Ch'ng S, Gangahanumaiah S, Bailey M. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018 Oct; 156(4): 1589-1595. e1. https://doi.org/10.1016/j.jtcvs.2018.04.025 |
| [5] | Hashim S, Chin LY, Krishnasamy S, Sthaneswar P, Raja Mokhtar RA. Effect of sternal closure with biological bone adhesive on pain visual analogue score and serum cytokine. J Cardiothorac Surg. 2015 Mar 17; 10: 32. https://doi.org/10.1186/s13019-015-0230-0 |
| [6] | Wang B, He D, Wang M, Qian Y, Lu Y, Shi X, Liu Y, Zhan X, Di D, Zhu K, Zhang X. Analysis of sternal healing after median sternotomy in low risk patients at midterm follow-up: retrospective cohort study from two centres. J Cardiothorac Surg. 2019 Nov 11; 14(1): 193. https://doi.org/10.1186/s13019-019-1000-1 |
[1-6]
. Sternal fixation with steel wires or cerclages is the standard procedure for closing a midline sternotomy in about 90% of instances
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [4] | Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, Ch'ng S, Gangahanumaiah S, Bailey M. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018 Oct; 156(4): 1589-1595. e1. https://doi.org/10.1016/j.jtcvs.2018.04.025 |
[2-4]
. Other methods, such as bands, plates, and method combinations, play a minor role
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [4] | Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, Ch'ng S, Gangahanumaiah S, Bailey M. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018 Oct; 156(4): 1589-1595. e1. https://doi.org/10.1016/j.jtcvs.2018.04.025 |
| [6] | Wang B, He D, Wang M, Qian Y, Lu Y, Shi X, Liu Y, Zhan X, Di D, Zhu K, Zhang X. Analysis of sternal healing after median sternotomy in low risk patients at midterm follow-up: retrospective cohort study from two centres. J Cardiothorac Surg. 2019 Nov 11; 14(1): 193. https://doi.org/10.1186/s13019-019-1000-1 |
| [7] | Allen KB, Icke KJ, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M. Sternotomy closure using rigid plate fixation: a paradigm shift from wire cerclage. Ann Cardiothorac Surg. 2018 Sep; 7(5): 611-620. https://doi.org/10.21037/acs.2018.06.01 |
| [8] | Dunne B, Murphy M, Skiba R, Wang X, Ho K, Larbalestier R, Merry C. Sternal cables are not superior to traditional sternal wiring for preventing deep sternal wound infection. Interact Cardiovasc Thorac Surg. 2016 May; 22(5): 594-8. https://doi.org/10.1093/icvts/ivw017 |
[2-4, 6-8]
. Recent advancements in sternal closure include the use of kryptonite bone cement, a biocompatible polymer that can adhere bone margins
| [5] | Hashim S, Chin LY, Krishnasamy S, Sthaneswar P, Raja Mokhtar RA. Effect of sternal closure with biological bone adhesive on pain visual analogue score and serum cytokine. J Cardiothorac Surg. 2015 Mar 17; 10: 32. https://doi.org/10.1186/s13019-015-0230-0 |
[5]
.
Wound complications following the closure of a sternotomy with wires are fairly rare, but they can be catastrophic for the patient and necessitate an extended and expensive treatment plan. As a result of sternal instability, complications range from prolonged incisional pain to dehiscence and deep sternal wound infections
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [9] | Cataneo DC, Dos Reis TA, Felisberto G, Rodrigues OR, Cataneo AJM. New sternal closure methods versus the standard closure method: systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. 2019 Mar 1; 28(3): 432-440. https://doi.org/10.1093/icvts/ivy281 |
[2, 3, 9]
. A severe complication of cardiac surgery is mediastinitis, an infection of the sternum and mediastinum that is associated with a high mortality rate of 14% to 47% and high treatment costs
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [4] | Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, Ch'ng S, Gangahanumaiah S, Bailey M. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018 Oct; 156(4): 1589-1595. e1. https://doi.org/10.1016/j.jtcvs.2018.04.025 |
| [6] | Wang B, He D, Wang M, Qian Y, Lu Y, Shi X, Liu Y, Zhan X, Di D, Zhu K, Zhang X. Analysis of sternal healing after median sternotomy in low risk patients at midterm follow-up: retrospective cohort study from two centres. J Cardiothorac Surg. 2019 Nov 11; 14(1): 193. https://doi.org/10.1186/s13019-019-1000-1 |
[2, 4, 6]
. Estimates place the direct cost of a sternal wound infection between 14,000 and 40,000 US dollars
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [7] | Allen KB, Icke KJ, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M. Sternotomy closure using rigid plate fixation: a paradigm shift from wire cerclage. Ann Cardiothorac Surg. 2018 Sep; 7(5): 611-620. https://doi.org/10.21037/acs.2018.06.01 |
| [10] | Lazar HL, Salm TV, Engelman R, Orgill D, Gordon S. Prevention and management of sternal wound infections. J Thorac Cardiovasc Surg. 2016 Oct; 152(4): 962-72. https://doi.org/10.1016/j.jtcvs.2016.01.060 |
[3, 7, 10]
. Misalignment of the sternal halves is a typical flaw of sternal fixation. In the early postoperative phase, only the holding power of the wire cerclage must withstand counterforces from the action of the respiratory muscles and the negative intrathoracic pressure associated with normal respiration. The sternal union is more stable the tighter the wire; however, the greater the likelihood that the wires will actually penetrate the bone. If the bone is severed, the wire sutures will loosen and the two halves of the sternum will separate. It has been demonstrated that the forces required to dislodge the cerclage are physiologically acceptable (400 N)
. Various biomechanical studies have demonstrated that breathing and sneezing can exacerbate this process.
Complications from the sternotomy are recorded in between 0.7% and 11% of cardiac surgery patients
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [7] | Allen KB, Icke KJ, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M. Sternotomy closure using rigid plate fixation: a paradigm shift from wire cerclage. Ann Cardiothorac Surg. 2018 Sep; 7(5): 611-620. https://doi.org/10.21037/acs.2018.06.01 |
[2, 3, 7]
. While 0.5%-4% of patients experience sternal instability, reports of superficial sternal wound infection range from 0.2-10%
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
[2, 3]
. Infection rates for deep sternal wounds ranged from 0.8% to 4% in large surveillance studies, with a median incubation period of 10 days
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [6] | Wang B, He D, Wang M, Qian Y, Lu Y, Shi X, Liu Y, Zhan X, Di D, Zhu K, Zhang X. Analysis of sternal healing after median sternotomy in low risk patients at midterm follow-up: retrospective cohort study from two centres. J Cardiothorac Surg. 2019 Nov 11; 14(1): 193. https://doi.org/10.1186/s13019-019-1000-1 |
| [8] | Dunne B, Murphy M, Skiba R, Wang X, Ho K, Larbalestier R, Merry C. Sternal cables are not superior to traditional sternal wiring for preventing deep sternal wound infection. Interact Cardiovasc Thorac Surg. 2016 May; 22(5): 594-8. https://doi.org/10.1093/icvts/ivw017 |
| [13] | Schimmer C, Reents W, Berneder S, Eigel P, Sezer O, Scheld H, Sahraoui K, Gansera B, Deppert O, Rubio A, Feyrer R, Sauer C, Elert O, Leyh R. Prevention of sternal dehiscence and infection in high-risk patients: a prospective randomized multicenter trial. Ann Thorac Surg. 2008 Dec; 86(6): 1897-904. https://doi.org/10.1016/j.athoracsur.2008.08.071 |
[2, 3, 6, 8, 13]
. Older patient age, diabetes, obesity, smoking, steroid medication, and chronic obstructive pulmonary disease (COPD) all contribute to a higher risk of developing this condition
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [4] | Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, Ch'ng S, Gangahanumaiah S, Bailey M. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018 Oct; 156(4): 1589-1595. e1. https://doi.org/10.1016/j.jtcvs.2018.04.025 |
| [13] | Schimmer C, Reents W, Berneder S, Eigel P, Sezer O, Scheld H, Sahraoui K, Gansera B, Deppert O, Rubio A, Feyrer R, Sauer C, Elert O, Leyh R. Prevention of sternal dehiscence and infection in high-risk patients: a prospective randomized multicenter trial. Ann Thorac Surg. 2008 Dec; 86(6): 1897-904. https://doi.org/10.1016/j.athoracsur.2008.08.071 |
| [14] | Balachandran S, Lee A, Denehy L, Lin KY, Royse A, Royse C, El-Ansary D. Risk Factors for Sternal Complications After Cardiac Operations: A Systematic Review. Ann Thorac Surg. 2016 Dec; 102(6): 2109-2117. https://doi.org/10.1016/j.athoracsur.2016.05.047 |
[2, 4, 13, 14]
.
Steelex® Sternum Set is a sterile, non-adsorbable stainless steel surgical material that is offered as twisted multifilament or monofilament for sternal closure. The set is available in two sizes, and sterilisation is accomplished using either ethylene oxide or gamma-irradiation. The current study is a retrospective, international, bicentric, observational, single arm, cohort study designed to compare Steelex Sternum Sets’ safety and performance in cardiac surgery with that of existing literature. To achieve this goal, eligible patients from both the OPTICABG and PREMIVALVE studies were included into the STERCCAS study. The applied stainless steel wire monofilament is CE-marked and was utilized for its intended purpose in both the OPTICABG
| [15] | Ursulescu A, Baumann P, Ferrer MT, Contino M, Romagnoni C, Antona C, Padró Fernández JM. Optilene, a new non-absorbable monofilament is safe and effective for CABG anastomosis. OPTICABG - A prospective international, multi-centric, cohort study. Ann Med Surg (Lond). 2018 Sep 15; 35: 13-19. https://doi.org/10.1016/j.amsu.2018.09.005 |
[15]
and PREMIVALVE studies
| [16] | Rufa M, Ursulescu A, Baumann P, Ferrer MT. A prospective, international, bicentric study to evaluate PremiCron suture material for cardiac valve surgery - PREMIVALVE a cohort study. Ann Med Surg (Lond). 2023 Apr 4; 85(4): 835-841. https://doi.org/10.1097/MS9.0000000000000442 |
[16]
. All patients included in the analysis were administered the stainless steel wire monofilament, irrespective of this retrospective investigation, as it was the standard suture used for sternal closure at both participating sites.
2. Materials and Methods
The current STERCCAS study adheres to the STROCSS Guideline, a recognized norm for the publication of cohort studies
| [17] | Mathew G, Agha R, Albrecht J, Goel P, Mukherjee I, Pai P, D'Cruz AK, Nixon IJ, Roberto K, Enam SA, Basu S, Muensterer OJ, Giordano S, Pagano D, Machado-Aranda D, Bradley PJ, Bashashati M, Thoma A, Afifi RY, Johnston M, Challacombe B, Ngu JC, Chalkoo M, Raveendran K, Hoffman JR, Kirshtein B, Lau WY, Thorat MA, Miguel D, Beamish AJ, Roy G, Healy D, Ather HM, Raja SG, Mei Z, Manning TG, Kasivisvanathan V, Rivas JG, Coppola R, Ekser B, Karanth VL, Kadioglu H, Valmasoni M, Noureldin A; STROCSS Group. STROCSS 2021: Strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int J Surg. 2021 Dec; 96: 106165. https://doi.org/10.1016/j.ijsu.2021.106165 |
[17]
.
2.1. Registration, Ethics Consideration and Informed Consent
Consistent with the principles outlined in the Declaration of Helsinki, the present retrospective cohort research was duly registered on the website www.clinicaltrials.gov.prior to analysis implementation. (NCT05439395, Hyperlink to registration: Study Record | ClinicalTrials.gov).
Both the OPTICABG study and the PREMIVALVE study received approval from the ethical committees overseeing the clinics involved. These same committees were also consulted for approval of the present retrospective study, STERCCAS. Ethics approval was needed to meet national requirements. The following Institutional Review Boards were able to get ethics approval: Ethics Committee, University of Tübingen, Germany, Project No. 171/ 2022BO2, and the Comité Ético de Investigación Clinica, Hospital de la Santa Creu i Sant Pau, Barcelona, Spain, Project No.22/101 (R-PS). A clinical study protocol was drawn up a priori, but a publication in a peer-reviewed scientific journal was not made.
All the enrolled patients in the OPTICABG and PREMIVALVE study gave their written informed consent before their inclusion in the study.
The research was conducted as a retrospective, multinational, bicentric cohort study with the purpose of assessing the effectiveness of the Steelex Sternum Set, stainless steel wire monofilament manufactured by B. Braun Surgical SA, Rubi, Spain, in sternum closure. The assessment utilized data obtained from two clinics situated in Germany and Spain, both of which were actively involved in the OPTICABG and PREMIVALVE studies. The analysis included only patients who underwent either a complete or a partial sternotomy closure using the stainless steel wire monofilament. The patients in the OPTICABG study were monitored for a period of up to 3 months post-surgery, whereas the patients in the PREMIVALVE study were followed up for a duration of 6 months post-surgery. The OPTICABG and PREMIVALVE studies have already documented the safety and efficacy measures that are routinely employed in cardiac surgery. The acquired data were subjected to comparison with the existing literature. The adverse events seen in the OPTICABG and PREMIVALVE studies, including sternum instability, sternum dehiscence, and superficial and deep sternal wound infection, were analysed to assess the effectiveness of the stainless steel wire monofilament in achieving sternal closure. These complications were considered as serious adverse events in the study. If the outcomes of our study were comparable or superior to the findings reported in published literature, it can be concluded that the applied stainless steel surgical suture material is both safe and efficacious.
Patients in the OPTICABG and PREMIVALVE studies were included if they were at least 18 years old, they gave informed consent, and their sternums had been closed using the stainless steel wire monofilament, Steelex Sternum Set after undergoing either a full or partial sternotomy for elective primary coronary artery bypass grafting or heart valve replacement/reconstruction, respectively.
2.4. Outcomes (Primary and Secondary)
The rate of sternal dehiscence/sternal instability, as well as superficial and deep sternal wound infections up to 6 months following surgery, was used as the primary endpoint in determining the non-inferiority of the deployed stainless steel wire monofilament.
Surgical Site Infection (SSI) is a term that is defined in accordance with the criteria established by the US Centres for Disease Control and Prevention (CDC). A SSI can be superficial (SSI A1) or deep (SSI A2).
Secondary variables:
1) Incidence of sternal dehiscence
2) Incidence of sternal instability
3) Incidence of superficial sternal site infection
4) Incidence of deep sternal site infection
5) Incidence of other cardiac and cerebral complications such as stroke, myocardial infarction, death, mediastinitis
6) Incidence of suture related complications (e.g. wire breakage)
7) Length of hospital stay
8) Length of intensive care unit stay
9) Quality of life up to 6 months after surgery using the EQ5D5L questionnaire
2.5. Statistical Methods and Analysis
No sample size calculation was performed due to the retrospective design of the study. All patients enrolled in the OPTICABG (N= 150) and PREMIVALVE (N=198) study were checked for eligibility and therefore, the maximal sample size for the STERCCAS analysis amounts to 348 patients.
2.5.2. Stastical Hypothesis
In this study, the Steelex Sternum Set was evaluated using a primary analysis, wherein its performance was compared to the findings described in existing literature. The focus of this comparison was on a composite endpoint that encompassed the principal problems observed after sternal closure, namely sternal dehiscence/instability, superficial sternal wound infection, and deep sternal wound infection. The results of the Steelex Sternum Set were analysed using a cumulative rate approach, along with a 95% confidence interval. This approach takes into account the occurrence of any adverse event within the defined category, over the whole study group.
The frequencies of the primary problems following sternal closure, as documented in the existing literature, are as follows and were utilized for comparative analysis:
1) incidence of sternal dehiscence or instability: 0.5% - 4%
2) incidence of superficial sternal wound infection, SSI A1: 0.2% - 10%
3) incidence of deep sternal wound infection, SSI A2: 0.8% - 6%.
4) Hence, it was anticipated that the cumulative rate for the combined endpoint would fall within the range of 1.5% and 20%.
2.5.3. Statistical Analysis Methods
Tables, figures, listings, and statistical tests assessed all data. The database was closed and the final programming was done using SAS. For summary results (mean, standard deviation), the number of data was listed. The study centre ID and patient ID assigned during data entry identified the patient data. The statistical analysis followed these guidelines: Variables with metric or ordinal scale were summarized as follows: • N observations, • Min, Max, • Median, • Mean. • Standard deviation (StD). Optional: missing data (Nmiss), upper and lower quartiles (Q3 and Q1), 95% confidence interval of the median, and pre-specified test p values.
To summarize categorical variables, we used: • Number of observations (N) • Relative frequencies (p, %). A "N/A" category identified missing values. Missing data were evaluated without estimations.
Standard comparison methodologies used: • Chi-Square test for binary data, • U-test using Wilcoxon-Mann-Whitney or Kruskal-Wallis for non-parametric data, • t test or One-Way-ANOVA for metric data assuming a normal distribution.
Statistics (box plots, bar charts) were used when applicable. The sponsor organized study data statistical analysis. A final biometric report was created. Statistical tests were two-tailed or one-tailed with alpha = 5% or 2.5%, respectively. Thus, two-sided 95% confidence intervals were used. The primary variable test was confirming, all other tests explained. The explanatory test p-values may indicate a difference in the sample rather than the population.
3. Results
3.1. Recruitment, Patient Population, Baseline Characteristics and Intraoperative Details
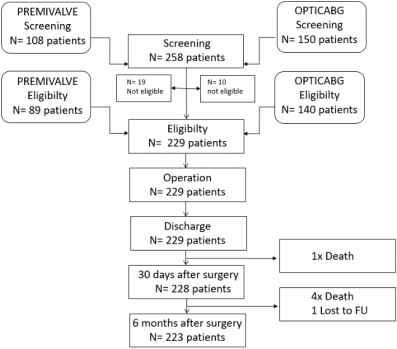
More than 250 patients were assessed, and 229 were ultimately enrolled. Eligible patients included 89 PREMIVALVE patients who received a Steelex Sternum Set following cardiac valve replacement and/or reconstruction and 140 OPTICABG patients who underwent coronary artery bypass graft surgery. The research population included 157 German patients and 72 Spanish patients. Recruitment of OPTICABG patients took place between 30th November 2015 and 8th May 2017. PREMIVALVE patients were enrolled from 29th January 2020 until 31st January 2022.
The discharge visit for 229 patients was reported. One patient died between the day of discharge and 30 days of follow-up. Until six months after surgery, an additional four fatalities and one patient lost to follow-up were reported. That is, 223 patients were evaluated six months after surgery (
Figure 1).
Figure 1. Flow-chart of the study.
Gender distribution was comparable in both study subgroups (OPTICABG: 76% males versus 24% females, and PREMIVALVE: 66% males versus 34% females). Patients averaged 67.27 ± 8.79 years of age (range: 41–84 years), and there was no significant difference in age between the OPTCABG and PREMIVALVE populations.
The mean BMI was 28.62 ± 4.49 kg/m
2, with a range of 19.70 to 48.34 kg/m
2. Obese patients were observed in both gender categories, but females tended to have a higher BMI.
Table 1 provides a comprehensive presentation of comorbidities and health status.
The thorax was accessed through either a complete sternotomy (67% of cases) or a partial sternotomy, namely in the third or fourth intercostal space. Sternal fixation was performed in the German clinic using Steelex Sternum Set (4x45 cm, USP 6, HRS 48, Tapercut 48mm, 1/2c), whereas the Spanish clinic preferred to apply Steelex Sternum Set in the following configuration (4x45cm, USP 5, HRS48, AXIA LPCE).
Over a period of 6 months, a total of five SSIs classified as A1, two SSIs classified as A2, and one case of sternal instability were seen. This resulted in a combined event rate of 3.49%, with a 95% confidence interval ranging from 1.67% to 6.85%. The observed rate was compared to existing literature data, which reported a cumulative rate of SSI and sternal dehiscence/instability ranging from 1.5% to 20%. The safety outcomes from the STERCCAS study revealed that the incidence of SSI and sternal dehiscence/instability associated with the used stainless steel wire monofilament was found to be within the lower range of the data reported in existing literature. These findings suggest that the Steelex Sternum Set is a reliable and efficacious method for closing the sternum.
The individual rates for superficial (A1) and deep (A2) SSIs and sternal dehiscence were as follows:
1) SSI (A1) superficial: N= 5/229; 2.18% CI 95% [0.79% - 5.15%]
2) SSI (A2), deep: N= 2/229; 0.87% CI 95% [0.03% - 3.34%]
3) Sternal instability: N= 1/229; 0.44% CI 95% [0.00% - 2.68%]
The above observed individual rates were in agreement with the reported literature rates.
1) Sternal SSI (A1): 0.2% - 10%
2) Sternal SSI (A2): 0.8 – 6%
3) Sternal instability/dehiscence: 0.5% - 4%
Furthermore, it could be shown that the individual event rates were at the lower level / range, when Steelex Sternum Set was used to close the sternum.
A total of five deaths (2.1%) were reported within a six-month period following the surgical procedure. A total of three fatalities were seen in the PREMIVALVE subgroup, whereas the OPTICABG subgroup saw two deaths. The primary cause of mortality in this study was identified as multi-organ failure, which occurred in two instances. Additionally, one patient experienced cardiogenic shock, another patient's reanimation attempts were unsuccessful, and one patient passed away following a stroke. There were no reports of either a myocardial infarction or a mediastinitis. A total of two strokes, accounting for 0.8% of the cases, were observed. A single instance of a significant adverse event associated with a medical device was documented, representing a prevalence rate of 0.43%. In a single patient from the OPTICABG subgroup, it was seen that five out of seven sternum wires had fractured within 8 days following the surgical procedure, necessitating a subsequent surgical intervention.
Table 1. Demography and baseline data.
Parameter | STERCCAS | OPTICABG | PREMIVALVE |
| N | PctN (%) | N | PctN (%) | N | PctN (%) |
Total | 229 | 100.00 | 140 | 100.00 | 89 | 100,00 |
Gender | | | | | | |
Female | 63 | 27.51 | 33 | 23.57 | 30 | 33.71 |
Male | 166 | 72.49 | 107 | 76.43 | 59 | 66.29 |
General Health Status | | | | | | |
ASA1 | 2 | 0.87 | 2 | 1.43 | | |
ASA2 | 59 | 25.76 | 20 | 14.29 | 39 | 43.82 |
ASA3 | 164 | 71.62 | 116 | 82.86 | 48 | 53.93 |
ASA4 | 4 | 1.75 | 2 | 1.43 | 2 | 2.25 |
NHYA Classification | | | | | | |
NYHA I | 20 | 8.73 | 18 | 12.86 | 2 | 2.25 |
NYHA II | 135 | 58.95 | 75 | 53.57 | 60 | 67.42 |
NYHA III | 73 | 31.88 | 47 | 33.57 | 26 | 29.21 |
NYHA IV | 1 | 0.44 | | | 1 | 1.12 |
Smoking | | | | | | |
No | 117 | 51.09 | 62 | 44.29 | 55 | 61.80 |
No, previous | 73 | 31.88 | 50 | 35 | 23 | 25.84 |
Yes, current | 38 | 16.59 | 28 | 71 | 10 | 11.24 |
N/A | 1 | 0.44 | | 20.00 | 1 | 1.12 |
LEVF | | | | | | |
< 21% | 2 | 0.87 | 1 | 0.71 | 1 | 1.12 |
21% - 31% | 9 | 3.93 | 9 | 6.43 | | |
31%-50% | 26 | 11.35 | 16 | 11.43 | 10 | 11.24 |
>50% | 191 | 83.41 | 114 | 81.43 | 77 | 86.52 |
N/A | 1 | | | | 1 | 1.12 |
Heart rhythm | | | | | | |
Sinus rhythm | 216 | 94.32 | 134 | 95.71 | 82 | 92.13 |
Atrial fibrillation | 13 | 5.68 | 6 | 4.29 | 7 | 7.87 |
4. Discussion
The STERCCAS study, a single-arm, retrospective, observational study conducted in Germany and Spain, enrolled patients treated using Steelex Sternum Set to close the sternum after cardiac valve replacement and/or reconstruction or coronary artery bypass graft surgery. The use of the stainless steel wire monofilament resulted in a low rate of postoperative complications and a high patient quality of life.
The midline sternotomy is widely employed as the primary surgical method in cardiac surgery, as supported by multiple studies
| [1] | Reser D, Caliskan E, Tolboom H, Guidotti A, Maisano F. Median sternotomy. Multimed Man Cardiothorac Surg. 2015 Jul 17; 2015: mmv017. https://doi.org/10.1093/mmcts/mmv017 |
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [4] | Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, Ch'ng S, Gangahanumaiah S, Bailey M. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018 Oct; 156(4): 1589-1595. e1. https://doi.org/10.1016/j.jtcvs.2018.04.025 |
| [5] | Hashim S, Chin LY, Krishnasamy S, Sthaneswar P, Raja Mokhtar RA. Effect of sternal closure with biological bone adhesive on pain visual analogue score and serum cytokine. J Cardiothorac Surg. 2015 Mar 17; 10: 32. https://doi.org/10.1186/s13019-015-0230-0 |
| [6] | Wang B, He D, Wang M, Qian Y, Lu Y, Shi X, Liu Y, Zhan X, Di D, Zhu K, Zhang X. Analysis of sternal healing after median sternotomy in low risk patients at midterm follow-up: retrospective cohort study from two centres. J Cardiothorac Surg. 2019 Nov 11; 14(1): 193. https://doi.org/10.1186/s13019-019-1000-1 |
[1-6]
. This medical procedure is utilized in the context of open-heart surgery, cardiac valve replacement, and coronary artery bypass surgery. The midline access procedure is characterized by its efficiency and simplicity, since it may be executed rapidly and with minimal blood loss and functional impairment. Consistent with the existing literature, our retrospective investigation found that a majority of the patients involved in the PREMIVALVE study (focused on cardiac valve replacement/reconstruction)
| [16] | Rufa M, Ursulescu A, Baumann P, Ferrer MT. A prospective, international, bicentric study to evaluate PremiCron suture material for cardiac valve surgery - PREMIVALVE a cohort study. Ann Med Surg (Lond). 2023 Apr 4; 85(4): 835-841. https://doi.org/10.1097/MS9.0000000000000442 |
[16]
and the OPTICABG study (focused on coronary artery bypass grafting)
| [15] | Ursulescu A, Baumann P, Ferrer MT, Contino M, Romagnoni C, Antona C, Padró Fernández JM. Optilene, a new non-absorbable monofilament is safe and effective for CABG anastomosis. OPTICABG - A prospective international, multi-centric, cohort study. Ann Med Surg (Lond). 2018 Sep 15; 35: 13-19. https://doi.org/10.1016/j.amsu.2018.09.005 |
[15]
underwent a median sternotomy procedure. A combined total of 229 patients were included in the aforementioned trials, with 153 individuals undergoing a midline sternotomy procedure to access the chest cavity, constituting approximately 67% of the study population. A minimally invasive method was selected for the remaining patients. Approximately 90% of sternal closures include steel wires. Furthermore, in the present study, all patients who underwent surgery through a midline sternotomy or a partial upper-sternotomy had their incisions closed using steel wires (specifically, the Steelex Sternum Set).
The documented occurrence of problems associated to sternotomy in patients undergoing cardiac surgery varies between 0.7% and 11%
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [7] | Allen KB, Icke KJ, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M. Sternotomy closure using rigid plate fixation: a paradigm shift from wire cerclage. Ann Cardiothorac Surg. 2018 Sep; 7(5): 611-620. https://doi.org/10.21037/acs.2018.06.01 |
[2, 3, 7]
. The potential problems range from minor issues, such as prolonged sternal pain or an unstable sternum resulting from non-union of the sternal bone, to more severe complications, such as deep sternal wound infection or mediastinitis. Sternal instability has been observed in a range of 0.5% to 4% of patients following cardiac surgery, as reported in several studies
| [4] | Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, Ch'ng S, Gangahanumaiah S, Bailey M. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018 Oct; 156(4): 1589-1595. e1. https://doi.org/10.1016/j.jtcvs.2018.04.025 |
| [6] | Wang B, He D, Wang M, Qian Y, Lu Y, Shi X, Liu Y, Zhan X, Di D, Zhu K, Zhang X. Analysis of sternal healing after median sternotomy in low risk patients at midterm follow-up: retrospective cohort study from two centres. J Cardiothorac Surg. 2019 Nov 11; 14(1): 193. https://doi.org/10.1186/s13019-019-1000-1 |
| [13] | Schimmer C, Reents W, Berneder S, Eigel P, Sezer O, Scheld H, Sahraoui K, Gansera B, Deppert O, Rubio A, Feyrer R, Sauer C, Elert O, Leyh R. Prevention of sternal dehiscence and infection in high-risk patients: a prospective randomized multicenter trial. Ann Thorac Surg. 2008 Dec; 86(6): 1897-904. https://doi.org/10.1016/j.athoracsur.2008.08.071 |
| [14] | Balachandran S, Lee A, Denehy L, Lin KY, Royse A, Royse C, El-Ansary D. Risk Factors for Sternal Complications After Cardiac Operations: A Systematic Review. Ann Thorac Surg. 2016 Dec; 102(6): 2109-2117. https://doi.org/10.1016/j.athoracsur.2016.05.047 |
| [18] | Robicsek F, Fokin A, Cook J, Bhatia D. Sternal instability after midline sternotomy. Thorac Cardiovasc Surg. 2000 Feb; 48(1): 1-8. https://doi.org/10.1055/s-2000-9945 |
[4, 6, 13, 14, 18]
. The occurrence of significant bleeding poses a significant risk in the context of repeat sternotomy procedures. The prevalence of superficial sternal wound infection has been documented to range from 0.2% to 10% in several studies
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
[2, 3]
. Extensive surveillance efforts have yielded findings indicating that the prevalence of deep sternal wound infection ranges from 0.8% to 4%, with an average incubation period of 10 days
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
| [6] | Wang B, He D, Wang M, Qian Y, Lu Y, Shi X, Liu Y, Zhan X, Di D, Zhu K, Zhang X. Analysis of sternal healing after median sternotomy in low risk patients at midterm follow-up: retrospective cohort study from two centres. J Cardiothorac Surg. 2019 Nov 11; 14(1): 193. https://doi.org/10.1186/s13019-019-1000-1 |
| [8] | Dunne B, Murphy M, Skiba R, Wang X, Ho K, Larbalestier R, Merry C. Sternal cables are not superior to traditional sternal wiring for preventing deep sternal wound infection. Interact Cardiovasc Thorac Surg. 2016 May; 22(5): 594-8. https://doi.org/10.1093/icvts/ivw017 |
| [13] | Schimmer C, Reents W, Berneder S, Eigel P, Sezer O, Scheld H, Sahraoui K, Gansera B, Deppert O, Rubio A, Feyrer R, Sauer C, Elert O, Leyh R. Prevention of sternal dehiscence and infection in high-risk patients: a prospective randomized multicenter trial. Ann Thorac Surg. 2008 Dec; 86(6): 1897-904. https://doi.org/10.1016/j.athoracsur.2008.08.071 |
[2, 3, 6, 8, 13]
.
In this study, a composite endpoint comprising the rate of surgical site infection (SSI) and sternal dehiscence/instability was employed to evaluate the efficacy of a stainless steel wire monofilament. The findings revealed a combined rate of 3.48%, which falls within the lower range of the above mentioned rates described in the existing literature. Additionally, the incidence rates of superficial and deep sternal infections, as well as sternal dehiscence, were found to be minimal and consistent with the existing literature. Our investigation observed a single instance of sternal dehiscence/instability, which occurred 8 days post-surgery. This finding aligns with existing literature that indicates such manifestations often occur around 5 days after surgery
| [2] | Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186. https://doi.org/10.1016/j.jtcvs.2018.02.033 |
| [3] | Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1. https://doi.org/10.1016/j.jtcvs.2016.10.093 |
[2, 3]
. There were no documented cases of mediastinitis in our group.
A notable limitation of this study pertains to its observational, retrospective, single arm design, which introduces the possibility of inaccuracies in data collecting. Additionally, the study had a limited sample size of patients and a relatively short follow-up duration. Furthermore, there was no inclusion of a control group, and the comparison was made using historical data. In addition, the study did not include any comparison assessments using different forms of therapy or other materials commonly used in sternum closure procedures. Although conducting a randomised, controlled trial to assess the efficacy of various materials used in sternal closure would greatly enhance the scientific validity of the study, it is improbable to be practically achievable due to the multitude of additional factors that contribute to favourable outcomes in patients undergoing open-heart surgery.
Moreover, it is crucial to acknowledge that the degree of expertise and the number of procedures conducted by the surgical team might have an influence on the outcome and may also introduce a potential source of bias.
5. Conclusions
The utilisation of Steelex Sternum Set to close the sternum in patients undergoing cardiac valve replacement and/or reconstruction or coronary artery bypass graft surgery yielded a low incidence of postoperative complications and an enhanced quality of life for participants in the STERCCAS study, a retrospective, single-arm observational investigation carried out in Germany and Spain. These results surpassed the rates of complications reported in the existing literature. As a result, Steelex Sternum Set is a suitable and risk-free technique for sternal closure in routine clinical settings involving a wide variety of patients.
Abbreviations
ASA: American Society of Anesthesiologists
BMI: Body Mass Index
CE: Certification in Europe
CDC: US Centre for Disease Control and Prevention
CI: Confidence Interval
COPD: Chronic Obstructive Pulmonary Disease
EQ: Euro Quality of Life Group
ID: Identification Number
LVEF: Left Ventricular Ejection Fraction
Min: Minimum
Max: Maximum
N: Number
N/A: Not Applicable
NCT: Notification Clinical Trial Number
Nmiss: Missing Data
NYHA: New York Heart Association
OPTICABG: OPTIlene suture for Coronary Bypass Graft
PctN: Percentage from total Number
PREMIVALVE: PREMIcron for VALVE Surgery
Q1: Lower Quartile
Q3: Upper Quartile
SSI: Surgical Site Infection
SSI A1: Superficial Surgical Site Infection
SSI A2: Deep Surgical Site Infection
StD: Standard Deviation
STERCCAS: STERnum Closure After CArdiac Surgery
STROCSS: Strengthening the Reporting of Cohort, Cross-Sectional and Case-Control Studies in Surgery
US: United States of America
USP: United Standard Pharmacopeia
Acknowledgments
The authors would like to thank Viktor Breul for statistical analysis.
Author Contributions
Magdalena Rufa: Conceptualization, Methodology, Writing – original draft, Writing – review & editing
Adrian Ursulescu: Visualization, Writing – original draft, Writing – review & editing
Petra Baumann: Conceptualization, Resources, Data curation, Formal Analysis, Supervision, Funding acquisition, Methodology, Writing – original draft, Writing – review & editing
Manel Tauron Ferrer: Visualization, Methodology, Writing – review & editing
Funding
B. Braun Surgical SA, Barcelona, Spain, was the one who sponsored and funded the study, including the publication’s open access expenses. Aesculap AG assumed responsibility for many aspects of the project, including project management, monitoring, data administration, statistical analysis, and research registration.
Conflicts of Interest
PB is employed by Aesculap AG. The other authors declare no conflicts of interest.
References
| [1] |
Reser D, Caliskan E, Tolboom H, Guidotti A, Maisano F. Median sternotomy. Multimed Man Cardiothorac Surg. 2015 Jul 17; 2015: mmv017.
https://doi.org/10.1093/mmcts/mmv017
|
| [2] |
Pinotti KF, Cataneo DC, Rodrigues OR, Cataneo AJM. Closure of the sternum with anchoring of the steel wires: Systematic review and meta-analysis. J Thorac Cardiovasc Surg. 2018 Jul; 156(1): 178-186.
https://doi.org/10.1016/j.jtcvs.2018.02.033
|
| [3] |
Allen KB, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M, Cohen DJ. Randomized, multicenter trial comparing sternotomy closure with rigid plate fixation to wire cerclage. J Thorac Cardiovasc Surg. 2017 Apr; 153(4): 888-896. e1.
https://doi.org/10.1016/j.jtcvs.2016.10.093
|
| [4] |
Marasco SF, Fuller L, Zimmet A, McGiffin D, Seitz M, Ch'ng S, Gangahanumaiah S, Bailey M. Prospective, randomized, controlled trial of polymer cable ties versus standard wire closure of midline sternotomy. J Thorac Cardiovasc Surg. 2018 Oct; 156(4): 1589-1595. e1.
https://doi.org/10.1016/j.jtcvs.2018.04.025
|
| [5] |
Hashim S, Chin LY, Krishnasamy S, Sthaneswar P, Raja Mokhtar RA. Effect of sternal closure with biological bone adhesive on pain visual analogue score and serum cytokine. J Cardiothorac Surg. 2015 Mar 17; 10: 32.
https://doi.org/10.1186/s13019-015-0230-0
|
| [6] |
Wang B, He D, Wang M, Qian Y, Lu Y, Shi X, Liu Y, Zhan X, Di D, Zhu K, Zhang X. Analysis of sternal healing after median sternotomy in low risk patients at midterm follow-up: retrospective cohort study from two centres. J Cardiothorac Surg. 2019 Nov 11; 14(1): 193.
https://doi.org/10.1186/s13019-019-1000-1
|
| [7] |
Allen KB, Icke KJ, Thourani VH, Naka Y, Grubb KJ, Grehan J, Patel N, Guy TS, Landolfo K, Gerdisch M, Bonnell M. Sternotomy closure using rigid plate fixation: a paradigm shift from wire cerclage. Ann Cardiothorac Surg. 2018 Sep; 7(5): 611-620.
https://doi.org/10.21037/acs.2018.06.01
|
| [8] |
Dunne B, Murphy M, Skiba R, Wang X, Ho K, Larbalestier R, Merry C. Sternal cables are not superior to traditional sternal wiring for preventing deep sternal wound infection. Interact Cardiovasc Thorac Surg. 2016 May; 22(5): 594-8.
https://doi.org/10.1093/icvts/ivw017
|
| [9] |
Cataneo DC, Dos Reis TA, Felisberto G, Rodrigues OR, Cataneo AJM. New sternal closure methods versus the standard closure method: systematic review and meta-analysis. Interact Cardiovasc Thorac Surg. 2019 Mar 1; 28(3): 432-440.
https://doi.org/10.1093/icvts/ivy281
|
| [10] |
Lazar HL, Salm TV, Engelman R, Orgill D, Gordon S. Prevention and management of sternal wound infections. J Thorac Cardiovasc Surg. 2016 Oct; 152(4): 962-72.
https://doi.org/10.1016/j.jtcvs.2016.01.060
|
| [11] |
Fedak PW, Kolb E, Borsato G, Frohlich DE, Kasatkin A, Narine K, Akkarapaka N, King KM. Kryptonite bone cement prevents pathologic sternal displacement. Ann Thorac Surg. 2010 Sep; 90(3): 979-85.
https://doi.org/10.1016/j.athoracsur.2010.05.009
|
| [12] |
McGregor WE, Trumble DR, Magovern JA. Mechanical analysis of midline sternotomy wound closure. J Thorac Cardiovasc Surg. 1999 Jun; 117(6): 1144-50.
https://doi.org/10.1016/s0022-5223(99)70251-5
|
| [13] |
Schimmer C, Reents W, Berneder S, Eigel P, Sezer O, Scheld H, Sahraoui K, Gansera B, Deppert O, Rubio A, Feyrer R, Sauer C, Elert O, Leyh R. Prevention of sternal dehiscence and infection in high-risk patients: a prospective randomized multicenter trial. Ann Thorac Surg. 2008 Dec; 86(6): 1897-904.
https://doi.org/10.1016/j.athoracsur.2008.08.071
|
| [14] |
Balachandran S, Lee A, Denehy L, Lin KY, Royse A, Royse C, El-Ansary D. Risk Factors for Sternal Complications After Cardiac Operations: A Systematic Review. Ann Thorac Surg. 2016 Dec; 102(6): 2109-2117.
https://doi.org/10.1016/j.athoracsur.2016.05.047
|
| [15] |
Ursulescu A, Baumann P, Ferrer MT, Contino M, Romagnoni C, Antona C, Padró Fernández JM. Optilene, a new non-absorbable monofilament is safe and effective for CABG anastomosis. OPTICABG - A prospective international, multi-centric, cohort study. Ann Med Surg (Lond). 2018 Sep 15; 35: 13-19.
https://doi.org/10.1016/j.amsu.2018.09.005
|
| [16] |
Rufa M, Ursulescu A, Baumann P, Ferrer MT. A prospective, international, bicentric study to evaluate PremiCron suture material for cardiac valve surgery - PREMIVALVE a cohort study. Ann Med Surg (Lond). 2023 Apr 4; 85(4): 835-841.
https://doi.org/10.1097/MS9.0000000000000442
|
| [17] |
Mathew G, Agha R, Albrecht J, Goel P, Mukherjee I, Pai P, D'Cruz AK, Nixon IJ, Roberto K, Enam SA, Basu S, Muensterer OJ, Giordano S, Pagano D, Machado-Aranda D, Bradley PJ, Bashashati M, Thoma A, Afifi RY, Johnston M, Challacombe B, Ngu JC, Chalkoo M, Raveendran K, Hoffman JR, Kirshtein B, Lau WY, Thorat MA, Miguel D, Beamish AJ, Roy G, Healy D, Ather HM, Raja SG, Mei Z, Manning TG, Kasivisvanathan V, Rivas JG, Coppola R, Ekser B, Karanth VL, Kadioglu H, Valmasoni M, Noureldin A; STROCSS Group. STROCSS 2021: Strengthening the reporting of cohort, cross-sectional and case-control studies in surgery. Int J Surg. 2021 Dec; 96: 106165.
https://doi.org/10.1016/j.ijsu.2021.106165
|
| [18] |
Robicsek F, Fokin A, Cook J, Bhatia D. Sternal instability after midline sternotomy. Thorac Cardiovasc Surg. 2000 Feb; 48(1): 1-8.
https://doi.org/10.1055/s-2000-9945
|
Cite This Article
-
APA Style
Rufa, M., Ursulescu, A., Baumann, P., Ferrer, M. T. (2024). A Bicentric, International, Retrospective Study to Assess Steelex Sternum Set for Sternal Closure in Cardiac Surgery – STERCCAS a Cohort Study. Journal of Surgery, 12(2), 37-44. https://doi.org/10.11648/j.js.20241202.14
 Copy
|
Copy
|
 Download
Download
ACS Style
Rufa, M.; Ursulescu, A.; Baumann, P.; Ferrer, M. T. A Bicentric, International, Retrospective Study to Assess Steelex Sternum Set for Sternal Closure in Cardiac Surgery – STERCCAS a Cohort Study. J. Surg. 2024, 12(2), 37-44. doi: 10.11648/j.js.20241202.14
Copy
|
Download
AMA Style
Rufa M, Ursulescu A, Baumann P, Ferrer MT. A Bicentric, International, Retrospective Study to Assess Steelex Sternum Set for Sternal Closure in Cardiac Surgery – STERCCAS a Cohort Study. J Surg. 2024;12(2):37-44. doi: 10.11648/j.js.20241202.14
Copy
|
Download
-
@article{10.11648/j.js.20241202.14,
author = {Magdalena Rufa and Adrian Ursulescu and Petra Baumann and Manel Tauron Ferrer},
title = {A Bicentric, International, Retrospective Study to Assess Steelex Sternum Set for Sternal Closure in Cardiac Surgery – STERCCAS a Cohort Study
},
journal = {Journal of Surgery},
volume = {12},
number = {2},
pages = {37-44},
doi = {10.11648/j.js.20241202.14},
url = {https://doi.org/10.11648/j.js.20241202.14},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.js.20241202.14},
abstract = {Sternal fixation with steel wires or cerclages, is the gold standard for closing a midline sternotomy, the standard incision in cardiac surgery. Rare wound complications can occur following a sternotomy wire closure. The objective of this study is to establish that the clinical efficacy of the Steelex Sternum Set is equivalent to the results documented in existing literature. The cohorts of the previously conducted OPTICABG and PREMIVALVE studies served as a foundation for the design of this retrospective, bicentric, international, single-arm study. The purpose of the study was to evaluate the clinical performance of the Steelex Sternum Set for sternal closure after coronary artery bypass grafting or cardiac valve replacement/reconstruction surgery. The primary endpoint was the incidence of a composite consisting of sternum instability, sternum dehiscence, superficial and deep sternal wound infection up to six months after surgery. A quantitative summary of the available clinical literature has been conducted for comparison purposes. There were 229 patients in total (89 PREMIVALVE and 140 OPTICABG). The combined rate of surgical site infection and sternal dehiscence/instability was 3.49%, compared to 1.5 - 20% described in the literature. Severe complications such as mortality, stroke, myocardial infarction, and mediastinitis occurred in about 0.8 - 2% of cases. The Steelex Sternum Set is a safe and appropriate method for sternal closure in a diverse patient population undergoing cardiac valve replacement and/or reconstruction, as well as coronary artery bypass graft surgery, in routine clinical settings.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - A Bicentric, International, Retrospective Study to Assess Steelex Sternum Set for Sternal Closure in Cardiac Surgery – STERCCAS a Cohort Study
AU - Magdalena Rufa
AU - Adrian Ursulescu
AU - Petra Baumann
AU - Manel Tauron Ferrer
Y1 - 2024/04/17
PY - 2024
N1 - https://doi.org/10.11648/j.js.20241202.14
DO - 10.11648/j.js.20241202.14
T2 - Journal of Surgery
JF - Journal of Surgery
JO - Journal of Surgery
SP - 37
EP - 44
PB - Science Publishing Group
SN - 2330-0930
UR - https://doi.org/10.11648/j.js.20241202.14
AB - Sternal fixation with steel wires or cerclages, is the gold standard for closing a midline sternotomy, the standard incision in cardiac surgery. Rare wound complications can occur following a sternotomy wire closure. The objective of this study is to establish that the clinical efficacy of the Steelex Sternum Set is equivalent to the results documented in existing literature. The cohorts of the previously conducted OPTICABG and PREMIVALVE studies served as a foundation for the design of this retrospective, bicentric, international, single-arm study. The purpose of the study was to evaluate the clinical performance of the Steelex Sternum Set for sternal closure after coronary artery bypass grafting or cardiac valve replacement/reconstruction surgery. The primary endpoint was the incidence of a composite consisting of sternum instability, sternum dehiscence, superficial and deep sternal wound infection up to six months after surgery. A quantitative summary of the available clinical literature has been conducted for comparison purposes. There were 229 patients in total (89 PREMIVALVE and 140 OPTICABG). The combined rate of surgical site infection and sternal dehiscence/instability was 3.49%, compared to 1.5 - 20% described in the literature. Severe complications such as mortality, stroke, myocardial infarction, and mediastinitis occurred in about 0.8 - 2% of cases. The Steelex Sternum Set is a safe and appropriate method for sternal closure in a diverse patient population undergoing cardiac valve replacement and/or reconstruction, as well as coronary artery bypass graft surgery, in routine clinical settings.
VL - 12
IS - 2
ER -
Copy
|
Download